History And Examination Of Traumatic Injuries
A history of the injury followed by a thorough examination should be completed in any traumatic injury.
Table of Contents
Dental History
The patient should be asked for pain and other symptoms and listed in order of importance to the patient.
- When did the injury occur?: Time interval between injury and treatment affects the prognosis of injuries like avulsions, crown fractures (complicated or uncomplicated), and dentoalveolar fractures
- Where did the injury occur?: This indicates the need for tetanus prophylaxis
- How did the injury occur?: Nature of trauma can suggest the type of injury expected
- Are there any lost teeth/fragments?: If there is loss of a tooth or fractured piece with a history of loss of consciousness, a chest radiograph should be taken to exclude inhalation
- Previous dental history: Previous trauma can affect pulpal vitality tests and the repair ability of the pulp. It can also affect the attitude of the patient toward the choice of treatment
Read And Learn More: Endodontics Notes
Medical History
The patient should be asked for
- Allergic reaction to medication
- Disorders like bleeding problems, diabetes, epilepsy, etc.
- Any current medication patient is taking
- Condition of tetanus immunization—In case of a contaminated wound, a booster dose should be given if more than 5 years have elapsed since the last dose. But for clean wounds, no booster dose is needed, if the time elapsed between the last dose is less than 10 years
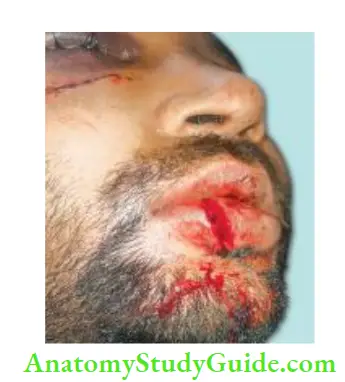
Extraoral Examination
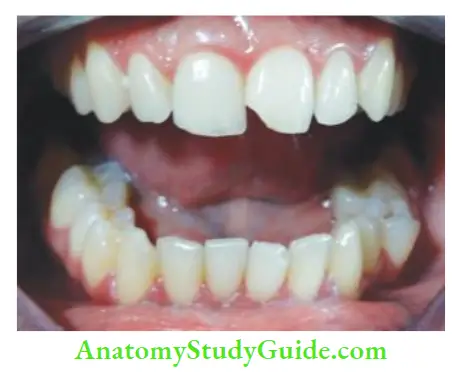
If a severe injury is seen, one should look for signs of shock (pallor, hypotension, and irregular pulse). One should check for facial swelling, discoloration, or lacerations which may suggest injury to underlying bone and multiple tooth injury. Limited or deviated mandibular movements indicate jaw fracture or dislocation.
Intraoral Examination
A thorough systematic intraoral examination should be carried out.
- Laceration, hemorrhage, and swelling of the gingiva should be examined for tooth fragments, etc.
- Look for abnormalities in occlusion, fractured crowns, or displacement of teeth
- Color of the tooth should be noted as it shows the vitality of the pulp
- Reaction to percussion should be compared with a contralateral normal tooth (a dull sound indicates root fracture)
- Mobility should be tested in a horizontal and vertical direction. If multiple teeth move together, one should suspect a fracture of the alveolar process.
- In case of excessive mobility, one should consider root fracture or tooth displacement
- Pulp vitality tests: Vitality tests should be performed at the time of initial examination and recorded to establish a baseline for comparison with subsequent repeated tests in the future. One should not assume that teeth which give a positive response at the initial examination will continue to give a positive response and vice versa.
- A tooth with a positive response may show necrosis and a negative response may not necessarily indicate a nonvital pulp. A negative response is due to a “shock-wave” effect which damages the apical nerve supply.
- The pulp may take as long as 9 months for normal blood flow to return to the coronal pulp of the traumatized tooth.

Radiographic Examination
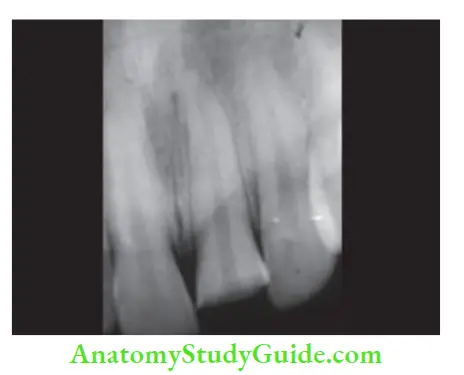
An occlusal exposure of the anterior region may show lateral luxation, root fracture, or discrepancy in the alveolar region. Periapical radiographs can assess crown and root fracture
Three angulations recommended by the International Association of Dental Traumatology (IADT) are
- Occlusal view
- Lateral view from the mesial or distal aspect of the tooth
- 90° horizontal angle with a central beam through the tooth.
Clinical Photographs
Clinical photographs are helpful for establishing clinical records and monitoring treatment progress. They also help as additional means of documenting injuries for legal purposes and insurance.
