Anaerobes Clostridium And Non-Sporing Anaerobes
Anaerobic bacteria do not have cytochrome system for oxygen metabolism and hence are unable to neutralize toxic oxygen metabolites. They can be classified as:
Table of Contents
- Obligate anaerobes:
- They cannot grow in presence of oxygen as they completely lack superoxide dismutase and catalase and are susceptible to the lethal effects of oxygen.
- For example, most of the Clostridia and non-sporing anaerobes
Read And Learn More: Micro Biology And Immunology Notes
- Aerotolerant anaerobes:
- They do not utilize oxygen for growth, but tolerate its presence.
- This is because they possess small amounts of superoxide dismutase and peroxidase (but lack catalase) which may neutralize the toxic oxygen radicals.
- Examples include
- Clostridium histolyticum and Bacteroides.
Clostridium
Clostridia are obligate anaerobic gram-positive bacilli, having bulging spores:
- Clostridia are saprophytes found in soil, organic matter, and also in intestine of animals including humans .
- Only few infect humans, such as C. perfringens, C. tetani,C. botulinum and C. difficile
- Industrial importance: Some clostridia, such asC. acetobutylicum and C. butyricum are used to prepare chemicals, such as acetone and butanol.
- They are motile (exhibit stately motility) except C. perfringens, C. ramosum and C. tetani VI.
- They are noncapsulated except C. perfringens andC. butyricum.
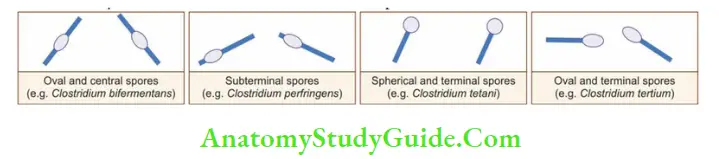
- Most of the clostridia bear a sub-terminal spores except:
- C. tetani: Produces spherical and terminal spore (drum stick appearance)
- C. tertium: Produces oval and terminal spore (tennis racket appearance)
- C. bifermentans: Produces central and oval spore.
Clostridium Perfringens
- C. perfringens (previously, C. welchii) is a saprophyte and commensal in the large intestine of human beings and animals:
- It is capsulated, nonmotile, gram-positive bacillus
- It bears sub-terminal bulging spores; but the gas gangrene strains do not produce spores.
Virulence Factors
- C. perfringens is invasive as well as toxigenic. The toxins and the other virulence factors can be grouped into:
- Four major toxins: Alpha (α), beta (β), epsilon (ε) and iota (ι).
- Alpha toxin (or lecithinase or phospholipase C) is the principle virulence factor for gas gangrene and food poisoning.
- Eight minor toxins: Gamma (γ), delta (δ) lambda (λ), kappa (κ), theta (θ), eta (η), mu (μ) and nu (υ)
- They also produce heat labile enterotoxin.
- Soluble substances produced by C. perfringens are neuraminidase, histamine, bursting factor (produce muscle lesions) and circulating factor (inhibit phagocytosis).
Clostridium Perfringens Clinical Manifestations
C. perfringens infections are mostly polymicrobial involving other clostridia species. Various manifestations include:
Clostridial Wound Infection
- MacLennan has classified them as:
- Simple wound contamination,
- Anaerobic cellulitis,
- Anaerobic myositis (gas gangrene).
Clostridial Enteric Infection
- Food poisoning: Caused by C. perfringens type A enterotoxin (coded by gene cpe)
- Enteritis necroticans (gas gangrene of the bowel):
- Ischemic necrosis of the jejunum and gas in tissue plane
- Also known as pigbel in Papua New Guinea and darmbrand in Germany.
- Caused by C. perfringens type C producing β toxin.
- Necrotizing enterocolitis: Resembles enteritis necroticans but associated with C. perfringens type A, has been found in previously healthy adults.
- Gangrenous appendicitis.
Other Clostridial Infections
- Bacteremia: C. perfringens followed by C. tertium andC. septicum.
- Skin and soft-tissue infections: C. perfringens, C. histolyticum, C. septicum, C. novyi, and C.sordellii cause necrotizing infections of the skin and soft tissues.
- Infection of the endometrium leading to toxic shock syndrome (C. sordellii).
- Meningitis and brain abscess.
- Panophthalmitis (due to C. sordellii or C. perfringens).
Clostridium Tetani
- C. tetani is obligate anaerobic, gram-positive bacillus with terminal round spores (drum stick appearance):
- It is the causative agent of ‘tetanus’ manifested by skeletal muscle spasm and autonomic nervous system disturbance.
- C. tetani is widely distributed in soil, hospital and intestine of man and animals.
Virulence Factors
- C. tetani produces two exotoxins: Tetanolysin and tetanospasmin:
- Tetanolysin is a heat labile, oxygen labile hemolysin. It plays no role in the pathogenesis.
- Tetanospasmin or tetanus toxin (TT) is a neurotoxin responsible for the pathogenesis oftetanus:
- It is oxygen stable but heat labile; coded by plasmid.
Mechanism of action: Toxin acts pre-synaptically at the inhibitory neuron terminals and prevents release of inhibitory neurotransmitter GABA and glycine → leads to spastic muscle contraction. Strychnine poisoning has a similar mechanism except that it acts post-synaptically.
Mode of Transmission
Tetanus bacilli enter through:
- Injury like road traffic accidents, unsterile surgery/abortion/delivery, otitis media (otogenic tetanus)
- It is noninfectious: There is no person to person spread.
Clinical Manifestations
- Incubation period is about 6–10 days. Shorter the IP, graver is the prognosis.
- Muscles of the face and jaw are often affected first (due to shorter distances for the toxin to reach the nerve terminals).
