Trachea, Oesophagus and Thoracic Duct
Describe trachea under the following heads
1. Trachea Extent,
2. Trachea Upper end,
3. Trachea Dimension,
4. Relations between the thoracic part of the trachea, and
5. Trachea Applied Anatomy.
Trachea Definition: It is a (windpipe) wide tube lying more or less in the midline, in the lower part of the neck present in the superior mediastinum.
1. Trachea Extent
- Its upper end lies at the lower border of the cricoid cartilage, opposite the 6th cervical vertebra.
- Lower end
- Living: 6th thoracic vertebra.
- Cadaver: The lower end lies at the lower border of the 4th thoracic vertebra, corresponding in front to the sternal angle.
Read And Learn More: Anatomy Important Question And Answers
Table of Contents
2. Trachea Upper end: Its upper end is continuous with the lower end of the larynx. Its lower end divides into the right and left principal bronchi.
3. Trachea Dimension
- Length: 10 to 15 cm in length.
- External diameter
- 2 cm in males and about
- 1.5 cm in females Q.
- Status variation: Lumen is smaller in the living than in the cadaver.
- Age variation: It is about 3 mm at one year of age. During childhood, it corresponds to the age in years, with a maximum of about 12 mm in adults.
4. Relations of the thoracic part of the trachea Anteriorly
- Manubrium sterni,
- Sternothyroid muscles,
- Thymus,
- Left brachiocephalic and inferior thyroid veins,
- Aortic arch, brachiocephalic and left common carotid arteries,
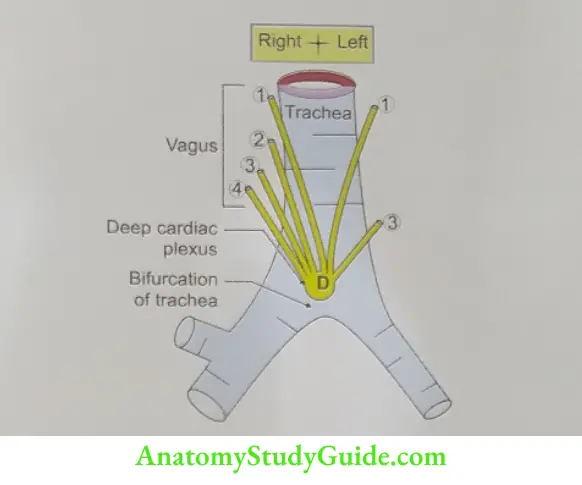
- Deep cardiac plexus, and
- Lymph nodes.
Posteriorly
- Oesophagus, and
- Vertebral column.
On the right side
- Right lung and pleura,
- Right vagus, and
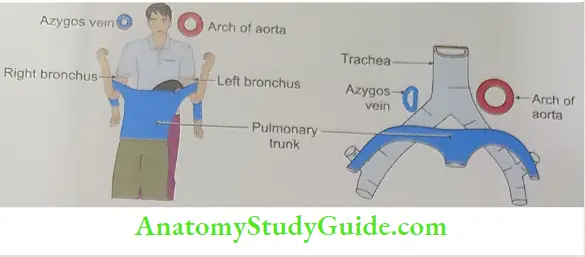
- Azygos vein
On the left side
- Arch of the aorta,
- Left common carotid,
- Left subclavian arteries, and
- Left recurrent laryngeal nerve.
Trachea Histology
- It has a fibroblastic wall supported by a cartilaginous skeleton formed by C-shaped rings.
- There are 16 to 20 rings.
- Posteriorly, there is a gap which is closed by a fibroelastic membrane and contains transversely arranged smooth muscle known as the trachealis. The serous glands.