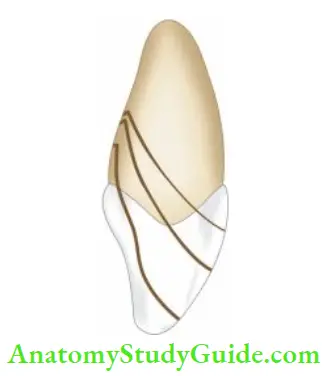
Crown Infraction
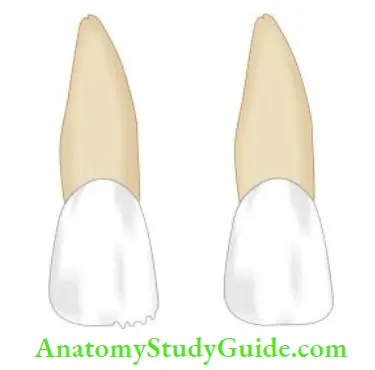
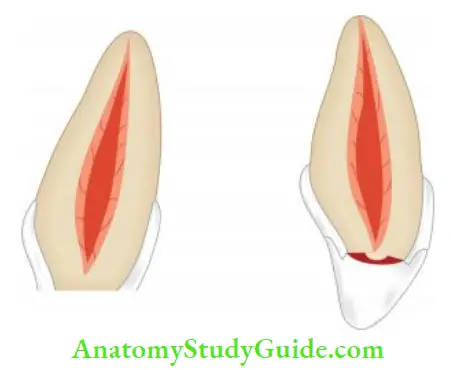
A crown infraction is an incomplete fracture of enamel without loss of tooth structure. This type of injury is very common but often unnoticed. It results from a traumatic impact to enamel and appears as a craze line running parallel with the direction of enamel rods and ending at the dentin enamel junction.
Crown Infraction – Biological Consequences
- Fracture lines are the weak points through which bacteria and their products can travel to the pulp
- The crown infraction can occur alone or can be a sign of a concomitant attachment injury where force taken up by attachment injury leaves enough force to crack the enamel.
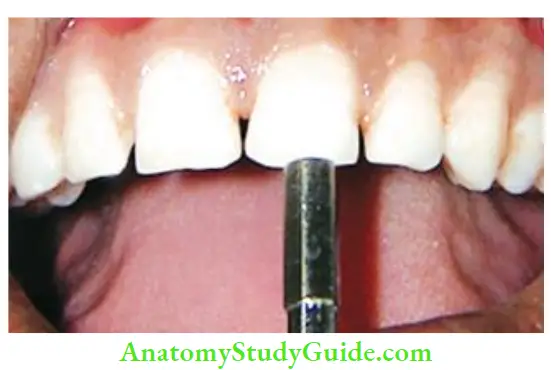
Crown Infraction Diagnosis
- Tooth-sustaining fracture is usually vital
- Easily recognized by viewing the long axis of a tooth from the incisal edge
- Examined by exposing it to the fiery optic light source, resin curing light, indirect light, or by transillumination.
Crown Infraction Treatment
Infracted tooth does not require treatment but vitality tests are necessary to determine the extent of pulp damage.
- Smoothening of rough edges by selectively grinding of enamel
- Repairing fractured tooth surface by composite if needed for cosmetic purposes
- Regular pulp testing should be done and recorded for future reference
- Follow-up of patient at 3, 6, and 12 months interval is done

Prognosis
Prognosis is good for infraction cases.
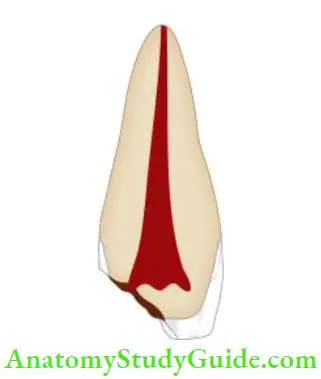
Uncomplicated Crown Fracture
A crown fracture involving enamel and dentin but not pulp is called an uncomplicated crown fracture. It occurs more frequently than the complicated crown fracture. This type of fracture is usually not associated with pain and it does not require urgent care.

Incidence
It accounts 26–92% of all traumatic injuries of teeth.
Biological Consequences
Minimal consequences are seen if only enamel is fractured but if dentin is exposed, a direct pathway for various irritants to pass through dentinal tubules to underlying pulp is formed
The pulp may remain normal or get chronically inflamed depending upon the proximity of the fracture to the pulp, the size of dentinal tubules, and time of the treatment provided
Diagnosis
If dentin is exposed, sensitivity to thermal changes is seen.
Treatment
- The main objective of treatment is to protect the pulp by obliterating dentinal tubules
- In the case of enamel fracture, selective grinding of the incisal edge is done to remove sharp edges and prevent injury to lips, tongue, etc.
