Breast
Question 1. Write a note on fibrocystic disease of the breast.
Answer:
Fibrocystic disease
Three principal morphologic changes seen are:
1. Cystic change
- Gross: Cysts contain turbid, semi-translucent fluid of brown or blue color, and are called blue dome cysts
- Microscopy: Cysts are lined by apocrine cells with round nuclei and abundant granular cytoplasm
- Mammography reveals calcifications
- Mass disappears after FNAC
Read and Learn More Preparatory Manual of Pathology Question and Answers
2. Fibrosis
- Cysts may rupture, resulting in leakage of contents into adjacent stroma
- Leakage of contents brings about a chronic inflammatory reaction and concomitant scarring, resulting in palpable nodularity
3. Adenosis
- Increase in the number of acini per lobule
Question 2. Write a note on gynecomastia.
Answer:
Gynecomastia
- It is defined as the enlargement of the male breast
- Cause: Increased estrogen levels as seen in cirrhosis of the liver
- Microscopically: Increase in dense collagenous connective tissue associated with ductal epithelial hyperplasia
Question 3. Mention the risk factors of carcinoma breast.
Answer:
Risk factors
1. Germline mutations
2. First-degree relatives with breast cancer: Risk is not increased if the only affected relative is the postmenopausal mother
3. Race/ethnicity
4. Age: 70–80 years
5. Age at menarche: Young age at menarche and late menopause
6. Age at first livebirth: Pregnancy before 20 years of age reduces the risk than nulliparous women or mothers more than 35 years of age
7. Benign breast disease: Atypical hyperplasia or proliferative changes in the breast increase the risk of invasive carcinoma
8. Estrogen exposure
- Menopausal hormone therapy increases the risk
- Oral contraceptives do not appear to increase the risk
- Oophorectomy, anti-estrogenic drugs (tamoxifen) or aromatase inhibitors reduce the risk
9. Breast density: High breast density increases the risk
10. Radiation exposure: Risk is greatest with exposure at young ages
11. Carcinoma of the contralateral breast or endometrium: Due to excess estrogen
12. Diet: Excess alcohol increases the risk
13. Obesity
- <40 years—decreased risk, due to anovulatory cycles
- Postmenopausal females: Increased risk
14. Breastfeeding: Lactation suppresses ovulation and triggers the terminal differentiation of luminal cells, thus reducing the risk
Question 4. Discuss etiopathogenesis of familial breast cancers.
Answer:
Familial breast cancers
- BRCA1, BRCA2, TP53, and CHEK2—tumor suppressor genes involved in familial breast cancers and have a role in DNA repair
1. BRCA-1 mutation
- Located on chromosome 17q21
- Increased risk of female breast, ovarian, and male breast cancer (lower than BRCA2), prostate, pancreas, and fallopian tube cancers
- Breast carcinomas are poorly differentiated and have medullary features
- Tumors are triple-negative (basal-like), ER-negative and HER2-negative
2. BRCA-2 mutation
- Located on chromosome 13q12–13
- Increased risk for female breast cancer, ovarian cancer, male breast cancer (more than BRCA1), prostate, pancreas, stomach, melanoma, gallbladder, bile duct, and pharynx cancers
- Poorly differentiated cancers, but are more often ER-positive than BRCA1 cancers
3. Germline mutations in TP53 (Li-Fraumeni syndrome)
- The most commonly mutated gene in sporadic breast cancers
- Most frequent in triple-negative cancers
- Associated cancers include: Sarcoma, leukemia, brain tumors, adrenocortical carcinoma
4. CHEK-2 mutations
- Increase the risk for breast cancer after radiation exposure
- 70–80% are ER-positive
- Associated with prostate, thyroid, kidney, and colon cancers
Question 5. Mention the types of breast cancers.
Answer:
- More than 95% of breast malignancies are adenocarcinoma
1. Carcinoma in situ
- The neoplastic proliferation of epithelial cells that are confined to the ducts and lobules by the basement membrane
- Includes ductal carcinoma in situ and lobular carcinoma in situ
2. Invasive carcinoma (“infiltrating” carcinoma)
- Has penetrated through the basement membrane and grows within the stroma
- Includes infiltrating ductal carcinoma (most common variant)
Question 6. Write a note on Paget’s disease of the nipple.
Answer:
Paget disease of the nipple
- A rare manifestation of breast cancer
- Presents as a unilateral erythematous eruption with pruritis
- A lesion may be mistaken for eczema
- From the DCIS lesion, these cells spread to the skin of the nipple via the lactiferous sinuses without crossing the basement membrane and are called Paget cells
- Tumor cells disrupt the normal epithelial barrier and allow extracellular fluid to seep out onto the nipple surface
- 50 to 60% of women with Paget’s disease, have an underlying invasive carcinoma, presenting as a palpable mass
- These invasive carcinomas are poorly different (ER-negative, HER2 overexpression)
Question 7. Discuss in detail the molecular subtyping of infiltrating breast cancers with examples.
Answer:
Molecular subtypes of invasive breast cancers
1. ER-positive, HER2-negative (i.e. “luminal”)
- The most common form of invasive breast cancer
- Includes low proliferation and high proliferation cancers (associated with BRCA-2 gene mutations)
2. HER2-positive (20% of cancers)
- The second most common molecular subtype of invasive breast cancer
- Can show germline TP53 mutations
3. ER-negative, HER2-negative tumors (“basal-like” triple-negative carcinoma; 15% of cancers)
- Associated with BRCA-1 gene mutations
Examples
1. ER-positive, HER2-negative (low proliferation) cancers
- Well to moderately differentiated mucinous, papillary, cribriform, and lobular carcinomas
2. ER-positive, HER2-negative (high proliferation) cancers
- Includes poorly differentiated lobular carcinoma
3. HER2-positive cancers
- Poorly differentiated cancers, for example, apocrine cancers and micropapillary cancers
4. ER-negative, HER2-negative cancers
- Poorly differentiated cancers, for example, squamous cell, spindle cell, medullary, adenoid cystic, metaplastic carcinomas
Question 8. Discuss the grading of invasive breast cancers.
