Chest Trauma, Cardiothoracic Surgery
Chest Trauma
Chest Trauma Introduction:
Table of Contents
In chest trauma, the mortality is very high unless promptly recognised and properly treated The margin of safety is very slim, initial care dictates the final result. With varying degree of severity, chest injuries occur in almost 80% of road traffic accidents.
Read And Learn More: Surgery of Urology Notes
Assessment Of Injury
Chest Trauma History:
- Time since the injury
- Details of the injury from the bystander or the police
- High-speed deceleration injury (aortic and cardiac rupture to be ruled out)
- Crushing accidents (tracheobronchial and oesophageal tear)
- Sudden abdominal compression (ruptured diaphragm)
- In stab injuries, length of the knife and direction of sta
Examination:
- The clothing should be removed carefully without moving the patient.
- Palpate for clinical evidence of fracture ribs, surgical emphysema, any paradoxical movement of the ribs and auscultate for air entry in both lungs.
- Even if it is a trivial injury, the patient should be admitted and observed for a minimum of 24 hours before discharge.
- It is reasonable to do unilateral or bilateral closed tube thoracostomy (ICT) on suspicion of haemothorax or pneumothorax when the patient is in respiratory distress even before a chest X-ray.

Main Aims Of Resuscitation
The standard method of resuscitation in all cases of polytrauma is as follows:
1. Airway:
- Aspiration of blood and secretions from oral cavity, pharynx and trachea
- Introduce plastic airway
- Endotracheal intubation
- Cricothyroidotomy as necessary
- Tracheostomy as necessary
2. Breathing:
- Intubation
- Intercostal chest tube (ICT)
- Closure of any open chest wounds
- These two steps (A and B) help in re-aerating the lung.
3. Circulation
- Control of major and life-threatening bleeding
- Volume infusion
4. Disability:
- Neurological
5. Exposure:
- All clothing is to be cut open without moving the patient.
Blunt Trauma To The Chest
Blunt Trauma To The Chest Causes:
- Road traffic accidents
- Fall from a height
- Crush injuries
- Assault with blunt object
Simple Rib Fracture
Rib fractures can be single or multiple
Single Rib Fracture:
- Often regarded as a trivial injury but should be treated with respect in elderly patients.
- Occurs due to direct injury or excessive flexion.
- The common site is at the costal angle or middle of the shaft.
- Patients will have pain on breathing, coughing and on palpation.
- They are treated with analgesics, intercostal nerve block and assurance.
Multiple Rib Fractures:
- When there are multiple rib fractures without any pneumo- or haemothorax and no other organs are involved, intercostal nerve block and a small amount of narcotics are required.
- Strapping is occasionally necessary in young adults.
- In elderly patients, consider hospitalisation for observation, pain control and pulmonary toilet.
- Chest X-ray is to be repeated after 24 hours and at the time of discharge, to rule out late-onset pneumothorax and haemothorax.
- Intermittent use of velcro belt rib support.
- Inform the patient of deep breathing, nebulisation, chest physiotherapy and coughing using the rib belt.
- Epidural analgesia is becoming the standard of care for pain management in patients with multiple rib fractures.
Sternal Fracture
- Commonly due to steering wheel injury—blunt trauma.
- Usually occurs at the sternal angle.
- Associated with costochondral dislocations.
- Classified as displaced and nondisplaced fractures
- Localised swelling, tenderness and deformity are the clinical findings.
Blunt Trauma To The Chest Treatment:
- Displaced fracture—requires surgical fixation with plates or steel wires.
- Nondisplaced fracture—conservative management.
Flail Chest
This results from severe chest injuries with multiple rib fractures.
Here there are fractures of three or more ribs at two places, anteriorly and posteriorly, so that certain segments of ribs will have no attachment to the chest wall. These ribs become indrawn due to intrathoracic negative pressure as the patient inhales and is driven outwards on expiration producing instability. This is called paradoxical respiration. It results in hypoventilation, carbon dioxide retention and respiratory failure. The flail chest is of three types: Anterior, posterior and lateral.
- Anterior flail: Fracture of the costochondral junction on both side of the sternum.
- Posterior flail: Fracture ribs of posterior chest wall.
- Lateral flail: Fracture shaft of the ribs.
Blunt Trauma To The Chest Treatment:
1. Commonly Done Procedures:
- Anterior flail: The flail segments are stabilised with metal plates and screws from costal cartilage to the sternum, introduced to stabilise the flail segments.
- Posterior flail: No treatment is required as the scapula acts as a support to stabilise the flail segment.
- Lateral flail: It is treated by chest wall stabilisation, by positive pressure ventilation or velcro rib belt, reduction of respiratory dead space by intercostal chest tube, removing air or blood reduction of the respiratory dead space, management of the pulmonary contusion and pain control. Epidural analgesia is recommended for pain management. Intercostal nerve blocks may also be used.
2. Other Methods:
- Surgical stabilisation is rarely indicated, i.e. open reduction of rib fracture or osteofixation with metal plates and screws.
- The recent method is to intubate and stabilise the flail segments with positive pressure ventilation, which has to be done for at least one week. This is called internal pneumatic fixation.
- Physiologic stabilisation with intubation and IPPV (intermittent positive pressure ventilation) must be initiated before hypoxia develops. IPPV produces satisfactory ventilation and helps the fractured ribs to unite in the position of inspiration, thereby reducing the deformity and improving the pulmonary function.
‘Stove In’ Chest
- Localised, severe, blunt or crush injury produces depression of a portion of the chest.
- Treatment is the same as that for flail chest. Sometimes, thoracotomy may be needed if there are internal injuries.
Pulmonary Injuries
Contusion Of The Lung
- Deceleration injuries or crush trauma often produces extensive parenchymal damage. Haemorrhage and interstitial oedema result in obliteration of alveolar spaces and consolidation of large areas of pulmonary tissue.
- Contusion of the lung can be unilateral or bilateral. The contusion can be in the form of a small area of damage with oedema and extravasation of the blood, or it may be widespread damage. Haemoptysis and excessive tracheobronchial secretions give the clue to the diagnosis.
- Chest X-ray: Early patchy consolidation. It must be differentiated from adult respiratory distress syndrome (ARDS).
- CT scan is more specific.