- For esthetic reasons, composite restoration is done
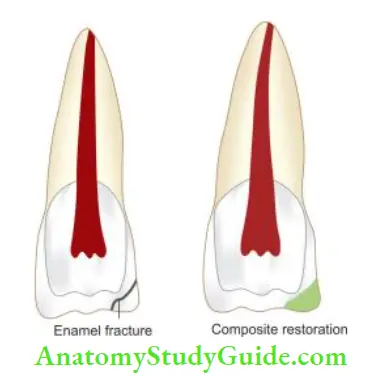


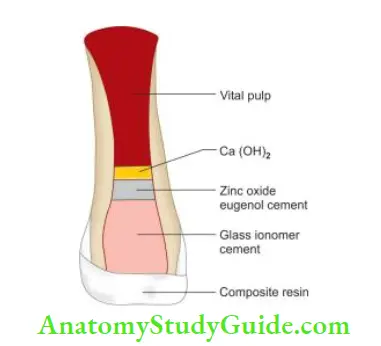
If both enamel and dentin are involved, a restoration is done to seal the dentinal tubules and restore the esthetics. Dentinal tubules can be sealed using calcium hydroxide, zinc oxide eugenol cement, glass ionomer cement, or dentin bonding agent.
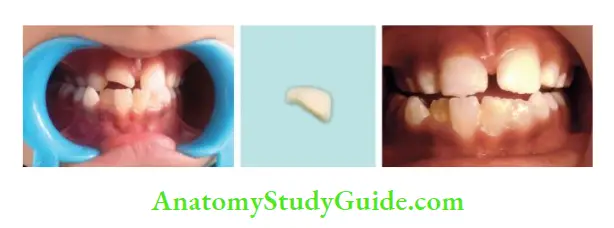
But eugenol cement should not be used where composite restoration is to be placed because eugenol may interfere with the polymerization of composites. If the fracture fragment of the crown is available, reattach it.
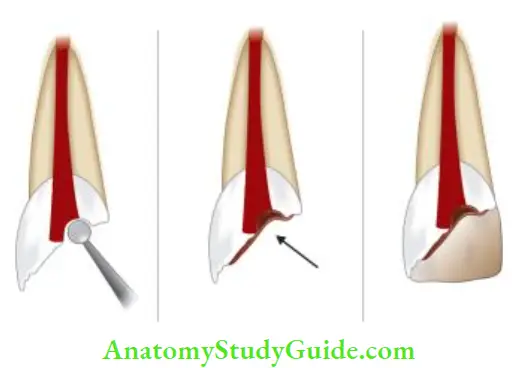
The following modifications are made for the reattachment of the fractured fragment:
- Beveling of enamel: Beveling helps to increase the retention of fragments by increasing the area for bonding and altering enamel prism orientation
- Internal dentinal groove: Internal dentinal groove is used as reinforcement for fragments but it compromises the esthetics because of the internal resin composite
- Internal enamel groove: Here V-shaped retention groove is placed in the enamel to which the fragment is attached. But due to the limited thickness of enamel, this procedure is difficult to perform
- Overcontouring: This technique is used when the fracture line is still noticeable after reattachment. Here, after joining the fractured fragment, a composite layer of 0.3 mm is placed superficially on the buccal surface. But composite can show abrasion and discoloration with time
- Simple reattachment: In this, the fragment is reattached using a bonding agent without any additional preparation
Prognosis
Patients should be recalled and sensitivity testing is done at regular intervals of 3, 6, and 12 months. The prognosis is good.
Complicated Crown Fracture
A crown fracture involving enamel, dentin, and pulp is called a complicated crown fracture.

Incidence
This type of fracture occurs in 2–13 % of all dental injuries.
Biological Consequences
- The extent of the fracture helps to determine the pulpal treatment and restorative needs
- The degree of pulp involvement may vary from pinpoint exposure to total uncovering of the pulp chamber
- If left untreated, it can lead to pulp necrosis
Diagnosis
Diagnosis is made by clinically evaluating the fracture, pulp status, and radiographs.
Treatment
- Factors like the extent of the fracture, and stage of root maturation are imperative in deciding the treatment plan for complicated root fracture. Maintaining the pulp vitality is the main concern of the treatment
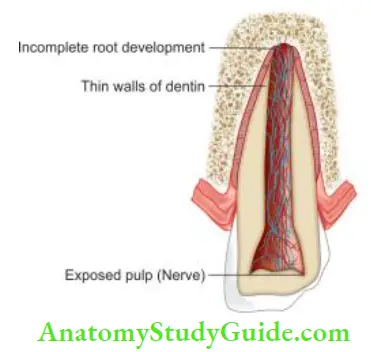
- In the case of immature teeth, abiogenesis, which is a normal process of root development, will occur only if the pulp is vital
- Roots of immature teeth become thin and fragile near the apex. The goal of treatment is to allow the apex to mature and dentin walls to thicken sufficiently to permit successful root canal therapy
Factors Affecting Pulpal Survival
Optimal blood circulation is necessary to nourish the pulp and keep it healthy. Type of injury, stage of root development, and degree of infection are the factors that affect circulation to the injured area and pulp vitality.
