Arterial Blood Pressure Definitions And Normal Values
Arterial blood pressure is defined as the lateral pressure exerted by the contained column of blood on the wall of arteries. The pressure is exerted when the blood flows through the arteries. Generally, the term ‘blood pressure’ refers to arterial blood pressure.
Table of Contents
Arterial blood pressure is expressed in four different terms:
- Systolic blood pressure
- Diastolic blood pressure
- Pulse pressure
- Mean arterial blood pressure.
Read And Learn More: Medical Physiology Notes
1. Systolic Blood Pressure
Systolic blood pressure (systolic pressure) is defined as the maximum pressure exerted in the arteries during systole of the heart.
The normal systolic pressure is 120 mm Hg. It ranges between 110 and 140 mm Hg.
2. Diastolic Blood Pressure
Diastolic blood pressure (diastolic pressure) is defined as the minimum pressure in the arteries during the diastole of the heart.
The normal diastolic pressure is 80 mm Hg. It varies between 60 and 80 mm Hg.
3. Pulse Pressure
Pulse pressure is the difference between systolic pressure and diastolic pressure.
Normally, it is 40 mm Hg.
4. Mean Arterial Blood Pressure
It is the average pressure existing in the arteries. It is not the arithmetic mean of systolic and diastolic pressures.
It is the diastolic pressure plus one-third of the pulse pressure. To determine the mean pressure, the diastolic pressure is considered more than the systolic pressure.
It is because the diastolic period of the cardiac cycle is longer (0.53 seconds) than the systolic period (0.27 seconds). Normal mean arterial pressure is 93 mm Hg (80 + 13 = 93).
Variations
Blood pressure is altered in physiological and pathological conditions. Systolic pressure is subjected to variations easily and quickly and its variation occurs in a wider range.
Diastolic pressure is not subjected to easy and quick variations and its variation occurs in a narrow range.
The diastolic pressure in different ages:
- At puberty: 80 mm Hg
- At 50 years: 85 mm Hg
- At 70 years: 90 mm Hg
- At 80 years: 95 mm Hg
2. Sex
In females, up to the period of menopause, the arterial pressure is low (up to 5 mm Hg) as compared to the males of the same age.
After menopause, the pressure in females becomes equal to that in males of the same age.
3. Body Built
The pressure is more in obese persons than in lean persons.
4. Diurnal Variation
In the early morning, the pressure is slightly low. It gradually increases and reaches the maximum at noon. It becomes low in the evening.
5. After Meals
The arterial Hood pressure is increased for a few hours after to increase in cardiac output.
6. During Steep
Usually, the pressure is reduced up to 15-20 mm Hg during deep sleep. However, it increases slightly during sleep associated with dreams.
7. Emotional Conditions
During excitement or anxiety, the blood pressure is increased due to the release of adrenaline.
8. After Exercise
After moderate exercise, systolic pressure increases by 20-30 mm Hg above the basal level due to an increase in the force of contraction and stroke volume.
Normally, diastolic pressure is not affected by moderate exercise. It is because the diastolic pressure depends upon peripheral resistance, which is not altered by moderate exercise.
After severe muscular exercise, the systolic pressure rises by 40-50 mm Hg above the basal level.
But, the diastolic pressure reduces because the peripheral resistance decreases in severe muscular exercise.
Pathological Variations
Pathological variations of arterial blood pressure are hypertension and hypotension.
Determinants Of Arterial Blood Pressure – Factors Maintaining Arterial Blood Pressure
There are some factors necessary for the maintenance of normal blood pressure, which are called local factors, mechanical factors, or determinants of blood pressure.
These factors are divided into two types:
Central factors which are pertaining to the heart:
- Cardiac output
- Heart rate
Peripheral factors which are pertaining to blood and blood vessels:
- Peripheral resistance
- Blood volume
- Venous return
- Elasticity of blood vessels
- The velocity of blood flow
- Diameter of blood vessels
- Viscosity of blood.
Central Factors
1. Cardiac Output
Systolic pressure is directly proportional to cardiac output. Whenever the cardiac output increases, the systolic pressure is increased and, when cardiac output is less, the systolic pressure is reduced.
The cardiac output increases in muscular exercise, emotional conditions, etc.
So in these conditions, the systolic pressure is increased. In conditions like myocardial infarction, the cardiac output decreases resulting in a fall in systolic pressure.
Cardiac output is the product of stroke volume and heart rate. Cardiac output in turn depends upon blood volume, venous return, heart rate, and force of contraction.
Cardiac output is directly proportional to blood volume. When blood volume increases, the ventricular filling is more, cardiac output is more and pressure rises.
When the blood volume is reduced, the cardiac output is less and blood pressure falls.
Cardiac output is also directly proportional to venous return. When the amount of blood returning to the heart is more, the ventricular filling is more with distention of the heart.
As per Frank Starling’s law, the force of contraction of the heart is directly proportional to the initial length of muscle fibers.
So, when the force of contraction is more, cardiac output is more and the systolic pressure rises.
2. Heart Rate
Moderate changes in heart rate do not affect arterial blood pressure much.
