Miscellaneous Bacteria
Miscellaneous Gram-Positive Bacteria
Listeria Monocytogenes
Listeria monocytogenes is a food-borne zoonotic pathogen that can cause serious human infections, particularly in neonates, pregnant women, and elderly people.
Table of Contents
Pathogenicity
- It can grow in refrigerated food and can tolerate preserving agents.
- Mode of transmission: Contaminated food (due to its ability to survive refrigeration [4°C], it is commonly found in stored foods soft cheeses, packaged meats, milk, and cold salads; followed by vertical transmission (mother to fetus).
- Intracellular survival: It is facultative intracellular organism. Survival inside the host cells is due to inhibition and lysis of phagosome by forming pores (mediated by listerio-lysin O).
- Direct cell-to-cell spread is due to host cell actin polymerization (mediated by listeriopods).
Read And Learn More: Micro Biology And Immunology Notes
Clinical Manifestations
- Infection in pregnancy: Before 20 weeks is rare, may lead to abortion, stillbirth.
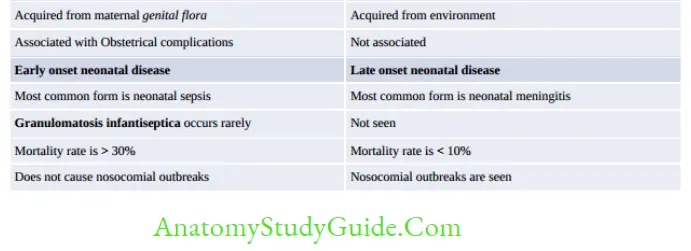
- Neonatal disease: Two types: early onset and late onset
- Adult:
- Associated with steroid therapy, HIV, DM, malignancy (fludarabine treated)
- Bacteremia > meningitis
- MC cause of meningitis in kidney transplanted patient after 1 month
- Also causes Gastroenteritis: Following contaminated milk, meat, and salad.

Lab Diagnosis
- Useful specimens are CSF, blood and amniotic fluid
- Gram-positive coccobacilli, catalase positive
- Shows tumbling type of motility
- Motile at 25°C but nonmotile at 37°C (Differential motility)
- Growth improves if cultured in thioglycollate broth at 4°C (cold enrichment)
- Media: Blood agar, chocolate agar, PALCAM agar (selective medium)
- Anton test: Instillation to rabbit eye causes conjunctivitis
- Biochemical tests: catalase positive, can grow in presence of 10% salt and low pH and CAMP test positive.
Treatment
- DOC: Ampicillin (also penicillin)
- Alternate: Cotrimoxazole (if allergic to penicillin)
- Cephalosporin not affective
Actinomycetes
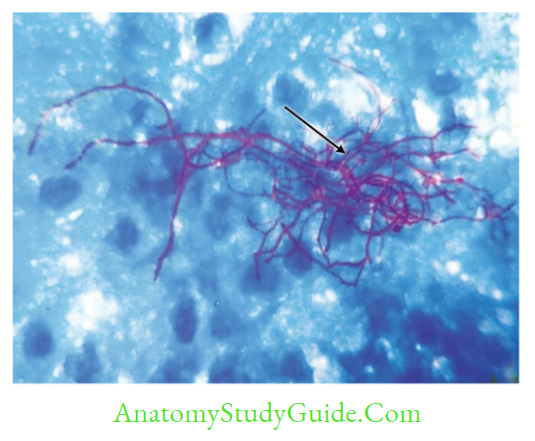
Actinomycetes are Gram-positive branching filamentous bacteria Human pathogenic actinomycetes: Actinomyces, Streptomyces, Nocardia, Actinomadura
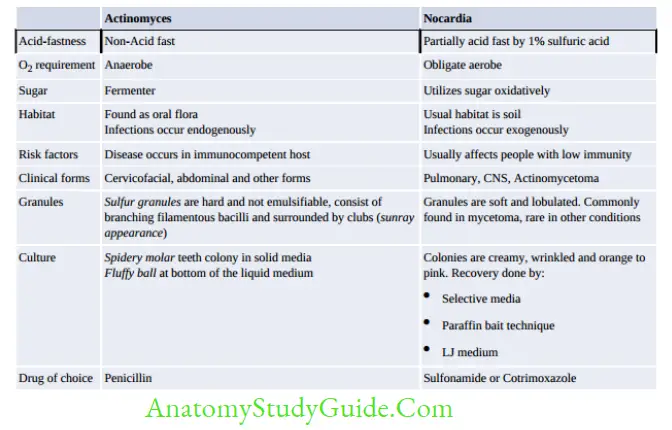
- Actinomyces is non-acid fast and anaerobic
- Nocardia: Aerobe and acid fast (1% sulfuric acid)
- Streptomyces and Actinomadura are aerobes and non-acid fast – Can cause actinomycetoma
![]()
Actinomadura
- It is the most frequent cause of actinomycetoma, significantly outnumbering the cases caused by Nocardia.
