Vibrio
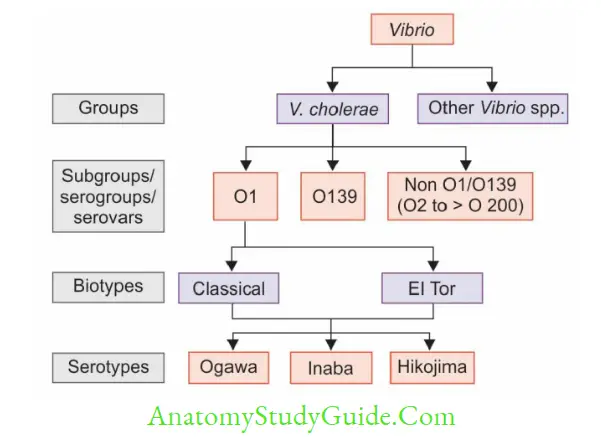
Table of Contents
Read And Learn More: Micro Biology And Immunology Notes
Classification (Gardner And Venkatraman)
Based on Salt Requirement
- Nonhalophilic vibrios: They cannot grow at higher salt concentrations.
- Examples, V. cholerae and V. mimicus
- Halophilic vibrios: Salt is their absolute requirement. They cannot grow in the absence of salt.
- They can tolerate and grow at higher salt concentration of up to 7–10%, e.g. V. parahaemolyticus, V. alginolyticus and V. vulnificus.
V.cholerae is Further Classified
- Serogrouping: Based on somatic O antigen side chain of LPS (lipopolysaccharide), V. cholerae can be grouped into more than 200 serogroups or serovars:
- O1 serogroup was responsible for all pandemics and most of the epidemics of cholera.
- Nonagglutinable (NAG vibrios) or non-cholera vibrios (NCV)- refers to non-O1 serogroups. O139 serogroup was identified in 1992 and causes cholera outbreaks India and Bangladesh.
- Non O1/O139 serogroups have occasionally caused sporadic outbreaks of diarrhea and extraintestinal manifestations, but have never caused epidemic cholera so far.
- Serotyping: O1 serogroup can be further divided into three serotypes: Inaba, Ogawa, and Hikojima; based on minor antigenic differences of O antigen:
Ogawa is the most common serotype isolated from clinical samples followed by Inaba.
- However, during epidemics, shifting between Ogawa to Inaba shift can takes place.
- Hikojima represents an unstable transitional state where both Inaba and Ogawa antigens are expressed.
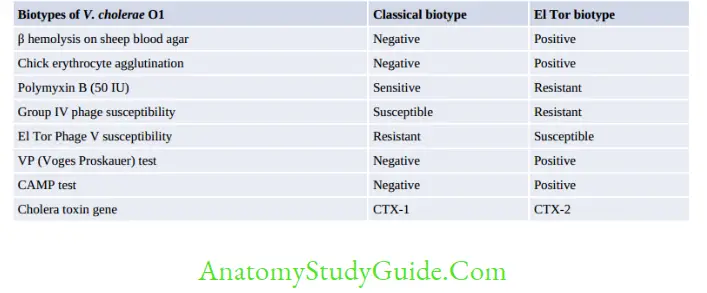
- Biotyping: Serogroup O1 has two biotypes classical and El Tor; differentiated by various biochemical reactions:
- Classical biotype was responsible for the first six pandemics of cholera.
- Currently, most of cholera cases are due to El Tor, although occasional classical isolates are still seen.
- However, some isolates do not fit in to both the biotypes and are called as El Tor variants.
- El Tor variants: Few variants of El Tor biotype have been described recently in Bangladesh and in few other places of Asia and Africa which show properties overlapping with that of the classical biotype, e.g. include:
- Matlab variants (El Tor hybrid): These strains could not be biotyped because they have a mixture of both classical and El Tor properties, were described first in Bangladesh in 2002.
- Mozambique variant (2004–2005): It has typical phenotypic properties and genome of El Tor, except that the cholera toxin and its gene (CTX) are of classical type.
Pathogenesis Of Cholera
- Pathogenesis of cholera is toxin-mediated. Both V. cholerae O1 and O139 are capable of producing cholera toxin, thus resulting in cholera:
- Transmission: Ingestion of contaminated water, or food.
- Infective dose: Being acid-labile; a high infective dose of 108 bacilli is required to bypass the gastric barrier.
- Factors promoting transmission include conditions reducing gastric acidity, such as hypochlorhydria, use of antacids.