- Fluid restriction, pulmonary care
- Chest physiotherapy
- Steroids and rarely ventilation
- Usually self-limiting, if there are no other severe injuries.
Pulmonary Injuries Complications:
- Pneumonia
- Atelectasis
- Respiratory failure
- ARDS
Pneumothorax
- Pneumothorax is the most common cause of respiratory insufficiency following chest trauma.
- Usually, if there is a rib fracture and evidence of subcutaneous emphysema, pneumothorax is certainly present.
- Pneumothorax can be closed (simple), open and tension.
- Small simple pneumothorax does not need any treatment.
- A repeat chest X-ray after 12–24 hours is essential to confirm that it is not progressing.
- It can be confused for a large bullae.
- Small pneumothorax can be missed easily.


- Bilateral pneumothorax is an emergency.
- Late pneumothorax can also occur.
- Open chest wound will produce complete collapse of lung and paradoxical shift of the mediastinum with each respiration (mediastinal flutter) causing hypoventilation and reduced cardiac output.
- Treatment is by closure of the wound, intercostal tube drainage (ICD) and surgery.
Tension Pneumothorax:
- Injury to the lung results in continuous valvular air leak. The accumulating air collapses the lung on the same side and pushes the mediastinum to opposite side. As a result of this tension, the intrapleural pressure increases, till it is above atmospheric pressure at the time of expiration. This reduces the venous return to the heart as well as compromises the ventilation.
- Tension pneumothorax is an emergency which should be treated urgently with needle thoracocentesis in the second intercostal space in the midclavicular line to release the tension. Thoracocentesis converts tension pneumothorax to simple pneumothorax.
- This should be followed by urgent ICD insertion and connected to underwater seal.
- Do not wait for chest X-ray.
Tension Gastrothorax:
This occurs due to herniation of dilated and obstructed stomach into the mediastinum due to diaphragmatic tear resulting in haemodynamic compromise. It should be treated by reducing the hernial contents and repair of diaphragmatic tear.
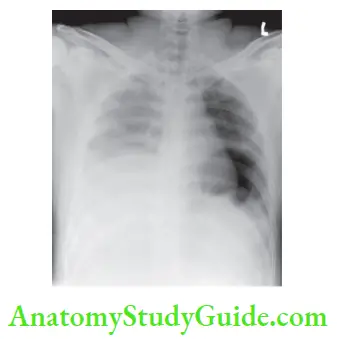
Haemothorax
- May be missed in chest X-rays in the supine position.
- Results from injury to internal mammary artery, intercostal artery and vascular lung adhesions.
- Classical signs are reduced—chest expansion, dullness to percussion and absent breath sounds on affected side.
- Treated by intercostal chest tube insertion
- If bleeding continues or features of shock develop, thoracotomy has to be considered.
- The bleeding may be delayed or may recur after several days.

Indications for Thoracotomy:
- The initial volume of blood loss is not as important as the amount of ongoing bleeding.
- Drainage is more than 1000 ml or 100 ml each hour for 4 hours.
- If clotted haemothorax is suspected (opacity persisting on chest X-ray even after ICD).
Pulmonary Injuries Complications
- Failure to adequately drain a haemothorax initially results in residual clotted haemothorax and empyema or late fibrothorax.
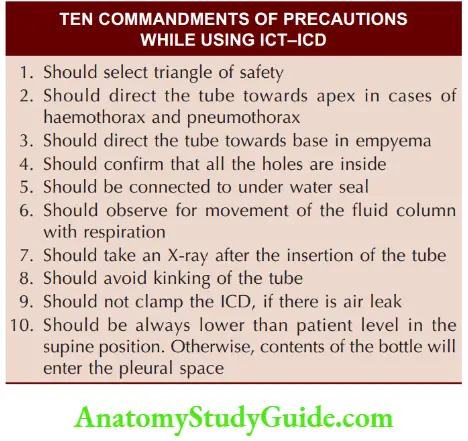
Intercostal Chest Tube (Ict) Insertion (Closed Tube Thoracostomy)
- Second intercostal space needle thoracostomy— anteriorly midclavicular line is ideal for pneumothorax and ICT in the fifth space in the midaxillary line for haemothorax.
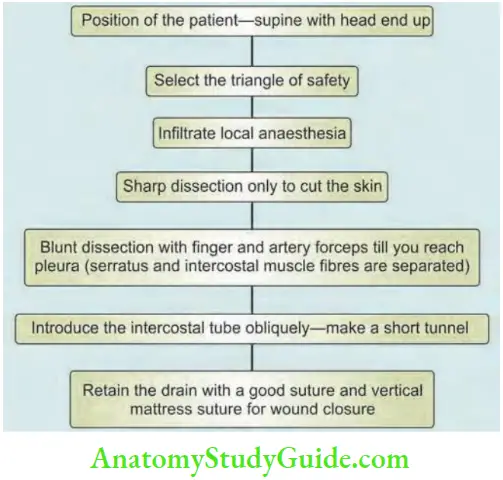
- Triangle of safety
- Above the level of nipples
- Anterior to midaxillary line
- Below and lateral to pectoralis major muscle
- Can be introduced from fifth intercostal space midaxillary line for pneumothorax also but the chest tube should reach the apex of the lung
- Infiltrate local anaesthetics up to the parietal pleura.
- 2–3 cm incision parallel to the ribs—deepened, suture taken.
- Insert the chest tube with trocar into the pleural cavity. Push the tube pointing towards the shoulder and not the mediastinum.
- Then the trocar is removed and the chest tube is connected to underwater seal. The ICT is fixed.
- Intercostal drainage (ICD) can also be done by connecting to 2 bottles (Fig. 62.9). When low thoracic suction is not available, the ICT is connected to wall suction.