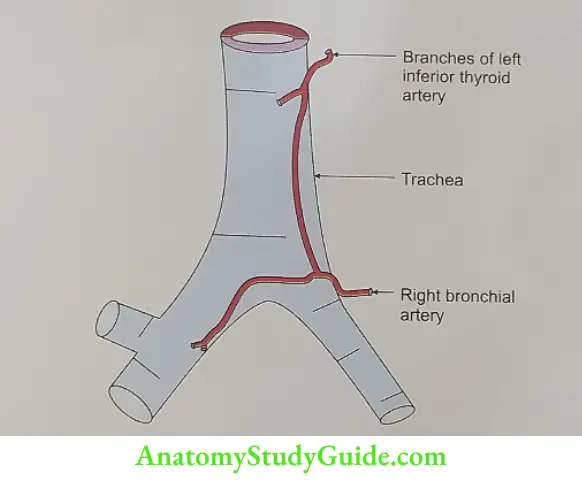
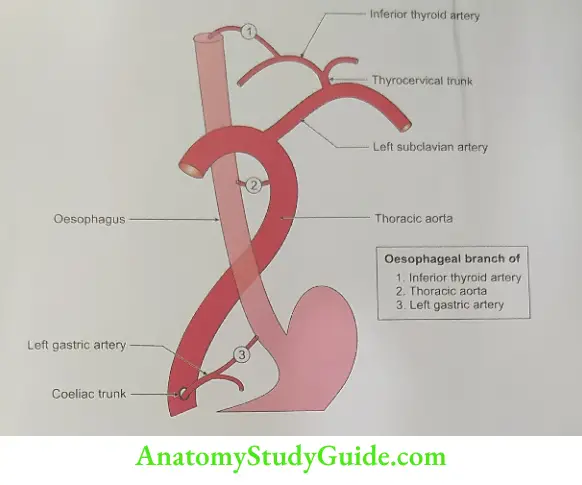
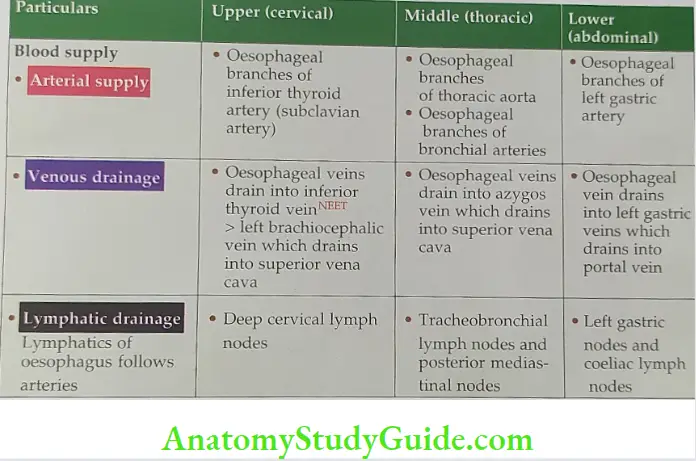
Arterial supply: Inferior thyroid arteries branches of thyrocervical trunk.
Venous drainage: Inferior thyroid vein which drains into the left brachiocephalic vein.
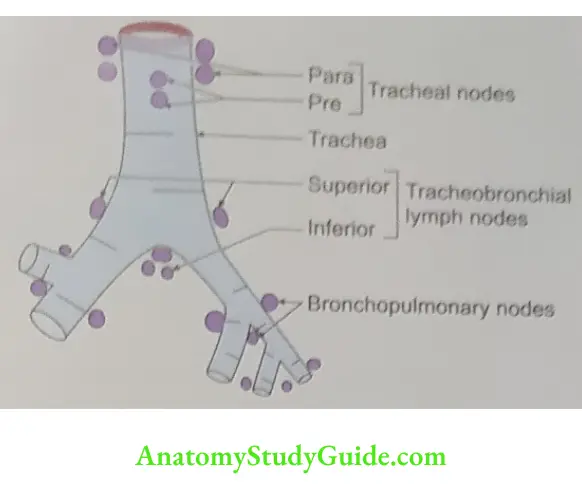
Lymphatic drainage: To the pretracheal and paratracheal lymph nodes.
