Spirochetes
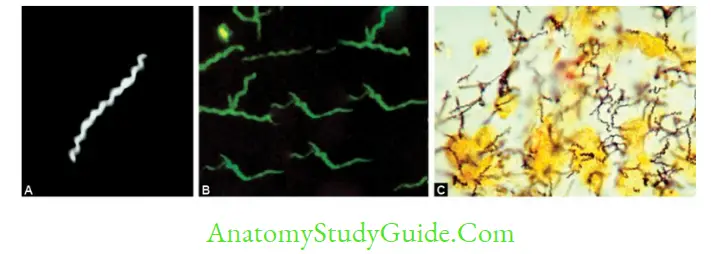
Spirochetes are thin, flexible, elongated spirally coiled helical bacilli (speira, meaning coil; and chaite, meaning hair).
Table of Contents
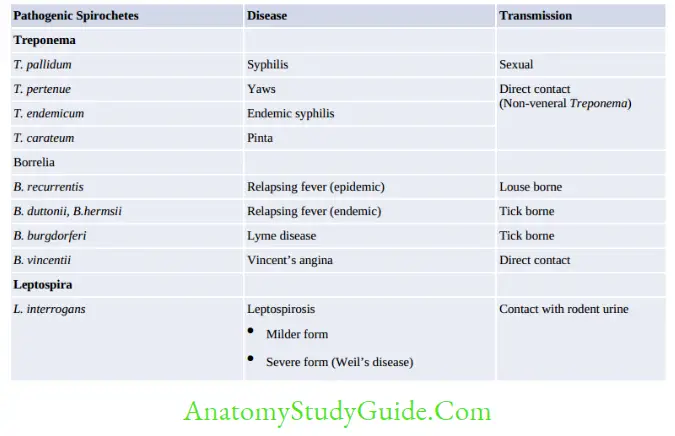
Most spirochetes are saprophytes. Only three are human pathogens: Treponema, Borrelia and Leptospira.
Read And Learn More: Micro Biology And Immunology Notes
Syphilis
Syphilis is one of the ancient sexually transmitted disease. Name was derived from a famous poem in the year 1530 which described a legend of a shepherd boy named Syphilus, who had suffered from the disease.
- Transmission: It is acquired by sexual contact. However, it can also be transmitted by nonvenereal modes such as direct contact, blood transfusion or transplacental transmission.
- Spread: T. pallidum rapidly penetrates through the minute abrasions on the skin or mucosa and, within a few hours, enters the lymphatics and blood to produce systemic infection and metastatic foci long before the appearance of a primary lesion.
- Incubation period is variable (9–90 days) and is inversely proportional to the number of organisms inoculated.
- Treponema pallidum is the causative agent of ‘syphilis’. ‘Pallidum’ refers to its pale-staining property. It was discovered by Schaudinn and Hoffmann in 1905.
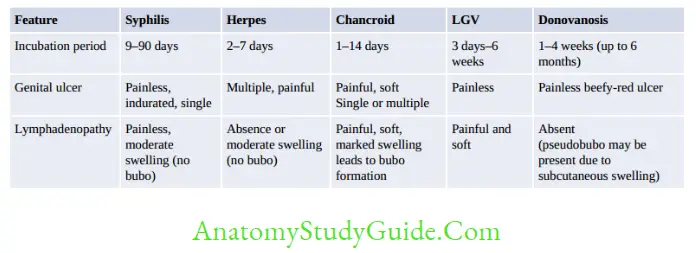
Clinical Manifestations
Approximately, 30% of persons who have sexual exposure with an infected partner develop syphilis; which can pass through various stages: primary, secondary, latent and tertiary (or late) stages.
Primary Syphilis
- Primary (or hard) chancre: Single painless indurated ulcer. MC sites are penis (in males), cervix or labia (in females).
- Regional (usually inguinal) lymphadenopathy: Painless firm, nonsuppurative, and often bilateral.
Secondary Syphilis
It usually develops 4–8 weeks after the healing of primary lesion and is characterized by:
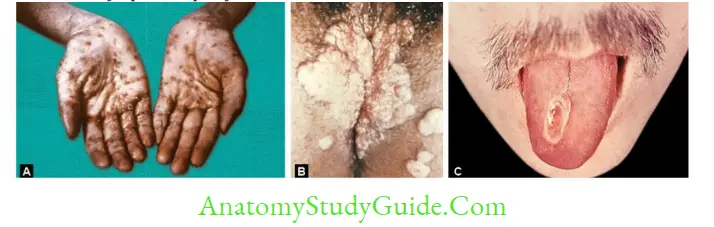
- Skin rashes (palms and soles)
- Condylomata lata (mucocutaneous lesion)
- Mucous patches (superficial mucosal erosions)
- Generalized lymphadenopathy
Latent Syphilis
It is characterized by absence of clinical manifestations of syphilis with positive serological tests for syphilis and normal CSF findings in patients with history of primary and secondary syphilis in the past.
