Hirschsprungs Disease Congenital Megacolon
Hirschsprung’s disease: Hirschsprung’s disease is also called congenital megacolon, aganglionic megacolon or primary megacolon. It is one of the common causes of neonatal intestinal obstruction.
Table of Contents
Hirschsprung’s disease Pathophysiology
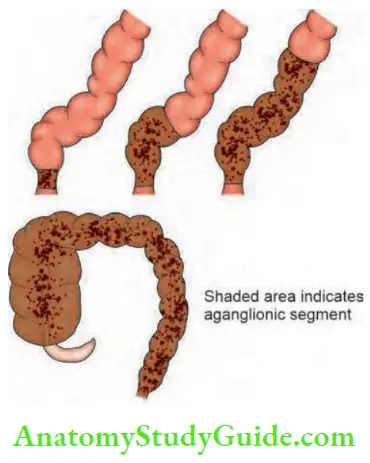
- The disease always involves the anus and rectum wherein parasympathetic ganglion cells are absent in the neural plexus of the intestinal wall. The defect involves internal sphincter.
- As a result of this, there is a terminally constricted, non-relaxing segment, in the rectum and sigmoid (lower part), above which the pelvic colon (sigmoid) is enormously dilated. Rectosigmoid area is involved in 80% of cases.
- Circular muscle hypertrophy, mucosal hyperaemia and ulcers are present in the dilated segments.
- In between, there may be a transition zone (cone), which contains a few parasympathetic ganglion cells.
- Rarely, Hirschsprung’s can also involve the entire sigmoid colon or even the entire colon.
- Hirschsprung’s rarely occurs in adults also.

Hirschsprung’s Disease Types
- Ultrashort segment: Anal canal and terminal rectum are aganglionic.
- Short segment: Anal canal and entire rectum is completely involved.
- Long segment: Anal canal, rectum and part of colon involved.
- Total colonic: Anal canal, rectum and the whole length of the colon is involved.
Hirschsprung’s Disease Treatment or Clinical Features:
Male children are commonly affected when compared to females.
Incidence: 1 in 4000 to 5000 live births.
- The child presents with acute neonatal intestinal obstruction as manifested by failure to pass meconium or delay in passing meconium with abdominal distension.
- Within 12–24 hours, all features of intestinal obstruction can be found. If it is complicated by enterocolitis, it may result in perforation and septicaemia.
- A severe diarrhoea with blood and mucus, abdominal distension and vomiting can occur within a few hours, followed by hypovolaemic shock.
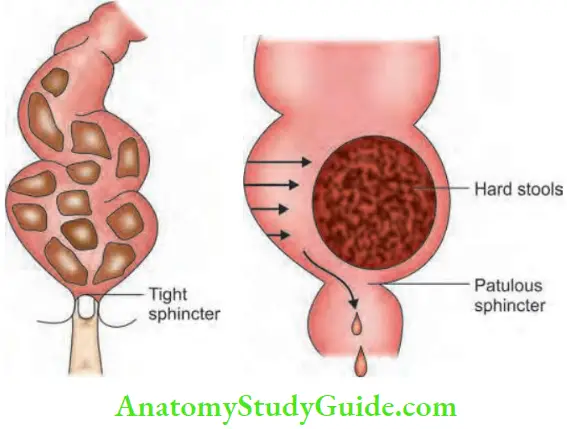
- Rectal examination reveals that the rectum is empty, finger is gripped by anal sphincter and there is no perianal soiling. On the other hand, in acquired megacolon, the rectum is loaded with faecal matter, perianal soiling is present and there is no sphincter activity
- Chronic variety: Chronic constipation manifests in the first few weeks of life. The child may be brought with abdominal distension. Stools are goat pellet-like
Hirschsprung’s Disease Differential Diagnosis
Acquired megacolon: Usually manifests by one to two years of age. The rectum is loaded with faecal matter.