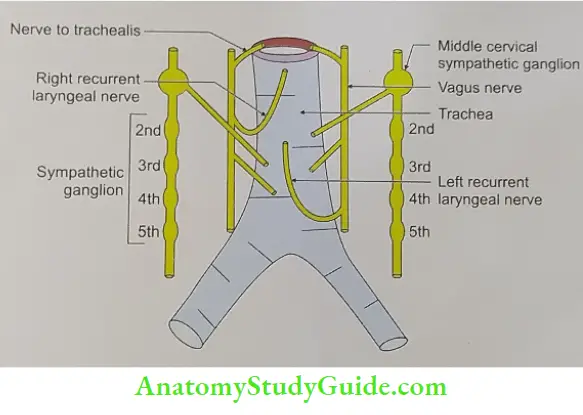
1. Nerve supply
- Parasympathetic: Nerves through vagi and recurrent laryngeal nerves. They are
- Sensory and secretomotor to the mucous membrane.
- Motor to the tracheal muscle.
- Sympathetic: Fibres from the middle cervical ganglion reach it along the inferior thyroid arteries. They are vasomotor in function.
Trachea Applied anatomy
- In radiographs, the trachea is seen as a vertical translucent shadow due to the contained air in front of the cervicothoracic spine.
- It is palpated in the suprasternal notch. Normally, it is median in position. Its shift indicates a mediastinal shift.
- Tracheostomy: It is a surgical procedure which allows air to enter directly into the trachea. It is done in case of blockage of air passage.
- As the tracheal rings are incomplete posteriorly, the oesophagus can dilate during swallowing.
- This allows the diameter of the trachea to be controlled by the tracheal muscle. The muscle narrows the calibre of the tube, compressing the contained air.
- This increases the explosive force of the blast of compressed air, as occurs in coughing and sneezing.
- The intimate relationship between the arch of the aorta, trachea and left bronchus is responsible for the physical sign known as ‘tracheal-tug’ or Oliver sign.
- It is characteristic of an aneurysm of the arch of the aorta. There is downward movement of the trachea during systole.
- Mucus secretions help in trapping inhaled foreign particles and the soiled mucus is then expelled by coughing.
- The cilia of the mucous membrane beat upwards, pushing the mucus towards the pharynx.
- The trachea may get compressed by pathological enlargements of the thyroid, the thymus, lymph nodes and the arch. This causes dyspnoea, irritative cough, and often a husky voice.
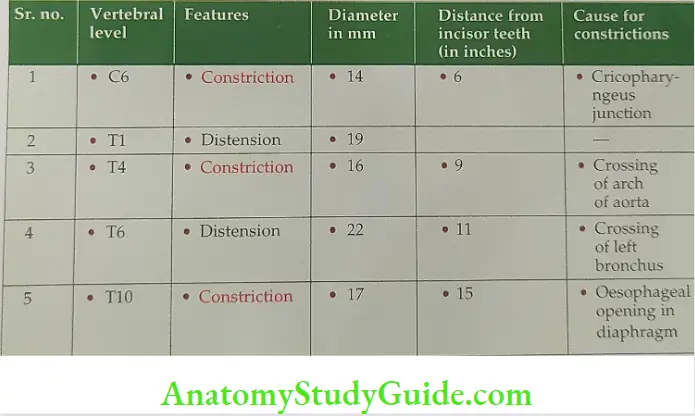
Constrictions in Oesophagus
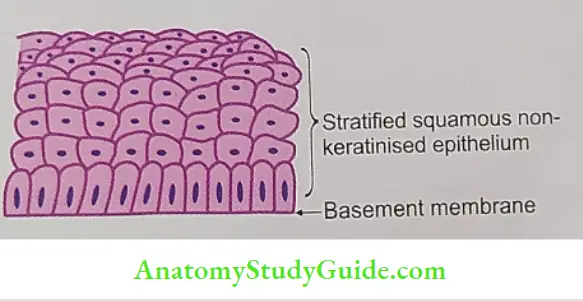
Lining Epithelium of Oesophagus
Stratified squamous non-keratinised epithelium.
The Peculiarity Of The Musculature Of Oesophagus
1. It is thick and differs in the upper, middle and lower parts of the oesophagus.
2. The upper one-third is formed by skeletal muscle.
- The middle one-third is formed by skeletal and smooth muscle.
- The lower one-third is formed by smooth muscle.
Where Do We Find Glands In the Oesophagus? What Is Their Clinical Import- Ance?
The wall of the oesophagus contains two types of glands that secrete mucus but are located in different parts of the organ.