However, marked alteration in the heart rate affects the blood pressure by altering cardiac output.
Peripheral Factors
3. Peripheral Resistance
This is the important factor, which maintains diastolic pressure. The diastolic pressure is directly proportional to peripheral resistance.
It is the resistance offered to the blood flow at the periphery. The resistance is offered at arterioles, which are called the resistant vessels.
When peripheral resistance increases, diastolic pressure is increased and when peripheral resistance decreases, the diastolic pressure is decreased.
The other details of peripheral resistance.
4. Blood Volume
Blood pressure Is directly proportional to blood volume. Blood volume maintains the blood pressure through the venom return end cardiac output.
If the blood volume increases, there Is an increase in venous return and rartNac output, resulting in elevation of blood pressure.
Blood pressure increases in polycythemia vera because (A increased blood volume.
The decrease in blood volume causes a fall in blood pressure because of reduced cardiac output.
It occurs in conditions like diarrhea, vomiting, and other conditions of dehydration and hemorrhage.
5. Venous Return
Blood pressure is directly proportional to venous return. When venous return increases, there is an increase in ventricular filling and cardiac output resulting in elevation of arterial blood pressure.
The venous return depends upon the muscle pump and respiratory pump. The details of venous return.
6. Elasticity of Blood Vessels
Blood pressure is inversely proportional to the elasticity of blood vessels.
Due to the elastic property, the blood vessels are distensible and are able to maintain pressure.
When the elastic property is lost, the blood vessels become rigid (arteriosclerosis) and pressure increases as in old age.
The deposition of cholesterol, fatty acids, and calcium ions produces rigidity of blood vessels and atherosclerosis leading to increased blood pressure.
7. Velocity of Blood Flow
The pressure in a blood vessel is directly proportional to the velocity of blood flow.
If the velocity of the blood flow increases, the resistance is increased. So, the pressure is increased.
8. Diameter of Blood Vessels
The arterial blood pressure is inversely proportional to the diameter of the blood vessel.
If the diameter decreases, the peripheral resistance increases leading to an increase in the pressure.
The blood vessels, especially the arterioles are always in a partially constricted state because of the vasomotor tone.
The vasomotor tone is the continuous stream of impulses that are produced by the vasomotor center, reaching the blood vessels through the vasomotor nerves.
These impulses cause vasoconstriction and increase the pressure.
9. Viscosity of Blood
Arterial blood pressure is directly proportional to the viscosity of blood.
When the viscosity of blood increases, the frictional resistance is increased and this increases the pressure.
In polycythemia and the increased amount of plasma proteins, the viscosity of blood is increased causing an increase in blood pressure. In anemia, the viscosity of blood is less. This decreases the blood pressure.
Regulation Of Arterial Blood Pressure
Arterial blood pressure varies even under physiological conditions. However, immediately it is brought back to a normal level because of the presence of well-organized regulatory mechanisms in the body.
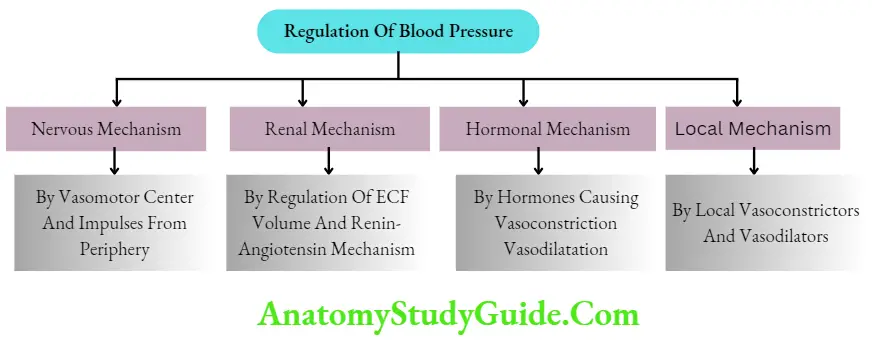
The body has four such regulatory mechanisms to maintain blood pressure within normal limits:
- Nervous mechanism or short-term regulatory mechanism
- A renal mechanism or long-term regulatory mechanism
- Hormonal mechanism
- Local mechanism.
Nervous Mechanism For Regulation Of Blood Pressure – Short-Term Regulation
Nervous regulation is rapid among all the mechanisms involved in the regulation of arterial blood pressure.
When arterial blood pressure alters, the nervous system brings the pressure back to normal within a few minutes.
Although the nervous mechanism is quick in action, it operates only for a short period and then it adapts to the new pressure. Hence, it is called short-term regulation.
The nervous mechanism regulating arterial blood pressure operates through the vasomotor system,
Vasomotor System
The vasomotor system includes three components:
- Vasomotor center
- Vasoconstrictor fibers
- Vasodilator fibers.
Vasomotor Center
The vasomotor center is bilaterally situated in the reticular formation of the medulla oblongata and the lower part of the pons.
The Vasomotor center consists of three areas:
- Vasoconstrictor area
- Vasodilator area
- Sensory area.
- Vasoconstrictor area
It is also called the pressor area. It forms the lateral portion of the vasomotor center.
