Thigh
Question 1. Describe the great saphenous vein under the following headings
- Formation and course,
- Tributaries,
- Perforators, and
- Applied anatomy.
Answer:
Great saphenous:
The great saphenous (in Greek saphenous = easily seen) vein is the longest superficial vein of the body and represents the preaxial vein of the lower limb. It drains the venous blood from the whole of the lower extremity, except the medial side of the leg.
Great saphenous Formation and course:
- It is formed on the dorsum of the foot, by the union of the medial end of the dorsal venous arch and the medial marginal vein of the foot. It runs upward in front of the medial malleolus and crosses obliquely on the medial surface of the lower third of the tibia.
- It ascends a little behind the medial border of the tibia to reach the knee. At the knee, it lies about the hand’s breadth posterior to the patella.
- Then, it runs along the medial side of the thigh to drain into the femoral vein after piercing the cribriform fascia of the saphenous opening.
- Peculiarities: It contains 10 to 15 valves, which prevent backflow of venous blood. One of the valves is always present at the saphenofemoral junction.
- Perforating veins (perforators) connect the saphenous vein to the deep vein.
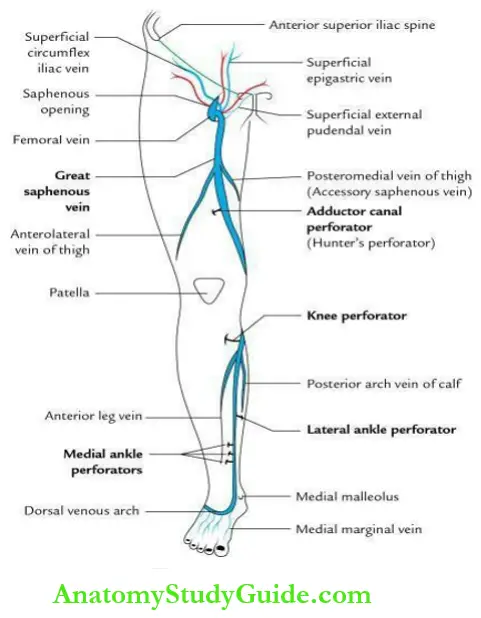
Great saphenous Tributaries:
- At commencement
- Medial marginal vein.
- In the leg (just below the knee)
- Anterior leg vein
- Posterior arch vein of calf
- Communicating vein to small saphenous vein
- In the thigh
- Posteromedial vein of thigh (accessory saphenous vein)
- Anterior lateral vein of the thigh
- Just before piercing cribriform fascia
- Superficial epigastric vein
- Superficial circumflex iliac vein
- Superficial external pudendal vein
- Just before termination
- Deep external pudendal vein
Great saphenous Perforators/perforating veins:
These are communicating veins that connect the superficial veins with the deep veins. They are provided with valves that permit the flow of blood only from superficial to deep veins.
Great saphenous Sites of perforators:
The number and location of the perforators are fairly constant in association with great saphenous veins.
Great saphenous From above downwards, these are:
- Adductor canal perforator, in the lower part of the adductor canal.
- Knee perforator, just below the knee, close to the medial border of the tibia.
- Lateral ankle perforator, at the junction of the middle and lower 1/3rd of the lateral leg.
- Three medial ankle perforators, close to the medial border of the lower third of the tibia.
Great saphenous Valves within long saphenous veins and perforating veins:
- The great saphenous vein has about 10–15 valves which prevent the backflow of blood. Of these valves, the one present at the junction of saphenous and femoral veins the saphenofemoral valve is constant and has a lot of functional significance.
- The perforators also have valves within their lumen which prevent the backflow of blood in superficial veins from deep veins.
Great saphenous Applied anatomy:
Great saphenous Varicose veins:
- These are dilated, tortuous, and enlarged superficial veins commonly seen in the lower limb. They often occur in people who are standing for a long time (e.g. traffic police personnel). The valve within the perforators and one at the saphenofemoral junction become incompetent. As a result, the flow of the blood is reversed.
- The defective veins become ‘high-pressure leaks’. Consequently, the superficial veins become dilated and tortuous forming varicose veins. The blood is stagnated in the superficial veins causing gradual degeneration of their valves and subsequent formation of varicose ulcers.
Great saphenous vein graft:
The great saphenous vein is commonly used for arterial grafting in coronary artery bypass surgery. Due to the presence of valves, a segment of the vein, to be used for grafting is reversed.
Question 2. Write a short note on superficial inguinal lymph nodes.
Answer:
Superficial inguinal:
The superficial inguinal lymph nodes (4 to 5 in number) are arranged in the form of the letter ‘T’.
- The horizontal set lies along the inguinal ligament.
- The vertical set lies along the upper part of the great saphenous vein.

