Clinical Microbiology (Infective Syndromes)
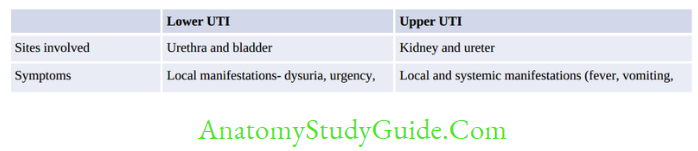
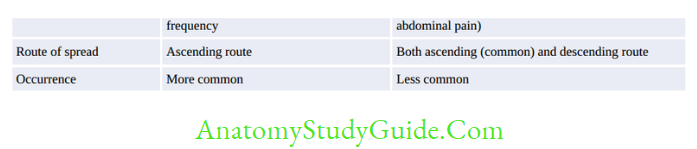
Urinary Tract Infections
Urinary tract infection (UTI) is the second most common infection after respiratory tract infections in the community.
Table of Contents
- UTI is the leading cause of gram-negative sepsis (urosepsis) especially in hospitalized patients and the urinary catheters are the origin of nearly 50% of nosocomial UTIs.
- UTI is the most common HAIs (hospital-acquired infections) accounting for 35%.
Predisposing Factors
- Prevalence: About 10% of humans develop UTI in some part of their life
- Gender: UTI is predominantly a disease of females. The higher prevalence in females is due to:
- Short urethra,
- Close proximity of urethral meatus to anus; so that there is more chance of introduction of endogenous bacteria into the urinary tract.
Read And Learn More: Micro Biology And Immunology Notes
- Age: Incidence increases with age.
- In males, increased incidence of UTI seen in old age.
- Incidence is 10–20% among adult females and reinfection is common in females (20–40 years of age),
- Pregnancy: Anatomical and hormonal changes in pregnancy favor development of UTIs.
Most females develop asymptomatic bacteriuria during pregnancy. - Structural and functional abnormality of urinary tract may cause obstruction to the urine flow and urinary stasis; which predisposes to infection
- Bacterial virulence such as expression of pili helps in bacterial adhesion to uroepithelium
- Weakened vesicoureteric reflux
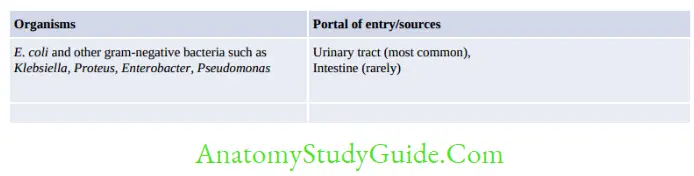
Microorganisms causing UTI
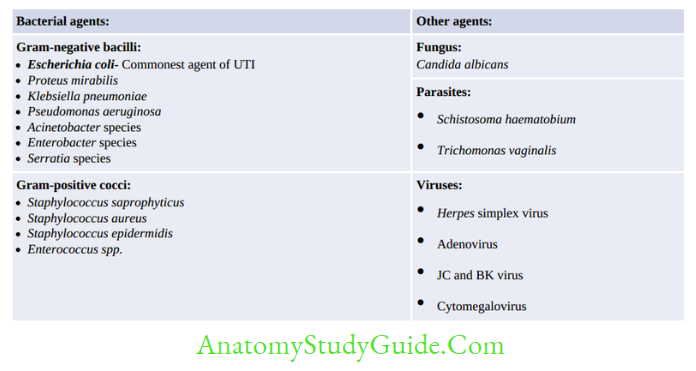
Most organisms are acquired by ascending route. Organisms acquired by descending route include – Staphylococcus aureus, Salmonella, Mycobacterium tuberculosis, Leptospira and Candida.
Treatment of UTI
- Treatment should be based on antimicrobial susceptibility testing report.
- Quinolones (e.g. norfloxacin), nitrofurantoin, cephalosporins, and aminoglycosides are among the preferred drugs.
- Higher antibiotics such as carbapenem (e.g. meropenem), beta lactam-beta lactam inhibitor combinations (e.g. piperacillin-tazobactam) or fosfomycin are used for treatment of hopsital acquired UTIs due to multidrug-resistant gram-negative bacilli.