- Early latent syphilis (occurs within first year after infection) and late latent syphilis (occurs after the first year).
- Patients are still infectious transmitting the infection either by bloodstream or in utero.
- Latent syphilis may have one of the following fates:
- Persistent lifelong infection (common)
- Development of late syphilis (rare)
- Spontaneous cure
Late or Tertiary Syphilis
One-third of untreated patients develop tertiary syphilis after several decades.
- Gumma (late benign syphilis): Occurs in 15% people
- Cardiovascular syphilis (10% people): Characterized by, aneurysm of ascending aorta and aortic regurgitation.
- Neurosyphilis: Invasion of CNS occurs in first few weeks of infection, but manifestations develop only in late stage. CNS and CVS lesions are called as quaternary syphilis:
- Meningeal syphilis (meningitis)
- Meningovascular syphilis (vasculitis of arteries leading to embolic stroke)
- General paresis of insane
- Tabes dorsalis (demyelination of the posterior columns).
- Cardiovascular syphilis: Characterized by aneurysm of ascending aorta and aortic regurgitation.
Congenital Syphilis
Placental transmission may occur at any stage of pregnancy, but fetal damage occurs only after fourth month of gestation. Manifestations of congenital syphilis include:
- Earliest manifestations occur within 2 yrs of age. Affected children are infectious and they suffer froy rhinitis (or snuffles), smucocutaneous lesions, bone changes, hepatosplenomegaly and lymphadenopathy.
- Late congenital syphilis occurs after 2 years and is noninfectious. It is characterized by interstitial keratitis, eighth-nerve deafness bilateral knee effusions (Clutton’s joints)
- Residual stigmata may remain for long time such as:
- Hutchinson’s teeth notched central incisors) Mulberry molar
- Saddle nose and saber shins.
Laboratory Diagnosis of Syphilis

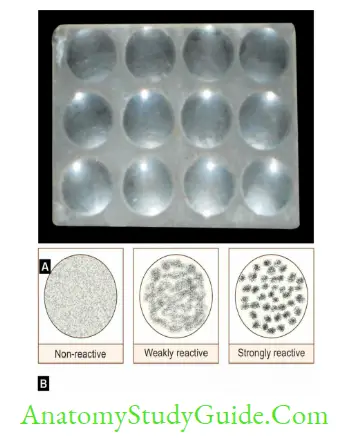
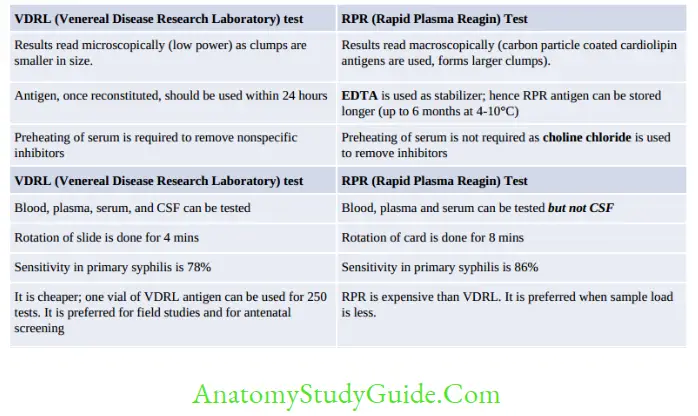
VDRL (Venereal Disease Research Laboratory)
VDRL test is a slide flocculation test (type of precipitation reaction)
- Antigen preparation: VDRL antigen is a cardiolipin antigen derived from bovine heart to which cholesterol and lecithin are added.
Antigen has to be reconstituted with buffer and should be used within 24 hrs. - Patient’s serum preparation: Inactivating serum by heating at 56°C for 30 min to remove the non-specific inhibitors.
- VDRL slide containing 12 concave rings are used.
Qualitative test: Drop of inactivated serum is mixed with a drop of VDRL antigen and the slide is rotated for 4 minutes:- Non-reactive: Uniformly distributed fusiform crystals represent the presence of VDRL antigen only
- Reactive: Medium to large clumps signifies antigen antibody complexes
- VDRL-CSF: VDRL test can also be performed to detect CSF antibodies. However, no preheating of CSF is needed.