Superficial inguinal Areas drained:
- The lower vertical set receives lymph from the whole of the lower limb except the lateral side of the back of the leg and the lateral side of the heel and foot.
- Upper horizontal set:
- The lateral group receives lymph from the buttocks, flanks, and back.
- The medial group receives lymph from the anterior abdominal wall, below the umbilicus, external genitalia except for the glans penis, and part of the anal canal below the pectineal line, vagina below the hymen, penile part of the male urethra and superolateral angle of the uterus.
Superficial inguinal Note:
Lymph from superficial inguinal lymph nodes is drained into deep inguinal lymph nodes.
Superficial inguinal Applied anatomy
The upper medial group of the superficial inguinal lymph node is often enlarged if there is
any infection in their drainage area (vide supra).
Question 3. Write a short note on the saphenous opening.
Answer:
Saphenous opening:
It is an oval opening in the fascia lata (deep fascia of the thigh) and lies about 4 cm below and lateral to the pubic tubercle. The saphenous opening has a sharp crescentic lateral margin, which lies in front of the femoral sheath. The medial margin is ill-defined and formed by the fascia covering the pectineus muscle. It lies at the deep level. The saphenous opening is closed by sieve-like fascia – the cribriform fascia.

Saphenous opening Structures piercing cribriform fascia:
- Long saphenous vein
- Superficial external pudendal artery
- Superficial epigastric artery
- Lymph vessels
Question 4. Write a short note on the femoral triangle.
Answer:
Femoral triangle:
It is a triangular depression on the anteromedial aspect of the upper 1/3rd of the thigh, with its apex directed downward.
Femoral triangle Boundaries
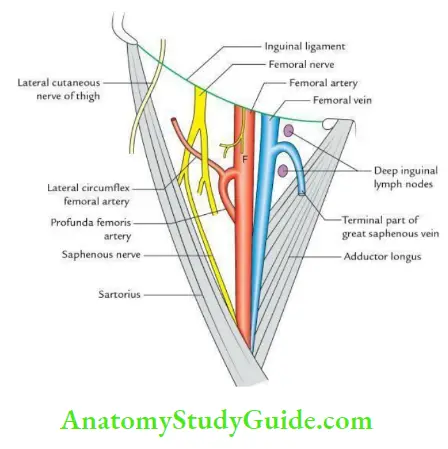
Femoral triangle Lateral:
Medial border of the sartorius.
Femoral triangle Medial:
Medial border of adductor longus.
Femoral triangle Base:
Inguinal ligament.
Femoral triangle Apex:
Meeting point of medial and lateral boundaries.
Femoral triangle Roof:
Skin, superficial and deep fasciae.
Femoral triangle Floor:
From medial to lateral: by adductor longus, pectineus, psoas major, and iliacus.
Femoral triangle Contents
- Main structures
- Femoral vein
- Femoral artery
- Femoral nerve
- Mnemonic: VAN (femoral Vein, femoral Artery, and femoral Nerve from medial to the lateral side.)
- Others
- The lateral cutaneous nerve of the thigh.
- Deep inguinal lymph nodes.
- Profunda femoris artery and its two branches the medial and lateral circumflex femoral arteries.
- Femoral branch of the genitofemoral nerve.
Femoral triangle Applied anatomy
- Femoral pulse: can be felt at the mid-inguinal point against the head of the femur.
- Swelling in the femoral triangle could be due to:
- Enlarged lymph nodes
- Psoas abscess
- Saphena varix
Question 5. Enumerate the structures damaged by stabbing at the apex of the femoral triangle. Give its applied importance.
Answer:
From before backward, these are:
- Femoral artery
- Femoral vein
- Profunda femoris vein
- Profunda femoris artery