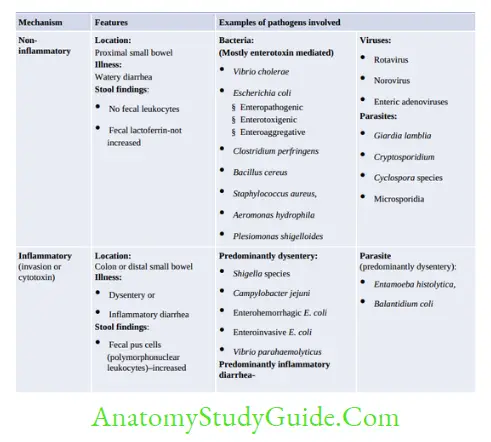
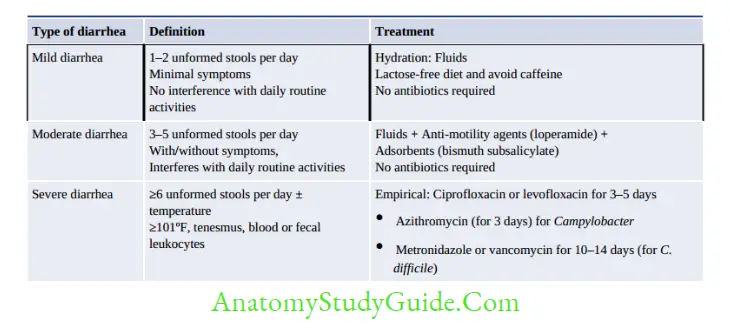
Diarrhea, Dysentery And Food Poisoning
- Diarrhea: Defined as passage of three or more loose or liquid stools per day, in excess than the usual habitat for that person (World Health Organization).
- Gastroenteritis: Defined as inflammation of the mucous membrane of stomach and intestine resulting in combination of diarrhea, vomiting and pain abdomen with or without mucus/blood/fever/dehydration.
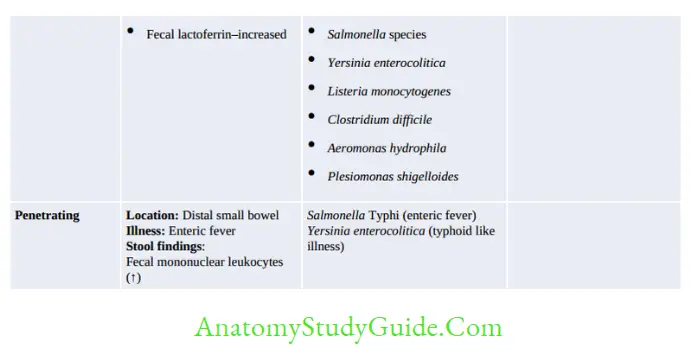
- Dysentery: It is characterized by diarrhea with increased blood and mucus, often associated with fever, abdominal pain, and tenesmus
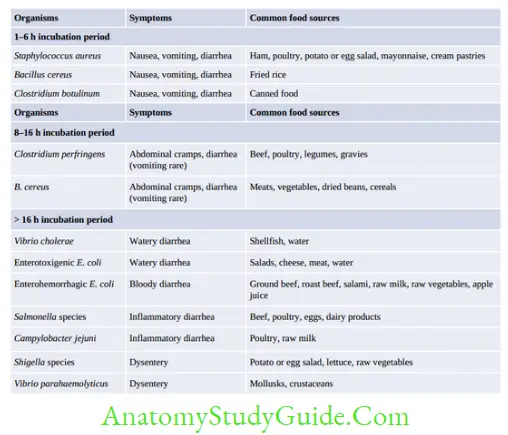
- Food Poisoning: It refers to an illness acquired through consumption of food or drink contaminated either with microorganisms, or their toxins.