- 1st symptom: Increase in the masseter tone leading to trismus or lock jaw, followed by muscle pain and stiffness, back pain, and difficulty in swallowing.
- In neonates, difficulty in feeding is the usual presentation
- As the disease progresses, painful muscle spasm develops which may be:
- Localized: involves the affected limb
- Generalized painful muscle spasm: leads to descending spastic paralysis.
- Hands, feet are spared and mentation is unimpaired
- Deep tendon reflexes are exaggerated
- Autonomic disturbance is maximal during the second week of severe tetanus-characterized by low or high blood pressure, tachycardia, intestinal stasis, sweating, increased tracheal secretions and acute renal failure.
Complications
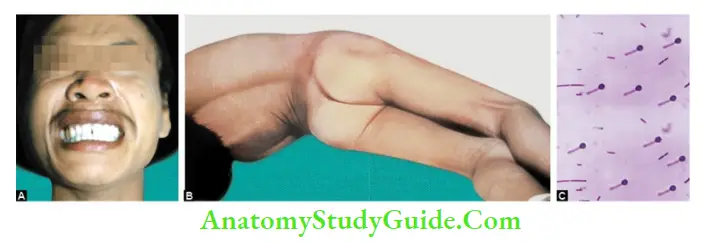
- Risus sardonicus: Characteristic, abnormal, sustained spasm of the facial muscles that appears to produce grinning.
- Opisthotonos position of the body occurs due to generalized spastic contraction of extensor muscles.
- Respiratory muscles spasm—may cause airway obstruction.
- Warm climate, rural area with fertile soil is associated with increased risk.
Laboratory Diagnosis
Treatment should be started immediately based on clinical diagnosis. Laboratory diagnosis helps only in confirmation.
- Specimen: Excised tissue bits from the necrotic depths of wounds.
- Gram staining:
- Reveal gram-positive bacilli with terminal and round spores (drumstick appearance)
- However microscopy alone is unreliable as it cannot distinguish C. tetani from morphologically similar clostridia like C. tetanomorphum and C. sphenoides.
- Culture: Culture is more reliable than microscopy:
- In RCM broth: C. tetani, being proteolytic turns the meat black and produces foul odor.
- Blood agar: C. tetani produces characteristic swarming growth.
- Toxigenicity test: For demonstration of toxin production
- In vitro hemolysis inhibition test: detects tetanolysin
- In vivo mouse inoculation test: detects tetanospasmin.
Treatment
- Passive immunization (tetanus immunoglobulin): It is the treatment of choice:
- Two preparations are available:
- Immunity Category
- Simple wound
- Wound <6 hrs, clean, non-penetrating,no/negligible tissue damage
Complicated wounds
(Other wounds)
- Category A Nothing required Nothing required
- HTIG (Human tetanus immunoglobulin): 250 IU (protects for 30 days)
- ATS (anti-tetanus serum, equine derived): 1500 IU (protects for 7–10 days)
- HTIG is preferred as ATS is associated with side effects, such as serum sickness and anaphylactoid reactions
- Combined immunization (Both active and passive immunization): Indicated in nonvaccinated person
- Antibiotics: Antibiotics has minor role as they cannot neutralize the toxin once released:
- However, they are useful (1) In early infection before expression of the toxin (before 6 hrs), (2) To prevent further release of toxin
- Metronidazole is the drug of choice. Penicillin can be given alternatively.
Prevention by Active Immunization (Vaccine)
Tetanus toxoid (TT) is used for active immunization. It is available either as
- Monovalent vaccine as TT and
- Combined vaccine as DPT
- Primary immunization of children: Under national immunization schedule of India, total seven doses are given; three doses of DPT at 6, 10 and 14 weeks of birth followed by two booster doses of DPT at 16–24 weeks and 5 years followed by two additional doses of TT at 10 years and 16 years.
Adult immunization:
- It is indicated if primary immunization is not administered in childhood.
- Four doses of TT is given; 2 doses of TT at 1 month interval followed by 2 booster doses at 1 yr and 6 yrs.
- Site: TT is given deep IM at anterolateral aspect of thigh (children) and in deltoid (adults).
- Protective titer of tetanus antitoxin is ≥ 0.01 unit/mL.
Prevention of Tetanus after Injury
All types of wounds need surgical toilet followed by immunization which depends on the wound type and immunization status of the individual.
Recommendation for prevention of tetanus after injury

- Category B Toxoid 1 dose Toxoid 1 dose
- Category C Toxoid 1 dose Toxoid 1 dose + HTIG
- Category D Toxoid complete dose Toxoid complete dose + HTIG
- Category A: Taken complete course of TT/booster within the past 5 years
- Category B: Taken complete course of TT/booster within the past > 5 years < 10 years
- Category C: Taken complete course of TT/booster within the past >10 years
- Category D: Not Taken complete course of TT/booster or immunity status is unknown.
Prevention of Neonatal Tetanus
Neonatal tetanus is defined by WHO as ‘child loses ability to suck and cry between day 3 and 28 of life and becomes rigid and has spasms’.
- It is also known as ‘8th day disease’ as the symptoms usually starts after 1 week:
- Most common reason: Unhygienic practices during deliveries, such as infected umbilical stumps due to application of cow dung, rarely by circumcision or by ear piercing.
- Seasonal: More common in July, August and September months.
- Neonatal tetanus can be prevented by: Discouraging home deliveries and promoting hospital or attended deliveries.
- Following aseptic clean practices are followed during deliveries: clean hand, clean surface, clean blade for cutting cord, clean cord tie, clean cord stump, clean towel and clean water.
- TT (2 doses) are given to all pregnant women during 2nd trimester at 1 month gap.
Leave a Reply