A stab wound at the apex of the femoral triangle may be fatal as it cuts all the major vessels of the lower limb.
Question 6. Write a short on the femoral sheath.
Answer:
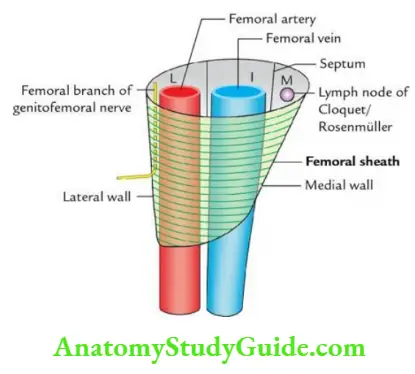
Femoral Sheath Introduction:
It is funnel–shaped fascial sleeve, enclosing the upper 1 and ½ inch of femoral vessels. It is 4 cm long. It is conical in shape with vertical lateral wall and oblique medial wall which slopes downwards and laterally.
Femoral sheath Formation
It is formed by the downward prolongation of the fascial layers of the abdominal cavity.
- Anterior wall by fascia transversalis.
- Posterior wall by fascia iliaca.
Femoral sheath Compartments
The femoral sheath is divided by two vertical septa into three compartments:
- Lateral compartment: Contains femoral artery and femoral branch of the genitofemoral nerve.
- Intermediate compartment: Contains femoral vein.
- The medial compartment is the smallest and is known as the femoral canal. It contains lymph nodes (lymph nodes of Cloquet or Rosenmüller).

Question 7. Write a short note on the femoral canal.
Answer:
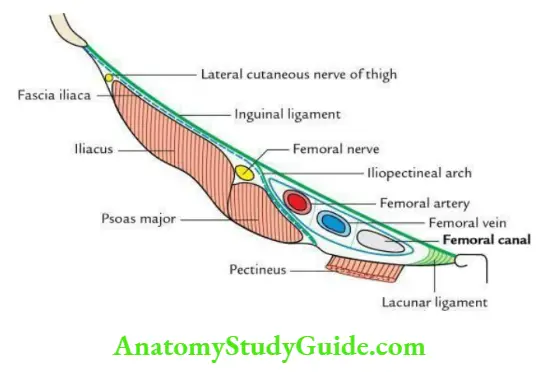
Femoral canal Introduction
- It is the small, conical medial compartment of the femoral sheath and is about 1.25 cm long.
- It does not provide a passage to the large vessels and is filled by fibrofatty tissue.
Femoral Ring:
The upper end of the femoral canal that opens into the abdomen is called the femoral ring. The ring is half an inch wide oval opening, which is closed by a condensation of extraperitoneal fat called femoral septum. The parietal peritoneum covering the septum from above shows a depression called the ‘femoral fossa’.
Femoral canal Boundaries:
- Anteriorly: Inguinal ligament.
- Posteriorly: Pectineal line and pectineus muscle and fascia.
- Laterally: Femoral vein.
- Medially: Lacunar ligament (concave margin).
Femoral canal Functions:
- Provides a dead space for expansion of the femoral vein during increased venous return.
- Provides passage to lymphatics from the lower limb to external iliac lymph nodes.
Femoral canal Applied anatomy:
The femoral ring is the potential site of weakness in the lower abdomen through which a viscus (intestine) may protrude into the femoral canal causing a femoral hernia. It is more common in females because:
- The femoral canal is wider in females due to the wider pelvis.
- The size of femoral vessels is smaller in females.
- Rise in intra-abdominal pressure during pregnancy.
The strangulated femoral hernia is released by incising the lacunar ligament. While doing so, the position of the accessory obturator artery should always be kept in mind.
The direction of enlarging hernial sac of the femoral hernia
- First, it passes downward through the femoral canal.
- Then, it passes forward to bulge through the saphenous opening.
- Finally, as it enlarges further, it passes upward and laterally along the superficial epigastric and superficial circumflex iliac vessels.

Femoral canal Covering of femoral hernia:
Femoral canal From within outward, these are:
- Peritoneum of hernial sac.
- Femoral septum.
- The anterior wall of the femoral sheath.
- Cribriform fascia.
- Superficial fascia.
- Skin.

Femoral canal Reduction of femoral hernia:
- The thigh is slightly flexed and medially rotated to get laxity of the fasciae and ligaments in the region.
- The hernia is then reduced in a direction opposite to the line of course taken by the hernial sac (vide supra).
Question 8. Write a short note on the femoral artery.
Answer:
Femoral artery Origin, course, and termination
- It is a continuation of the external iliac artery behind the inguinal ligament at the mid-inguinal point.
- After its origin, the artery passes downward and medially, successively in the femoral triangle and adductor canal.
- At the lower end of the adductor canal, it passes through adductor hiatus to continue as a popliteal artery.