Pulp Capping and Pulpotomy
Pulp capping and pulpotomy are the measures that permit abiogenesis to take place and may avoid the need for root canal therapy. The choice between pulp capping and pulpotomy depends on
- Size of the exposure
- Presence of hemorrhage
- Time elapsed since injury
Pulp Capping
Pulp capping implies placing the dressing directly onto the pulp exposed.
Indications
It is indicated in case of very recent exposure (<24 h) with a simple restorative plan
Technique
- After adequate anesthesia, apply a rubber dam
- Rinse the exposed dentinal surface with saline followed by disinfection with 0.12% chlorhexidine or betadine
- Place calcium hydroxide or MTA over the exposed pulp
- Restore the tooth with a permanent restoration.
Follow-up
Vitality tests, palpation tests, percussion tests, and radiographs should be carried out at 3 weeks; 3, 6, and 12 months; and every 12 months subsequently to see continued root development.
Prognosis
The prognosis is up to 80% and it depends on:
- The ability of calcium hydroxide to disinfect the superficial pulp and dentin and to necrose the zone of superficially inflamed pulp
- Quality of bacterial tight seal provided by restoration.
Pulpotomy
Pulpotomy refers to the coronal extirpation of the vital pulp tissue.
Two types:
- Partial pulpotomy
- Full (cervical) pulpotomy
1. Partial Pulpotomy/Cvek Pulpotomy
Partial pulpotomy implies the removal of the coronal pulp tissue to the level of healthy pulp.
Indications
It is indicated in vital, traumatically exposed, young permanent teeth with incomplete root formation. The objective is that the remaining pulp tissue continues to be vital after partial pulpotomy.
Technique
- After anesthetizing the area, apply the rubber dam
- Prepare a 1–2 mm deep cavity into the pulp using a diamond bur
- Use a wet cotton pellet to impede hemorrhage
- Place a thin coating of calcium hydroxide mixed with saline solution or anesthetic solution over it
- Seal the access cavity with hard-setting cement like IRM
Follow-up
Satisfactory results and evaluation following pulpotomy should show
- Absence of signs or symptoms
- Absence of resorption, either internal or external
- Evidence of continued root formation in developing teeth
Prognosis
The prognosis is good (94–96%).

- (A) Preoperative radiograph;
- (B) Partial pulpotomy using calcium hydroxide;
- (C) Radiograph showing continuous development of root.
2. Cervical Pulpotomy/Deep Pulpotomy
The cervical pulpotomy involves the removal of the entire coronal pulp to the level of root orifices.
Indications
- When the gap between traumatic exposure and the treatment provided is >24 h
- When pulp is inflamed to deeper levels of coronal pulp
Technique
Coronal pulp is removed in the same way as in partial pulpotomy except that it is up to the level of root orifice.
Follow-up
Satisfactory results and evaluation following pulpotomy should show
- Absence of signs or symptoms
- Absence of resorption, either internal or external
- Evidence of continued root formation in developing teeth
- The main disadvantage of this treatment is that sensitivity tests cannot be done because of the loss of coronal pulp. This radiographic examination is important for follow-up
Prognosis
80–95% success rate is reported.
Prerequisites for Success
Vital pulp therapy has an extremely high success rate if the clinician strictly adheres to the following requirements:
Treatment of a noninflamed pulp:
- Treatment of a noninflamed pulp is found to be better than the inflamed pulp. Therefore, optimal time for treatment is first 24 h when pulp inflmmation is superficial
Pulp dressing:
- Calcium hydroxide is the dressing of choice. It causes necrosis of superficial layers of the pulp, which results in mild irritation to the adjacent vital pulp tissue. This irritation initiates an inflammatory response resulting in the formation of a hard tissue barrier
- Bioceramics like mineral trioxide aggregate (MTA), dentine produce optimal results
Bacterial tight seal: It is the most significant factor for successful treatment because the introduction of bacteria during the healing phase can cause failure.
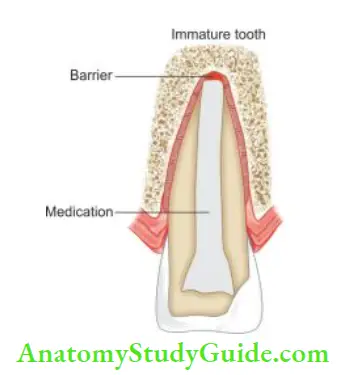
Apexification
Apexification is a method of inducing a calcified barrier at the apex of a nonvital tooth with incomplete root formation.