The vasoconstrictor area sends impulses to blood vessels through sympathetic vasoconstrictor fibers.
So the stimulation of this area causes vasoconstriction and a rise in arterial blood pressure.
This area is also concerned with the acceleration of heart rate.
Vasodilator area
It is otherwise called a depressor area. It forms the medial portion of the vasomotor center.
This area suppresses the vasoconstrictor area and causes vasodilatation. It is also concerned with cardioinhibitory.
Sensory area
It is in the nucleus of tractus solitaries which is situated in the posterolateral part of the medulla and pons.
This area receives sensory impulses via glossopharyngeal and vagal nerves from the periphery, particularly, from the baroreceptors.
The sensory area in turn, controls the vasoconstrictor and vasodilator areas.
2. Vasoconstrictor Fibers
The vasoconstrictor fibers belong to the sympathetic, division of the autonomic nervous system These fit cause vasoconstriction by the release of the transmitter substance, noradrenaline.
The noradrenalin acts through alpha receptors of smooth muscle fiber: in blood vessels.
Vasoconstrictor fibers play a major role than vasodilator fibers in the regulation of blood pressure.
Vasomotor Tone
The vasomotor tone is the continuous discharge of impulses from the vasoconstrictor center through the vasoconstrictor fibers.
The vasomotor tone plays an important role in regulating the pressure by producing a constant partial state of constriction of the blood vessels.
Thus, arterial blood pressure is directly proportional to vasomotor tone.
The vasomotor tone is also called sympathetic vasoconstrictor tone or sympathetic tone.
3. Vasodilator Fibers
Vasodilator fibers are of three types:
- Parasympathetic vasodilator fibers
- Sympathetic vasodilator fibers
- Antidromic vasodilator fibers.
- Parasympathetic vasodilator fibers
These vasodilator fibers cause dilatation of blood vessels by releasing the chemical mediator, acetylcholine.
Sympathetic vasodilator fibers
Some of the sympathetic fibers cause vasodilatation in certain areas by secreting acetylcholine Such fibers are called sympathetic vasodilator or sympathetic cholinergic fibers.
The sympathetic cholinergic fibers, which supply the blood vessels of skeletal muscles are important in increasing the blood flow to muscles by vasodilatation during conditions like exercise.
The cholinergic sympathetic vasodilator fibers form an important part of the vasomotor system The signals for the vasodilator fibers are generated in the cerebral cortex The signals are relayed through the fibers from the cerebral cortex to the lateral grey horn of the spinal cord via the hypothalamus, midbrain, and medulla.
In the spinal cord, these impulses activate the preganglionic sympathetic fibers.
These fibers in turn activate the postganglionic fibers. The postganglionic fibers cause dilatation of blood vessels by secreting acetylcholine.
Antidromic vasodilator fibers
Normally, the impulses produced by a cutaneous receptor am receptor) pass through sensory nerve fibers these impulses pass through the other icon in the opposite direction and reach: supplied by these branches.
These dilate the blood vessels. It is called the .ixon reflex. And, the nerve fibers are called vasodilator fibers.
Mechanism Of Action Of Vasomotor Center In The Regulation Of Blood Pressure
The vasomotor center regulates arterial blood pressure by causing vasoconstriction or vasodilatation.
However, its actions depend upon the impulses it receives from other structures such as baroreceptors, chemoreceptors, higher centers, and respiratory centers.
Among these structures, baroreceptors and chemoreceptors play a major role in the short-term regulation of blood pressure.
1. Baroroccptor Mechanism
The baroreceptors are the receptors, which give a response to changes in blood pressure. The baroreceptors are also called pressoreceptors.
Situation
Baroreceptors are situated in the carotid sinus and wall of the aorta
Nerve supply Functions
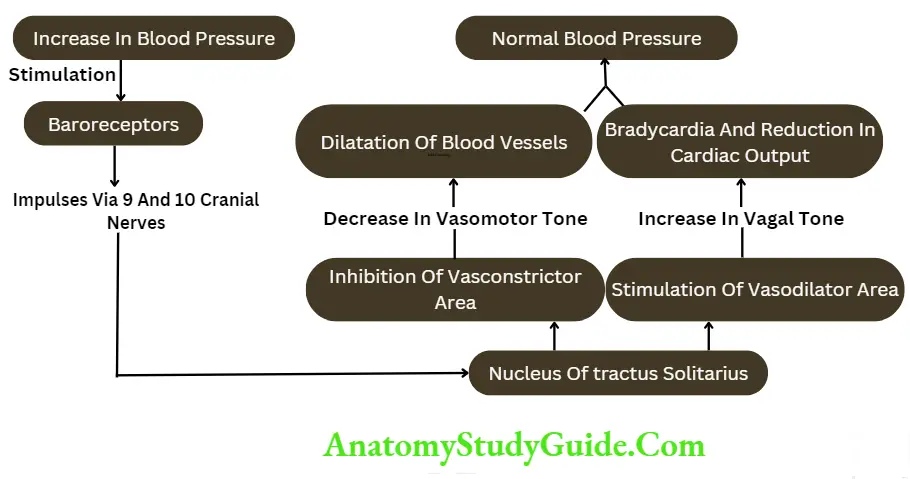
- When blood pressure increases: When arterial blood pressure rises rapidly, the baroreceptors are activated which in turn send stimulatory impulses to nucleus of tractus solitarius.
