Endodontic Emergencies Definition And Classifiation
The endodontic emergency is defined as any condition leading to an unscheduled visit associated with pain or swelling ensuing from pulpoperiapical pathosis requiring immediate diagnosis and treatment.
Table of Contents
A true emergency is a condition that requires an unscheduled visit with diagnosis and treatment at the same time. However, urgency indicates a less severe problem which can be rescheduled for the next visit.
Read And Learn More: Endodontics Notes
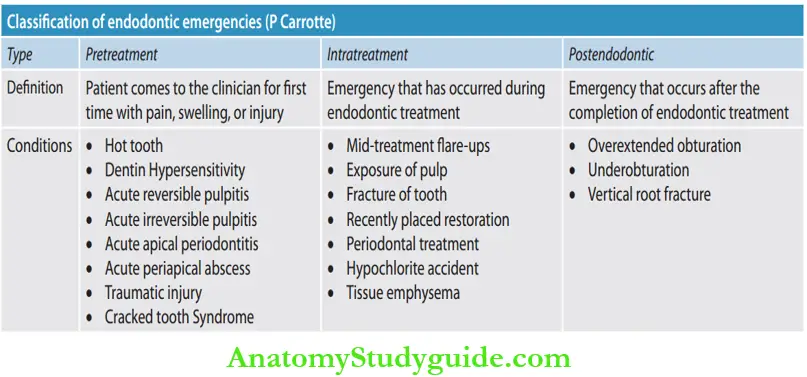
Classifiation of Endodontic Emergencies by P Carrotte:
According to P Carrotte, endodontic emergencies can be classified into three types based on their time of occurrence related to endodontic treatment.
Diagnosis Of Endodontic Emergencies
Complete history of the patient along with clinical examination is the basic step for the successful management of an endodontic emergency. Following steps are taken for accurate diagnosis.
Endodontic Emergencies History of the Patient
The most common component in the chief complaint of emergency patients is pain. Initial questions should help establish two basic components of pain; time (chronicity) and severity (intensity). The patient should be asked, “How painful the tooth is?” “When does it hurt?” “What makes it worse?” etc.
A complete history regarding the pain chronology, i.e. mode, periodicity, frequency and duration, and pain quality, that is, sharp, dull, recurrent stabbing, throbbing should be taken. After the patient has provided complete history regarding his or her problem, both subjective questioning and objective examination are performed carefully
Endodontic Emergencies Subjective Examination:
A patient should be asked questions about the history, location, duration, severity, and aggravating factors of pain. For example, if pain occurs on mastication, when teeth are in occlusion, and is localized in nature, it is periodontal in origin but if thermal stimuli lead to severe explosive pain and the patient is unable to localize, it is pulpal in origin.
Endodontic Emergencies Objective Examination:
In the objective examination, tests are done to reproduce the symptoms that mimic what the patient reports subjectively. For example, if the patient complains of pain to thermal changes and on mastication, the same pain can be reproduced by applying cold and pressure, thus identifying the offending tooth.
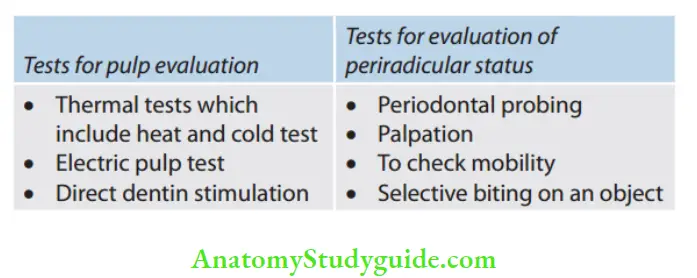
The objective examination includes extraoral examination, intraoral examination, and diagnostic tests for periradicular as well as pulp tissues
Endodontic Emergencies Radiographic Examination:
Good quality intraoral periapical and bitewing radiographs may detect caries, restorations, pulp exposures, root resorption, and periradicular pathologies.