Inoculum Size
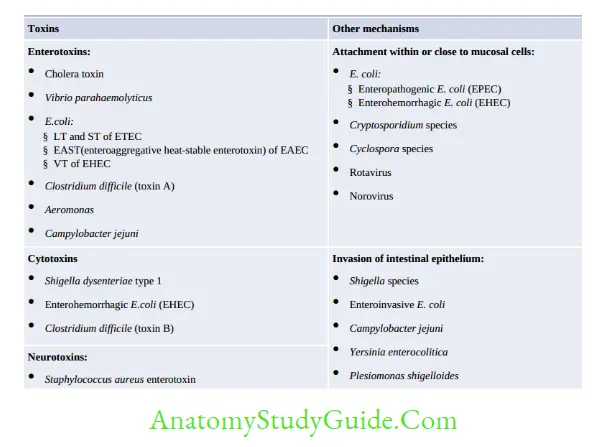
Enteric pathogens differ from each other in their infective dose required to initiate infection:
- Shigella, enterohemorrhagic E. coli, Giardia, or Entamoeba: 10–100 bacteria or cysts
- Vibrio cholerae: 105–108 bacilli
- Salmonella: 103–105 bacilli.
Host Factors Promoting Diarrheal Diseases
- Suppression of the normal flora
- Neutralization of gastric acidity: Promote the acid labile pathogens (e.g. V. cholerae)
- Inhibition of intestinal motility:
- Impaired host immunity
- People with blood group O show increased susceptibility to disease due to V. cholerae,
Shigella, E. coli O157, and Norovirus.
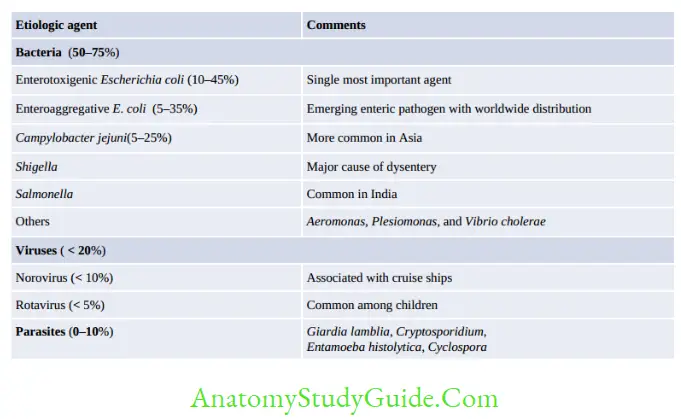
Traveler’s Diarrhea
- It is the most common travel-related infectious illness.
- Occurs in about 20–50% of people traveling from temperate industrialized countries to tropical regions of Asia, Africa, and Central and South America
- Characterized by a sudden onset of abdominal cramps, anorexia, and watery diarrhea.
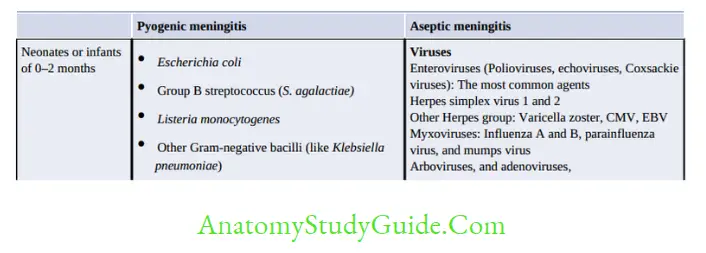
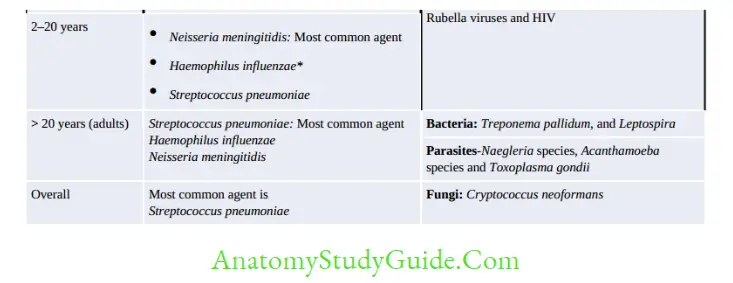
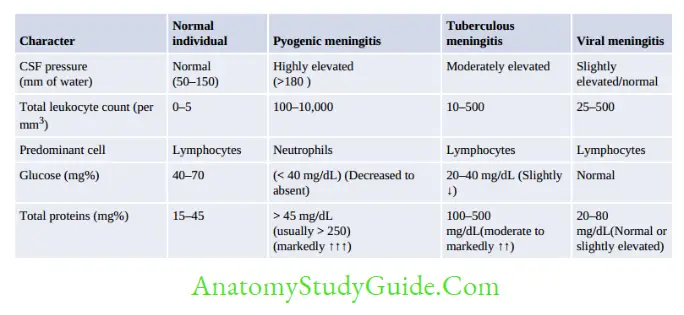
Meningitis
Meningitis is an inflammation of the meninges surrounding the brain and spinal cord. In true sense, it implies to infection of subarachnoid space or the leptomeninges (arachnoid and piamater) but not dura mater.