- Actinomadura madurae and A. pellettieri are important species
- Granules are usually white to yellow except in case of A. Pelletier that produces red-colored granules
- Microscopy of the specimens containing granules reveals branching filamentous bacilli
- Colonies have a molar tooth appearance
- Most isolates are susceptible to amikacin and imipenem.
Tropheryma whipplei
Tropheryma whipplei is a gram-positive actinomycete not closely related to any known genus.
It is the agent of Whipple’s disease affecting the small intestine.
- Whipple’s disease is characterized by fever, abdominal pain, diarrhea, weight loss and migratory polyarthralgia.
- Mesenteric lymph nodes of the small intestine are primarily involved.
- Laboratory diagnosis:
- Histopathological staining of intestinal biopsy shows vacuoles within the macrophage containing PAS stain positive bacilli.
- Culture of T.whipplei has been unsuccessful.
- PCR targeting 16S rRNA can be done to identify the bacilli.
Treatment of Whipple’s disease include: - DOC: Doxycycline and hydroxychloroquine for 1 year, followed by lifelong doxycycline
- Alternate regimen include: IV ceftriaxone or IV meropenem for 14 days followed by doxycycline and hydroxychloroquine for 1 year.
Erysipelothrix Rhusiopathiae
- Gram-positive bacilli
- Catalase negative, H2S positive
- Causes erysipeloid skin lesion violaceous swelling with severe pain, but no pus.
- Most common site is finger (called ‘seal finger’ and ‘whale finger’).
- Treatment: DOC is penicillin G, however it is intrinsically resistant to vancomycin.
Miscellaneous Gram-Negative Bacteria
Campylobacter
Campylobacter species are microaerophilic curved gram-negative bacilli. They are zoonotic, cause both diarrheal (C.jejuni; accounts for 80-90% of total cases) and systemic diseases (C.fetus).
Epidemiology
- Mode of transmission: by ingestion of raw or undercooked food-poultry (most common), raw (unpasteurized) milk or water, through direct contact with animals,oral-anal sexual contact
- MC Age affected: C.jejuni (children) and C.fetus (extremes of age)
- Developing versus developed countries:
- In developing countries: It is hyperendemic, mostly asymptomatic except < 2 years(symptomatic).
- In developed countries, Campylobacter is the leading bacterial cause of diarrheal disease.
- Seasonality: Incidence peaks during summer and early autumn.
Pathogenesis
- Motility of the strain (possesses single polar flagellum and exhibits darting motility)
- Capacity to adhere to host tissues
- Toxins play a minor role:
- Enterotoxin (Heat-labile, similar to cholera toxin)
- Cytotoxins (cytolethal distending toxin, or CDT)
- Proteinaceous capsule-like structure (S-layer) expressed by C. fetus.
Clinical Manifestations
- Intestinal infection: Characterized by inflammatory diarrhea, abdominal pain and fever, rarely bloody stools.
- Extraintestinal infection is mainly due to C.fetus developing mostly in immunocompromised hosts and at the extremes of age.
- In persons with the HLA-B27: Reactive arthritis and other rheumatologic manifestations.
Laboratory Diagnosis
- Gram staining of smear of feces may show curved gram-negative bacilli appearing comma (resembling Vibrio), S-shaped or spiral (gull wing shaped).
- Dark ground microscopy demonstrates the darting motility of the bacilli.