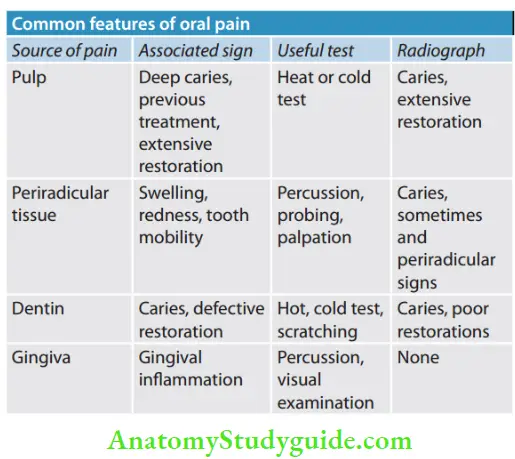
Endodontic Emergencies Diffrential Diagnosis:
After all findings and tests, differential diagnosis should be made.
Pre-Treatment Endodontic Emergencies
Pre-Treatment Endodontic Emergencies Hot Tooth
A hot tooth refers to a painful tooth which requires immediate pain relief at the first appointment. The most common cause of hot tooth is irreversible pulpitis. Since pulpal tissue has a very concentrated sensory nerve supply, particularly in the chamber, it becomes more difficult to anesthetize a hot tooth.
The teeth most difficult to anesthetize are the mandibular molars followed by mandibular and maxillary premolars, maxillary molars, mandibular anterior teeth, and maxillary anterior teeth.
Pre-Treatment Endodontic Emergencies Theories:
- Hyperalgesia: Inflammation within the tooth alters the actual nerve (by changing the resting potentials and decreasing excitability threshold) making it more difficult to anesthetize
- Nervous patient: In nervous or apprehensive patients, the pain threshold further reduces causing difficulty to anaesthetize
- Location: It is assumed that if the area of anesthetic to be administered is away from the target, it becomes difficult to anesthetize. The anesthetic solution may not penetrate to the sensory nerves that innervate the pulp, especially in the mandible
- Local tissue changes because of inflammation: It states that in the area of inflammation, the acidic pH of inflamed tissue decreases the amount of base form of anesthetic available to penetrate the nerve membrane causing anesthetic to be less effctive. But it can be true only in cases of swelling. This theory fails to explain if the injection site is away from the area of inflammation
- Central core theory: It states that nerves outside of the nerve bundle supply molar teeth, whereas nerves on the inside supply anterior teeth, so, the anesthetic solution may not penetrate into nerve trunk to make all nerves numb
- Tetrodotoxin-resistant (TTXr) channels: Special class of sodium channels is present on C-fibers, called TTXr. During inflammation, neuroinflammatory reactions start and sodium channel expression on C-fibers shifts from TTX-sensitive to TTXr causing inflammatory hyperalgesia. These channels have been shown to be five times more resistant to anesthetic than TTX-sensitive channels. Bupivacaine is more potent than lidocaine in blocking TTXr channels and may be the anesthetic of choice when treating the “hot tooth”
Pre-Treatment Endodontic Emergencies Management:
- Explaining patient: The patient should be informed about the treatment so as to avoid the fear of the unknown and reduce anxiety
- Management of anxious patients: It is done by keeping short or no waiting times and use of iatrosedation. Verbal sedation, talking to the patient, music, hypnosis, and relaxation techniques like deep breathing
are helpful
- Management of anxious patients: It is done by keeping short or no waiting times and use of iatrosedation. Verbal sedation, talking to the patient, music, hypnosis, and relaxation techniques like deep breathing
- Role of premedication:
- Prescribe anti-inflammatory to be taken 1 hour before the treatment
- Provide a time gap between the anesthetic injection and starting the procedure. Premedication with lorazepam 1 mg (after checking interaction with other drugs) the night before sleep followed by 90 min prior to the procedure is helpful
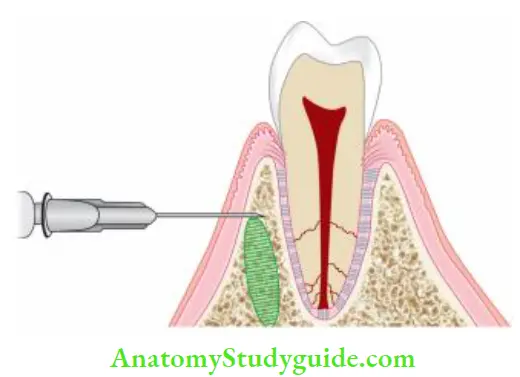
- Additional anesthetic or supplemental injections are necessary to achieve profound anesthesia. Infiltration, supplemental intraligamentary, or intraosseous injections are most helpful along with pulpal anesthesia. Intraosseous injection allows the anesthetic solution to be deposited directly into the cancellous bone around the tooth apices causing better pain relief. Intrapulpal can be painful because here needle is inserted into sensitive and inflamed pulp.