Advantages of nontreponemal tests
- Monitoring the response to treatment: Reagin tests usually become negative 6–18 months after the effective treatment for syphilis, depending on the stage at which treatment is given.
- Neurosyphilis: VDRL can also be used to detect CSF antibodies.
- Reagin antibody becomes detectable 7–10 days after the appearance of primary chancre (or 3–5 weeks after infection).
- Sensitivity of nontreponemal tests varies from 78–85% in primary, 100% in secondary and 95–98% in latent stage.
Disadvantages of nontreponemal tests:
- Biological false positive (BFP) reactions: Defined as positive nontreponemal tests, with negative treponemal tests and not caused by technical faults and no clinical feature. It occurs in 1% of cases:
- BFP antibody is usually of IgM type, while reagin antibody in syphilis is mainly IgG.
- Types of BFP: Conditions in which BFP reactions occur can be classified into:
- Acute BFP reactions persist for < 6 months, e.g. acute infections, injuries or inflammatory conditions
- Chronic BFP reactions last for > 6 months, e.g. SLE and other collagen diseases such as rheumatoid arthritis.
- Other conditions include lepromatous leprosy, relapsing fever, malaria, tropical pulmonary eosinophilia, viral hepatitis, infectious mononucleosis, HIV, pregnancy and IV drug abusers.
- Prozone phenomena: False negative if antibody titer in patient’s sera is high
- Sensitivity of nontreponemal tests is low in late stage of syphilis.
- Screening tests: Nontreponemal tests are used as screening tests which should be confirmed by treponemal tests.
- If treponemal tests are found positive: It confirms syphilis
- If treponemal tests are found negative: It indicates false positive nontreponemal tests.
One-Liners for Serological Tests in Syphilis
- For monitoring treatment: Ideal test is VDRL > RPR
- Primary syphilis: Most Sensitive: Western blot and EIA> TPPA > RPR > FTA-ABS
- Secondary syphilis: All tests equally sensitive (100%)
- Latent syphilis: Most Sensitive: All treponemal test
- Late syphilis: Most Sensitive: FTA-ABS > TPHA
- Overall most specific: TPHA, EIA, USR, TRUST (All 99%) > TPPA
- First test to be positive: FTA-ABS
- Rapid and mass screening: VDRL.
Diagnosis of Congenital Syphilis
Definitive diagnosis: Demonstration of T.pallidum by DGM of umbilical cord, placenta, nasal discharge, or skin lesion
Presumptive diagnosis:
- Infant born to a mother who had syphilis at the time of delivery regardless of findings in the infant and
- Reactive treponemal test in infant and
- One of the following additional criteria:
- Clinical signs/symptoms of congenital syphilis
- Abnormal CSF findings without other cause
- Reactive VDRL-CSF test
- Reactive IgM antibody test specific for syphilis (IgM FTA ABS or IgM ELISA): As IgM does not cross the placenta, its presence in neonatal serum confirms the diagnosis of congenital syphilis.
Screening of Congenital syphilis based on VDRL test (IgG):
Serial IgG in baby (VDRL):
- If maternal transfer → titer falls in 3 months,
- If Congenital infection → titer rises in 3 months Simultaneous
- VDRL test of mother and baby:
- If mother’s titer > baby’s titer → Indicates maternal transfer
- If baby’s titer > mother’s titer → Indicates congenital infection
- Sample: Baby serum (Most appropriate) > cord blood> Maternal serum
Treatment of Syphilis
- Penicillin is the drug of choice for all the stages of syphilis:
- Primary, secondary, or early latent syphilis: Single dose of Penicillin G
- Late latent CVS or benign tertiary stage: Penicillin G, single dose weekly for 3 weeks.
- Neurosyphilis or associated HIV: Aqueous crystalline or procaine penicillin G for 10–14 days.
- Alternate drug is used in patients with penicillin allergy:
- Primary, secondary, latent, CVS or benign tertiary syphilis: Tetracycline is recommended.
- Neurosyphilis or pregnancy or associated HIV: Desensitization to penicillin has to be done following which penicillin is administered.
