Basic Paediatric Medicine Introduction
Children are not miniature adults. The organ systems of children are significantly different from those of adults. It is necessary to understand the significant anatomical, physiological and pharmacokinetic differences between the organ systems of adults and children.
Table of Contents
This chapter enumerates the differences of clinical importance between adults’ and children’s organ systems. The drug dosages for children have also been discussed in detail.
Read And Learn More: Paediatric Dentistry Notes
Organ Systems In Children
The various organ systems in children are not only different in size/volume from their adult/mature counterparts but also different in a few other salient features.
They include anatomical, physiological or metabolic aspects. These distinct features are clinically significant. The precautions to be taken in specific situations in paediatric dentistry have also been discussed.
1. Paediatric Respiratory System
The differences between the adult and children’s respiratory systems are as follows:
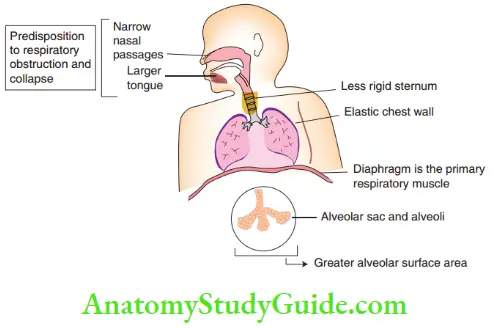
- The nasal passages are narrow and the tongue is proportionally larger than the oral cavity in children. The airway diameter is narrow in children.
- Significance: These factors predispose the young patient to respiratory obstruction and collapse of small and large airways.
- Caution:
- The following errors in the techniques of isolation used during dental procedures may cause serious obstruction and collapse of airways in children:
- Rubber dam or mask compressing the nares
- Gauze pack depressing the oral cavity
- Retractor displacing the tongue posteriorly
- Administration of anaesthesia in a child with a respiratory infection will increase secretions and oedema, thus compromising the airway. Elective anaesthetic administration should be avoided in such children to prevent laryngospasm, bronchospasm, acute subglottic oedema and perioperative hypoxia.
- The following errors in the techniques of isolation used during dental procedures may cause serious obstruction and collapse of airways in children:
- The chest wall is more elastic in children.
- Caution: Very less ventilation pressure is required to expand the lungs.
- The sternum is less rigid in children. It offers less support to the ribs and intercostal muscles.
- Significance: The ribs lie more horizontally in a resting position in children. This makes the respiratory (intercostal) muscles inefficient to work. Thus, the diaphragm is the primary respiratory muscle in children.
- Caution: The paediatric patient must be kept at a 20°–30° head-up position to avoid any breathing difficulty. The supine position should be avoided for children during dental treatment as the gastric organs may impart pressure on the diaphragm in this position. This may limit the efficiency of the only effective respiratory muscle in children.
- The child attains the number of alveoli required for adults in the sixth year of life. However, the ratio of the lung volume to the body size remains the same, thus resulting in a greater alveolar surface area in children.
-
- Significance: The ratio of lung volume to body size remains constant in children and adults. This results in a greater alveolar surface area in children. So, children have increased alveolar ventilation (AV). The AV is directly proportional to the rate of transport of gases to the bloodstream and the brain. Thus, the body reacts more quickly to changes in inhaled gas concentration.
- Caution:
- Children can be adequately anaesthetised with lower gas concentrations of nitrous oxide and halothane.
- Children are at a higher risk of anaesthetic overdose effects such as bradycardia, hypotension and hypoventilation.
- Vital signs have to be carefully monitored while performing dental procedures under general anaesthesia.
2. Cardiovascular System
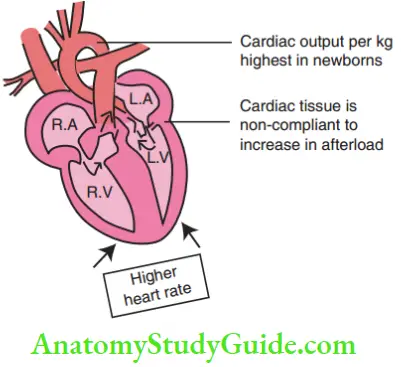
The heart rate is around 120 beats per minute in a newborn and falls to below 100 at the age of 4 years. It reaches the adult count of 72 beats per minute at around 10–12 years of age.