- Oesophageal cardiac glands: They are present in the lamina propria of the proximal and distal parts of the oesophagus. They resemble the mucous glands located in the cardiac region of the stomach.
1. Submucosa contains proper oesophageal glands
- They are compound tubuloalveolar mucous glands.
- They are scattered along the entire length of the oesophagus.
- They produce mucus that lubricates the lumen of the oesophagus.
Glands In Oesophagus Functions
- They protect the mucosa.
- They facilitate the smooth passage of food material (bolus) through the oesophagus to the stomach.
Describe the Oesophagus under the following heads
1. Oesophagus Gross anatomy,
2. Oesophagus Histology, and
3. Oesophagus Applied anatomy.
1. Oesophagus Gross anatomy
- Introduction: It is the longest muscular tube of the gastrointestinal tract extending from the pharynx to the stomach.
- Extent: It extends from the lower border of the cricoid cartilage (6th cervical vertebra) to the cardiac orifice of the stomach (10th thoracic vertebra).
- The oesophagus has a physiological sphincter at the lower end of the oesophagus.
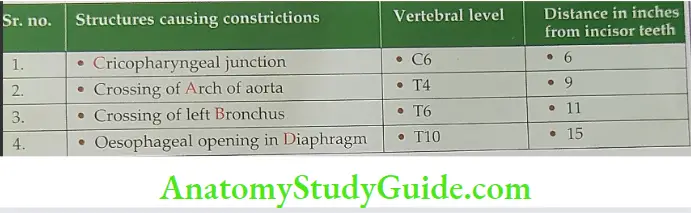
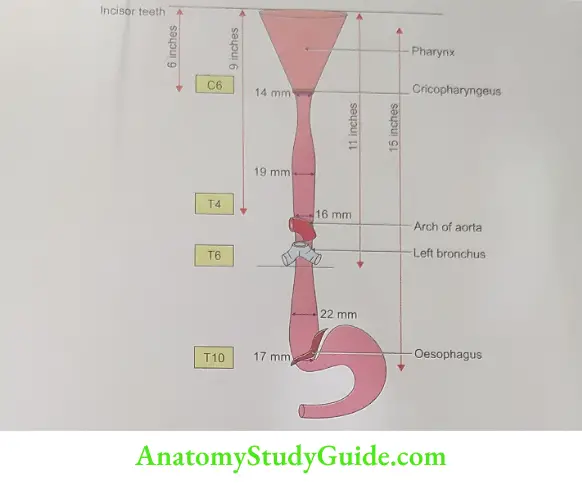
- Oesophagus Constrictions: It shows four constrictions at the following levels
- Where it is crossed by the Aortic arch.
- Where it is crossed by the left Bronchus.
- At its commencement (caused by the Cricopharyngeus sphincter).
- Where it pierces the Diaphragm.
Oesophagus Nerve supply
- Sympathetic fibres: These arise from T5 – T9 segments of the spinal cord and form the oesophageal plexus.
- Parasympathetic fibres: These are derived from vagi and recurrent laryngeal nerves. The nerve cells in the myenteric and submucous plexuses act as postganglionic neurons for parasympathetic fibres only.
- The congenital absence of these nerve cells produces disturbance in peristalsis relaxation). and the condition is known as cardiospasm or achalasia (a-not; achalasia-
2. Oesophagus Histology: It is formed by four layers from the inside out.
consists of
- Mucosa: It is thick and is in the collapsed state thrown into longitudinal folds. It
- The surface epithelium of stratified squamous non-keratinized. It is replaced by columnar epithelium at the gastro-oesophageal junction.
- Lamina propria.
- Thick muscularis mucosa which shows an internal circular layer and an external longitudinal layer. A nerve plexus may be found among the muscle fibres.
- Submucosa: It contains all connective tissues. It contains mucous glands which the oesophagus. It contains are sparse and are found in the upper and lower ends. The secretion lubricates
- Submucous glands, and
- Plexus of
- Arteries,
- Veins,
- . Lymphatics and
- Nerves.
Muscularis externa: It consists of inner circular and outer longitudinal, which are the longest smooth muscle cells of the body. are of skeletal muscle in the upper part and smooth muscle in the lower part. It is a Serosa lined by a thick fibrous coat.