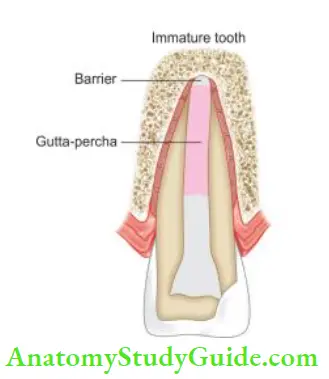
- Apexification using calcium hydroxide: After cleaning the canals, pack calcium hydroxide into the canal till the apical third. Place a cotton pledget and seal the coronal surface with IRM. When completion of hard tissue is suspected (after 3–6 months), remove calcium hydroxide and take a radiograph. If the formation of hard tissue is found satisfactory, obturate the canal using the softened gutta-percha technique. One should avoid excessive lateral forces during obturation because of the thin walls of the root
- Apexification using MTA: MTA is preferred over calcium hydroxide for apexification. After cleaning the canal, place calcium hydroxide for 1 week. After 1 week, remove the calcium hydroxide and fill the apical 3–5 mm with MTA. Place a moist cotton pledget and temporary restoration over it. After 24 hours, a root canal is obturated coronal to MTA using thermoplasticized gutta-percha
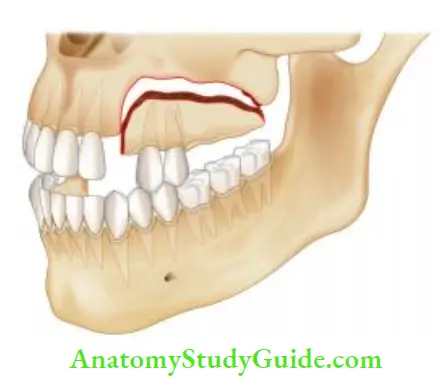
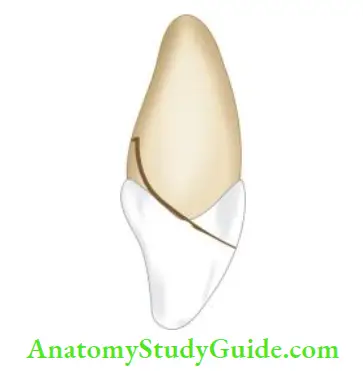
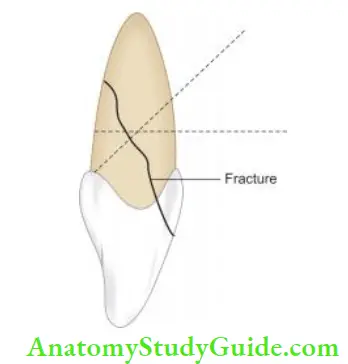
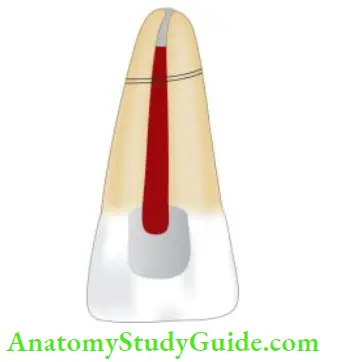
Crown Root Fracture
Crown root fracture involves enamel, dentin, and cementum with or without the involvement of pulp.
It is usually oblique in nature involving both crown and root. This type of injury is considered as more complex type of injury because of its greater severity and involvement of the pulp.
Incidence
It contributes 5% of total dental injuries. In anterior teeth, it occurs by direct trauma causing chisel-type fracture which splits crown and root. In posterior teeth, fracture is rarely seen but it can occur because of indirect trauma like large-sized restorations, pin placements, highspeed instrumentation, etc.
Biological Consequences
- Biological consequences are similar to as that of complicated or uncomplicated fractures depending upon pulp involvement
- In addition to these, periodontal complications are also present because of the encroachment of the attachment apparatus
Diagnosis
Crown root fractures are complex injuries which are difficult both to diagnose and treat. A tooth with crown root fracture exhibits the following features:
- The coronal fragment is usually mobile. The patient may complain of pain on mastication due to movement of the coronal portion
- Inflammatory changes in pulp and periodontal ligament are seen due to plaque accumulation in the line of fracture
- Patients may complain of sensitivity to hot and cold
- Radiographs are taken at different angles to assess the extent of the fracture
- Indirect light and transillumination can also be used to diagnose this type of fracture
Treatment
The primary goal of treatment is the elimination of pain which is mainly because of the mobile crown fragment. It can be done by applying bonding agents to bond the loose fragments together, temporary crown placement, or by using glass ionomer cement.