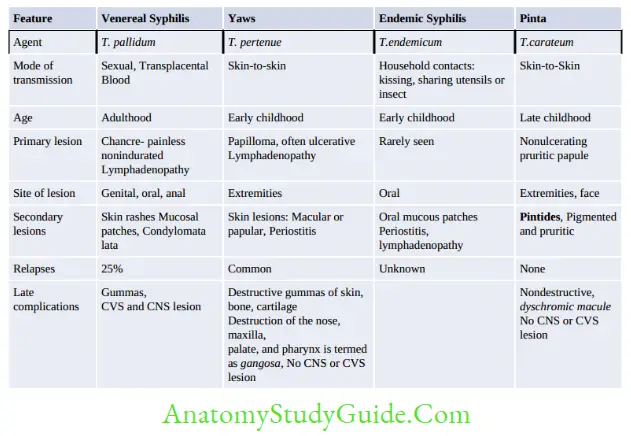
Nonvenereal Treponematoses
Endemic treponematoses can traditionally be distinguished from venereal syphilis by (Table given below):
- Mode of transmission (direct contact, not sexual)
- Age of acquisition (childhood)
- Geographic distribution (rural areas of developing nations of tropics, travellers in developed nations)
- Associated with poor hygiene
- Clinical features (described in the text)
Yaws eradication
- In 2012, WHO initiated the Yaws Eradication Strategy, also referred to as “the Morges strategy”, aiming for global eradication by 2020.
- Criteria for Eradication include absence of new indigenous case for three years and absence of evidence of transmission for 3 years, measured with sero-surveys (RPR test) among children.
- Mass treatment of azithromycin to at least 90% of the targeted at-risk population is carried out.
- India actively participated in yaws eradication programme in 1996 and has reported no new cases since 2003 and has achieved the yaws free status in the year 2016 (as declared by WHO).
Borrelia
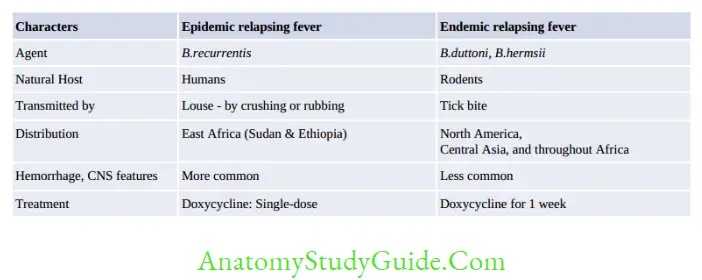
Relapsing Fever
- Relapsing fever is so named because: Alternate periods of febrile and afebrile episodes
- Reason for relapse is antigenic variation, shown by its causative agent B. recurrentis.
Lab diagnosis
- Microscopic examination of Blood:
- Wet film under dark ground or phase contrast microscope
- Giemsa and Leishman staining or QBC
- Serology (Antibody detection)
- ELISA, IFA: Not reliable, gives false positive
- GlpQ assay: It is the most reliable serological method. It is an immunoblot assay detecting antibody against the recombinant GlpQ antigen (Glycerophosphodiester phosphodiesterase).
- Animal inoculation into mice: Causes intraperitoneal infection
- Molecular methods: Multiplex Real-time PCR has been developed targeting 16SrRNA and glpQ genes
Lyme Disease
- Agent: B. burgdorferi, B. garinii and B. afzelii
- Transmission: Tick-borne (Ixodes ricinus)
- Clinical manifestation: Lyme disease occurs through four stages:
- Stage 1: Erythema migrans (annular lesions)
- Stage 2: Disseminated infection: skin lesions, meningitis, neuritis, nodal block, or joint pain.
(Neurological abnormalities: Occur in 15% of cases which include meningitis, encephalitis and a typical lymphocytic meningoradiculitis seen in cases from Europe and Asia; called as Bannwarth’s syndrome)
- Stage 3: Persistent infection: arthritis, encephalopathy or acrodermatitis.
- Post-Lyme syndrome (Chronic): Few patients present with chronic fatigue symptoms and neurocognitive manifestations, develop after months to years of infection.
- Lab diagnosis: Diagnosis mainly on clinical ground.
- Isolation from skin lesions or blood- modified Kelley’s medium
- Microscopic detection – Dark ground, phase contrasts, Immunfluroscence, silver staining
- Molecular methods:
- PCR detecting specific DNA is superior to culture in joint fluid
- Common gene targets include 16S rRNA, flaB, ospA (outer surface lipoprotein)
- PCR-RFLP (restriction fragment length polymorphism) of the intergenic rrf-rrl region has been used for genomospecies detection.