- Now, the nucleus of tractus solitarius acts on both the vasoconstrictor area and vasodilator areas of the vasomotor center.
- It inhibits the vasoconstrictor area and excites the vasodilator area.
- The inhibition of the vasoconstrictor area reduces vasomotor tone. Reduction in vasomotor tone causes vasodilatation resulting in decreased peripheral resistance.
- The simultaneous excitation of the vasodilator center increases vagal tone.
- This decreases the rate and force of contraction of heart leading to a reduction in cardiac output.
- These two factors, i.e. decreased peripheral resistance and reduced cardiac output bring the arterial blood pressure back to normal level.
- When blood pressure decreases: The fall in arterial blood pressure or the occlusion of common carotid arteries decreases the pressure in the carotid sinus.
- This causes the inactivation of baroreceptors. Now, there is no inhibition of the vasoconstrictor center or excitation of the vasodilator center. Therefore, the blood pressure rises.
- The information regarding blood pressure within the range of 50-200 mm Hg (mean arterial pressure) reaches the vasomotor center through the carotid baroreceptors.
- The information about the blood pressure range of 100200 mm Fig goes through the aortic baroreceptors.
- Both carotid and aortic baroreceptors are stimulated by the rising pressure than the steady pressure and their response depends upon the rate of increase in the blood pressure.
- Since the baroreceptor mechanism acts against the rise in arterial blood pressure it is called pressure buffer mechanism or system and, the nerves from baroreceptors are called the buffer nerves.
2. Chemoreceptor Mechanism
Chemoreceptors are the receptors giving response to a change in chemical constituents of blood. Peripheral chemoreceptors influence the vasomotor center.
Chemoreceptor Mechanism Situation
The peripheral chemoreceptors are situated in the carotid body and aortic body.
Nerve Supply Function
- Civceptors are sensitive to lack of oxygen, excess of o on dioxide, and hydrogen ion concentration in blood.
- Whenever blood pressure decreases, the blood flow decreases resulting in decreased oxygen content and excess of carbon dioxide and hydrogen ions.
- These factors stimulate the chemoreceptors, which send impulses to excite the vasoconstrictor center.
- The blood pressure rises and blood flow increases. Chemoreceptors play a major role in maintaining respiration rather than blood pressure.
Sinoaortic mechanism
The mechanism of action of baroreceptors and chemoreceptors in the carotid and aortic region constitute a sinoaortic mechanism.
The nerves from the baroreceptors and chemoreceptors are called buffer nerves because these nerves regulate the heart rate (Chapter 101), blood pressure, and respiration.
3. Higher Centers
The vasomotor center is also controlled by the impulses from the two higher centers in the brain.
Cerebral cortex
Area 13 in the cerebral cortex is concerned with emotional reactions. During emotional conditions, this area sends impulses to the vasomotor center. The vasomotor center is activated, the vasomotor tone is increased and the pressure rises.
Hypothalamus
Stimulation of posterior and lateral nuclei of the hypothalamus causes vasoconstriction and an increase in blood pressure. Stimulation of the preoptic area causes vasodilatation and a decrease in blood pressure. The impulses from the hypothalamus are mediated via the vasomotor center.
4. Respiratory Centers
During the beginning of expiration, arterial blood pressure increases slightly, i.e. by 4-6 mm Hg.
And it decreases during the later part of expiration and during inspiration. It is because of two factors:
- Radiation of impulses from respiratory centers towards the vasomotor center at different phases of the respiratory cycle
- Pressure changes in the thoracic cavity lead to alteration of venous return and cardiac output.
Renal Mechanism For Regulation Of Blood Pressure – Long-Term Regulation
- The kidneys play an important role in the long-term regulation of arterial blood pressure.
- When blood pressure alters slowly over several days/months/years, the neural mechanism adapts to the altered pressure and loses sensitivity to the changes.
- It cannot regulate the pressure anymore. In such conditions, the renal mechanism operates efficiently to regulate blood pressure. Therefore, it is called long-term regulation.
Kidneys regulate arterial blood pressure in two ways:
- By regulation of ECF volume
- Through the renin-angiotensin mechanism.
By Regulation Of Extracellular Fluid Volume
- When the blood pressure increases, kidneys excrete large amounts of water and salt, particularly sodium by means of pressure diuresis and pressure natriuresis.
- Pressure diuresis is the excretion of a large quantity of water in urine because of increased blood pressure.
- Even a slight increase in blood pressure doubles the water excretion. Pressure natriuresis is the excretion of a large quantity of sodium in the urine.
- Because of diuresis and natriuresis, there is a decrease in the ECF volume and blood volume, which in turn brings the arterial blood pressure back to normal blood pressure decreases, and the reabsorption of Yinwr burn renal tubules is increased.
- This in turn hCF volume, blood volume and cardiac output resub b? kt restoration of blood pressure.