Objectives of treating crown root fracture are to:
- Allow the subgingival portion of the fracture to heal
- Restoration of the coronal portion
Depending upon extent of the fracture, the following should be considered while managing crown root fracture:
- If there is no pulp exposure, the fragment can be treated by bonding alone or by removing the coronal structure and then restoring it with composites
- If pulp exposure has occurred, pulpotomy or root canal treatment is indicated depending upon the condition of the tooth
- When the remaining tooth structure is adequate for retention, endodontic therapy followed by a crown is done. If the fractured fragment is available, one should attempt to reattach it
- When the root portion is long enough to accommodate a post retained crown, then surgical removal of the coronal fragment followed by surgical extrusion of the root segment is done
- To accommodate a post retained crown, after removal of the crown portion, orthodontic extrusion of the root can also be done
- When the fracture extends below the alveolar crest level, the surgical repositioning of tissues by gingivectomy, osteotomy, etc. should be done to expose the level of fracture and subsequently restore it
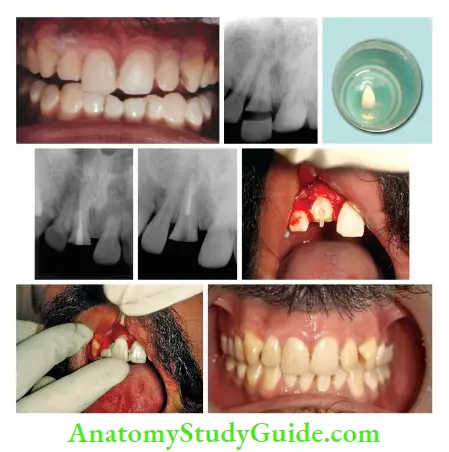
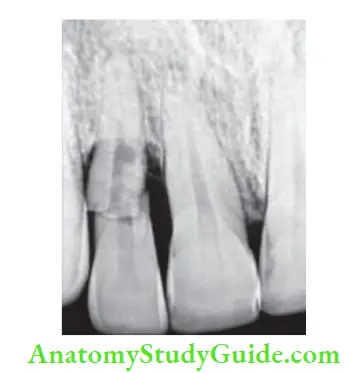
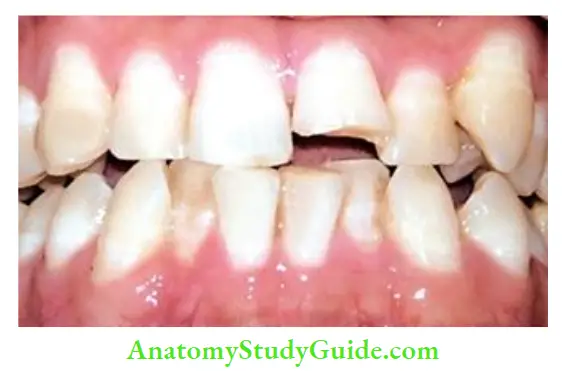
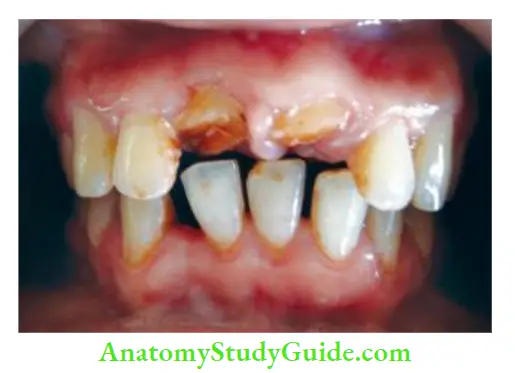
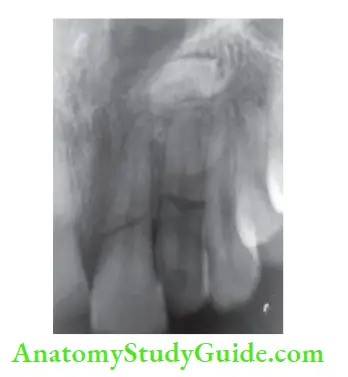
- (A) Photograph showing fractured right maxillary central incisor;
- (B) Radiograph showing oblique fracture in the middle third of crown;
- (C) Fractured fragment removed and preserved in saline;
- (D) Postobturation radiograph of the fractured tooth;
- (E) Post-space preparation;
- (F) Fiber post-cementation;
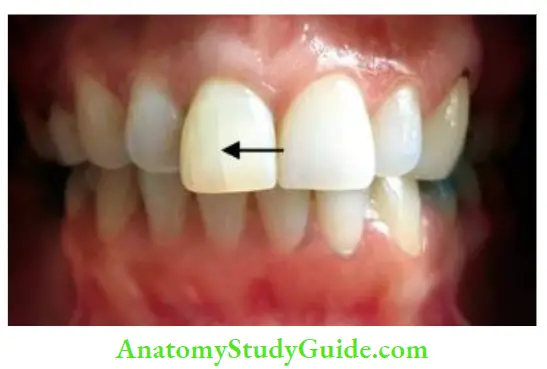
- (G) Reattachment of the fractured fragment;
- (H) Postoperative photograph.

Prognosis
If the pulp is not involved, the condition should be evaluated from time to time. Long-term prognosis depends on the quality of coronal restoration. Otherwise, the prognosis is similar to a complicated or uncomplicated fracture.