3. Oesophagus Applied anatomy
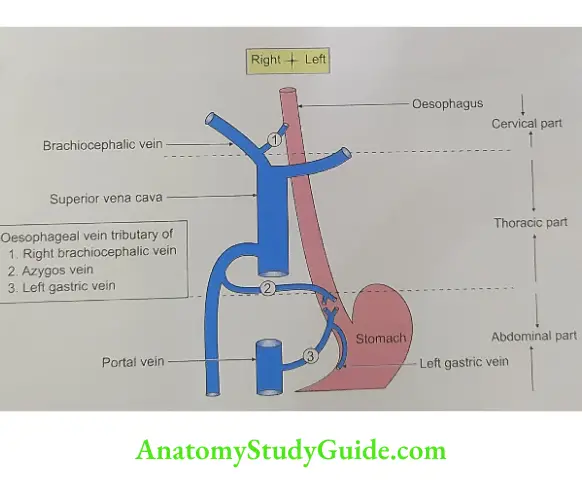
- Oesophageal varices: The lower end of the oesophagus is one of the main sites of portocaval anastomosis. Here the tributaries of the left gastric vein anastomose profusely with the tributaries of azygos and hemiazygos veins.
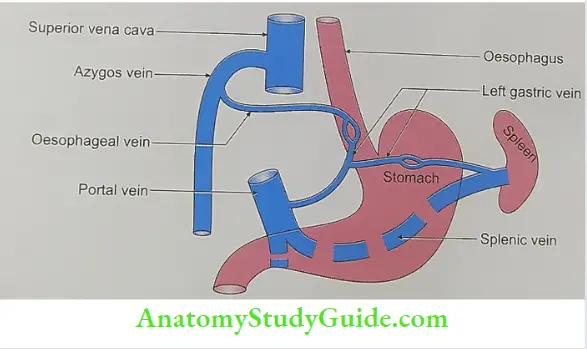
- In portal hypertension, there is shunting of the blood from the portal to the caval system. There is dilatation and tortuosity of these collateral channels which is called oesophageal varices. Rupture of these veins results in haematemesis (i.e. vomiting of frank red-coloured blood). This differentiates haematemesis arising from perforation of gastric ulcers which is black-red in colour.
- Dysphagia: Difficulty in swallowing which is seen in obstruction called barium swallow. dysphagia while painful swallowing odynophagia. This can be diagnosed by
- Achalasia cardia: It is due to neuromuscular in-coordination of muscles of the lower end of the oesophagus. This results in loss of peristalsis and there is a failure of relaxation of the lower end of the oesophagus. Consequently, the food accumulates in the oesophagus causing regurgitation. The regurgitant does not include gastric contents and is not sour-tasting. Achalasia is the most common oesophageal motility disorder, with an incidence of 6 per 100,000 individuals.
Describe the Thoracic Duct under the following heads
1. Thoracic Duct Gross anatomy,
2. Thoracic Duct Tributaries,
3. Thoracic Duct Histology,
4. Thoracic Duct Development, and
5. Thoracic Duct Applied anatomy.
1. Thoracic Duct Gross anatomy
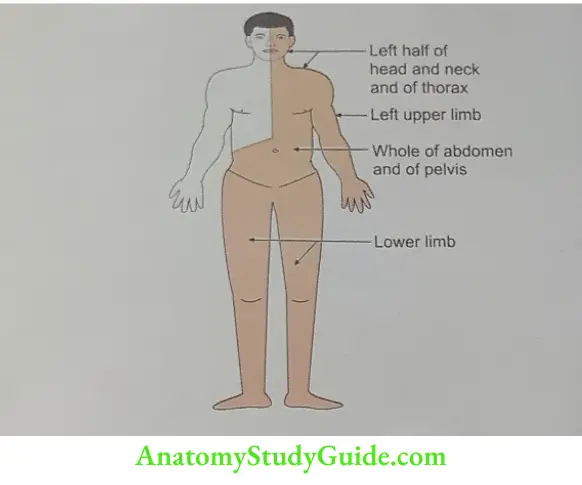
- Introduction: It is a lymphatic channel present in the thoracic region. It drains the lymph from the lower half and left upper half of the body.