- Culture media are:
- Transport medium: Cary-Blair medium can be used.
- Selective media: (1) Skirrow’s, (2) Butzler’s and (3) Campy BAP selective media.
- Culture conditions: Microaerophilic (5% O2) and Thermophilic Grow at 42°C except C.fetus (nonthermophilic).
Treatment
Fluid and electrolyte replacement is the mainstay of treatment. Antibiotics can be given,
Diarrheal disease: Oral macrolides are the drug of choice (erythromycin or azithromycin).
- Systemic infection: Parenteral gentamicin (or imipenem or chloramphenicol)
Helicobacter
Helicobacter pylori is curved gram-negative rod that colonizes stomach and is associated with peptic ulcer disease and gastric carcinoma.
Pathogenesis
H. pylori colonizes the stomach of 50% of the world’s human population (30% in developed countries to nearly 80% in developing countries). The colonization is favored by the following factors:
- Motility: H. pylori is highly motile (conferred by 4 to 8 unipolar flagella), which allows it to remain in the viscous environment of the mucus layer overlying the gastric mucosa
- Acid-resistance: It may be due to:
- Urease enzyme: It produces abundant urease that catalyzes urea hydrolysis to produce ammonia which in turn buffers the gastric acid
- Amidase and arginase: May contribute to the production of ammonia
- Ure-I protein: It regulates the passage of urea acros the cell membrane into cytoplasm.
- Adhesins: It binds to mucosal epithelium with the help of Blood group antigen-binding adhesin (binds to Lewis blood group antigen) and Adherence-associated lipoprotein
- Resistance to oxidative stress: It produces detoxifying enzymes that protect the organism against the effects of oxygen-derived free radicals.
- Induces pathological changes by:
- Secrets vacuolating cytotoxin (VacA) and Cytotoxin associated gene A (CagA)
- Molecular mimicry: Lipopolysaccharide of H. pylori is identical to the Lewis blood
group antigen on gastric parietal cells which contributes to the development of chronic active gastritis. - Environmental risk factors: Smoking increases the risk of ulcers and cancer in H.pyloricolonized individuals and Diets high in salt and preserved foods increase cancer risk,
whereas diets high in antioxidants and vitamin C are protective.
Clinical Manifestations
- Acute gastritis (Antrum is the most common site involved, cardiac end is not involved),
- Antral gastritis: Predisposes to duodenal ulcers
- Pan gastritis: Predisposes to adenocarcinoma of stomach
- Peptic ulcer disease: 80% of duodenal ulcers and 60% of gastric ulcers are due to H.pylori.
- Chronic atrophic gastritis
- Autoimmune gastritis
- Promotes pernicious anemia
- Adenocarcinoma of stomach and non-Hodgkin’s gastric lymphoma
Laboratory Diagnosis
Invasive Test
Endoscopy-guided multiple biopsies can be taken from gastric mucosa (antrum and corpus) and are subjected to:
- Histopathology with Warthin-Starry silver staining
- Microbiological methods:
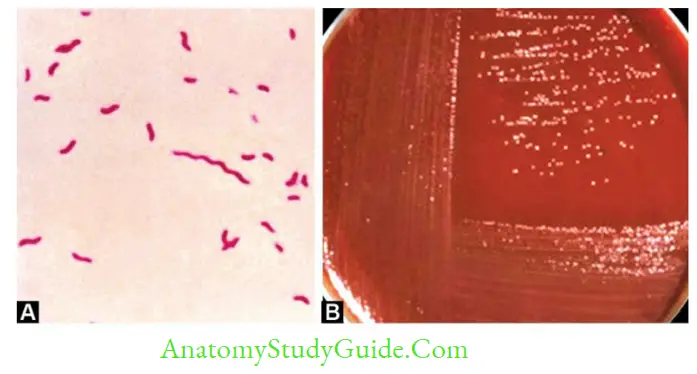
- Gram staining: Curved gram-negative bacilli with seagull shaped morphology
- Culture media for H.pylori: Culture is the most specific test, however, it is not sensitive.