Lung Laceration
Minor laceration: Haemopneumothorax. Usually intercostal chest tube is enough.
Major laceration: Haemopneumothorax
- Introduce intercostal chest tube
- Continuous air leak or bleeding through ICT and lung not expanding. Requires thoracotomy and repair or resection of lobe.
Shock Lung
Shock Lung Definition:
- Alveolar collapse due to shock as a result of oedema, impaired perfusion, and reduction in alveolar space resulting in respiratory failure is called shock lung.
- It is also called Acute Respiratory Distress Syndrome (ARDS).
Shock Lung Causes:
- Major chest trauma with multiple rib fractures and lung contusion
- Septic shock and septicaemia
- Disseminated intravascular coagulation
- Massive blood transfusion
- Major burns
- Cardiopulmonary bypass (also called ‘Pump lung’)
- Acute pancreatitis
- Aspiration of gastric contents
Shock Lung Pathogenesis:
- Diffuse inflammation of the lung
- Extensive intravascular coagulation due to micro thromboembolism
- Focal disorders of the circulation, primarily because of sluggish microcirculation due to leukostasis, and sludge, leading to extensive hyaline thromboses
- Increased capillary permeability due to damaged capillaries
- Diffuse alveolar damage, decreased production of surfactant by type II pneumocytes leading to bilateral extensive fine atelectasis
- The net result is pulmonary consolidation, decrease in the lung compliance, poor gas exchange leading to stiff lung.
Shock Lung Investigations:
- Arterial blood gas analysis
- Chest X-ray
- CT scan
Shock Lung Treatment:
- Ventilatory support (intermittent positive pressure ventilation)
- Antibiotics—broad spectrum
- Low to moderate doses of steroids may help in early ARDS, in patients requiring high doses of vasopressors to maintain blood pressure.
- Intensive care—supportive therapy can be remembered as FASTHUG
F—Feeding (usually enteral)
A—Analgesia
S—Sedation once a day and check neurological status
T—Thromboembolism prophylaxis
H—Head-end elevation (20–30°)
U—Ulcer (gastric) prophylaxis, and
G—Glucose (blood) control.
Injury To Trachea And Major Bronchi
Tracheal Injuries
Injuries occur as a result of trauma sustained due to crush injuries. Common in cervical trachea
Injury To Trachea Symptoms:
- Acute airway obstruction
- Subcutaneous emphysema—mediastinal and cervical
- Pneumothorax
- Voice impairment
Injury To Trachea Treatment:
Intubation, tracheostomy, surgery and repair.
Major Bronchial Injuries
- Blunt trauma produces stereotype injury to main bronchus of either side. Lobar bronchi are less commonly injure
- Lesion is often a circumferential laceration with complete separation or a partial tear.
Injury To Trachea Symptoms:
- Pneumothorax, uncontrolled air leak
- Haemoptysis
- Surgical emphysema
- Bronchoscopy for confirmation
Injury To Trachea Surgery:
- Endobronchial intubation
- Bronchoplasty, injury to the lobar bronchus— resection of the lobe of the lung.
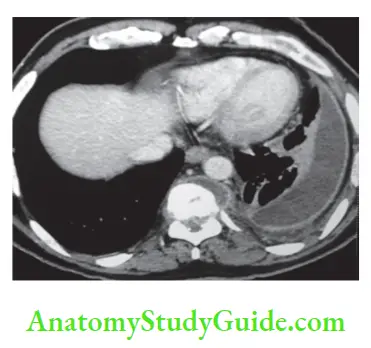
Injury To The Diaphragm
Injury To The Diaphragm Features:
- Due to crush injury
- Industrial—due to fall of heavy weights over the abdomen.
- Commonly, left diaphragm tear occurs.
- Missed in chest X-ray in the supine position.
Summary of Blunt Chest Injury:

- Diagnosed by CECT of the abdomen or chest X-ray reveals the Ryle’s tube in the chest or coils of bowel (gas shadow) in the chest and elevated fundic air bubble. Diagnostic laparoscopy is also a good investigation in cases of rupture diaphragm.
- When in doubt, do diagnostic laparotomy



Injury To The Aorta (Rupture Of The Aorta)
- Deceleration injuries
- Gets avulsed at the region of ligamentum arteriosus
- Complete rupture—immediate death
- Incomplete rupture—shock, widening of mediastinum, unequal pulses.
Injury To The Aorta Surgery:
- Repair is done using a cardiopulmonary bypass.
Myocardial Contusion
- Deceleration injuries
- Anterior chest impact
- Clinical features include arrhythmias, reduced cardiac output, cardiac tamponade.
Surgical Emphysema
Surgical Emphysema Types
- Localised
- Extensive from the eyelids to the scrotum, quite alarming in appearance. Indicates lung injury. X-ray chest may show pneumothorax or air in the subcutaneous plane.
Surgical Emphysema Treatment:
- Localised: Not extending, no pneumothorax— observation.
- Pneumothorax—ICT.
- Extensive: ICT to be introduced on the side where it is maximum.
- ICT may be required on both sides.