Through Renin-Angiotensin Mechanism
The details about the source of renin secretion, formation of angiotensin, and conditions when renin is secreted.
Actions of Angiotensin
When blood pressure and ECF volume decrease, renin secretion from the kidneys is increased.
It converts angiotensinogen into angiotensin I. This is converted into angiotensin 1 by ACE (angiotensin-converting enzyme).
Angiotensin 2 acts in two ways to restore blood pressure:
- It causes constriction of arterioles in the body so that the peripheral resistance is increased, and blood pressure rises.
- In addition, angiotensin 2 causes constriction of afferent arterioles in kidneys so that the glomerular filtration reduces.
- This results in the retention of water and salts. This increases ECF volume to a normal level. This in turn increases the blood pressure to a normal level.
- Simultaneously, angiotensin 2 stimulates the adrenal cortex to secrete aldosterone.
- This hormone increases the reabsorption of sodium from renal tubules. Sodium reabsorption is followed by water reabsorption resulting in increased ECF volume and blood volume.
- It increases the blood pressure to a normal level.
Actions of Angiotensin 3 and Angiotensin 4
Like angiotensin 2 angiotensins 3 and 4 also increase blood pressure and stimulate the adrenal cortex to secrete aldosterone.
Hormonal Mechanism For Regulation Of Blood Pressure
Hormones
Many hormones are involved in the regulation of blood pressure.
Hormones, which increase the blood pressure:
- Adrenaline
- Noradrenaline
- Thyroxine
- Aldosterone
- Vasopressin
- Angiotensin
- Serotonin.
Hormones, which decrease the blood pressure:
- A vasoactive intestinal polypeptide (VIP)
- Bradykinin
- Prostaglandin
- Histamine
- Acetylcholine
- Atrial natriuretic peptide
- Brain natriuretic peptide
- C-type natriuretic peptide.
1. Adrenaline
Adrenaline is secreted by the adrenal medulla. It is also released by sympathetic postganglionic nerve endings.
- Adrenaline regulates blood pressure by acting through the heart and blood vessels.
- It increases systolic pressure by increasing the force of contraction of the heart and cardiac output.
- It decreases diastolic pressure by reducing the total peripheral resistance.
- Adrenaline causes constriction of blood vessels through alpha receptors. It also causes dilatation of blood vessels through (32 receptors in some areas of the body like skeletal muscle, liver, and heart.
- So, the total peripheral resistance is reduced leading to a decrease in diastolic pressure.
2. Noradrenaline
- Noradrenaline is secreted by the adrenal medulla. It is also released by sympathetic postganglionic nerve endings.
- Noradrenaline increases diastolic pressure due to its general vasoconstrictor effect.
- It has stronger effects on blood vessels than on the heart. It causes constriction of all blood vessels throughout the body via alpha receptors.
- So it is called a “General vasoconstrictor”. The action of noradrenaline is to increase the total peripheral resistance and diastolic pressure.
- It also increases the systolic pressure slightly, by increasing the force of contraction of the heart.

3. Thyroxine
- Thyroxine secreted from the thyroid gland increases systolic pressure but decreases diastolic pressure.
- It increases the systolic pressure by increasing cardiac output. The cardiac output is increased because of an increase in the blood volume and force of contraction of the heart.
- The action of thyroxine on diastolic pressure is indirect. Due to increased metabolic activity by thyroxine, large quantities of metabolites are produced.
- These metabolites cause vasodilatation and so the peripheral resistance is reduced. It decreases the diastolic pressure.
- Because of the actions of thyroxine, generally, the mean arterial pressure is not altered.
- Systolic pressure is increased and the diastolic pressure is decreased. So, only the pulse pressure increases.
4. Aldosterone
Aldosterone is secreted from the adrenal cortex. It causes retention of sodium and water and thereby increases the ECF fluid volume and blood volume leading to an increase in blood pressure.
Thus, an increase in the secretion of aldosterone increases the blood pressure by increasing the blood volume.
5. Vasopressin
Vasopressin or ADH which is secreted posterior pituitary has a potent action on the blood vessels, particularly the arteries.
It causes constriction of the arteries in all parts of the body. Due to the vasoconstriction, the blood pressure is increased.
However, the amount of this hormone required to cause the vasopressor effect is very much high than the amount required to cause the antidiuretic effect.
6. Angiotensins
Angiotensin 2, 3, and 4 which are obtained from angiotensinogen cause constriction of systemic arterioles and elevate blood pressure.
7. Serotonin
It is otherwise known as 5-hydroxytryptamine. Serotonin is secreted from many sources. It produces vasoconstriction and an increase in blood pressure.
8. Vasoactive Intestinal Polypeptide (VIP)
This polypeptide is secreted in the stomach and small intestine. A small amount of this hormone is also secreted in the large intestine.
VIP is a vasodilator and causes dilatation of peripheral blood vessels and a decrease in blood pressure.
9. Bradykinin
Bradykinin is produced in blood during the conditions like inflammation. During such conditions, the enzyme in the blood called kallikrein is activated.
It acts on a2 globulin to form kallidin, which is converted into bradykinin.