- Media for Campylobacter can be used, such as Skirrow’s media
- Chocolate agar can be used
- Plates are incubated at 37°C under microaerophilic condition
- Biochemical tests: Oxidase, catalase, and urease tests are positive.
- Biopsy urease test (rapid urease test): Detects urease activity in gastric biopsies. It is rapid, sensitive, and cheap.
Noninvasive Test
- Urea breath test: It is very popular nowadays as it is non-invasive and is:
- Most consistent and accurate test
- Most sensitive, quick and simple
- Used for monitoring of treatment (becomes negative after improvement)
- Stool antigen (coproantigen) assay: Used for
Monitoring of treatment,Screening of children.
Antibody (IgG) detection by ELISA: Used for
Screening before endoscopy, Seroepidemiological study
![]()
Treatment Regimen for H. pylori Infection
Treatment in H.pylori infections is indicated for (1) duodenal or gastric ulceration, (2) low-grade gastric B cell lymphoma
However, treatment is not recommended for asymptomatic colonizers or primary prophylaxis for gastric cancer because of risk of adverse side effects and development of antibiotic resistance
Legionella
Legionellae are fastidious gram-negative, short rods, associated with two respiratory syndromes: Pontiac fever and Legionnaires’ disease
- Most cases are associated with serogroup 1 followed by 4, and 6.
- Other species rarely cause human infection, such as L.micdadei (Pittsburgh pneumonia agent,acid fast) and L.longbeachae.
Epidemiology
- Reservoir: Legionella inhabits on aquatic bodies:
Natural water sources, such as rivers or even inside amebae,
Artificial aquatic sources, such as air conditioners. - Transmission:
- Aspiration (MC mode) via oropharyngeal colonization or directly via drinking of contaminated water.
- Aerosols from contaminated air conditioners, nebulizers, and humidifiers
- Direct instillation into the lungs during respiratory tract manipulations
- There is no man to man transmission, there is no animal reservoir and no carrier.
- Predisposing factors for Legionella infections include:
- Smoking, alcoholism and chronic lung disease—impair mucociliary clearance
- Advanced age
- Immunosuppression-transplantation, HIV infection, steroid therapy
- Prior hospitalization
- Patients with nasogastric tubes or those undergoing surgery with general anesthesia promotes aspiration.
Pathogenesis
After Legionellae enter the lungs through aspiration or direct inhalation:
- Attachment and invasion to respiratory mucosa
- Coiling phagocytosis: Macrophages phagocytose legionellae by a coiling mechanism.
- Legionella evades intracellular killing by inhibiting phagosome-lysosome fusion.
Clinical Manifestations
- Pontiac Fever: It is an acute, flu-like illness
- Legionnaires’ Disease (Pneumonia): This is an interstitial atypical pneumonia:
- It is the fourth common cause of community-acquired pneumonia, accounting for 2–9%of cases).
- It is responsible for 10–50% of cases of nosocomial pneumonia. Serogroup 6 is more commonly involved in hospital outbreaks.
Extrapulmonary Legionellosis:
- The most common extrapulmonary site is heart; (myocarditis, pericarditis and prosthetic-valve endocarditis)
- Other manifestations include: Sinusitis, peritonitis, pyelonephritis, skin and soft tissue infection.
Laboratory Diagnosis
- Gram stain reveals numerous neutrophils but no organisms (as legionellae are poorly stained, often missed or sometimes appear as faint pleomorphic gram-negative rods or coccobacilli)
- Silver impregnation and Giemsa stains can be used
- Direct fluorescent antibody (DFA)
- Culture: Buffered charcoal, yeast extract (BCYE) agar is the recommended media.
- Antibody Detection: used for epidemiologic purpose. A single titer of more than 1:128 or fourfold rise in titer is considered as significant.
- Urinary Antigen: It is rapid, cheaper, easy to perform,
Remains positive even after antibiotics. Next to culture, it is highly sensitive, and specific - PCR is useful for isolation from environmental water. Most common targets are mip (macrophage inhibitor protein) gene, 5S and 16S rRNA and 16S–23S spacer region genes.
Treatment
Macrolides (azithromycin) and the respiratory quinolones are antibiotics of choice.
