Fistula In Ano
Abnormal communication between the anal canal and rectum with exterior (perianal skin) is called fistula in ano. Even though multiple openings are seen in the perianal skin, the internal opening is always single.
Table of Contents
Aetiopathogenesis
- They occur due to persistent anal gland infection, which results in anorectal abscesses, rupture inside as well as outside resulting in a fistula. Once a fistula occurs, it persists because of infection and absence of rest to the part. As there are many anal glands, often, the problem persists despite initial treatment of one fistula.
- In India, tuberculosis is common. Patients with pulmonary tuberculosis have 1–2% chance of developing multiple anal fistulae. Whenever a patient presents with multiple anal fistulae, it is but natural to think of tubercular aetiology. Such fistulae are not indurated and there is watery discharge without pus.
- In Western countries, ulcerative colitis and Crohn’s disease are responsible for multiple anal fistulae.
- Colloid carcinoma of the rectum can present as multiple fistulae in ano. This type of carcinoma has the worst prognosis. Rectal examination should be done in every patient with anal fistula.
- Other causes of anal fistula are given in below
Fistula In Ano Classification
1. Standard Classification
- Subcutaneous
- Submucous
- Low anal
- High anal
- Pelvirectal
Special Types of Fistula In Ano:
- Fistula carcinoma
- Ileitis—Crohn’s
- Schistosomiasis
- Tuberculosis
- Ulcerative colitis
- Lymphogranuloma venereum
- Anal fissure abscess
- Students can remember as FISTULA
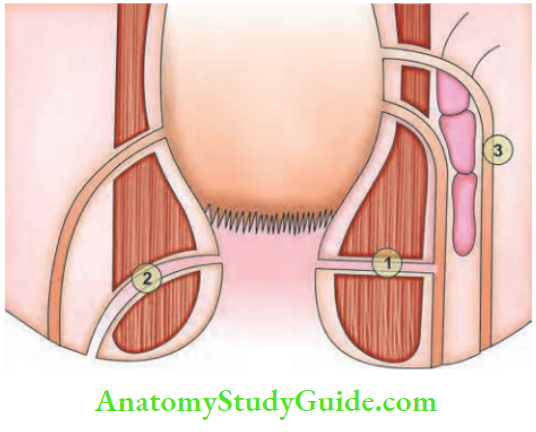
2. Park’s Classification:
- Intersphincteric
- Trans-sphincteric
- Supralevator (internal opening is situated above the anorectal bundle).
Fistula In Ano Clinical Features
- Persistent seropurulent discharge keeps the part always wet.
- Previous history of anal gland infection, with recurrent abscess.
- External opening can be single/multiple, with pouting granulation tissue, may discharge blood.
- Internal opening in carcinoma felt as a ‘button hole’ defect inside the rectum.
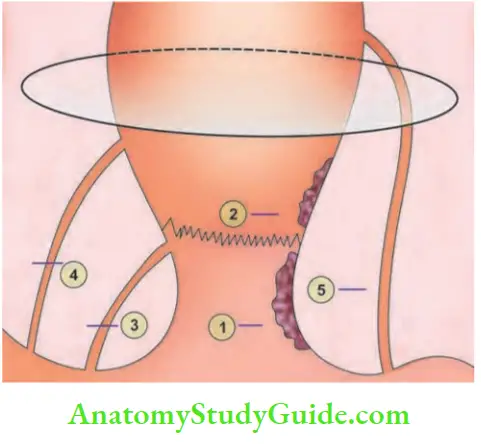
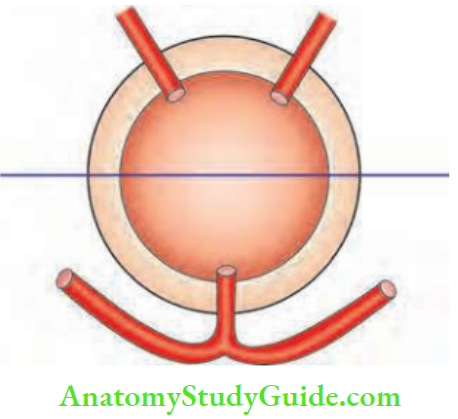
- Goodsall’s rule: A fistula, with an external opening in the anterior half of anus within 3.75 cm tends to be direct type and in the posterior half, indirect type or curved and sometimes horseshoe type. It may communicate with the opposite side.