- Antibody detection:
- ELISA and western blot: First month-both IgM and IgG; later IgM disappears
- Limitations: Antibodies persist for long time and false positive in unrelated infections
- Fourfold rise of antibody is more significant
- Two test approach: CDC recommends to perform ELISA first → confirmed by western blot.
- C6 peptide IgG ELISA
- PMNs in joint fluid but lymphocytosis in CSF
- Treatment:
- For all stages except CNS and CVS infection: Oral doxycycline is the drug of choice, except for children where amoxicillin is given.
- Duration of treatment: Localized skin infection (14 days), Early disseminated infection (21 days), Acrodermatitis (30 days) and Arthritis (30–60 days).
- For CNS or CVS infection: Ceftriaxone is given for 14–28 days.
Borrelia Vincentii
- It is a commensal of mouth
- Vincent’s angina: Ulcerative gingivostomatitis (predisposing conditions such as malnutrition, viral infection).
- Often associated with fusiform bacillus (Leptotrichia which is formerly called Fusobacterium fusiformis).
- Disease is characterized by inflamed pharyngeal mucosa covered by greyish membrane resembling diphtheria, but it peels off easily
- Treatment: Penicillin and metronidazole are effective.
Leptospira
Classification
Species: Leptospira, comprises of two species:
- L. interrogans (pathogenic for humans): Causes leptospirosis or Weil’s disease involving liver and kidney.
- L. biflexa (saprophyte)
Serovars and serogroups:
- L. interrogans comprises of 26 serogroups which further consist of over 300 serovars.
- Although all serogroups and serovars are morphologically identical, produce similar clinical
picture but they differ in their geographical distribution and in severity of infection.
Genotypic Classification
- DNA hybridization, Leptospira has been classified into 17 genomic species.
- It is considered to be the gold standard techniue for species level identificationof leptospires.
- Seldom used due to its complexity.
Epidemiology
- Mode of transmission: It is zoonotic. Direct human-to-human transmission does not occur.
It is transmitted by: - Indirect contact with water, moist soil and wet surfaces contaminated with animal urine
or - Direct contact with urine and products of parturition, placenta of infected animals
- Source: Although > 100 animals can be infected; but important sources of infection are rats, dogs, cattle, and pigs.
- 3Rs: Important epidemiological determinants for leptospirosis include exposure to rodents, rainfall and rice field.
- Incidence: The incidence rate ranges from 0.1–1/100,000 per year in temperate climates to 10–100/100,000 in tropical countries. During outbreak the incidence may reach over 100/100,000.
- Global distribution: Leptospirosis is worldwide in distribution.
Highest burden has been reported from urban slums of Brazil, India and Thailand. - In India: Leptospirosis has been reported more commonly from coastal districts of Andaman and Nicobar (hence leptospirosis is also called as Andaman Hemorrhagic fever), Gujarat, Kerala, Maharashtra and Tamil Nadu followed by Andhra Pradesh, Karnataka, Dadar and Nagar Havelli, Daman and Diu, Puducherry, Goa and Odisha.
- Regional Medical Research Centre is the national leptospirosis reference centre of India, located in Portblair.
- Classic serovar: Animal associations include:
- Icterohemorrhagiae and Copenhageni in domestic rats (Rattus norvegicus, R.rattus): MC serovar in India
- Grippotyphosa in opossums and raccoons (emerging in USA)
- Canicola in dogs
- Hardjo in cattle and buffalo
- Pomona in pigs
Clinical Manifestations
The incubation period is around 10 (4–20) days. In general, the manifestations can be divided into two distinct clinical syndromes.