Dentin Hypersensitivity
- Dentin hypersensitivity is defined as “sharp, short pain arising from exposed dentine in response to stimuli typically thermal, chemical, tactile, or osmotic and which cannot be ascribed to any other form of dental defect or pathology”
- The primary underlying cause for dentin hypersensitivity is exposed dentin tubules. Dentin may become exposed by two processes; either by loss of covering periodontal structures (gingival recession) or by loss of enamel.
- Two main principal treatment options are plugging the dentinal tubules to prevent the fluid flow and desensitizing the nerve, making it less responsive to stimulation

Acute Reversible Pulpitis:
Acute reversible pulpitis is characterized by the following features:
- Localized inflammation of the pulp
- Lowering of threshold stimulation for Aδ nerve fiers
- Exaggerated, non lingering response to stimuli
Acute Reversible Pulpitis Management:
- Removal of the cause; in case of deep caries, excavate the place restoration.
- Recontouring of recently placed restoration which causes pain
- Removal of restoration and replacing it with sedative dressing if painful symptoms still persist following tooth preparation
Acute Irreversible Pulpitis:
If the inflammatory process progresses, irreversible pulpitis can develop. It is characterized by
- History of spontaneous pain and exaggerated response to hot or cold that lingers even after removal of stimulus
- Extensive restoration or caries involving the pulp
- The tooth may be responsive to electrical and thermal tests
Acute Irreversible Pulpitis Management:
- Anesthetize the affected tooth and apply a rubber dam
- Prepare the access cavity and extirpate the pulp
- Thorough irrigation and debridement of the pulp chamber
- Determine the working length
- Extirpate the pulp followed by cleaning and shaping of the root canal
- Through irrigation of the root canal system
- Drying of the root canal with sterile absorbent points
- Placement of a dry cotton pellet or pellet moistened with CMCP, formoterol, or eugenol in the pulp chamber and sealing it with the temporary restoration
- Relief of the occlusion
- Appropriate analgesics therapy and antibiotics, if needed
Acute Apical Periodontitis:
It is an inflammation of the periodontal ligament caused by tissue damage usually from occlusal trauma or extension of pulpal pathology. Pressure on a tooth is transmitted to the fluid which pushes on nerve endings in the periodontal ligament. It is characterized by:
- The tooth may be elevated out of its socket because of the increase in fluid pressure in the periodontal ligament
- Discomfort on biting or chewing
- Sensitivity to percussion (hallmark diagnostic test)
Acute Apical Periodontitis Management
- For vital teeth:
Symptomatic treatment and occlusal adjustment if required. - For nonvital teeth
- Anesthetize the involved tooth and prepare the access Cavity
- Extirpate the pulp and determine the working length
- Complete the cleaning and shaping of the root canal and copiously irrigate
- Place sedative dressing and give temporary restoration
- Relieve the occlusion if indicated
- Prescribe analgesics to reduce the pain
Acute Periapical Abscess:
An acute periapical abscess is a severe inflammatory response to microorganisms or their irritants that have been leached into periradicular tissues.