- Crossing of the protective layer of mucus:
- In the small intestine, vibrios penetrate the mucus layer which may be achieved by
- Its highly active motility, producing mucinase and hemagglutinin protease (cholera lectin).
- Adhesion to the intestinal epithelium is facilitated by fimbria called toxin co-regulated pilus (TCP).
Cholera toxin (CT): Consists of two peptide fragments:
-
- A & B Fragment B is the binding fragment and it binds to GM1ganglioside receptors present on the intestinal epithelium
- Fragment A is the active fragment (27kDa),
- causes ADP ribosylation of G protein → upregulates the activity of adenylate cyclase → result is the intracellular accumulation of cyclic AMP.
- Increase in cyclic AMP leads to: Accumulation of sodium chloride in the intestinal lumen.
- Water moves passively into lumens leads to accumulation of isotonic fluid resulting in watery diarrhea.
- Loss of fluid and electrolytes leads to shock (due to profound dehydration) and acidosis (due to loss of bicarbonate).
- Gene for cholera toxin (CTX) is phage coded.
- ToxR gene regulates the expression of CT, TCP and other virulence factors
- Chromosomes: V. cholerae has two circular chromosomes (in contrast to most other bacteria having one chromosome)
Other virulence factors:
- Zonaoccludens toxin: Disrupts the tight junctions between mucosal cells Siderophore: Required for iron acquisition
- Bacterial endotoxin (LPS): Unlike other gram-negative bacilli, the LPS of V. cholerae does not contribute to the pathogenesis of cholera.
- However, it is immunogenic, and is included as a component in killed vaccines.
Clinical Manifestations (Cholera)
- V. cholerae O1 or O139 infection ranges from:
- Asymptomatic (75%),
- Mild diarrhea or cholera (20%),
- Explosive diarrhea (cholera gravis, in 5% of cases).
- Incubation period: Varies from 24 to 48 hours.
- Watery diarrhea: Sudden onset of painless watery diar
- Rice water stool: The stool is typically non-bilious, slightly cloudy, gray, and watery with mucus flakes but without blood or pus cells, with a fishy, inoffensive odor.
- Vomiting and muscle cramps may be present but fever is usually absent.
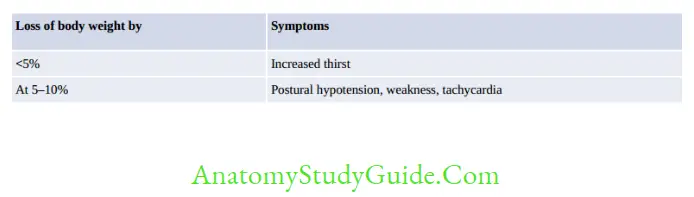
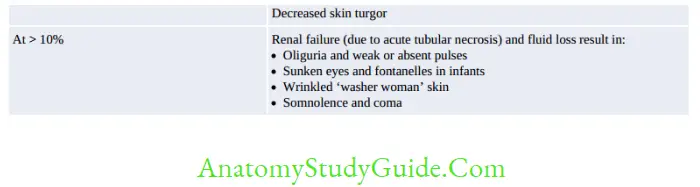
- Complications are directly proportional to the fluid loss resulting in loss of body weight.
Epidemiology
History of Pandemics
- Cholera can occur in many forms: sporadic, limited outbreaks, endemic, epidemic or pandemic.
- Home land of cholera was the delta region of the Ganges and Brahmaputra in West Bengal (India) and Bangladesh
- First six pandemics (1817 to 1923): All were caused by the classical biotype of V. cholerae
- which had spread from Bengal to involve most of the world which resulted in several thousands of deaths.
- Seventh pandemic started in 1961 and it differed from the first six pandemics by:
- It was the only pandemic that originated outside India, i.e. from Indonesia (Sulawesi, formerly Celebes Island) in 1961.
- India was affected in 1964 and the whole world was encircled by 1991.
- It was the only pandemic to be caused by El Tor biotype.
- El Tor produced a much milder cholera; with more carrier rate than the classical.
- This is due to the fact that El Tor is much hardier but less virulent than the classical vibrios.
- O139 (Bengal strain) was isolated first from Chennai in 1992.
- Since it was not agglutinated by any of the antisera available at that time (O1 to O138),
- it was designated as a new serogroup O139 or the Bengal strain.
- O139 appears to be a derivative of O1 El Tor, but differs from the latter in having a distinct LPS and being capsulated.
