Evolution of Techniques in Recording Posterior Palatal Seal
Define PPS. Describe various methods to record apps and their advantages and disadvantages.
Answer:
Posterior palatal seal (PPs) is defined as, “The soft tissues along the junction of the hard and soft palates on which pressure within the physiologic limits of the tissues can be applied by a denture to aid in the retention of the denture.” (GPT)
Posterior Palatal Seal
Factors Important In Recording PPS
- 1 to 2 mm distal to the expected denture border should be present in the impression tray
- Determine the type of soft palate classification.
- The “post-dam” should be located by the dentist.
Read And Learn More: Complete Dentures Question and Answers
Techniques To Record PPS
Marc Appelbaum (1979) reported the different techniques:
- Conventional Approach by Hardy and Kapur 1958
- Fluid Wax Technique Nelson 1970
- Arbitrary Scraping of Master Cast by Boucher
- Adding a Posterior Palatal Seal to an Existing Denture by Moghadam and Scandrett 1974
- Extended palate technique by Silverman 1971
- A semi-physiologic method by Calamini.
Techniques To Record PPS Conventional Approach
- An accurate and fully extended final impression on which shellac or resin tray is made.
- Ask the patient to rinse with an astringent mouthwash and dry the PPS region.
- Locate the hamular processes with (a “T” burnisher or mouth mirror) and mark with an indelible pencil.
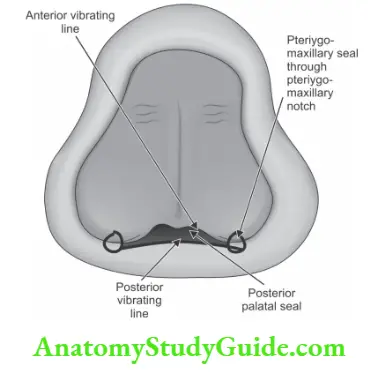
- Locate the pterygomaxillary notch and mark the notch and extend 3 to 4 mm anterolateral to the tuberosity, approximating the mucogingival junction. Repeat on the opposite side and the outlining of the pterygomaxillary seal is complete.
- The patient is asked to say “ah” in short bursts meanwhile observe the movement of the soft palate between shallow displacement and marked muscular activity, the posterior vibrating line is marked with an indelible pencil.
- Connect the posterior vibrating line through the pterygomaxillary seal and ask the patient to keep the mouth open. The resin or shellac tray is then inserted and seated firmly in the mouth and the lines marked should have been transferred to the tray.
- The tray is then returned to the master cast to complete the transfer of the posterior border.
- Locating the anterior vibrating line with the “T” burnisher. It is the compressible tissue anterior to the Posterior vibrating line.
- The use of the Valsalva maneuver or visualizing the area while the patient says “ah” with short vigorous bursts may also be used. This line is marked with an indelible pencil and transferred to the master cast.
- The visual outline is in the shape of Cupid’s bow. The area between the anterior and posterior vibrating lines is usually narrowest in the midpalatal region because of the projection of the posterior nasal spine.
- A Kingsley scraper is then used to score the cast. The deepest areas of the seal are located on either side of the midline, one-third the distance anteriorly from the posterior vibrating line, and it is scraped to a depth of approximately 1 to 1. 5 mm.
- The median palatal raphe has little submucosa and hence, this area is scraped to a depth of approximately 0. 5 to 1. 0 mm only.
- As the seal approaches the anterior vibrating line there is just a slight scraping of the cast. The posterior to the deepest portion of the seal is also tapered to the posterior vibrating line. If the seal is not tapered it may lead to tissue irritation.
- If a shellac tray is used, moisten the cast and readapt shellac to the scored cast, and check the retention in the mouth by asking the patient to say “ah” in a short, unexaggerated manner. If no space is noted between the trial base and the soft palate then an adequate posterior seal has been created.
- If a resin tray is used, add small amounts of autopolymerizing resin until a good seal is achieved. Use a separating medium.
Techniques To Record PPS Advantages of the Conventional Method
- As the trial base has good retention, the recording of jaw relation is accurate.
- Patients will be ensured of a good retentive complete denture prosthesis as they are able to experience the retentive qualities of the trial base.
- The practitioner will be able to assess the retentive qualities of the finished denture.
- The new denture wearer will be able to realize the posterior extent of the denture.
Techniques To Record PPS Disadvantages of the Conventional Approach
- Not a physiologic technique and hence depends upon accurate transfer of the vibrating lines and careful scraping of the cast.
- Potential for over-compression of the tissues.
Techniques To Record PPS Fluid Wax Technique
- After the transfer markings are copied onto the final impression as (Zinc oxide eugenol or plaster) the same method as the Conventional technique.
- Any one of four types of wax can be used (Iowa wax, white, developed by Dr. Earl S Smith; Korecta wax No. 4, orange, developed by Dr. OC Applegate; H-L physiologic paste, yellow-white, developed by Dr. CS Harkins; or Adaptol, green, developed by Nathan G. Kaye).