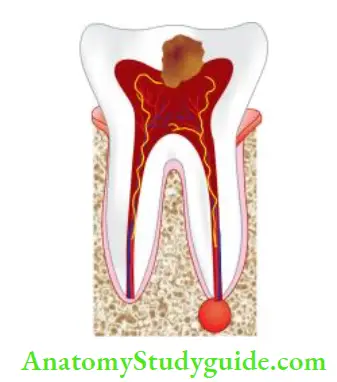
Acute Periapical Abscess is characterized by the following features:
- Swelling along with pain and a feeling that the tooth is elevated in the socket
- May not have radiographic evidence of bone destruction because flids rapidly spread away from the tooth
- Systemic features such as fever and malaise may be present
- Mobility may or may not be present
Acute Periapical Abscess Management
- Biphasic treatment:
- Pulp debridement
- Incision and drainage
- Do not leave the tooth open between appointments
- In case of localized infections, antibiotics provide no additional benefit
- In case of systemic features, antibiotics should be given
- Relieve the tooth out of occlusion in cases of hyper occlusion
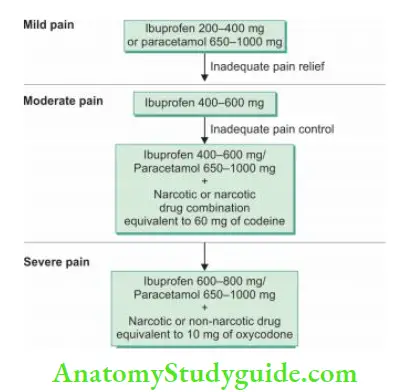
- To control postoperative pain, NSAIDs should be prescribed
- Speed of recovery will rely on canal debridement
LA (Local anesthetics) is contraindicated in periapical abscess cases because of the following reasons:
- Pain caused by injection in the distended area
- Chances of dissemination of virulent organisms
- Ineffectiveness of local anesthetics
Traumatic Injury:
The main objective of the treatment should be immediate relief of pain. Patients with traumatic injury may present; luxation injury, fracture of crown or root, or avulsion of the tooth.
- In case of luxation injury, the main aim is to relieve the pain and reposition the dislocated tooth.
- In case of a fracture of the root or crown, check the prognosis of the fracture and give treatment accordingly.
- Avulsion of the tooth means the complete and total displacement of the tooth out of the socket.
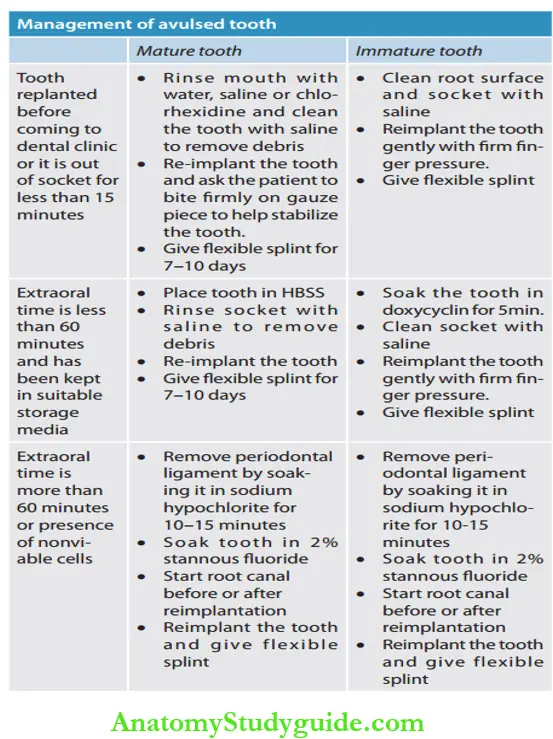
The main aim of reimplantation is to preserve a maximum number of periodontal ligament cells and prevent them from drying since drying can result in loss of their normal physiology and morphology.
Among various storage media available, the order of efficacy is ViaSpan=HBSS>coconut water>milk>green tea>egg white. Water is the least desirable.
Management Options for an Avulsed Tooth:
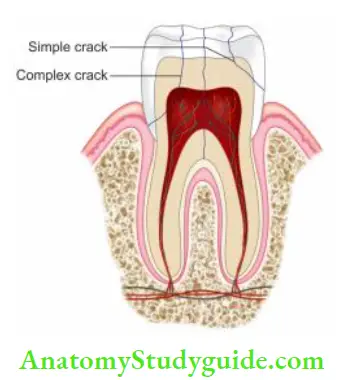
Cracked Tooth Syndrome
- A fracture plane of unknown extent and direction passing through tooth structure may involve pulp and/ or periodontal ligament resulting in cracked tooth syndrome.