Cardiac output = stroke volume × heart rate.
- Significance: The significance of stroke volume, cardiac output and heart rate in children is as follows:
-
- Stroke volume is the volume of blood pumped by the heart with one contraction from the left ventricle. As the cardiac muscle in children is inelastic, rapid modulation of stroke volume is not possible.
- The heart rate influences cardiac output greatly. There is a greater risk of hypotension with a decrease in heart rate in children than in adults.
- Cardiac output per kilogram of body weight is highest in a newborn.
- The cardiac tissue is non-compliant to increase in afterload. Thus, cardiac failure is more common with fluid overload and systemic hypertension in children.
- A decrease in heart rate leading to a decrease in cardiac output can have a significant impact on the uptake of inhaled anaesthetic agents.
- Forty per cent of the cardiac output perfuses into the brain. This depresses the CNS with a central reduction in vasomotor tone. This can worsen hypotension with significant bradycardia.
3. Paediatric Nervous System
The nervous system is immature in young children, with a more marked parasympathetic tone. In young children, there is a greater risk of significant bradycardia due to vagal stimulation.
- Paediatric Nervous System Caution:
- Manoeuvres such as defecation, bladder distension, application of throat packs, tracheal intubation and pressure on eyeballs can increase vagal stimulation.
- Children undergoing manipulation of the airway like endotracheal intubation need premedication with parasympathetic blockers (atropine substitutes) to eliminate the risk of bradycardia due to vagal stimulation.
- Blood pressure increases with age. The systolic blood pressure is 60–75 (mm Hg) in a newborn. It reaches 100 at the age of 3 years and 120 by 15 years. To counteract this hypotensive response with a decrease in heart rate, the child should be well hydrated prior to an anaesthetic procedure.
- General anaesthetic procedures should be rescheduled in case of recurrent vomiting, diarrhoea, poor oral intake or any other sign of dehydration in the child.
4. Paediatric Gastrointestinal System
The gastrointestinal system of children is different from that of adults in the following ways
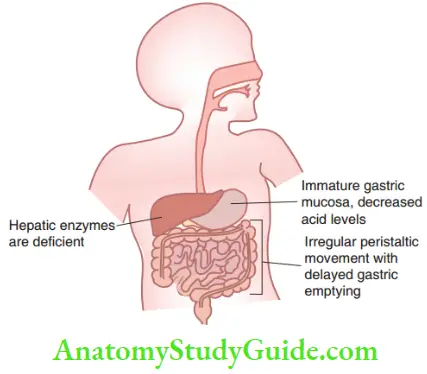
- The gastric mucosa in children is immature and secretes lower levels of acid. The acidity reaches the adult level by the age of 3 years. The adult level of acidity maintains the pH of the stomach of around 2. In children less than 3 years, the pH is higher than 2 owing to decreased acid secretion.
- Significance: Decreased acidity favours the absorption of weakly acidic drugs such as penicillins and cephalosporins. It delays the absorption of weakly basic drugs such as benzodiazepines.
- The peristaltic movement is irregular in infants. Gastric emptying is also delayed.
- Significance: This altered mobility of the gut delays the gastric absorption of the drugs.
- Hepatic enzymes such as cytochrome P-450, glucuronyl transferase and pseudo-cholinesterase are relatively deficient in infants and young children. Thus, children are at a higher risk of drug toxicity.
- Caution: Drugs such as diazepam, phenobarbitone and phenytoin have a prolonged clinical effect due to lower levels of cytochrome P-450 enzyme. Drugs such as acetaminophen, morphine and steroids are conjugated by glucuronyl transferase enzyme into an excretable form. This enzyme is deficient in neonates. So, the aforementioned drugs have to be used with caution. The pseudo-cholinesterase enzyme, which detoxifies\succinyl choline, is deficient in infants. So, succinylcholine has to be administered with caution.