Bradykinin is a vasodilator substance and causes a reduction in blood pressure.
10. Prostaglandins
$rrdin PGE2 is a vasodilator substance. It is from almost all tissues of the body. it decreases blood pressure.
11. Histamine
It is secreted in nerve endings of the hypothalamus, limbic cortex, and other parts of the cerebral cortex.
Histamine is also released from tissues during allergic conditions, inflammation, or damage. Histamine causes vasodilatation and decreases the blood pressure.
12. Acetylcholine
It is the cholinergic neurotransmitter released from many sources. Acetylcholine causes vasodilatation and decreases blood pressure.
13. Atrial Natriuretic Peptide
Atrial natriuretic peptide (ANP) is a hormone secreted by the atrial musculature of the heart. It causes dilatation of blood vessels and decreases the blood pressure.
14. Brain Natriuretic Peptide
hormone also causes dilatation of blood vessels and decreases blood pressure.
15. C-type Natriuretic Peptide
C-type natriuretic peptide (CNP) is secreted by several tissues including the myocardium and vascular endothelium.
CNP decreases blood pressure through vasodilatation.
Local Mechanism For Regulation Of Blood Pressure
In addition to nervous, renal and hormonal mechanisms, some local substances also regulate blood pressure.
The local substances regulate the blood pressure by vasoconstriction or vasodilatation.
Local Vasoconstrictors
The local vasoconstrictor substances are of vascular endothelial origin and are known as endothelins (ET).
Endothelins are peptides with 21 amino acids. Three types of endothelins ET1, ET2, and ET3 are identified so far.
Endothelins are produced by the stretching of blood vessels. These peptides act by activating phospholipase, which in turn activates the prostacyclin and thromboxane A2. These two substances cause constriction of blood vessels and an increase in blood pressure.
Local Vasodilators
The local vasodilators are of two types:
- Vasodilators of metabolic origin
- Vasodilators of endothelial origin.
Vasodilators of Metabolic Origin
The vasodilators of metabolic origin are carbon dioxide, lactate, hydrogen ions, and adenosine.
Vasodilators of Endothelial Origin
Nitric oxide (NO) is an endothelium-derived relaxing factor (EDRF). It is synthesized from arginine.
The production is stimulated by acetylcholine, bradykinin, VIP, substance P, and platelet breakdown products.
As nitric oxide is a vasodilator, deficiency of this leads to hypertension.
The other functions of nitric oxide are penile erection with vasodilatation and engorgement of corpora cavernosa, activation of macrophages in the brain, destruction of cancer cells, and relaxation of smooth muscles of the gastrointestinal tract.
There are three types of nitric oxide L namely, N03 (nitric oxide), NO+ (nitrosonium cation), and l NO” (nitroxyl anion).
Measurement Of Arterial Blood Pressure
Blood pressure was first measured in horses in 1733, by Stephen Hales with a long tube of about 9 feet in length.
Later, Poiseuille reduced the length of the tube to one foot and used mercury to balance the column of blood.
In 1847, Ludwig placed a float on the top of the mercury column and made continuous recording possible.
The introduction of rubber tubing, anesthesia, and manometer enabled the accurate measurement of blood pressure. Blood pressure is measured by two methods:
- Direct method
- Indirect method.
Measurement Of Arterial Blood Pressure Direct Method
The direct method to measure arterial blood pressure is employed only in animals.
The animal is given suitable anesthesia, then the neck is opened and a tracheal cannula is inserted into the trachea.
This tracheal cannula is connected to a respiratory pump so that the respiration in the animal is controlled artificially to avoid any disturbance during the experimental procedure.
A venous cannula is inserted through the femoral vein. It is used to infuse saline to compensate for blood loss during experimental procedures.
The carotid artery is cannulated and connected to a mercury manometer. By using a kymograph, the blood pressure can be recorded continuously in the form of a graph.
The cannula inserted into the carotid artery can also be connected to an electronic pressure transducer, which in turn is connected to a recording device like a polygraph to obtain the recordings.
Measurement Of Arterial Blood Pressure Indirect Method
The indirect method is used to measure arterial blood pressure in men as well as animals.
Measurement Of Arterial Blood Pressure Apparatus
The apparatus used to measure blood pressure in human beings is called a sphygmomanometer.
Along with a sphygmomanometer, the stethoscope is also necessary to measure blood pressure.
Measurement Of Arterial Blood Pressure Principle
When external pressure is applied over the artery, the blood flow through it is obstructed.
And, the pressure required to cause occlusion of blood flow indicates the pressure inside the vessel.
Measurement Of Arterial Blood Pressure Procedure
The brachial artery is usually chosen because of convenience. The arm cuff is tied around the upper arm above the cubital fossa. The cuff should not be too tight or too loose.
The cuff is connected to the sphygmomanometer. Now, blood pressure can be measured by three methods.
- Palpatory method
- Auscultatory method
- Oscillatory method.
1. Palpatory method
First, the radial pulse is felt. While feeling the pulse, the pressure is increased in the cuff by inflating air into it, with the help of a hand pump.