- It is commonly seen in teeth with large and complex restorations
- A crack tooth can be diagnosed after taking the case history of the patient which includes detailed history regarding dietary and parafunctional habits and any previous trauma
- During tactile examination, pass the tip of the sharp explorer gently on the tooth surface, so as to locate the crack bycatch
- The patient can be asked to bite on an orangewood stick, rubber wheel, or tooth slooth. Pain during biting, especially upon release of pressure is a classic sign of cracked tooth syndrome
Cracked Tooth Syndrome Treatment:
Urgent care involves immediate reduction of its occlusal contacts by selective grinding of the tooth or its antagonist.
Definitive Treatment;
- Definitive treatment of the cracked tooth aims to preserve the pulpal vitality by providing full occlusal coverage for cusp protection
- Full coverage crown if the fracture involves crown portion only
- If the fracture involves pulp and is superficial to the alveolar crest, go for endodontic treatment and restoration of the tooth
- If a fracture of the root extends below the alveolar crest, extract the tooth
Intratreatment Emergencies
Mid-Treatment Flare-ups:
To summarize, the etiology of mid-treatment flare-ups:
- Overinstrumentation
- Inadequate debridement
- Missed canal
- Hyperocclusion
- Debris extrusion
- Procedural complications
Risk Factors Contributing to Interappointment Flare-Ups:
- Preoperative pain, percussion, sensitivity, and swelling
- Retreatment
- Apprehension
- History of allergies
Prevention:
- Psychological preparation of the patient
- Long-acting anesthetics such as bupivacaine should be preferred
- Complete cleaning and shaping of the root canal
- Analgesics should be prescribed for the relief of pain
Risk Factors Contributing to Interappointment Flare-Ups Treatment:
- Reassure patients
- Adjust occlusion
- Complete debridement along with cleaning and shaping of the root canal system
- Prescribe analgesics
- Never leave the tooth open for drainage
- Recall the patient until the painful symptoms subside
Exposure of Pulp:
Pulp exposure during tooth preparation can result in severe sharp pain. In these cases, pain can be relieved by complete extirpation of the pulp.
Fracture of Tooth:
Fractures of the tooth can occur during endodontic treatment. It can result in pain due to contamination of the root canal. If the fracture is vertical extending apical to the alveolar crest, one should go for extraction of the tooth; or in the case of the multirooted tooth, one should go for redirection or hemisection.
Recently Placed Restoration:
A recently placed restoration may present pain because of many factors like high restoration, microleakage, inadequate pulp protection, galvanism due to dissimilar metal restoration, or chemical irritation from restorative materials or micro exposure of the pulp.
Periodontal Treatment:
Periodontal treatment can result in exposure of the lateral canal which can communicate with periodontal ligament space and cause pain.
Hypochlorite Accident:
Hypochlorite accident occurs when sodium hypochlorite gets extruded beyond the tooth apex. It manifests a combination of symptoms like severe pain, swelling, and profuse bleeding both through the tooth and interstitial tissues.
Etiology:
It can result due to forceful injection of hypochlorite, irrigation of tooth with wide apical foramen, immature apex, or apical resorption.
Hypochlorite Accident Clinical Features:
Edema, ecchymosis along with tissue necrosis, paresthesia, and secondary injection are commonly seen after a hypochlorite accident. Most patients recover within 7–10 days, but scarring and paresthesia may take a long time to heal.
Hypochlorite Accident Management:
- Immediate aspiration and application of icepacks
- Since infection because of tissue destruction can spread, prescribe antibiotics, analgesics, and antihistaminics
- In severe cases, steroids and hospitalization for surgical wound debridement is also indicated
- Home care instructions are given to patients like cold compresses to minimize pain and swelling followed by warm compresses (after 24 h) to encourage healing
Hypochlorite Accident Prevention:
- Use needles with closed-end and lateral vents
- The tip of the needle should be 1–2 mm short of the apex
- Never bind the needle in the canal, it should allow back flow of the irrigant
- Oscillate the needle in the canal
- Do not force the irrigant into the canal
Hypochlorite Accident Tissue Emphysema:
It is defined as a collection of gas or air in the tissue spaces or facial planes.