- Two ICTs, one apical and the other basal, may need to be introduced if there is a continuous air leak.
- The emphysema usually subsides within a week. Multiple incisions and expelling the air from the subcutaneous space manually are not required but may be carried out for cosmetic purposes or if patient has respiratory distress.
Penetrating Thoracic Wounds
Stab Wounds:
They depend on the type of weapon, length and direction of the stab.
Projectile Wounds:
- Relatively low velocity revolver bullets may perforate one or two lobes of the lung with a little damage and only drainage of the pleural space is requireThere will be entry and exit wounds.
- High velocity perforating wounds cause more damage to the tissue, adjacent to the tract. If the damage is extensive, lobectomy or pneumonectomy has to be considered.
- Bomb fragments, because of irregular shape, commonly carry with them pieces of ribs and are associated not only with severe haemorrhage and air leak from the torn pulmonary vessels and bronchus but also with haemorrhage from irregular entry and exit wounds. Urgent thoracotomy is necessary.
Penetrating Thoracic Wounds Treatment:
Emergency thoracotomy is a life-saving procedure in the trauma centre. Thoracotomy for polytrauma has a poor prognosis than for isolated thoracic injuries.
Penetrating Thoracic Wounds Indications:
- Decompression of cardiac tamponade
- Control of bleeding, allow for internal cardiac massage
- Clamping of descending thoracic aorta for exsanguinous bleeding in the abdomen.
Penetrating Thoracic Wounds Surgery:
Anterolateral thoracotomy through 5th intercostal space, entered in 1–2 minutes.
Mediastinal Emphysema
- The emphysema is mainly suprasternal.
- On auscultation, pericardial crunching sounds synchronous with the heart beat, are heard.
- If there is haemodynamic instability, bilateral intrapleural ICT has to be introduced as a precaution against tension pneumothorax.
- Rule out oesophageal and tracheal injury.
Principles of Managing Chest Injuries:
- Pulmonary physiotherapy: Most important in all chest injury patients.
- Aspiration of secretions: Tracheal aspiration, nasotracheal suction, aspiration of oral cavity and pharynx.
- Relieving pain: Oral narcotics, parenteral narcotics, thoracic epidural analgesia, intercostal nerve block.
- Physiotherapy assistance
- Encourage coughing
- Chest percussion and vibration
- Deep inspiratory efforts
- Humidification of air, nebulisation
- Early mobilisation
- Treatment of pneumothorax or haemothorax: Insertion of intercostal chest tube.
- Treatment of shock: First of all, the causes of shock in chest injuries has to be determined by thorough assessment of the patient. Once the cause is found out, depending upon the nature of the problem, the patient is treated in an intensive care unit.
- FAST (Focussed Abdominal Sonography in Trauma): Focussed assessment with ultrasonography for trauma and rapid assessment for ruling out fluid collection in the abdomen, chest and pericardium.
- Surgery: Depending upon the severity and location, surgery is done.
- Treatment of complications
- Thromboembolism
- Tracheostomy complications
- Prolonged ICU complications.
Empyema
Empyema Definition
The collection of the p:us in the pleural space is called empyema.
Aetiopathogenesis:
- It is the end stage result of pleural effusion and infection. A few examples are—following haemothorax, lung abscess, pneumoniIn India, tuberculosis is an important cause of empyema (Figs 62.15 and 62.16).
- Oesophageal perforations—iatrogenic or spontaneous also result in empyema.
- Rupture of subphrenic abscess, rupture of hydatid cyst, rupture of amoebic liver abscess also can result in empyema.
- The classical events which follow empyema following pneumonia are exudative phase with pleural effusion,followed by thickening of fluid—fibropurulent stage and when the lung is covered by thick cortex, it is called organising phase.


Empyema Diagnosis:
- History of fever diagnosed as pneumonia or tuberculosis
- Pain in the chest, difficulty in breathing
- Tenderness over the chest
- Toxic features in acute empyema specially in children
- Presence of thick pus with thick cortex of fibrin and coagulum over the lung.
Empyema Investigations
- Chest X-ray may show collapse of the lung, tracheal deviation, evidence of pneumonia or tuberculosis.
- Aspiration of pleural fluid and analysis—exudative in cases of pneumoniSend for bacterial culture.
- CT scan may show split pleura sign. Tuberculous spine can be diagnosed as a cause of empyema
Surgical Management of Pleural Effusions and Empyema:
- Video-Assisted Thoracoscopic Surgery (VATS): With 3–4 ports, video-assisted procedures have become very popular. Minimal incision, less pain and recovery is fast. Drainage, pleural biopsy, talc pleurodesis, debridement of empyema, intercostal tube drainage (ICD) all can be done.
- Rib resections, and drainage through a window—Eloesser’s method.
- Modified Eloesser drainage surgery soon after completion of surgery.
- This surgery is a palliative operation for chronic empyema collapsed lung and bronchopleural fistulIn these patients, any major lung resection is fraught with high risk of sepsis and stump blowout.
- An inverted U-shaped incision is taken on the lower rib and the flap is stitched to the diaphragm for clearing of the purulent secretions.
- The Eloesser flap is a surgical method devised by “Dr Leo Eloesser in 1935.” It was originally planned for tuberculous empyema
- Decortication: More radical procedure involves thoracotomy, debridement, excision of thick cortex or the covering of the lung, so that lung will expan This is done by posterolateral thoracotomy.
Empyema Complications:
- Toxicity, septic shock, multiorgan failure in untreated cases
- Damage to the lungs—lobectomy, pneumonectomy.


Empyema necessitates: It is a type of empyema which presents as a swelling in the subcutaneous plane with communication to the pleural space/cavity. It is a tense, tender, fluctuant swelling with local rise of temperature. The intercostal bulge is also seen. On asking the patient to cough, expansile impulse is felt. Otherwise, management is similar to that of empyema such as drainage, treating the cause, ATT in tuberculosis and antibiotics in pyogenic infections.
Bronchopleural Fistula
Bronchopleural Fistula Definition:
It is fistulous communication between the main stem, lobar and segmental bronchus to the pleural space.
Bronchopleural Fistula Causes:
- Following lobectomy or pneumonectomy or bacterial/tuberculous infection.
- It may occur when large airways are in communication with the pleural space.
Bronchopleural Fistula Pathogenesis:
- There will be a large empty space left behind following pneumonectomy. This space will be filled with air. Over a period of time, air is absorbed and fluid gets filled up which gets fibrosed slowly. When this fluid gets infected, the stump may break down and cause bronchopleural fistulThe gaping of bronchial stump occurs resulting in bronchopleural fistula.
- Invariably the fluid which accumulates later will be infected.
Bronchopleural Fistula Clinical Features:
- History and clinical features suggestive of empyema
- History of lung surgery
- Persistent air leak in the intercostal drain
- Pus in the ICD
Chest X-ray:
- The lung does not fully expand.
Bronchopleural Fistula Treatment:
- Treatment is extremely difficult and disappointing.
- Propped up/sitting position and turn to the diseased side so as to get a dependent drainage
- Intercostal drain connected to underwater seal
- Pleurocutaneous window drainage can be done
- Specific treatment includes control of infection, treat the primary cause, suturing, et
Surgical Anatomy Of Mediastinum And Mediastinal Masses
The mediastinum is a broad central partition that separates the two laterally placed pleural cavities. It extends from the sternum to the bodies of the vertebrae; and from the superior thoracic aperture to the diaphragm.
Contents: The thymus gland, pericardial sac, heart, trachea and major arteries and veins. It also serves as a passageway for structures such as the oesophagus, thoracic duct and various components of the nervous system as they traverse the thorax on their way to the abdomen.
Division of Mediastinum:
- A transverse plane extending from the sternal angle (the junction between manubrium and the body of the sternum) to the intervertebral disc between 4th and 5th thoracic vertebrae separates the mediastinum into the superior mediastinum and inferior mediastinum.