Pathogenesis
Routes of Infection:
- Hematogenous spread (most common route)
- Direct spread from an infected site present close to meninges—otitis media, mastoiditis,sinusitis, etc.
- Anatomical defect in CNS as a result of surgery, trauma, congenital defects
- Direct intraneural spread along the nerve: This is the least common route, occurs in cases of rabies virus or herpes simplex virus infection.
Treatment
If pyogenic meningitis is suspected
- Empirical therapy:
- Adult: IV cefotaxime or ceftriaxone and vancomycin
- If Listeria is suspected, IV ampicillin can be added
- For neonates: IV ampicillin plus gentamicin
- Definitive therapy: Treatment is modified based on the organism isolated and its sensitivity pattern, once the culture report is available.
- For tubercular meningitis: An antitubercular drug is started according to RNTCP guidelines.
- For cryptococcal meningitis: Amphotericin B plus flucytosine for 2–4 weeks for Induction phase and Fluconazole for 6–12 months for maintenance phase.
- For viral meningitis: IV acyclovir is given.
Bloodstream Infections
Bloodstream infections (BSIs) refer to presence of microorganisms in blood, which are a threat to every organ in the body.
- Bacteremia refers to the presence of bacteria in blood without any multiplication
- Septicemia is a condition in which bacteria circulate and actively multiply in the bloodstream (and may produce their products, e.g. toxins) that cause harm to the host.
Types of Bloodstream Infections (BSI)
Two major categories: Intravascular and Extravascular.
Intravascular Bloodstream Infections
They originate within the cardiovascular system, lead to continuous bacteremia:
- Infective endocarditis (Modified Duke criteria for the clinical diagnosis)
- Mycotic aneurysm
- Suppurative thrombophlebitis
- CRBSI (catheter-related bloodstream infection).
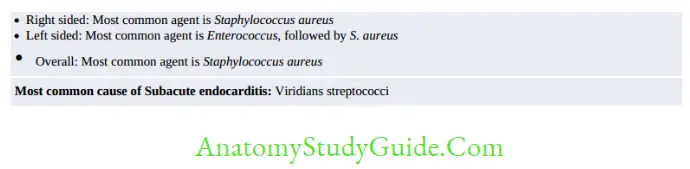
- Infective Endocarditis: It is the infection of endocardium, characterized by presence of ‘vegetation’ which is composed of mass of platelets, fibrin, microcolonies of organisms, and scanty inflammatory cells.
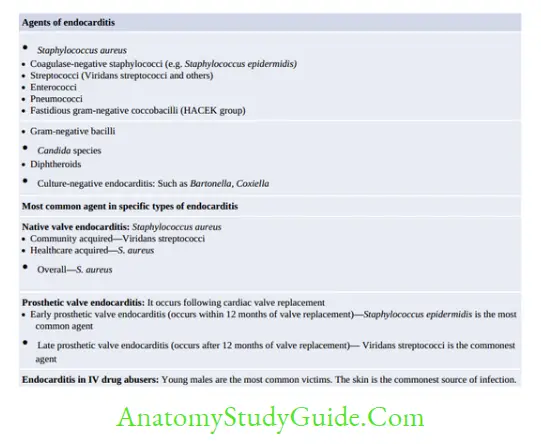
Treatment of infective Endocarditis:
- Empirical treatment consists of vancomycin and gentamicin/ceftriaxone.