5. Paediatric Renal System
The differences between the adult and paediatric renal systems are the main reason for the modifications in drug dosages in infants. The differences between the infant and adult renal systems are as follows:
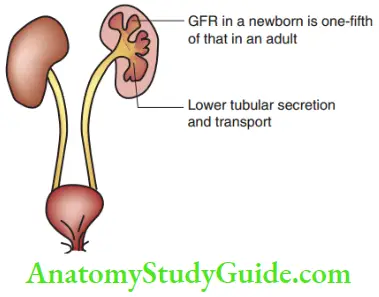
- The glomerular filtration rate (GFR) attains the adult level by 1 year. It is only one fit of the adult level in the newborn.
- Caution: Drugs such as penicillin and barbiturates that depend on GFR for excretion have to be prescribed with caution.
- The rate of tubular secretion and transport is low in infants and toddlers.
- Caution: Drugs such as morphine and atropine are excreted through tubular secretion and transport. These drugs have a slower rate of excretion owing to the lower rate of tubular secretion/transport in children less than 3 years. This can lead to the risk of accumulation of the drug and associated toxicity. Hence, these drugs have a narrower margin of safety and are to be prescribed with caution.
6. Paediatric Integumentary System (Blood And Body Fluids)
The differences between the adult and children integumentary systems are as follows:
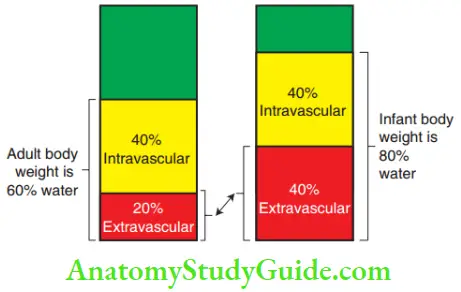
- Eighty per cent of the infant’s weight is the total body water when compared with 50%–60% in adults. This is due to the increased proportion of extracellular fluid (40%) in infants when compared with that of adults (20%).
- Significance: This demands the administration of water-soluble drugs at a higher dose per unit of body weight in infants for clinical efficacy.
- Serum proteins such as albumin and globulin are deficient in infants. Drugs that are carried by plasma proteins are less active when they are bound to plasma proteins and active in a free unbound form.
- Significance; Protein-bound drugs such as digoxin and warfarin have to be administered at lower levels.
- The proportion of the body weight contributed by fat is around 10%–15% in an infant. It increases to 20%–25% in the first few months and falls again with age.
- Significance: Lipid-soluble drugs and those extensively bound to fatty tissues have a decreased rate of excretion when compared with drugs that are unbound (circulate in the body in a free form). Children have a higher proportion of body fat. Hence, the clinical efficacy of drugs such as benzodiazepines/barbiturates that are lipid-bound is higher in children than in adults.
Drug Prescription In Paediatric Dentistry
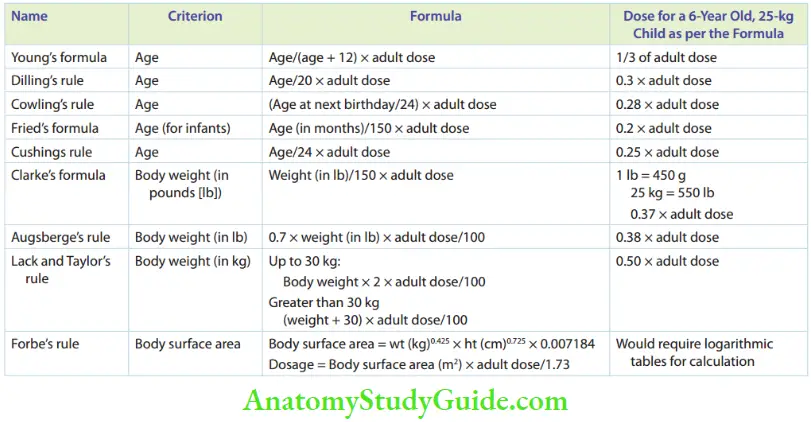
Several formulae have been used to compute the right dosage of drugs for children. Table 5.1 lists all the formulae. Several parameters such as age, body weight and surface area have been used.