Femoral artery Branches
Femoral artery In femoral triangle
Femoral artery Superficial (inguinal) branches
- Superficial external pudendal artery
- Superficial epigastric artery
- Superficial circumflex iliac artery
Femoral artery Deep branches
- Deep external pudendal artery
- Profunda femoris artery
- Muscular
- In adductor canal
- Descending genicular artery
- Muscular branches
Femoral artery Applied anatomy
- Femoral pulse can be felt at the mid-inguinal point against the femoral head.
- The femoral artery is often used for angiography.
- The femoral vein is located by feeling the pulsations of the femoral artery and then going medial to it for venepuncture.
- Ligation of femoral artery:
- If the femoral artery is ligated proximal to the origin of profunda femoris artery (PFA), anastomosis is established between the branches of PFA and branches of external and internal iliac arteries.
- If the femoral artery is ligated distal to the origin of the profundal femoris artery, the collateral circulation is established between the branches of PFA and branches of the popliteal artery and descending genicular artery.
Question 9. Write a short note on the profunda femoris artery.
Answer:
Femoris artery:
It is the largest branch of the femoral artery and is the chief source of blood supply to all
the compartments of the thigh.

Femoris Artery Origin:
It arises from the lateral side of the femoral artery about 4 cm below the inguinal ligament in front of the iliacus and spirals medially behind the femoral vessels.
Femoris Artery Course:
It leaves the femoral triangle by passing between the pectineus and adductor longus and descends successively first between the adductor longus and brevis and then between the adductor longus and Magnus.
Femoris artery Termination:
It terminates as the fourth perforating artery after piercing the adductor magnus to reach the back of the leg.
Femoris artery Branches
In addition to muscular branches, it gives off 3 sets of branches:
- Medial circumflex femoral artery: It arises in the femoral triangle. It leaves the femoral triangle by passing posteriorly between the pectineus and the psoas major. It gives the acetabular branch before terminating into transverse and ascending branches.
- Lateral circumflex femoral artery: It also arises in the femoral triangle (the largest branch). It divides into ascending, transverse, and descending branches.
- Perforating arteries: These are 4 in number, the last being the continuation of the profunda femoris artery itself.
Question 10. Write a short note on the cruciate anastomosis.
Answer:
Cruciate anastomosis:
It is an arterial anastomosis on the upper part of the back of the thigh at the lower margin of the quadratus femoris.
Cruciate Anastomosis Formation:
It is formed by four arteries that anastomose like a red cross:
- Transverse branch of medial circumflex femoral artery
- Transverse branch of lateral circumflex femoral artery
- Descending branch of the inferior gluteal artery
- Ascending branch of the first perforating branch of profunda femoris artery
Cruciate Anastomosis Note:
This anastomosis forms an indirect connection between the internal iliac and femoral arteries to provide collateral circulation if required.
Question 11. Write a short note on trochanteric anastomosis.
Answer:
Trochanteric anastomosis:
It is an arterial anastomosis in the trochanteric fossa.
Trochanteric anastomosis Formation
It is formed by the following 4 arteries:
- Descending branch of the superior gluteal artery.
- A branch from an inferior gluteal artery.
- Ascending branch of the lateral circumflex femoral artery.
- Ascending branch of the medial circumflex femoral artery.
Question 12. Write a short note on the femoral nerve.
Answer:
Femoral Nerve Origin:
It arises from the lumbar plexus in the substance of the psoas major.
Femoral nerve Root valve:
Posterior divisions of L2, L3, and L4 spinal nerves.
Femoral nerve Course:
It emerges at the lateral border of the psoas major on the posterior abdominal wall and lies between it and the iliacus. It enters the thigh by passing deep into the inguinal ligament lateral to the femoral artery. About 4 cm below the ligament, it splits into anterior and posterior divisions.
Femoral nerve Branches:

Femoral nerve Applied anatomy:
- Referred pain: Pain of hip joint disease is often referred to the knee joint and vice versa. It is also felt on the medial side of the thigh.
- Injury to femoral nerve: It causes paralysis of the quadriceps femoris causing loss of knee extension.
Question 13. Write a short note on the adductor canal/Hunter’s canal/sub sartorial canal.
Answer:
Hunter’s Canal Introduction:
- It is a musculoaponeurotic tunnel situated on the medial side of the middle third of the thigh.
- It extends from the apex of the femoral triangle to the adductor hiatus.
- It provides a passage to the femoral vessels. Which reaches the popliteal fossa through the adductor hiatus as the popliteal artery.
Hunter’s Canal Boundaries:
It is triangular in cross-section and presents the following boundaries:
- Anterolateral: Vastus medialis.
- Posterior (floor): Adductor longus above and adductor magnus below.
- Anteromedial (roof): A fibrous sheet extending between anterolateral and posterior boundaries and is overlapped by the sartorius muscle. The sub-sartorial plexus of nerves lies between the fibrous sheet and the sartorius muscle.