- Rifampin may be added to the regimen if prosthetic valve endocarditis is suspected.
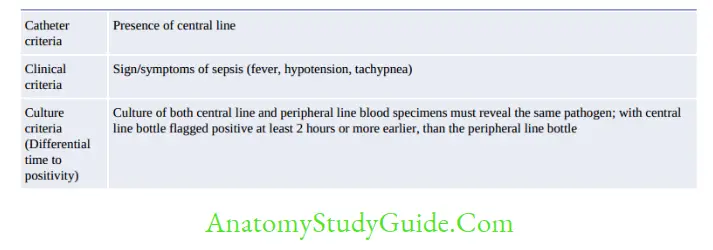
CRBSI (catheter-related bloodstream infection): Severely-ill patients in ICUs are often put on central line; which helps in administration of medication and parenteral nutrition. Central lines may get infected due to mishandling during insertion or during daily maintenance which leads to development of CRBSI.
Extravascular Bloodstream Infections
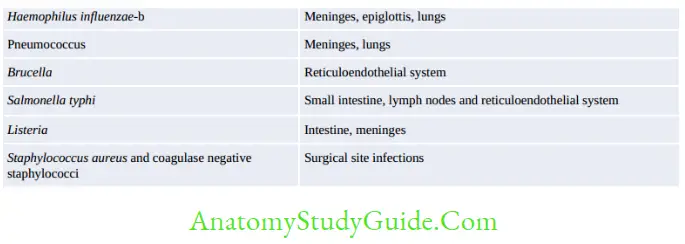
Most cases of clinically significant bacteremia are of extravascular origin.
- The organisms multiply at the primary site such as lungs, and drained by lymphatics and reach the bloodstream
- The organisms are either removed by the cells of the reticuloendothelial system or they multiply more widely and thereby causing septicemia
- Portal of entry: The most common portals of entry for bacteremia are the genitourinary tract (25%), followed by respiratory tract (20%), abscesses (10%), surgical site wound infections (5%), and biliary tract (5%). In up to 25% of cases, the portal of entry remains uncertain
- Agents: The organisms invading the bloodstream.
Treatment of Sepsis/Bloodstream Infection
A de-escalation approach is usually followed which means:
- Empirical treatment consists of higher class of antimicrobials with both gram-negative and gram-positive coverage; e.g. carbapenem such as meropenem plus vancomycin.
- Definitive treatment can be tailored according to the culture sensitivity report.
Fever of Unknown Origin
Petersdorf and Beeson classification (1961) was traditionally used for defining PUO.
- Temperatures of > 38.3°C (>101°F)
- For a duration of > 3 weeks; and
- Failure to reach a diagnosis despite 1 week of inpatient investigation.
This classification has stood for more than 30 years, but later in 1990s, it was revised as Durack and Street classification. As per this classification, FUO has been classified into 4 types: (1)Classic FUO, (2)Nosocomial FUO, (3) Neutropenic FUO and (4) HIV-associated FUO.
Thereafter it is further modified in 2015. According to Harrison 19th edition, FUO is now defined as:
- Fever > 38.3°C (101°F) on at least two occasions
- Illness duration of > 3 weeks
- No known immunocompromised state
- Diagnosis that remains uncertain after a thorough history-taking, physical examination and the obligatory investigations.