- These waxes are designed to flow at mouth temperature and are painted onto the impression surface within the outline of the seal area after melting.
- The impression is carried to the mouth and held in place under gentle pressure for four to six minutes to allow time for the material to flow.
- A 30° flexion of the head and the tongue is firmly positioned against the mandibular anterior teeth (handle). The patient is asked to periodically rotate the head so that all functional positions of the soft palate are recorded.
- If the tissue has been contacted, the wax will have a glossy appearance. Wherever it appears dull more wax should be added and the procedure repeated.
- The secondary impression is reinserted and held for three to five minutes under gentle pressure, followed by two to three minutes of firm pressure applied to the mid-palatal area of the impression tray. During this time, the head and tongue positions must be maintained.
Techniques To Record PPS Advantages
- It is a physiologic technique displacing tissues within their physiologically acceptable limits.
- Over-compression of tissues is avoided.
- The posterior palatal seal is incorporated into the trial denture base for added retention.
- Mechanical scraping of the cast is avoided.
Techniques To Record PPS Disadvantages
- More time is necessary during the impression appointment.
- Difficulty in handling the materials and added care during the boxing procedure.
Arbitrary Scraping Of Master Cast
This technique is the least accurate as it relies on the dentist’s recollection of the palatal configuration and tissue compressibility to locate the anterior and posterior vibrating lines and the depth to which the cast should be scraped.
Arbitrary Scraping Of Master Cast Disadvantages
1. Underextension
- As a result of the practitioner’s use of the fovea palatine as the landmark for terminating the denture base deprives 4 to 12 mm of tissue coverage, which can improve the retention of the denture.
- If the hard and soft palates and the accurate marking of the vibrating lines are not carried out, the proper posterior border extension cannot be determined.
- When the laboratory technician is asked to trim and polish the processed denture borders.
2. Underpostdamming
- When the mouth is in the wide-open position, the pterygomandibular fold becomes taut. When the patient assumes any position other than a wide-open position, a space will be present between the denture base and the tissue, since the fold is no longer activated.
- The diagnosis of this condition consists of placing the wet denture base into the mouth and slowly pressing in the midpalate region until it is firmly seated, all the while observing the distal denture border.
- If air bubbles can be seen escaping from beneath the distal border, then at that point the denture base is underpostdammed.
3. Overpostdamming
If excessively overpostdammed upon denture insertion the posterior border will be displaced inferiorly. If it is moderately overpostdammed, tissue irritation will be seen across the posterior palatal region.
4. Overextension
- If over-extended the patient complains that swallowing is painful and difficult. Small ulcerated areas in the region of the soft palate will be seen. Mark these lesions and transfer them to the denture base, the precise position of the overextension can be removed with a bur and then carefully repolished.
- If the denture base covers the hamuli, the patient will experience sharp pain, especially during function.
Posterior Palatal Seal
Adding A Posterior Palatal Seal To An Existing Denture
Only if the existing prosthesis has correct esthetic, phonetic requirements, proper vertical dimension, and centric relation positions with proper denture border extensions then only correction of the posterior seal area is done. If not a new prosthesis is the option.
Arbitrary Scraping Of Master Cast Techniques
- Fluid wax technique.
- Softened green stick modeling compound.
- A combination of fluid wax and green stick compound.
- Using the Light cured resin.

Arbitrary Scraping Of Master Cast Fluid Wax Technique
- Moghadam and Scandrett suggested this procedure. All of the steps outlined for locating, marking, and placing the wax in the seal area are the same except that the wax is placed on the processed denture base.
- After the wax has flown adequately, the denture is removed from the mouth and the anterior extent of the seal is marked on the denture.
- Utility wax is placed vertically across the palate, separating the posterior two-thirds from the anterior region and extending around the posterior portion of the denture.
- The dental stone is vibrated into the denture-wax surface outlined by the utility wax. After the stone has set, the wax is eliminated, the denture cleaned and the area distal to the anterior vibrating line is ground.
- After applying lubricant to the unground areas, including the polished surface, and a separating medium is applied to the stone cast, a denture is replaced on the stone cast and held firmly with rubber bands.
- Acrylic is added till the space between the denture and cast is filled. After waiting till the initial set has taken place it is placed in a pressure pot with water (140°F) for 20 minutes under 30 psi pressure.
- The cast and denture are separated, the excess acrylic is trimmed and the border is polished lightly. The above procedures can be done using green stick compound (by Carroll and Shaffer) and a combination of both (by Lauciello and Conte) and Light cured resin instead of Fluid wax alone.
- Light-cured resin allows for accurate placement of the seal by adding material selectively, similar to the fluid wax technique, curing it in stages. The curing procedure requires the use of high-intensity white light.
Posterior Palatal Seal
Arbitrary Scraping Of Master Cast Advantages
- No exothermic reaction irritates the oral tissues
- Minimal volumetric shrinkage during curing
- More closely approximates a physiologic technique
- Can be performed with relatively little chair time.
The only disadvantage is the cost of the curing unit.
Leave a Reply