- Thus, it is invasive and can cause bacteremia and extraintestinal manifestations also.
- There is no cross protection between O1 and O139. Currently, O139 still causes a minority of cases in India and Bangladesh.
Current Situation
- In the world: Cholera is a notifiable disease.
- In 2016, only 1,32,121 cholera cases and 2,420 deaths were reported to WHO worldwide; out of which, 54% of cases were reported from Africa, 13% from Asia and 32% from Hispaniola.
- Several outbreaks have been recently reported from Yemen (2016-2018) Nigeria (2017), and Somalia in 2018.
- Majority of cases are due to O1 El Tor. Occasional cases may occur due to O139 and classical biotype, especially in Bangladesh.
- In India: Almost all the states have been affected Both morbidity (number of cases) and mortality (deaths) have greatly reduced.
- In 2011, about 2,341 cases were reported with 10 deaths.
- El Tor dominance continues, while O139 causes minority of cases.
Epidemiological Determinants
- Reservoir: Humans are the only reservoir. There is no animal reservoir.
- Source of infection may be either asymptomatic cases or carriers.
- Carriers are apparently healthy people who shed the bacilli in feces. Carriers may be:
- Incubatory carriers: They are less common as cholera has a short incubation period of 1–2 days.
- Convalescent carriers are the recovered patients who shed the bacilli for 2–3 weeks.
- Contact or healthy carriers result from a subclinical infection. They shed the bacilli for less than 10 days.
- Chronic carriers: Minority of convalescent carriers become chronic carriers.
- Cholera season: Maximum transmission occurs in, heavy rainfall and flooding
- Factors determining severity of the disease include:
- Lack of pre-existing immunity Persons with ‘O’ blood group are at greater risk of severe disease if infected, while those with type AB blood group are at least risk.
- Age: During inter epidemic period, all the age groups are affected equally, however during epidemics it affects more commonly children.
- Habitat: V. cholerae is a natural inhabitant of coastal sea salt water and brackish estuaries.
- Persistence of V. cholerae:
- During epidemics, it is maintained by carriers and subclinical cases.
- In inter epidemic period, it is maintained in sea water, crustaceans and planktons.
Laboratory Diagnosis
Specimens
- Freshly collected watery stool before starting the antibiotics.
- Rectal swab is preferred specimen for convalescent patients or carriers.
- Transport/Holding Media
- Venkatraman-Ramakrishnan (VR) medium
- Alkaline salt transport medium
- Cary-Blair medium
- Autoclaved sea water.
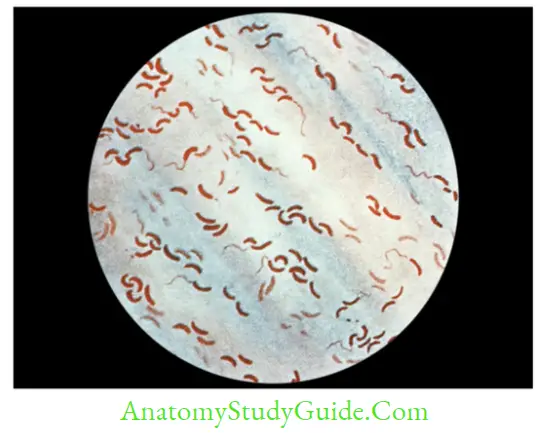
Direct Microscopy
Gram staining of fecal smear reveals short curved comma-shaped gram-negative rods, arranged in parallel rows, (fish in stream appearance) Darting motility or shooting star motility (actively motile frequently changing their direction, also seen in Campylobacter and Aeromonas).
Culture
Cultural conditions: V. cholerae is:
- Nonfastidious and strongly aerobic
- Hemodigestion on blood agar
- Growth is better in alkaline medium. The optimum pH is 8.2
- NaCl (0.5–1%) stimulates the growth, however, high concentrations of NaCl (> 6%) are inhibitory.
Culture medium:
- Enrichment broth:
- Alkaline peptone water (APW)
- Monsur’s taurocholate tellurite peptone water (pH 9.0).