Calymmatobacterium Granulomatis
It is the agent of granuloma inguinale (also called Granuloma venereum or Donovanosis)
Present name is Klebsiella granulomatis
- Clinical feature:
- Painless ulcer: Ulcerogranulomatous beefy red ulcer that bleeds readily
- No lymphadenopathy, however pseudobulbs seen due to subcutaneous abscess.
- Donovan bodies (stained by Wrights, Giemsa): Large cyst like macrophages filled with deeply stained capsulated bacilli having a safety-pin (bipolar) appearance.
- Culture: Embryonated hens egg and on HEp-2 cell lines.
- Treatment: DOC is Azithromycin, Alternate: Cotrimoxazole, Erythromycin and Tetracycline.
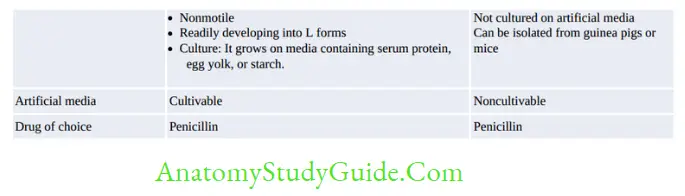
Rat Bite Fever
Agents: Streptobacillus moniliformis and Spirillum minus
Gardnerella Vaginalis
It causes bacterial vaginosis.
- It is a gram variable (mostly gram-negative coccobacilli), possess metachromatic granules
- Other organisms implicated in BV- Mycoplasma hominis, Mobilincus, Prevotella, Ureaplasma and Peptostreptococcus
- Treatment: DOC Metronidazole

Pasteurella Multocida
It is probably the most common organism in human wounds inflicted by the bites of cats and dogs.
- Clinical findings: Causes wound infection, regional lymphadenopathy and respiratory infection.
- Laboratory diagnosis:
- Nonmotile gram-negative coccobacilli with a bipolar staining.
- They resemble yersiniae, however differ from the latter in being:
- Oxidase-positive and indole positive
- Failure to grow on MacConkey agar
- Treatment: Penicillin G is considered as the drug of choice for P. multocida infections.
Francisella Tularensis (Tularemia)
- Transmission: Direct contact with rodents > Tick bite > Inhalation and Ingestion
- Subspecies: F. tularensis has four subspecies: tularensis, holarctica, novicida, and mediasiatica.
- The first three are found in North America; whereas subspecies mediasiatica is found in central Asia
- Subspecies tularensis is the most common and the most virulent among all.
- Clinical manifestations: Tularemia is characterized by various clinical syndromes
- Ulceroglandular tularemia (MC form): Ulcerative lesion at the site of inoculation, with regional lymphadenopathy
- Pulmonary tularemia
- Oropharyngeal tularemia and Lemming fever in Norway
- Oculoglandular tularemia
- Typhoid-like illness
- Agent of bioterrorism (under class A).
- Laboratory diagnosis:
- Small gram-negative coccobacillus with bipolar appearance, nonmotile and capsulated and filamentous
- Filterable, fastidious and obligate aerobe.
- Media: Francis blood dextrose cysteine agar
- Antibody detection is the mainstay of diagnosis.
- Treatment: Gentamicin is considered as the drug of choice.
Chromobacterium Violaceum
It is a saprophyte of water and soil in tropics.
- It occasionally causes skin lesions, sepsis, and liver abscesses
- It is a motile, gram-negative, facultative anaerobe, non-sporing, coccobacillus.
- It produces characteristic violet color non-diffusible pigment (called violacein).
Capnocytophaga Species
Several species, such as C. ochracea, C. gingivalis and C. sputigena have been a part of human mouth flora.
- They occasionally cause periodontal diseases, and sepsis in immunocompromised hosts.
- Species, such as C. canimorsus and C. cynodegmi are commensals in mouth of dogs and are transmitted by dog bites.
- Laboratory diagnosis:
- They are fusiform or filamentous gram-negative coccobacilli
- Highly fastidious, require carbon dioxide for optimal growth
- They produce yellow orange pigment
- They lack flagella but exhibit gliding motility on agar surface.
Treatment: Due to their ability to produce β lactamases, ampicillin + sulbactam is the drug of choice.
Leave a Reply