- Appearance: Beaded.
- Measurement: Length x width (cm) 45 × 0.5
- Extent: Lower border of T12 vertebra to 7th cervical vertebra.
- Commencement: It commences from the cranial end of cisterna chyli.
- Termination: It terminates in the left brachiocephalic vein at the junction of the left subclavian and left internal jugular veins.
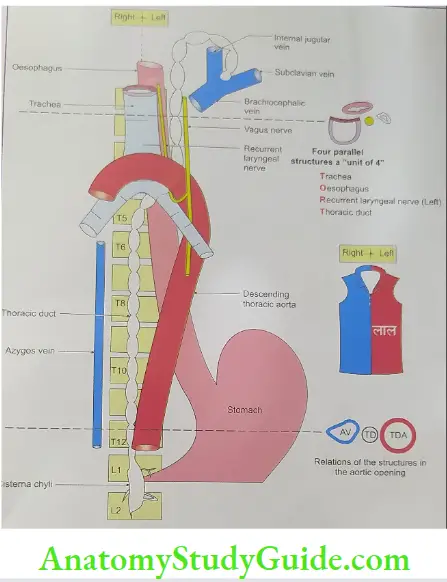
- Course and relations
- It passes through the aortic opening of the diaphragm which is present at the 12th thoracic vertebra.
- Here it accompanies on the left side by descending thoracic aorta and on the right side by azygos vein.
- It lies posterior to the oesophagus up to the 5th thoracic vertebra.
- It ascends upward and at the level of the 5th thoracic vertebrae, it takes a left turn and enters the superior mediastinum.
- At the level of the 7th cervical vertebra, it arches laterally, which is 3 to 4 cm above the left clavicle.
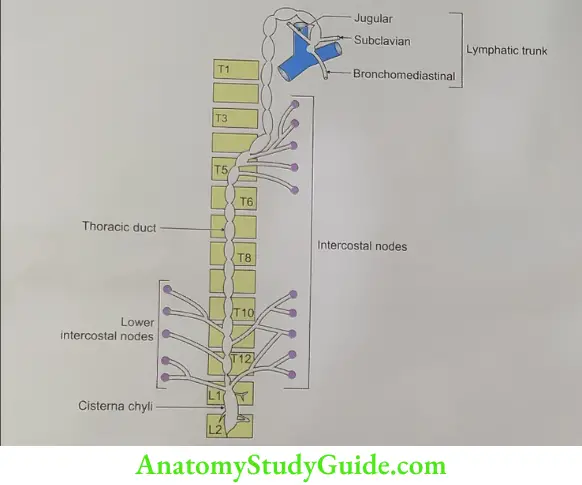
2. Thoracic Duct Tributaries
- At commencement, it receives a confluence of the lymph trunk.
- In the thorax, it receives lymph trunk from
- The upper lumbar region,
- Posterior mediastinum, and
- Upper 6 intercostal spaces.
- In the neck, it receives two tributaries
- Left subclavian lymph trunk, and
- Left jugular lymph trunk.
The thoracic duct does not drain from
- Head, neck: Right side of head and neck,
- Thorax
- The right side of the thoracic wall,
- Right lung,
- Right half of the heart,
- Upper limb: Right upper limb
- Abdomen: The convex surface of the liver
3. Thoracic Duct Histology: It has three layers
- Tunica externa,
- Tunica media: It shows connective tissue fibres arranged along the long axis of the vessels, and
- Tunica intima: It shows a well-defined subendothelial layer.
4. Thoracic Duct Development: It develops from
- Two longitudinal channels are present by the side of the primitive vertebral column.
- They are connected by transverse channels at the level of the 5th thoracic vertebra. The right upper and left lower limbs of the original longitudinal channel disappear and the remaining part gives to the thoracic duct.
.
5. Thoracic Duct Applied anatomy
- Obstruction of the duct is caused by
- Surrounding tumour or by
- Microfilaria.
- Injury of the duct leads to leakage of chyli and the condition is called chylothorax.
Leave a Reply