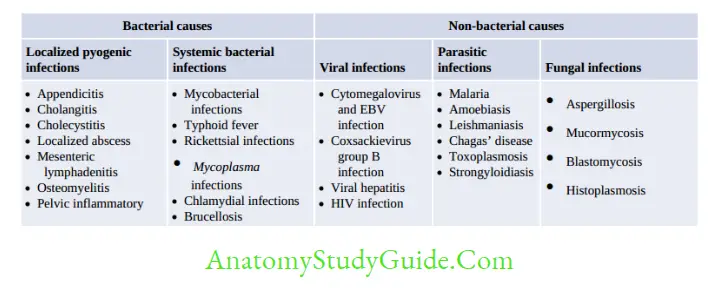
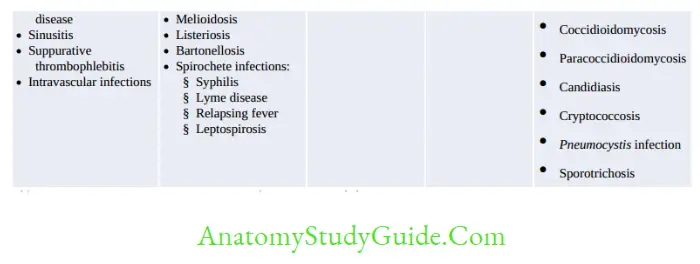
Infections (36%) accounts for majority of FUO cases followed by Neoplasms (19%).
Other Infective Syndromes
Congenital Infection
Vertical transmission (spread of infections from mother-to-baby) may occur by transplacental route (congenital infection), during labor and delivery, or after delivery.
Congenital infection (transmission from placenta to fetus): They often lead to defects in fetal development or even death.
Examples include TORCH syndrome:
- Toxoplasmosis
- Other infections (congenital syphilis, hepatitis B, Coxsackievirus, Epstein-Barr virus,varicellazoster virus, Plasmodium falciparum and human parvovirus)
- Rubella
- Cytomegalovirus (CMV)
- Herpes simplex virus
- Perinatal infections (during labor and delivery): CMV, Gonococcus, Chlamydia, HSV, HPV and Group B streptococci
- Postnatal infections (after delivery): CMV, HIV and Group B streptococcus.
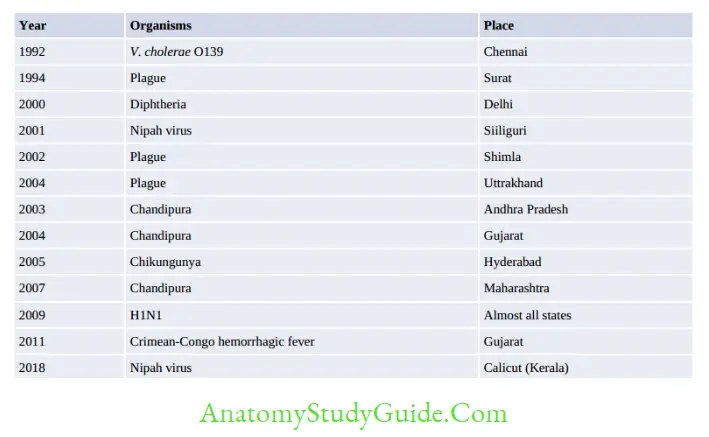
Emerging and Re-Emerging Infection
Emerging infection: Incidence in human increased in last two decades (newly appearing disease or those spreading newly to a geographical area). Example include: - Crimerian congo hemorrhagic virus in India (Ahmedabad- Jan 2011)
- Plasmodium knowlesi
- H1N1 -2009 and Avian flu (H5N1)-2005,
- SARS-2003 (did not affect India)
- HGV, HEV, HHV8, Sin Nombre
Re-emerging infection: Incidence was brought down in past but again increased due to breakdown in public health measure including emergence of drug resistance - India: Plague in Gujrat (1994), Chikungunya (2005), Dengue (North), V.cholerae O139 (south east costal)
- MRSA, MDRTB, Leptospira (South, Andaman)

Microbiological Profile Of Osteomyelitis
- MC cause of osteomyelitis – S. aureus in all sites (hematogenous long-bone and Vertebral and sternal).
- Sickle cell disease-Salmonella osteomyelitis is frequently cause
- IV drug users- P. aeruginosa is common (Harrison 19th/p844)
- Diabetic foot osteomyelitis – Polymicrobial (MC is S. aureus followed by anaerobes and
- Gram-negative like E.coli) (Harrison 19th/p845) Implant-associated osteomyelitis- Coagulase-negative staphylococci (S. epidermidis) are the second most common etiologic agents (after S. aureus). (Harrison 19th/p842)
- Streptococcus agalactiae is common in children next toS. aureus
Leave a Reply