- Inferior mediastinum is further partitioned into the anterior, middle, and posterior mediastinum by the pericardial sac.
- Anterior mediastinum: It lies between the back of the sternum and the anterior aspect of the great vessels and pericardium. It contains the thymus, internal mammary arteries, lymph nodes, connective tissue and fat.
- Middle mediastinum: It extends from the pericardium anteriorly to the ventral surface of the thoracic spine posteriorly. It contains the pericardium, heart, great vessels, airway and oesophagus.
- Posterior mediastinum: It is made up of the spine and includes the costovertebral sulci. The posterior compartment contains the proximal intercostal neurovascular bundles, the spinal ganglia, the sympathetic chain, lymphatic tissue, and connective tissue.
Anterior Mediastinal Masses
“Terrible Ts”: Thymic tumours, Teratoma/germ cell tumour, (Terrible) lymphoma, and Thyroid.
1. Thymoma:
- The most common anterior mediastinal primary tumour; 20% of adult mediastinal neoplasms.
- Presentation between ages 30 and 50 (most patients are >40 years old).
- 50% are asymptomatic but others have symptoms secondary to compression: Chest pain, cough, dyspnoea, compression of the superior vena cava resulting in head and neck venous congestion, facial oedema
Differential diagnosis of mediastinal masses:

- Myasthenia gravis: Seen in 30–50% of thymoma patients; others can have hypogammaglobulinemia (10%), endocrine disorders, connective tissue disorders.
Staging:
Anterior Mediastinal Masses Investigations:
- Chest X-ray may show a mediastinal mass.
- A contrast CT scan of the thorax is the investigation of choice which will detect a mass lesion and its relationship to the adjacent structures.
Masaoka’s clinical stage:


- MRI can also be done.
- A preoperative biopsy is not necessary.
Anterior Mediastinal Masses Surgery:
- Surgery is the main modality of the treatment—a complete resection of the thymus. Median sternotomy is done to remove the tumour.
- A minimally invasive (thoracoscopic or robotic) approach is another option.
2. Germ Cell Tumours (GCT):
- The mediastinum is the most common location for extragonadal germ cell tumours in adults.
- They are classified as benign (teratomas, dermoid cysts) or malignant (seminomas, nonseminomatous GCTs).
- Seminomas are more common than nonseminomatous GCTs.
- Occur in the second decade—late teens
- 20% are malignant
- Cystic teratomas are dermoid cysts, less malignant compared to solid teratomas which have more chances of malignancy.
- Diagnosis is by tumour markers: Alfa fetoproteins (AFP) and beta-hCG. AFP is normal in teratoma and “pure” seminomas. Ninety percent of nonseminomatous germ cell tumours have elevated AFP and/or beta-hCG.
- They are highly radiosensitive.
3. Lymphomas:
- The most common are nodular sclerosing Hodgkin’s lymphoma and primary mediastinal B-cell lymphoma.
- May present with systemic symptoms such as fevers, weight loss or night sweats but can also present with symptoms such as chest pain, dyspnoea, wheezing, stridor, hoarseness, dysphagia, or superior vena cava syndrome due to compression of mediastinal structures.
- Core biopsy is required for the diagnosis.
- Immunohistochemistry studies have to be done.
- CT scan will help in ruling out other diseases.
- Mediastinal mass ratio (MMR)—the ratio of the mass to the chest diameter is calculated.
- Chemotherapy is the treatment of choice.
4. Thyroid Masses:
- Intrathoracic thyroid tissue—ectopic or substernal, typically causes symptoms of shortness of breath or dysphagiSometimes they produce dangerous airway obstruction, deviation of the trachea or narrowing.
- The intrathoracic mass is usually continuous with the thyroid gland in the neck; only 2% of cases are separate from the cervical thyroid and are truly intrathoracic.
- Diagnosis is by CT scan and technetium scan.
- Majority can be managed with cervical incision—a few may require sternotomy.
- Less commonly, intrathoracic mobilisation via VATS is done.
- Possibility of collapse of trachea should be kept in mind after thyroidectomy—one should be ready with re-intubation/tracheostomy.
Middle Mediastinal Masses
- Lymphadenopathy is the most common lesion presenting as a mass in the middle compartment of the mediastinum.
- The most common causes include lymphoma, sarcoid and metastatic lung cancer.
- Mediastinoscopy is a very useful technique to biopsy lymphadenopathy in this region.
- Cystic masses comprise approximately 20% of middle mediastinal masses.
1. Bronchogenic Cysts:
- Bronchogenic cysts are the most common cystic lesion.
- Secondary to abnormal lung budding during development.
- Bronchogenic cysts are more common in men, in the right paratracheal region and in the subcarinal location.
- Often presents with substernal pain, cough, recurrent infection symptoms or dyspnoea.
2. Enteric Cysts:
- They are the third most common benign oesophageal masses after leiomyomas and polyps, and are usually asymptomatic.
- Three criteria are required to establish their diagnosis:
- Oesophageal attachment
- The presence of two layers of muscularis propria
- Epithelium characteristic of the gastrointestinal tract.
3. Pericardial Cysts:
- Seventy percent arise in the right cardiophrenic angle.
- Symptoms can include shortness of breath, right heart failure secondary to compression, infection and bleeding.
Middle Mediastinal Masses Management:
- Bronchogenic and enteric cysts need surgical resection to establish a definitive diagnosis and to decrease the risk of infection or malignant degeneration.
- Pericardial cysts can be typically observed, if asymptomatic, but resection can be utilised, if there are symptoms or if the diagnosis is not completely established by imaging.
- Simple drainage is generally not recommended because these cysts typically recur without complete resection.
Posterior Mediastinal Masses
Neurogenic tumours represent more than 60% of posterior mediastinal masses. These lesions are classified based upon their neural cell of origin. 95% of posterior mediastinal masses arise in the intercostal nerve rami or the sympathetic chain region.
1. Schwannomas and Neurofibromas:
- These are benign lesions that arise from the intercostal nerve sheath and make up 90% of adult neurogenic tumours.
- Neurilemmomas or schwannomas constitute 75% of this group of masses. These tumours are firm, encapsulated masses consisting of Schwann cells.
- Neurofibromas are nonencapsulated, soft, friable and are associated with von Recklinghausen neurofibromatosis.
- The surgery of choice for removal of these tumours is by thorocoscopy or thoracotomy.
- Postoperative complications include Horner’s syndrome, partial sympathectomy, recurrent laryngeal nerve damage and paraplegia.
2. Malignant Tumours of Nerve Sheath Origin:
- Malignant nerve sheath tumours are spindle cell sarcomas of the posterior mediastinum and include malignant neurofibromas, malignant schwannomas and neurogenic fibrosarcomas.
- They affect men and women equally in the third to fifth decades of life and are closely associated with neurofibromatosis, with a 5% risk of sarcomatous degeneration.
- Pain and nerve deficits are common.
- Complete surgical resection is the optimal treatment but in patients with unresectable tumours, adjuvant chemotherapy and radiation are options.
3. Autonomic Ganglionic Tumours:
- Neuroblastomas and ganglioneuroblastomas are malignant tumours that occur most commonly in children and originate from the sympathetic ganglia.
- Ganglioneuromas are benign lesions that arise from the sympathetic ganglia, and are most common in young adults. Lesions that arise from paraganglionic cells include phaeochromocytomas and paragangliomas.
- Some neurogenic tumours are “dumb-bell shaped” and arise near intervertebral foramen, and have a posterior mediastinal and intraspinal component.
- Resection usually requires a combined approach with neurosurgery and thoracic surgery.
Pulmonary Aspergilloma
- Pulmonary aspergilloma, is a mycetoma or fungus ball, caused by fungus of Aspergillus species.
- The most common place affected by aspergillomas is the lung.
- Tuberculosis of the lungs and immunocompromised conditions are risk factors.
- The fungus settles in a cavity and grows to a big ball— called fungal ball.
- Majority of the cases are asymptomatic.
- Cough, chest pain, haemoptysis, abscess formation are the features.
- Diagnosis is by chest X-ray and CT scan (Fig. 62.21), majority of the cases do not require any treatment.
- In symptomatic cases—recurrent hemoptysis (rarely), removal of the lesion, lobectomy may be required.