Hypochlorite Accident Etiology:
- During periapical surgery when air from the air rotor is directed toward the exposed soft tissues
- When the blast of air is directed toward open root canals to dry them
- As a complication of fracture involving the facial skeleton.
Tissue Emphysema Clinical Features:
- Development of rapid swelling, erythema, and crepitus (crepitus is pathognomonic of tissue emphysema)
- Dysphagia and dyspnea, and if emphysema spreads into the neck region, it can cause difficulty in breathing and its progression to the mediastinum.
Hypochlorite Accident Diffrential Diagnosis:
- Angioedema
- Internal hemorrhage
- Anaphylaxis.
Tissue Emphysema Treatment:
- Antibiotics to prevent risk and spread of infection
- Application of moist heat to decrease swelling
- If the airway or mediastinum is obstructed, immediate medical attention and hospitalization of the patient.
Tissue Emphysema Prevention:
- While using air pressure, a blast of air should be directed at horizontal direction against the walls of the tooth and not periodically
- During surgical procedures, use low-speed or highspeed impact handpieces which do not direct air toward tissues.
Postendodontic Emergencies
Following the completion of endodontic treatment, patients usually complain of pain, especially on chewing. The incidence of pain after obturation is small and a number of visits does not make much difference. Chances of experiencing postoperative discomfort increase if the pain is present preoperatively.
Painful episodes are caused by pressure exerted by the insertion of root canal filling materials or by chemical irritation from ingredients of root canal cement and pastes.
Factors responsible for postobturation pain
Overextended Obturation:
It leads to pain. Periapical inflammation results in the firing of proprioceptive nerve fiers in the periodontal ligament. These results are short-lived and abate in 24–48 hours. No treatment is usually necessary in these cases.
Under Obturation:
Under obturation may result from incomplete cleaning and shaping of the root canal which may cause pain. It may be due to the presence of viable pulp tissue left in the canal and the failure of the resolution of inflammation. In such cases, retreatment is indicated.
Persistent Pain:
Persistent pain or sensitivity for longer periods may indicate failure of resolution of inflammation. In rare cases, inflamed but viable pulp tissue may be left in the root canal in such cases, retreatment is indicated.
Vertical Root Fracture:
Vertical fracture of crown and/or root can occur:
- During obturation due to wedging forces of the spreader or plugger
- During postplacement in structurally weakened endodontically treated tooth
- Due to fracture of coronal restoration because of lack of ferrule effect on remaining root structure.
- Diagnosis: Periodontal probing may reveal a single isolated narrow pocket adjacent to the fracture site. Radiograph may show lateral diffuse widening of the periodontal ligament. Surgical exposure of the tooth may reveal vertical root fracture (VRF).
- Management: The prognosis of VRF is poor and the tooth generally undergoes extraction.
High Restoration:
It is managed by selective occlusal grinding.
Management of Postobturation Emergencies
Most of the time, there is some discomfort following obturation which subsides in 2–5 days. To manage postobturation endodontic emergencies, the following can be done:
- Reassure the patient
- Prescribe analgesics
- Check occlusion
- Do not retreat randomly. Retreatment is done only in cases of persistent untreatable problems.
Endodontic Emergencies Conclusion
One of the greatest challenges in clinical dentistry is managing endodontic emergencies. One should diagnose the emergency and manage it efficiently and under profound pulpal anesthesia.
Reassurance of the patient is the first and foremost step in the treatment of an endodontic emergency to control the patient’s anxiety and overreaction. Sometimes the patient reports severe pain but there is no evidence of acute apical abscess and the root canal treatment has been done properly.
These patients are treated with reassurance and analgesics, again the symptoms subside spontaneously. But if an apical abscess develops with inadequate root canal treatment, apical surgery may be needed.
Leave a Reply