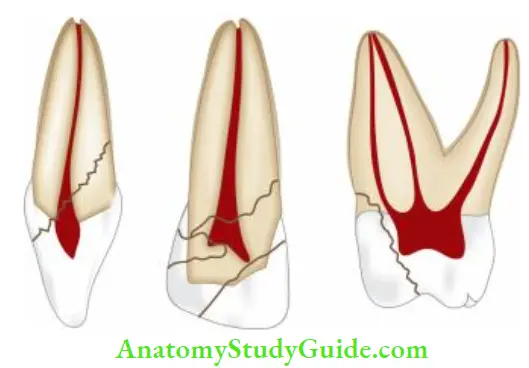
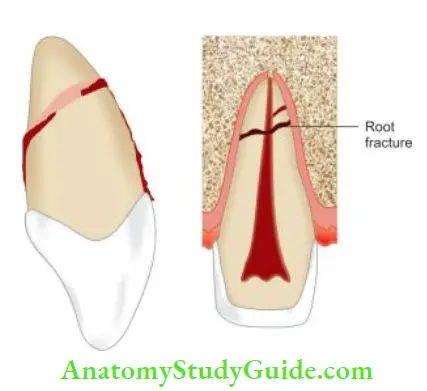
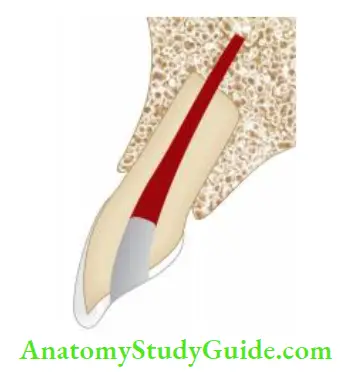
Root Fracture
These are uncommon injuries but represent a complex healing pattern due to the involvement of dentin, cementum, pulp, and periodontal ligament.
Incidence
- Root fracture form only 3% of the total dental injuries
- These fractures commonly result from a horizontal impact and are transverse to oblique in nature
- These are most commonly seen in mature roots and least common in incomplete roots
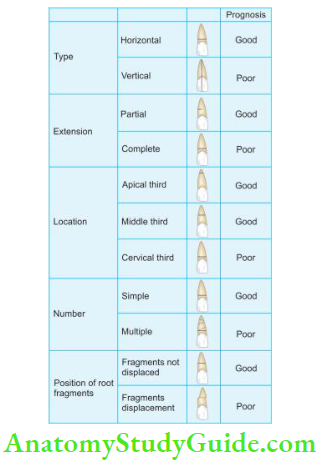
Classifiation of Root Fracture
Biological Consequences
When root fractures occur horizontally, the coronal segment is displaced to varying degrees. If the vasculature of the apical segment is not affected, it rarely becomes necrotic.
Diagnosis
- Displacement of coronal segment usually reflects the location of the fracture
- Radiographs at varying angles (usually at 45°, 90°, and 110°) are mandatory for diagnosing root fractures.
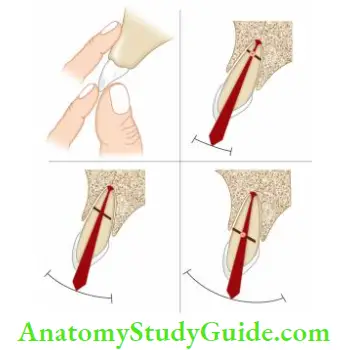
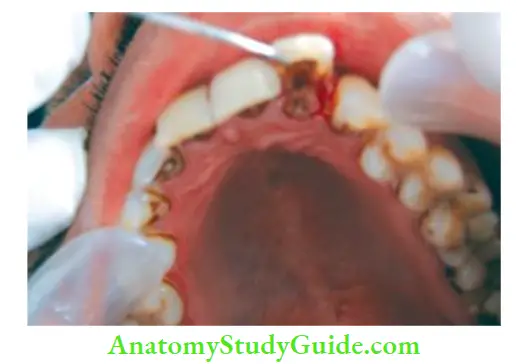
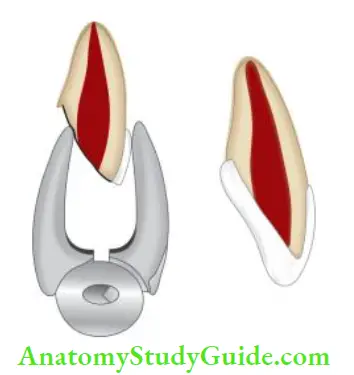
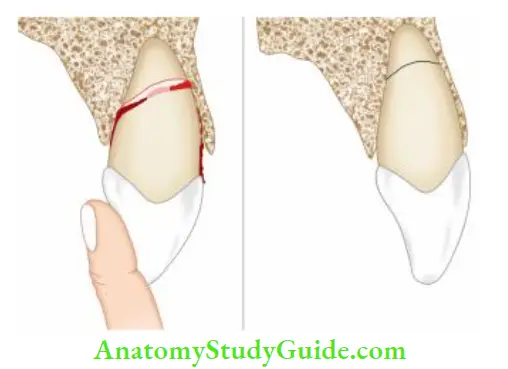
- (A) Palpating the facial mucosa with one finger and moving the crown with another finger;
- (B to D) Arc of mobility of incisal segment of the tooth with root. As fracture moves incisively, the arc of mobility increases.