Bronchogenic Carcinoma
Bronchogenic Carcinoma Introduction:
Bronchogenic cancer is the most frequent cause of cancer death in men and women and accounts for 14.5% of all cancer diagnoses and 27.6% of all cancer deaths in the United States. Cigarette smoking is unequivocally the most important risk factor in the development of lung cancer. In India, bronchogenic carcinoma has become number one cancer in men overtaking other cancers. The diagnosis is often delayeMany patients present as metastasis in bones. Surgical resection alone cannot be curative in many cases because of late presentation of the cases. Prognosis is poor in spite of the treatment.
Bronchogenic Carcinoma Risk Factors:
- Cigarette smoking: It is described as pack years—a pack containing 20 cigarettes. It is calculated by number of packs of cigarette smoked per day by the number of years he has smoked, e.g. one pack year is equal to smoking 20 cigarettes per day for one year.
- Industrial carcinogens: Asbestos, arsenic, chromium or nickel, organic chemicals, radon.
- Radon is the second leading cause of lung cancer. Radon is a natural radioactive gas released from the normal decay of uranium in the soil.
Bronchogenic Carcinoma Pathology—Types:
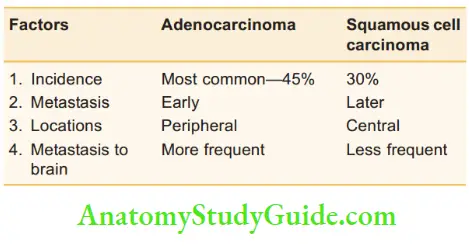
- Adenocarcinoma (ADA) of the lung is the most frequent histologic type and accounts for approximately 45% of all lung cancers. Women smokers have more incidence of adenocarcinomAdenocarcinoma of the lung develops from the mucus-producing cells of the bronchial epithelium. Cells are cuboidal to columnar cells. Most of these tumours (75%) are peripherally metastasise earlier than squamous cell carcinoma of the lung and more frequently to the central nervous system (CNS)—cases can present as weakness of the limbs, hemiparesis, etc.
- Bronchioloalveolar carcinoma is an adenocarcinom Sometimes it can be a more indolent disease. It is well differentiated and spreads along alveolar walls without invasion of stroma, blood vessels or pleura.
- Squamous cell carcinoma (SCCA) of the lung occurs in approximately 30% of patients with lung cancer. Approximately 75% of these tumours are centrally located and tend to expand against the bronchus, causing extrinsic compression. These tumours are prone to undergo central necrosis and cavitation. Squamous cell carcinoma tends to metastasise later than adenocarcinomMicroscopically, keratinisation, stratification and intercellular bridge formation are exhibiteSCCA may be more readily detected on sputum cytology than ADA.
- Large cell undifferentiated carcinoma may be made in approximately 10% of all lung tumours. These tumours tend to occur peripherally and may metastasise relatively early. Small cell lung cancer represents approximately 20% of all lung cancers; approximately 80% are centrally locateThe disease is characterised by an aggressive tendency to metastasise. It often spreads early to mediastinal lymph nodes and distant sites, especially bone marrow and brain.
- Small-cell lung cancer appears to arise in cells derived from the embryologic neural crest. Microscopically, these cells appear as sheets or clusters of small dense cells, with dark nuclei and little cytoplasm. This oat-like appearance under the microscope gives the term oat cell carcinoma to this disease. These tumours are often advanced at presentation, with an aggressive tendency to metastasise both by lymphatics and by blooChemoradiotherapy is generally used for treatment. However, the 5-year survival rate is only 5%.
Clinical comparison of extrahepatic with intrahepatic portal hypertension:
Bronchogenic Carcinoma Clinical Features:
- Cough and haemoptysis: It is a nonspecific symptom in many patients and diagnosis is delayed because it is often thought to be a smoker’s cough.
- Dyspnoea is due to pleural effusion or due to restrictive pulmonary disease.
- Bloody effusion, clubbing of the fingers, localised chest pain are other features.
- Hoarseness due to recurrent laryngeal nerve paralysis, back ache due to metastasis in vertebrae, or neurological features due to metastasis in brain are also presenting features in many cases.
- Myopathy similar to myasthenia gravis can occur in small cell carcinoma.
Bronchogenic Carcinoma Diagnosis and Spread:
- In addition to chest X-ray, CT scan, sputum for malignant cells, diagnosis can also be made with bronchoscopic biopsy and CT-guided biopsy. Spread is common PET scan: 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) is the investigation of choice to detect the distant lesions.
- Brain CT or magnetic resonance imaging (MRI).
- Mediastinoscopy.
- CT of the chest, abdomen, MRI brain: Mediastinal lymph node masses, metastases to the adrenal glands, brain, lung and bone are common.
- Bone metastases are osteolytiWhole body bone scan is needed.
Bronchogenic Carcinoma Treatment:
Can be grouped into three major categories:
1. Stages 1 and 2 tumours are contained within the lung and may be completely resected with surgery.
2. Resectable stages 3A and 3B tumours are locally advanced tumours with metastasis to the ipsilateral mediastinal (N2) lymph nodes (stage IIIA) or involving mediastinal structures (T4N0M0). These tumours, by their advanced nature, may be mechanically removed with surgery followed by systemic chemotherapy. Radiotherapy can also be given to locally advanced disease.
3. Stage IV disease includes metastatic disease and is not typically treated by surgery, except for patients requiring surgical palliation. Systemic therapies— chemotherapy for metastatic disease are common.