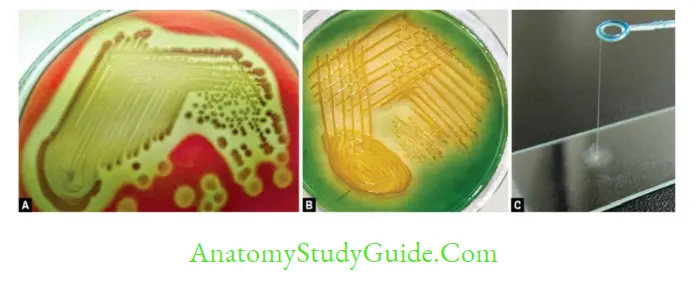
Selective media:
- Alkaline bile salt agar (BSA)
- Monsur’s gelatin taurocholate trypticase tellurite agar (GTTTA) medium
- TCBS agar (thiosulfate, citrate, bile salts, sucrose and pH of 8.6)-V. cholerae produces yellow colonies due to sucrose fermentation.
- Sucrose nonfermenters (V. mimicus and V. parahemolyticus) produce green colonies.
Biochemical Reactions
- Important biochemical properties of V. cholerae include:
- Catalase and Oxidase positive
- Indole and nitrate test positive (together called Cholera red reaction)
- String test positive
- Susceptible to O/129 (vibriostatic agent).
- Biotyping: To differentiate classical and El Tor
- Serogrouping: To differentiate O1 and O139
- Serotyping: To differentiate Ogawa, Inaba and Hikojima serotypes of serogroup O1
Treatment Of Cholera
- Fluid replacement: It is the most important measure to replace the ongoing fluid losses
- In mild to moderate fluid loss: oral rehydration solution (ORS)
- In severe cases: Intravenous fluid replacement till the consciousness arrives, thereafter replaced by ORS.
- Antibiotics: They may decrease the duration and volume of fluid loss and hastens clearance of the organism from the stool (prevents development of carrier stage)
- Drug of choice for acute infection:
- Macrolides such as erythromycin or azithromycin for adults, children and also in pregnancy.
- Alternatively, doxycycline, tetracycline or ciprofloxacin can be given
- Chemoprophylaxis: Tetracycline for 3 days or Doxycycline (single dose of 300 mg).
Vaccine
- Injectable killed vaccines: They are no longer in use. As they provide little protection, produces adverse effects.
- Oral cholera vaccines (OCV) are currently in practice.
- Two types of oral vaccines.
- Killed Whole-Cell Vaccine
- Two types: Whole cell (WC) vaccine and Whole cell recombinant B subunit cholera vaccine (WC/rBS) (Dukoral)
- Schedule: Two oral doses are given at 7 days gap. C/I to children < 2 years.
- Protection is short lived. (At 6 months, 58% for WC vaccine and 85% for WC/rBS vaccine) Children are better protected than adults.
- WHO recommends for using vaccine during epidemics in the community but not during inter epidemic period.
Oral live attenuated vaccines:
- CVD 103-HgR, Peru-15 and V. cholerae 638 for classical and/or El Tor biotypes of V. choleraeO1.
- CVD-112 and Bengal-15 vaccine trials are ongoing for V. cholerae O139.
Halophilic Vibrios
- Halophilic vibrios can withstand higher salt concentration(> 6%).
- V. parahaemolyticus
Manifestations include:
- Food-borne gastroenteritis is the MC presentation, following raw or uncooked sea food (e.g. Oyster) intake.
- It presents as watery diarrhea (MC) or rarely dysentery with abdominal cramps.
- Extraintestinal manifestations are rare, such as wound infection, otitis and sepsis.
Laboratory diagnosis: The distinct properties are:
- Morphology: It is capsulated, shows bipolar staining in fresh isolates and pleomorphism in older cultures Motile by peritrichous flagella (but does not show darting motility) On TCBS agar it produces green colonies (sucrose nonfermenter)
- Kanagawa phenomenon: It causes β hemolysis on Wagatsuma agar (a special type of high salt blood agar)
- Swarming on blood agar Urease test is positive in few strains Salt tolerance test: It can resist maximum of 8% NaCl.
- V. vulnificus
-
- Also called (L+) Vibrio as it is the only vibrio that ferments lactose. It produces the most severe infection of all vibrios.
- Primary sepsis usually occurs in patients with underlying liver disease and iron overload or rarely in renal insufficiency and immunosuppression.
- Primary wound infection
- Occasionally, it may cause gastroenteritis.
- V. alginolyticus
-
- V. alginolyticus can occasionally cause eye, ear, and wound infections.
- Few cases of otitis externa, otitis media, and conjunctivitis have been reported.
- It rarely causes bacteremia in immunocompromised hosts.
- It is the most salt-tolerant Vibrio and can grow at salt concentrations of > 10%.
Leave a Reply