Hunter’s Canal Contents:
- Femoral artery
- Femoral vein
- Nerve to vastus medialis
- Saphenous nerve
- Saphenous branch of descending genicular artery, from the femoral artery
- Anterior and posterior divisions of the obturator nerve
Hunter’s canal Applied anatomy:
- The femoral artery is ligated in the adductor canal in the treatment of popliteal aneurysm.
- To control the bleeding following the rupture of the popliteal aneurysm, a tourniquet is applied to the thigh in the region of the adductor canal.
Question 14. Describe the obturator nerve in brief.
Answer:
Nerve in brief:
It is a nerve of the adductor compartment of the thigh and supplies adductor muscles along with the skin on the medial aspect of the thigh.
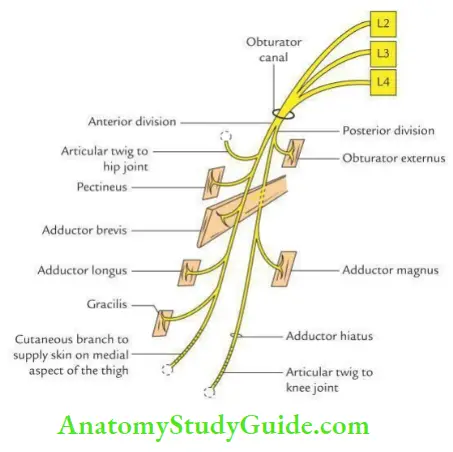
Nerve in Brief Origin:
It arises from ventral divisions of the ventral rami of L2, L3, and L4 within the substance of the psoas major muscle.
Nerve in Brief Course:
- In pelvis
- It runs medially to emerge at the medial border of the psoas, where it lies behind the common iliac vessels.
- Now, it runs lateral to internal iliac vessels along the lateral pelvic wall to enter the obturator foramen.
- In the obturator canal, it divides into anterior and posterior divisions.
- In thigh
- Anterior division passes downward into the thigh in front of the obturator externus and then descends behind the pectineus and adductor longus in front of the adductor brevis.
- The posterior division enters the thigh by piercing the anterior part of the obturator externus. Then, it descends behind the adductor brevis and adductor
Magnus.
A nerve in brief Branches:

A nerve in brief Applied anatomy:
- Referred pain: Since the obturator nerve supplies both hip and knee joints, the pain of one joint is referred to the other.
- Surgical division of obturator nerve: It is sometimes done to relieve the adductor spasm of the thigh in spastic paraplegia.
Question 15. Write a short note on the lumbar plexus.
Answer:
Lumbar plexus:
The lumbar plexus is formed in the substance of the psoas major muscle by the ventral rami of L1 to L4 spinal nerves with a contribution from the subcostal nerve (T12).
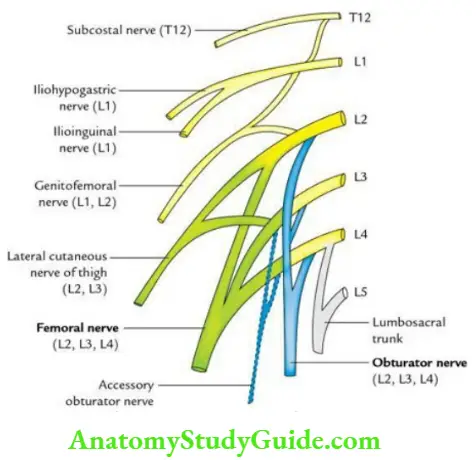
Lumbar plexus Branches:
- Iliohypogastric nerve (L1)
- Ilioinguinal nerve (L1)
- Genitofemoral nerve (L1, L2: ventral divisions)
- Lateral cutaneous nerve of thigh (L2, L3: dorsal divisions)
Lumbar plexus Note:
Sometimes (in 30% of cases), accessory obturator nerve may arise from ventral divisions of L3, L4.
Question 16. Give the origin, insertion, nerve supply, and actions of the sartorius muscle.
Answer:
Sartorius’s muscle:
The sartorius is the longest muscle in the body, which crosses the front of the thigh obliquely from the lateral to the medial side.
Sartorius muscle Origin:
From anterior superior iliac spine.
Sartorius muscle Insertion:
Into the upper part of the medial surface of the tibia.
Sartorius muscle Nerve supply:
Femoral nerve.
Sartorius muscle Actions:
- Flexion of the thigh at the hip joint.
- Flexion of the leg at the knee joint.
- Abduction and lateral rotation of the thigh.
Sartorius muscle Note:
All of the above actions of the sartorius muscle are required in assuming a crossed-leg working position, as in tailors, hence the name sartorius (L. sartor = tailor).
Question 17. Write a short note on fascia lata.
Answer:
Fascia lata:
- It is a very strong deep fascia that encloses a wide area of the thigh like a sleeve. (Latin, Latus = broad).
- It sends 3 intermuscular septa (medial, lateral, and posterior) inwards to the linea aspera of the femur and divides the thigh into 3 compartments, viz. anterior, medial, and posterior.
- On the upper medial aspect of the thigh, it presents an oval opening 4 cm below and lateral to the pubic tubercle called a saphenous opening which provides entry to the saphenous vein into the femoral vein.
Question 18. Write a short note on the iliotibial tract.
Answer:
Iliotibial tract:
It is a 2 cm wide thick fibrous band reinforcing the fascia lata on the lateral aspect of the thigh.