Mild anicteric febrile illness: Occurs in 90% of patients. It is biphasic; septicemic phase followed by immune phase
Weil’s disease (Hepato-renal-hemorrhagic syndrome): It is a severe form of icteric illness, occurs in 10% patients. Typical biphasic course may not be present. It is more severe and fulminant
Laboratory Diagnosis
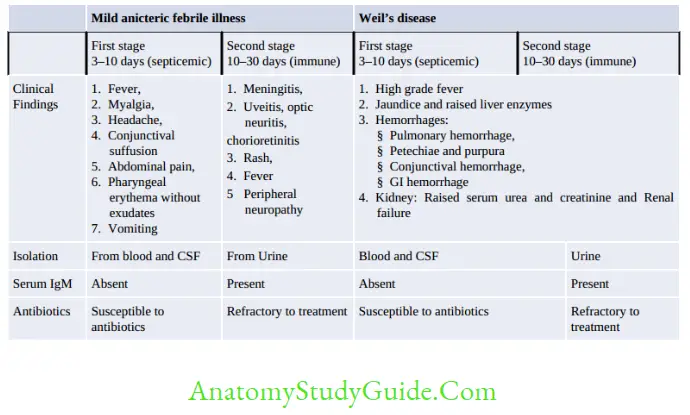
- Specimens: CSF and blood (in first 10 days of infection) and urine (between 10–30 days of infection)
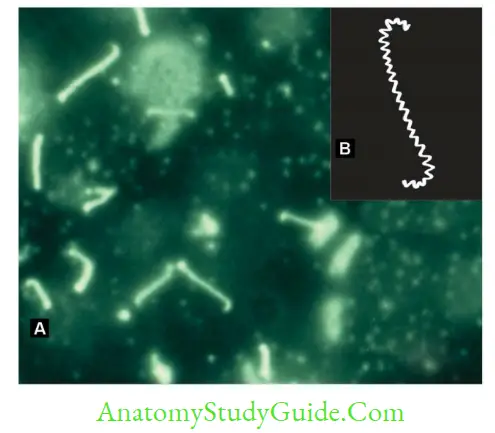
- Microscopy
- Dark ground or phase contrast microscope or silver impregnation staining:
Reveals spirally coiled bacilli (tightly and regularly coiled), with characteristic hooked ends like umbrella handle. - They are highly motile; exhibit spinning and translational movements.
- Dark ground or phase contrast microscope or silver impregnation staining:
Isolation:
- Culture condition: Leptospira is obligate aerobe and slow growing. Incubated at 30°C for 4–6 weeks
- Culture media: As Leptospira is highly fastidious, requires enriched media such as:
- EMJH medium (Ellinghausen, McCullough, Johnson, Harris) -most commonly media
- Korthof’s media with rabbit blood and Fletcher’s semisolid media
Advantages:
- Isolation confirms the diagnosis.
- Useful to maintain the stock culture of the Leptospira in the laboratories.
Disadvantages:
- Culture technique is laborious, technically demanding and time consuming.
- False positive results: It may occur due to contamination of culture media
- False negative results: It may occur due to prior antibiotics, or incubating in improper temperature and pH
Animal Inoculation: Hamsters (4–6 weeks old) and young guinea pigs
Serology for antibody detection:
- IgM antibodies appear early within one week of illness, reach peak levels in third or fourth week and then decline slowly and become undetectable within six months
- IgG antibodies appear later than IgM; reach peak level after few weeks of illness and
may persist at low level for years.
Antibody detection tests can be broadly classified into 2 types:
- Genus-specific tests: uses broadly reactive genus specific antigen prepared from nonpathogenic L. biflexa Patoc 1 strain. Various tests available are:
- Macroscopic slide agglutination test Microcapsule agglutination test (MCAT) Latex agglutination test
- ELISA: It detects IgM and IgG separately
- Lepto dipstick assay: It detects IgM antibodies
- Immunochromatographic test (ICT): It detects IgM and IgG antibodies separately.
Serovar-specific test: Microscopic agglutination test (MAT) detects antibodies against specific serovars of L. interrogans.
- It is the gold standard method and the reference test for the diagnosis of leptospirosis
Cross agglutination and absorption test (CAAT): Detects the relatedness between the strains.
Molecular methods:
- Various genes such as 16S or 23SrRNA or IS1533 insertion sequence are targeted.
- PCR detects early before seroconversion occurs. However, PCR is not serovar specific.
- PCR-RFLP or PFGE are the methods to determine the genomospecies of Leptospira.
Nonspecific findings such as: Altered renal function and liver function tests.
Treatment
- Mild leptospirosis should be treated with oral doxycycline (100 mg twice a day for 7 days). Amoxicillin can be given alternatively
- Severe leptospirosis: Penicillin is the drug of choice (1.5 million units IV, four times a day for 7 days), alternatives being ceftriaxone or cefotaxime.
Prevention
Vaccine
- Whole cell vaccines (mono- or polyvalent) containing specific serovars of Leptospira are available in many countries.
- SPIROLEPT manufactured by Sanofi-Pasteur is available for subcutaneous injection as two doses at a 15-days interval, with the third dose 4–6 month after the first dose, followed by biannual revaccination. The efficacy rate is around 60–100%.
General Measures
- Chemoprophylaxis with doxycycline-for anticipated short-term exposures, such as military training or travelling or fresh-water swimming
- General sanitation approaches including proper waste disposal
- Rodent control
- Avoidance of swimming in contaminated places
- Health education.
Leave a Reply