Congenital Heart Diseases
Congenital Heart Diseases Introduction:
- Abnormal heart structures since birth.
- It develops between 3rd and 8th week of foetal life.
- 1st operation for congenital heart disease was ligation of PDA by Gross in 1938.
- With new advances in neonatal cardiopulmonary bypass (CPB), outcomes have improved.
Congenital Heart Diseases Development:
- At 12 weeks, primitive vascular tube is fully developed.
- Foetal circulation differs from adult in that right and left ventricles pump blood in parallel rather than in series to receive increasingly oxygenated blood.
- 3 important structures are ductus venosus, foramen ovale and ductus arteriosus.
Changes at Birth:
- Pulmonary vascular resistance falls (breathing).
- Pulmonary vasodilation and ductus arteriosus constricts within 30 minutes of delivery (due to increased oxygen levels).
- Reversal of pulmonary and systemic pressure gradient. Termination of blood flow from pulmonary artery into aorta.
- Taping/cutting umbilical cord.
- Venous return from placenta stops.
- IVC and right atrial pressure decrease and left right atrial pressure increases (due to increased systemic vascular resistance).
- Foramen ovale closes.
Abnormalities
- Persistence of normal channels (patent ductus arteriosus—PDA, patent foramen ovale).
- Failure of septation (atrial septal defect—ASD, ventricular septal defect—VSD, tetralogy of Fallot—TOF).
- Stenosis (intracardiac—supravalvular, valvular, infravalvular, coarctation of aorta).
- Atresia/abnormal connections (transposition of great arteries—TGA, total anomalous pulmonary venous connections—TAPVC).
Incidence;
Eight cases per 1000 live births in the UK.
Congenital Heart Diseases Aetiology:
Unclear: Infection/envirotoxins/genetics.
Congenital Heart Diseases Diagnosis:
In utero foetal ECHO.
Congenital Heart Diseases Classification:
- Cyanotic (1/3rd) and acyanotic (2/3rd)
- Right to left shunts (similar to TOF)
- Left to right shunts (similar to ASD, VSD, PDA)
- Parallel systemic and pulmonary flow (similar to TGV)
- Aortic stenosis, coarctation of aorta
- Mixing of systemic and pulmonary flow (similar to TAPVC): Heart failure in infancy.
Cyanotic Congenital Heart Disease
1. Tetralogy of Fallot (TOF):
Most common cyanotic congenital heart disease:
The child adopts squatting posture during hypoxic spells which increases systemic vascular resistance and venous return to heart. This directs the blood into pulmonary circulation and oxygenation improves. Chest X-ray shows boot-shaped heart. Treatment—single or twostage surgery
2. Transposition of Great Vessels (TGA):
- Most common cause of cyanosis in newborn.
Congenital Heart Diseases Features:
- Aorta arises from right ventricle and pulmonary artery from left ventricle.
- Incompatible with life unless associated with ASD or VSD.
- Chest X-ray—‘Egg on side’ appearance.
Congenital Heart Diseases Treatment:
- Rashkind percutaneous balloon atrial septoplasty.
- Definitive repair—arterial switch (2 stages).
- Mustard or Senning surgery.
3. Total Anomalous Pulmonary Venous Drainage:
- Pulmonary venous drain disconnected from left atrium and drains to right side, e.g. inferior vena cava (IVC) or superior vena cava (SVC)
- Presents with failure to thrive.
- Treatment—surgery.
4. Eisenmenger’s Syndrome:
- It occurs following the reversal of a previous left to right shunt as with ASD or VSD.
- Similar to pulmonary hypertension.
- Closure of shunt contraindicated.
Acyanotic Congenital Heart Disease
1 . Patent Ductus Arteriosus:
Acyanotic Congenital Heart Definition:
Persistence of the foetal ductus arteriosus in the postnatal period.
Embryology:
- Derived from the 6th aortic arch
- Essential for the foetal circulation
- Blood ejected by right ventricle flows exclusively through the ductus to the lower extremity and placenta bypassing the high resistance pulmonary circulation in the foetus.
At Birth:
- Physiological closure occurs in 1–6 days
- Anatomical closure occurs in 2–3 weeks
Mode of Closure:
Smooth muscle constriction in response to rising arterial oxygen tension.
Pathophysiology:
Shunt occurs across the ductus both in systole and diastole resulting in left ventricle overload and pulmonary plethora.
- Shunt depends on the size of the ductus and pulmonary and systemic vascular resistance. Continuous murmur is due to shunt during both systole and diastole.
Acyanotic Congenital Heart Clinical Features:
- Incidence: M: F = 1:2
- It depends on the size of the ductus, pulmonary vascular resistance, age at presentation and associated anomalies.
- Small ductus: Asymptomatic