While doing this, the mercury column in the sphygmomanometer shows the pressure in the cuff.
When the radial pulse disappears, the pressure is further increased by about 20 mm Hg.
Then, the pressure in the cuff is slowly reduced by releasing the valve of the hand pump.
This is done by feeling the pulse and simultaneously watching the mercury column in the apparatus. Pressure is noted when the pulse reappears.
This pressure indicates systolic pressure. The disadvantage of this method is that the diastolic pressure cannot be measured.
2. Auscultatory method
This is the most accurate method to determine arterial blood pressure. After determining the systolic pressure in the palpatory method, the pressure in the cuff is raised by about 20 mm Hg above that level so that, the brachial artery is occluded due to compression.
Now the chest piece of the stethoscope is placed over the cubital fossa, and the pressure is released from the cuff.
While doing so, a series of sounds are heard through the stethoscope. These sounds are known as Korotkoff’s sounds named after the discoverer Korotkoff (1905).
While reducing the pressure, Korotkoff’s sounds appear in four phases.
Measurement Of Arterial Blood Pressure First phase
While decreasing the pressure from the arm cuff, the occlusion of the artery is relieved and when the blood starts flowing through the artery, the first sound appears suddenly.
In a normal person, it appears, when the pressure is reduced to 120 mm Hg.
It is a clear and tapping sound. It indicates systolic pressure. It slowly becomes louder when the pressure is reduced further by 10 mm Hg from the initial level.
Measurement Of Arterial Blood Pressure Second phase
Following the clear and taping sound, a murmuring sound is heard when the pressure is reduced further by about 15 mm Hg.
Measurement Of Arterial Blood Pressure Third phase
After the murmuring sound, a very clear and louder sound is heard. It is of gong type. It is heard while reducing the pressure by another 15 mm Hg.
Measurement Of Arterial Blood Pressure Fourth phase
Next to the gong-type sound, a mild and muffled sound is heard when the pressure is decreased further by 5 mm Hg.
It disappears afterward. The disappearance of the sound indicates diastolic pressure.
Thus, in the auscultatory method, the appearance of the clear taping sound during the first phase indicates the systolic pressure, and, the disappearance of the muffling sound shows diastolic pressure.
3. Oscillatory method
When the pressure in the arm cuff is increased above the level of systolic pressure, the artery is occluded due to compression.
At this stage, the mercury column tee mane meter remains static. When the pressure is reduced, some oscillations occur at the top mercury column.
While deflating the cuff further, the amplitude and duration of the oscillations increase suddenly.
It denotes systolic pressure. When the cuff pressure is reduced further, the amplitude and duration of the oscillations are reduced. It reflects diastolic pressure.
Because of its inaccuracy, this method is not followed in routine clinical practice.
By connecting the manometer to an appropriate recording device, the oscillations of the mercury column can be recorded graphically.
Automatic Blood Pressure Instrument
Nowadays automatic blood pressure instrument is widely used. The instrument has a microprocessor-driven air pump that automatically inflates the earmuff at a fixed pressure value.
Then, it records the pressure oscillation pattern during a stepwise deflation.
The principle of measuring pressure depends on the nonlinear properties of the brachial arterial wall, which induce nonconstant oscillations of the cuff pressure during deflation.
The sensors in the instrument detect the oscillometric waves and determine the systolic pressure, diastolic pressure, pulse pressure and mean arterial pressure. The instrument determines the pulse rate also.
The automatic instrument does not need expert personnel to measure blood pressure since it has self-measuring facilities. However, the accuracy of the oscillometric method is still controversial.
The microprocessor-controlled blood pressure monitors that are fixed around the wrist or finger are also available.
Applied Physiology
The pathological variations of arterial blood pressure are:
- Hypertension
- Hypotension.
Applied Physiology Hypertension
Applied Physiology Definition
Hypertension is defined as persistently high blood pressure. Clinically, when the systolic pressure remains elevated above 150 mm Hg and diastolic pressure remains elevated above 90 mm Hg, it is considered hypertension.
If there is increase only in systolic pressure, it is called systolic hypertension.
Types of Hypertension
Hypertension is divided into two types:
- Primary hypertension
- Secondary hypertension.
1. Primary hypertension or essential hypertension
Primary hypertension is elevated blood pressure in the absence of any underlying disease.
It is also called essential hypertension. The arterial blood pressure is increased because of increased peripheral resistance, which occurs due to some unknown cause.
Primary hypertension is of two types:
- Benign hypertension
- Malignant hypertension.
Benign hypertension: It is high blood pressure that does not cause any problems.
It is defined as essential hypertension that runs a relatively long and symptomless course.
In the early stages of this condition, there is a moderate increase in blood pressure with systolic pressure of 200 mm Hg and diastolic pressure of about 100 mm Hg.
However, in resting conditions and sleep, the blood pressure returns to normal level.
Later, there is further increase in blood pressure and it does not come back to normal level in resting conditions.
The persistent increase in pressure over the years causes the development of vascular, cardiac, or renal diseases.
Malignant hypertension: It is a severe form of hypertension with a rapid course leading to progressive cardiac and renal diseases. It is also called accelerated hypertension.