Answer:
- Microscopic grading of the breast carcinoma is done by Nottingham modification of the Bloom-Richardson system
Scoring is done based on
1. Tubule formation
2. Nuclear pleomorphism
3. Mitotic rate
- Carcinomas are graded into grade I (well differentiated), grade II (moderately differentiated), and grade III (poorly differentiated) types
- Grade I carcinomas (well-differentiated carcinoma) grow in a tubular pattern with small round nuclei and a low proliferative rate
- Grade II carcinomas (moderately differentiated carcinoma) show some tubule formation, but solid clusters or single infiltrating cells are also present, with a greater degree of nuclear pleomorphism and mitotic figures
- Grade III carcinomas (poorly differentiated carcinoma) show tumor cells present in solid sheets of cells with enlarged irregular nuclei, high mitotic rate, and frequent areas of tumor necrosis
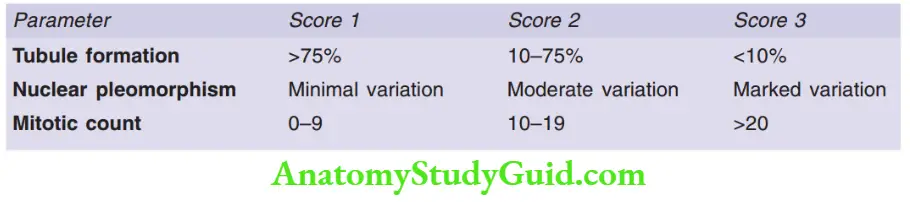
If the total score is 3–5: Grade I; Score 6–7: Grade II; Score 8–9: Grade III
Question 9. Write a note on comedo carcinoma breast.
Answer:
Comedo carcinoma
Gross
- Presents as a mass in the duct, through which the necrotic material can extrude out, hence termed comedones
Microscopy
- The involved duct is enlarged in size and is lined by atypical pleomorphic tumor epithelial cells, with increased mitotic activity
- The duct lumen is filled with necrotic material, which can also show areas of coarse calcification
- Surrounding these ducts, myoepithelial cells are also visible
Note: Areas of definite stromal invasion and intra-ductal spread to the nipple (Paget’s disease) should always be looked for
Question 10. Discuss in detail the prognostic indicators of breast carcinomas.
Answer:
Prognostic indicators
1. Invasive carcinoma versus carcinoma in situ (CIS): CIS has an excellent prognosis
2. Distant metastases: If present, indicates poor prognosis
3. Lymph node metastases
- Axillary lymph node status is the most important prognostic factor for invasive carcinomas in the absence of distant metastases
- Lymphatic vessels in most breast carcinomas drain first to sentinel nodes
4. Tumor size
The risk of axillary lymph node metastases increases with the size of the primary tumor
5. Locally advanced disease
Carcinomas invading into skin or skeletal muscle are difficult to treat surgically
6. Inflammatory carcinoma
- Edematous skin is adhered to the breast by Cooper’s ligament and mimics the surface of an orange peel, an appearance referred to as peau d’orange
- Occurs due to dermal lymphatic being filled with metastatic carcinoma
- Poor prognosis
7. Lymphovascular invasion: Poor prognostic factor
8. Molecular subtype
- ER and HER-2 expression and proliferation have different prognostic implications
- ER and PR-positive cancers respond well to hormonal therapy and less to chemotherapy
- ER or PR-negative cancers respond poorly to hormonal therapy but respond well to chemotherapy
- HER2 overexpression is associated with poorer survival
9. Special histologic types
- Tubular, mucinous, lobular, papillary, and adenoid cystic carcinomas have a better prognosis than NOS-type
- Metaplastic cancers and micro-papillary cancers have worse prognoses
10. Histologic grade
- Nuclear grade, tubule formation, and mitotic rate classify invasive carcinomas into three groups
11. Proliferative rate
Carcinomas with high proliferation rates (Ki-67 positivity) have poorer prognosis but respond better to chemotherapy
Question 11. Write a note on fibroadenoma.
Answer:
Fibroadenoma
- The most common benign tumor of the female breast
- Presents as a palpable mass can be multiple and bilateral
Morphology
Gross
- Size: Less than 1 cm to tumors that replace entire breast
- Tumors are well-circumscribed, grayish white nodules, which on cut surface show slit-like spaces
Microscopy
- Intra-lobular stroma is delicate and myxoid
- Pericanicular pattern: Epithelium is surrounded by stroma
- Intra-canicular pattern: Epithelial is compressed and distorted by stroma
Question 12. Write a note on the phyllodes tumor.
Answer:
Phyllodes tumor/osteosarcoma phyllodes
- Arises from intra-lobular stroma
- Age group: Sixth decade
- Associated with gain in the chromosome 1q
- HOXB13 over-expression is associated with higher tumor grade
Gross
- Small to massive tumors
Microscopy
- Composed of nodules of proliferating stroma covered by epithelium
- Distinguished from fibroadenoma based on higher cellularity, higher mitotic rate, nuclear pleomorphism, stromal overgrowth, and infiltrative borders
Note: High-grade phyllodes are difficult to differentiate from malignant sarcomas
Leave a Reply