Treatment of Root Fractures
The prognosis of root fracture depends upon
- Amount of dislocation and degree of mobility of coronal segment: More is the dislocation, the poorer is the prognosis
- Stage of tooth development: More immature the tooth, the better the ability of pulp to recover from trauma
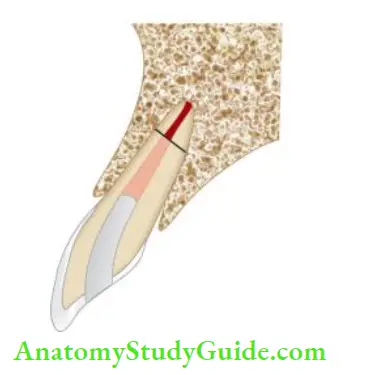
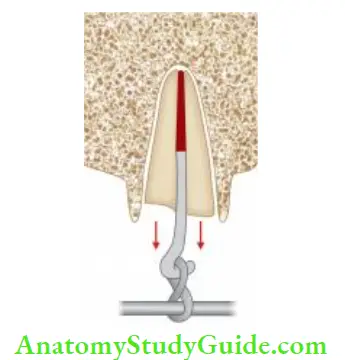
Apical Third Fracture
- The prognosis is good if the fracture is at the apical third level provided there is no mobility and the tooth is asymptomatic
- To facilitate pulpal and periodontal ligament healing, displaced coronal portions should be repositioned accurately. It is stabilized by splinting for 2–3 weeks and the tooth is kept out of occlusion
- Since the apical third has vital pulp, the prognosis is good. If pulp in the coronal third is also vital and the tooth is made stable, no additional treatment is needed
- If the pulp in the coronal portion is nonvital, then root canal therapy of the coronal segment and no treatment of the apical segment is suggested
- If the tooth fails to recover, surgical removal of the apical segment is suggested
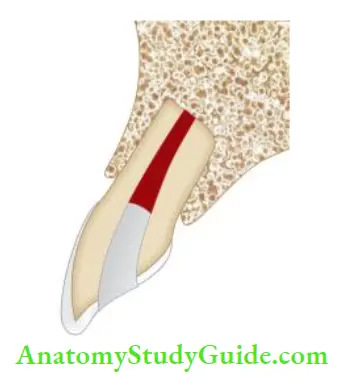
Mid-Root Fracture
The treatment plan and prognosis of mid-root fracture depend upon
- Mobility of coronal segment
- Location of the fracture line
- Status of pulp
- Position of the tooth after fracture
Various treatment options are
- Root canal therapy for both coronal and apical segments, when they are not separated
- Root canal therapy for the coronal segment and surgical removal of the apical third if the apical segment is separated
- Apexification procedure of coronal segment, i.e. inducing hard tissue barrier at the exit of the coronal root canal and no treatment of apical segment. Another method is to use MTA for creating an apical barrier in the coronal segment. This is the most commonly used procedure nowadays
- Intraradicular splint in which a rigid type of post is used to stabilize the two root segments
- In endodontic implants, here, the apical portion of the implant replaces the surgically removed apical root segment

- (A) Preoperative radiograph;
- (B) Working length radiograph;
- (C) Master cone radiograph;
- (D) Postobturation radiograph.

Coronal Third–Root Fracture
- The prognosis is poor because it is difficult to immobilize the tooth
- Because of the constant movement of the tooth, repair does not take place
- If the fracture level is at or near the alveolar crest, root extrusion is indicated. Here coronal segment is removed and the apical segment is extruded orthodontically to allow restoration of the missing coronal tooth structure
Healing of Root Fracture
According to the Andreasen and Hjorting-Hansen, root fracture can show healing in the following ways:
- Healing with calcified tissue in which fractured fragments are in close contact
- Healing with interproximal connective tissue in which radiographically fragments appear separated by a radiolucent line
- Healing with interproximal bone and connective tissues. Here fractured fragments are seen separated by a distinct bony bridge radiographically
- Interproximal inflammatory tissue without healing, radiographically it shows a widening of the fracture line
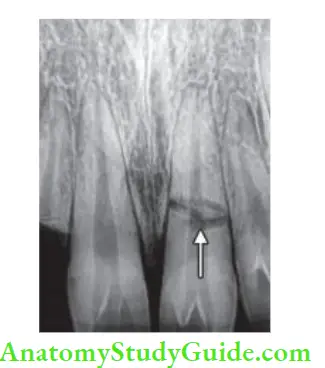
Follow-up Procedure
- Pulp testing and radiographic examination should be performed at 3 weeks, 6 weeks, 6, and 12 months after the injury
- Radiographs are taken to predict the healing of root fractures. Resorption within the root canal originating at the fracture line indicates healing following pulpal damage after trauma. But resorption within the bone at the level of the fracture line indicates pulp necrosis which requires endodontic therapy.

- (A) Calcified tissue;
- (B) Interproximal inflammatory tissue seen in root fracture;
- (C) Interproximal bone;
- (D) Formation of connective tissue between the segments.
Leave a Reply