In this case, the blood pressure is elevated to a great extent. Systolic pressure rises to about 250 mm Hg and diastolic pressure rises to 150 mm Hg.
It is always developed due to the combined effects of primary and secondary hypertension.
Malignant hypertension causes severe damage to the tunica intima of small blood vessels and organs like the eye (retina), heart, brain, and kidneys. It is a fatal disease since it causes death within a few years.
2. Secondary hypertension
Secondary hypertension is high blood pressure due to some underlying disorders.
The different forms of secondary hypertension are:
- Cardiovascular hypertension: It is produced due to cardiovascular disorders such as:
- Atherosclerosis – hardening of blood vessels due to fat deposition
- Coarctation of the aorta – narrowing of the aorta.
Endocrine hypertension: It is developed because of hyperactivity of some endocrine glands:
- Pheochromocytoma – tumor in the adrenal medulla
- Hyperaldosteronism – excess secretion of aldosterone from the adrenal cortex
- Cushing’s syndrome – excess secretion of glucocorticoids from the adrenal cortex.
Renal hypertension: The renal diseases causing hyphens son are:
- Stenosis of renal arteries
- Tumor of juxtaglomerular cells leading to the formation of excess angiotensin 2
- Glomerulonephritis.
Neurogenic hypertension:
The nervous disorders, which produce hypertension are:
- Increased intracranial pressure
- The lesion in tractus solitarius
- Sectioning of nerve fibers from carotid sinus.
Hypertension during pregnancy: Some pregnant women develop hypertension because of toxemia during pregnancy.
The arterial blood pressure is elevated by the low glomerular filtration rate and retention of sodium and water.
It may be because of some autoimmune processes during pregnancy or the release of some vasoconstrictor agents from the placenta or the excessive secretion of hormones causing a rise in blood pressure.
Hypertension is associated with convulsions in eclampsia.
Experimental Hypertension
Hypertension can be produced in experimental animals by various methods. These methods correlate with the causes of hypertension in human beings.
Experimental hypertension can be produced by the following methods:
- Clamping the renal artery
- Denervation of baroreceptors in the carotid sinus and aortic arch
- Injections of corticosteroids
- Infusion of salt with aldosterone.
Goldblatt hypertension: It is one of the experimental hypertension produced in dogs by Goldblatt and it is named after him. He removed one kidney of the dog and clamped the artery of the other kidney.
It produced a slow and steady increase in arterial pressure. The elevation of blood pressure was due to excessive secretion of renin from the intact kidney leading to the formation of a large quantity of angiotensin
It is known as ‘one kidney’ Goldblatt hypertension. Hypertension is also developed when the artery of one kidney is clamped without doing anything with the kidney on the other side.
It is called ‘two kidneys’ Goldblatt hypertension. It is due to the renin-angiotensin mechanism and retention of salts.
Manifestations of Hypertension
Severe manifestations of primary hypertension:
- Renal failure
- Left ventricular failure
- Myocardial infarction
- Cerebral hemorrhage
- Retinal hemorrhage.
Treatment of Hypertension
Secondary hypertension is cured by treating the disease-causing hypertension.
Primary hypertension can be controlled but cannot be cured. It is controlled by different types of antihypertensive drugs.
1. Beta adrenoceptor blockers: The beta-adrenoceptor blockers or beta antagonists (adrenergic beta blockers or beta blockers) block the effect of sympathetic nerves on heart and blood vessels by binding with beta-adrenoceptors, so that, there is a reduction in cardiac output and inhibition of vasoconstriction leading to fall in blood pressure.
2. Alpha adrenoceptor blockers: The alpha-adrenoceptor blockers or alpha antagonists (adrenergic alpha blockers or alpha-blockers) block the effect of sympathetic nerves on blood vessels by binding with alpha adrenoceptors leading to vasodilatation and a fall in blood pressure.
3. Calcium channel blockers: These drugs block the In my calcium and thereby, reduce 11 y of myocardium. It causes a decrease m cardiac output and a fall in blood pressure.
4. Vasodilators: These agents reduce blood pressure by causing vasodilatation.
- Primary hypotension
- Secondary hypotension.
1. Primary hypotension
- Primary hypotension is low blood pressure that develops in the absence of any underlying disease and develops due to some unknown cause.
- It is also called essential hypotension. Frequent fatigue and weakness are the common symptoms of this condition.
- However, persons with primary hypotension are not easily susceptible to heart or renal disorders.
2. Secondary hypotension
It is the hypotension that occurs due to some underlying diseases.
The diseases which cause hypotension are:
- Myocardial infarction
- Hypoactivity of the pituitary gland
- Hypoactivity of adrenal glands
- Tuberculosis
- Nervous disorders.
Orthostatic hypotension
- Orthostatic hypotension is the sudden fall in blood pressure while standing for some time.
- It is due to the effect of gravity. It develops in persons affected by myasthenia gravis or some nervous disorders like tabes dorsalis, syringomyelia, and diabetic neuropathy.
- The common symptom of this condition is orthostatic syncope. The syncope.
Leave a Reply