Fistula In Ano Diagnosis
- External opening is found at the bottom of a depressed area or with granulation tissue or it is seen discharging pus.
- Internal opening may be felt on digital examination as indurated area or sometimes can be seen with proctoscopy or after sigmoidoscopy.
- The entire track may be palpable as indurated cord like structure.
- Endorectal ultrasonography and MRI seem to identify internal openings and fistula. However, they can be selectively used in deserving cases.
- Examination under general or regional anaesthesia
Fistula In Ano Treatment
1. Fistulotomy:
It is indicated in low fistula (internal opening below the anorectal bundle). A probe is passed through the external opening into the rectum and along the length of this tract the fistula is laid open. It is done under anaesthesia.
The wound is left open and allowed to heal by granulation tissue developing from the floor of the fistula (marsupialisation). Intersphincteric and low trans-sphincteric fistulas of recent origin are treated by fistulotomy and marsupialisation.






Fistula In Ano Advantages
- Least chance of recurrence
- Relatively easy procedure
- A minor degree of incontinence
2. Fistulectomy
- All chronic fistulae (low) are treated by fistulectomy by excising the entire fibrous tissues and tract. Here also, the wound is kept open.
- This can also be done for posterior semi-horseshoe and horseshoe fistulae. Some incontinence can occur.
3. Fistulectomy with or without Colostomy
- It is indicated in high fistula in ano. The internal opening is situated above the anorectal bundle. Hence, during fistulectomy, there is a chance of injury to the anorectal bundle which may cause incontinence.
- Temporary or permanent colostomy may be necessary.
- If there is a cause, treat the cause. Surgery of intersphincteric fistula and trans-sphincteric fistula may result in incontinence.
4. Use of Seton or Medicated Thread (Ksharasutra): Ksharasutra is an Ayurvedic term. It is a medicated thread passed through the entire tract and both ends are tied and tightened once a week so that by 6 weeks it cuts through
Seton:
- It is a Latin word. Seton means bristle—material such as thread, wire, or gauze that is passed through subcutaneous tissues.
- Varieties of materials used as setons—plastic tubes, infant feeding tubes, prolene suture material, medicated thread used in Ayurvedic method—Ksharasutra. Ksharasutra is a Sanskrit phrase in which Kshar refers to anything corrosive or caustic; while sutra means a thread.
- Loose setons for long-term palliation. Examples:
- Fistulae associated with Crohn’s disease, complicated recurrent fistulae.
- Cutting tight setons: Used in complicated high fistulae wherein a fistulotomy may result in anal incontinence.
- So, the seton is tied, and the patient will tighten it every day for 8–12 weeks till it comes down. Once it comes down, the seton is removed. This will decrease the chances of incontinence.
- The main advantage of Seton is it eliminates sepsis by keeping the track open.
- The disadvantage is that the patient will always feel a foreign body sensation in the rectum and anal canal.
5. Ligation of Intersphincter Fistula Tact (LIFT):
Novel approach through intersphincter which involves ligation of tract close to internal opening and removal of the intersphincter tract.
Recent Advances in Fistula Surgery:
- Biological agents: The basic principle is to plug and seal the tract. It allows the ingrowth of healthy tissue.
- Thus initially fibrin glue was used but the results are not good in the long term. Porcine small intestinal mucosa or porcine dermal collagen also has been used. Results are not satisfactory.
- Video-assisted anal fistula treatment (VAAFT): A novel sphincter-saving procedure for treating complex anal fistulae.
- Visualisation of the fistula tract using the fistuloscope.
- Aim is correct localisation of the internal fistula opening under direct vision.
- A stapler or cutaneous-mucosal flap closes the internal opening after endoscopic treatment of the fistula.
- Fistuloscopy is done under irrigation and followed by an operative phase of fulguration of the fistula tract.
- Total closure of the internal opening and suture reinforcement with cyanoacrylate. You can remember as VAAFT
Ten Commandments For Fistula In Ano
- Should find out the internal and external openings.
- Should try to define the type of fistula about the sphincter.
- Should define low or high fistula.
- Should rule out special types of fistula.
- Should conduct thorough examination again under anaesthesia before surgical procedure.
- Should do MRI in difficult, recurrent and complicated fistula.
- Should do fistulotomy in all intersphincteric fistulae and trans-sphincteric involving 30% of the voluntary musculature.