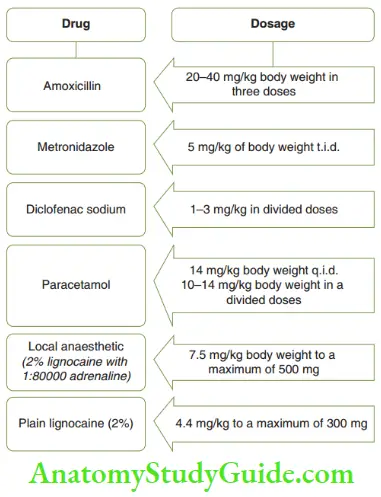
Young’s formula is more widely used in Indian clinical practice due to its ease of calculation. Another simple and commonly used method to compute drug dosage is to calculate the dose from the therapeutic dose of the drug in accordance with the body weight in kilograms. Show this calculation for a few important drugs.
1. Lignocaine dosage in children
The dosage of lignocaine administration with and without adrenaline for children is explained as follows:
- Dosage of lignocaine with adrenaline: Two important features have to be followed to compute the dosage of lignocaine with adrenaline for children. They are as follows:
- The therapeutic dose of 2% lignocaine with 1:80000 adrenaline is 7.5 mg/kg body weight.
- One millilitre of the same contains approximately 21 mg of lignocaine. With these two points in mind, the dosage for administering lignocaine with adrenaline is computed as follows: 2% lignocaine with adrenaline (1:80000)For a child who weighs 30 kg 30 × 7.5 = 225 mgOne millilitres contains approximately 21 mg Threfore, 225/21 = 10 mL (approximately) Threfore, 10 mL of 2% lignocaine with adrenaline can be safely administered.
- Dosage for lignocaine without adrenaline: Plain lignocaine is indicated in children with thyrotoxicosis. This is because the thyroxine hormone sensitises the myocardium to catecholamines like adrenaline leading to arrhythmias. The two salient points to be followed to compute lignocaine dose in children are as follows:
- The therapeutic dose of 2% lignocaine without adrenaline is 4.4 mg/kg body weight.
- One millilitre of the same contains approximately 21 mg of lignocaine.With these two points in mind, the dosage for administering lignocaine is computed as follows:
For a child who weighs 30 kg30 × 4.4 = 132 mg1 mL = 21 mg (approximately)132/21 = 6 mL
Therefore, 6 mL of plain 2% lignocaine can be administered safely.
The drug-dosage calculation can be predicted by the body weight of the patient. Hence, a weighing machine is mandatory for drug-dosage calculation in paediatric dental practice.
Basic Paediatric Medicine Summary
- The organ systems in a child are significantly different from those of adults. The clinically significant differences are as follows:
- Paediatric respiratory system
- Narrower nasal passages that are more prone to obstruction and collapse
- Elastic chest wall that makes ventilation easier
- The diaphragm is the primary respiratory muscle. A supine position can pressurise the diaphragm to compromise breathing.
- Greater AV (alveolar ventilation), hence the body reacts faster to inhaled gases
- Paediatric cardiovascular system
- Heart rate is higher and a major determinant of cardiac output over stroke volume.
- The parasympathetic tone is more pronounced, increasing the risk of bradycardia.
- Paediatric gastrointestinal system
- Gastric acid secretion is lower.
- Peristaltic movements are irregular.
- Hepatic enzymes are deficient.
- Paediatric renal system
- Glomerular filtration and tubular secretion are comparatively lower.
- Paediatric integumentary system
- The proportion of the extracellular fluid volume is higher.
- Plasma proteins are deficient.
- Body fat is higher.
- Paediatric respiratory system
- Drug-dosage prescription can be predictably done by a dose calculation from the body weight of the child.
Leave a Reply