Iliotibial tract Origin:
It arises from gluteus maximus and tensor fascia latae.
Iliotibial tract Insertion:
Lateral condyle of the tibia.
Iliotibial tract Action:
It stabilizes the hip and knee during flexion and extension of the knee.
Question 19. Give the origin, insertion, nerve supply, and actions of the rectus femoris muscle.
Answer:
Femoris muscle:
The rectus femoris is one of the 4 components of the quadriceps femoris muscle. It is bipinnate and lies in the midline in front of the thigh. It crosses in front of both hip and knee joints.
Femoris muscle Origin:
Femoris muscle Two heads:
- Straight head: From anterior inferior iliac spine.
- Reflected head: From the groove above the acetabulum.
Femoris muscle Insertion:
Into tibial tuberosity.
Femoris muscle Note:
The patella is encased in the tendon of the rectus femoris before its insertion into the tibial tuberosity.
Femoris muscle Nerve supply:
Femoral nerve (L2, L3, L4: dorsal divisions).
Femoris muscle Actions:
Hip flexion and knee extension.
Question 20. Write a short note on the extensor apparatus of the knee joint (patella–femoral complex).
Answer:
It is formed by the following 4 components. From above downward, these are:
- Tendon of quadriceps femoris
- Patella
- Ligamentum patellae
- Tibial tuberosity
Question 21. Give the origin, insertion, nerve supply, and actions of the pectineus muscle.
Answer:
Pectineus muscle:
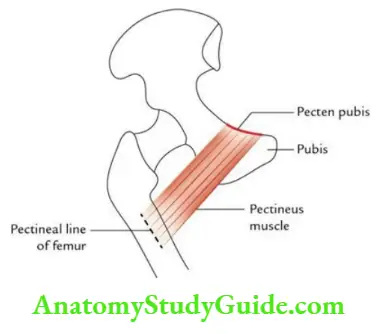
It is a flat quadrilateral muscle of the adductor compartment of the thigh. It lies on the upper medial aspect of the thigh.
Pectineus muscle Origin:
From pecten pubis and pectineal surface of pubis.
Pectineus muscle Insertion:
On the pectineal line of the femur.
Pectineus muscle Nerve supply:
Femoral and obturator nerves (i.e. dual nerve supply).
Pectineus muscle Action:
Adduction of the thigh and flexion of the hip joint.
Question 22. Give the origin, insertion, nerve supply, and actions of the adductor magnus muscle.
Answer:
Magnus muscle:
It is the largest, composite, and most posterior muscle of the adductor group of thigh muscles.
Magnus muscle Origin:
- Adductor part: From the outer part of the ischiopubic ramus.
- Hamstring part: From inferolateral part of ischial tuberosity.
Magnus muscle Insertion:
The medial margin of the gluteal tuberosity, linea aspera, medial supracondylar line, and adductor tubercle.
Magnus muscle Nerve supply:
- Adductor part by obturator nerve (L3 and L4).
- The hamstring part is the tibial part of the sciatic nerve (L4).
Magnus muscle Actions:
- The adductor part, adducts the thigh.
- The hamstring part extends the thigh.
Leave a Reply