- Should do fistulectomy in low fistula—it will open up the infected cavity better even though the wound will be bigger than a simple fistulotomy wound.
- Should use setons in high fistula or complicated fistula wherein a fistulotomy may result in recurrence or incontinence or when staged procedures are planned.
- Should explain to the patient about the possibility of some degree of incontinence and consent for colostomy in high fistula.
Fissure In Ano Definition
Longitudinal tear in the lower end of anal canal results in a fissure in the ano. It is the most painful condition affecting the anal region. Commonly seen in young patients.
Aetiopathogenesis
- 90% of anal fissures occur in the posterior part of the anal canal and 10% anteriorly. It is initiated by hard stool causing a crack. As a result of this, defaecation results in pain. Anal fissure is more common posteriorly in the midline because of relative ischaemia.
- Due to pain, internal sphincter spasm takes place which makes constipation worse resulting in a chronic fissure.
- Anterior fissures occur in elderly women secondary to repeated pregnancies. This is due to damaged pelvic floor and lack of support to anal mucous membrane. Acute fissure in females may occur after vaginal delivery

Various Factors which Precipitate Anal Fissure
- Faeces—hard
- Ischaemia
- Surgical procedures—haemorrhoidectomy
- Sphincter hypertonia
- Underlying diseases—Crohn’s, sexually transmitted diseases, etc.
- Repeated childbirth
- Enthusiastic usage of ointments and abuse of laxatives
- Remember as FISSURE
Fissure In Ano Clinical Features
- Severe pain during and after defecation, burning in nature, lasting for about ½ to 1 hour because of which defecation is postponed.
- Severe constipation is present.
- Stools are hard, pellet and there is a drop of blood or streaks of fresh blood.
- Drop of blood is due to an anal fissure. A splash of blood is due to haemorrhoids, bloody slime is due to carcinoma.
- Sentinel pile refers to tag of skin at the outer end of the fissure.
- In some cases, a fissure may be associated with a small perianal abscess resulting in worsening of pain.
Fissure In Ano Diagnosis
- When the buttocks are spread apart, a longitudinal tear and a hypertrophied, thickened skin is seen near the lower end of fissure—sentinel pile.
- Per rectal examination can be done (with lignocainejelly application) and sphincter spasm can be appreciated.
- Proctoscopy is contraindicated because the condition is very painful.
Difference Between Acute Fissure In Ano And Chronic Fissure In Ano:

Fissure In Ano Treatment
1. Conservative:
- Avoid constipation—encourage a fibre diet, and mild laxatives and not to postpone defecation.
- Surface anaesthetic creams: Lignocaine jelly.
- Metronidazole and antibiotics
- Sitz bath
2. Agents which Decrease Sphincter Pressure:
- Glyceryl trinitrate (0.2%) topical application: Significant headache and 50% recurrence are drawbacks.
- It reduces spasm and increases vascular perfusion.
- Purified botulinum toxin injection into internal sphincter: It inhibits presynaptic release of
Treatment of chronic fissure in ano:

Acetylcholine from cholinergic nerve endings and causes temporary paresis of striated muscle. Cost, perianal thrombosis and sepsis are drawbacks. Injection produces prolonged but reversible effects, thus avoiding permanent injury. Calcium channel blockers: Nifedipine, diltiazem oral and topical applications (2%) also have been used.
Role of Botulinum Toxin Injection:
- Achalasia cardia and other oesophageal motility disorders.
- Anal fissures
- Sphincter of Oddi dysfunction
- Frey syndrome
3. Surgical Treatment
Lateral anal sphincterotomy of Notaras (or dorsal) is the best alternative procedure:
- Here internal sphincter is divided away from the fissure either in right or left lateral positions. The procedure can be easily done by using a bivalved speculum in the anal canal.
- This is the procedure of choice. Sphincterotomy should be limited to the length of the fissure to avoid incontinence.
Fissurectomy and local advancement flap:
- This is indicated in persistent, chronic, nonhealing fissures. After excision of the fissure, the resulting defect in the anal canal is closed by a small (rhomboid) advancement flap.
- This should be considered not as a first line of treatment. Recovery from this operation takes much more time than other treatments for anal fissures.
3. Lord’s dilatation:
- It is also called blunt sphincterotomy—a few fibres of the internal sphincter are divided. It relieves the spasm and the fissure heals.
- Rarely, in female patients, it may result in incontinence. It is not a recommended treatment nowadays.
Leave a Reply