Differential Diagnosis:
- Hypothyroidism
- Meconium plug syndrome
- Intestinal pseudo-obstruction
- Colonic neuronal dysplasia
Hirschsprung’s disease Complications
- Intestinal obstruction, perforation, peritonitis
- Enterocolitis
- Growth retardation
Hirschsprung’s disease Investigations:
- Full-thickness rectal wall biopsy: Under GA there is an absence of parasympathetic ganglion cells and hypertrophic nerve fibres in the nerve plexus. It should be taken above the anorectal junction. Today submucosal suction biopsy is more popular than biopsy since it avoids haemorrhage, infection and scarring.
- Barium enema: 3.6% solution of barium is used, the intermediate zone appears as a cone with proximal dilatation and a distal narrow zone which is characteristic of Hirschsprung’s disease.
Hirschsprung’s disease Treatment
- Emergency Cases:
- Right transverse loop colostomy: In most of cases, the aganglionic segment is limited to the rectosigmoid region.
- A full thickness biopsy of the colostomy is sent for histopathological examination.
- Definitive Surgery:
- Can be done usually between the age of 3 and 6 months (8 to 10 kg of weight).
- Resection of aganglionic bowel (anorectum) followed by a pull-through procedure. Maintaining continence is the main aim.
- A few points of comparison between ‘Duhamel’s and Swenson’s pull-through’ are mentioned below.
Duhamel’s:
- Retrorectal pull- Through
- Technically easy
Swenson’s:
- Endorectal pull – Through
- Difficult
Steps of Duhamel’s Pull-through Surgery
- The rectum is transected above the peritoneal fold and is closed.
- The proximal ganglionic segment is pulled down behind the rectum (retrorectal space created by using blunt dissector).
- An incision is made in the posterior wall of the anorectal above the dentate line and is deepened through the entire bowel wall.
- The end of the proximal colon is sutured to the opening in the posterior anal canal all around.
- The adjacent walls of the rectum (posterior wall) and colon (anterior wall) are crushed by using a Kocher’s forcep which falls off by itself by the 14th day.
- The open end of the rectum (above) is closed end to side to the colon.
- Other types of surgery: Soave’s mucosectomy and pull-through operation.
Pseudointestinal Obstruction
Acute colonic pseudo-obstruction (ACPO) is also called Ogilvie’s syndrome. It is massive colonic distension in the absence of a mechanically obstructing lesion.
Pseudo-obstruction Pathogenesis
- It occurs mainly due to malfunctioning of sacral parasympathetic nerves (S2–S4). It results in atony of the descending colon resulting in functional obstruction.
- It is interesting to note that the junction of the dilated and collapsed bowel is near the splenic flexure.
- This is the place wherein parasympathetic supply by the vagus ends and sacral autonomic nervous system starts. An increased sympathetic tone results in colonic dilatation due to inhibition of contraction.
Pseudo-obstruction Clinical Features
- Elderly bedridden patients with cardiac/lower respiratory illness are the victims.
- Aerophagia and drugs which decrease colonic mobility are precipitating factors.
- Failure to pass faeces and flatus for several days.
- Tachypnoea due to elevation of the diaphragm due to distended colon is common.
- Rectal examination reveals some faeces (in cases of mechanical obstruction, the rectum is empty).
- Plain X-ray abdomen erect may or may not show one or two air fluid levels. Distension is mainly colonic.
- Carcinoma colon is to be differentiated by barium enema.
- Caecal perforation is a dangerous complication.
- Hence, look for right iliac fossa tenderness.
Pseudo-obstruction Causes
1. Retroperitoneal irritation:
- Blood
- Urine
- Fracture spine and pelvis
2. Drugs:
- Levodopa
- Tricyclic antidepressants
3. Metabolic:
- Uraemia
- Diabetes
- Myxoedema
- Hypokalaemia
4. Viral infections
Pseudo-obstruction Treatment
- It is conservative, provided acute abdomen is ruled out.
- Colonoscopic decompression is the method of choice.
- Prokinetic drugs such as cisapride or mosapride have been tried in selected cases.
- Rarely, even after colonoscopic decompression, caecal tenderness continues. If distension persists, laparotomy followed by tube caecostomy may have to be done.
Leave a Reply