- Infants: Congestive heart failure
- Children: Dyspnoea on exertion, repeated respiratory tract infection.
Acyanotic Congenital Heart Complications;
- Reversal of shunt
- Infective endocarditis
- Congestive heart failure
Acyanotic Congenital Heart Treatment:
It can be divided into surgical and nonsurgical methods.
1. Surgical methods
- The presence of PDA is sufficient indication for surgery even without symptoms.
- In infants: Large PDA with congestive cardiac failure not responding to antifailure measures, surgery is indicated.
Surgery:
- Triple ligation
- Division and suturing
- Right lateral position and posterolateral thoracotomy
- Thorax entered through 4th intercostal space
- It can also be done by thoracoscopy and videoassisted thoracoscopic surgery (VATS) and clipping of PDA.
Care during surgery:
Left recurrent laryngeal nerve must be carefully preserved.
Complications during surgery:
- Haemorrhage, left recurrent laryngeal nerve palsy
- Chylothorax
2. Nonsurgical methods:
- Pharmacological closure: In preterm infants— indomethacin
- Transcatheter closure: Interventional cardiology
- Double umbrella device—Rashkind
- Gianturco coils
- Lock Clamshell occluder.
2. Coarctation of Aorta:
Coarctation of Aorta Definition:
Congenital narrowing of the descending thoracic aorta usually occurring just distal to the left subclavian artery origin, adjacent to the site of insertion of the ductus arteriosus.
Incidence:
- 0.2–0.6 per 1000 live births
- 5–8% of all cases of congenital heart diseases.
Coarctation of Aorta Aetiology:
Flow theory: Reduced flow in the aorta due to multiple abnormalities in the heart during the foetal period Ductal sling theory: When there is isolated coarctation, this theory is applicable. Abnormal extension of contractile ductal tissue into the adjacent aorta which results in coarctation.
Coarctation of Aorta Types:
Infantile—preductal and adult—juxtaductal.
Coarctation of Aorta Classification:
- Group 1: Isolated coarctation
- Group 2: Coarctation with VSD
- Group 3: Coarctation with complex intracardiac anomalies.
Coarctation of Aorta Clinical Features;
Depend on: Age and symptoms at presentation, location of the coarctation, severity of the coarctation, and associated anomalies.
Coarctation of Aorta Symptoms:
- Visual disturbances, exertional dyspnoea
- Upper extremity hypertension
- Headache, epistaxis
- Claudication of the lower limbs
Coarctation of Aorta Signs:
- A systolic murmur is heard over the precordium and posteriorly between the scapula.
- Feeble femoral pulses.
- Enlarged collateral vessels are seen (Suzman’s sign) and palpable between scapula and bruit can be heard here.
- The systolic gradient between arm and leg blood pressure.
Collaterals:
- Subclavian artery and its branches
- Internal mammary artery
- Intercostal artery
- Scapular, cervical, vertebral, epigastric and spinal arteries.
Coarctation of Aorta Investigations:
- ECG: LVH with LV strain
- CXR: Notching of the ribs (Dock’s sign) from the third rib onwards, above four years of age.
Coarctation of Aorta Diagnosis:
- Two-dimensional echocardiogram, cardiac catheterisation
- Transoesophageal echocardiogram (TEE)
- Angiogram
Coarctation of Aorta Treatment:
Nonsurgical (infants): Balloon dilation and stenting
2. Surgery
- Left posterolateral thoracotomy
- Thorax entered through the fourth intercostal space
- Arterial line in the right upper limb
- Preserve the vagus and recurrent laryngeal nerves
- Arterial line in the lower limb
- Lower limb pressure during cross-clamping of aorta, to be kept above 45 mmHg
- If the pressure is low, then create a shunt from the aortic arch to the descending thoracic aorta with the help of a cannula.
- Patch angioplasty.
Complications of surgery:
- Haemorrhage, RLN injury, phrenic nerve injury
- Horner’s syndrome, chylothorax
- Paradoxical hypertension, paraplegia, stroke.
Late complications
- Recoarctation, aneurysm and left arm ischaemia (when subclavian flap aortoplasty is done).
Pseudocoarctation: A rare condition which results from congenital elongation of the aortic arch which leads to redundancy and kinking of the aorta and may appear similar to coarctation but there is no obstruction to blood flow.
3. Atrial Septal Defect:
Defect in septum between left and right atrium leading to left to right shunt.
Atrial Septal Defect Types
ASD is of three types:
- Ostium secundum: Defect in floor of fossa ovalis. Presents late in life.
- Ostium primum: Endocardial cushion defect associated with mitral valve defects (mitral regurgitation) and trisomy 21. Presents earlier in life.
- Sinus venous: Defect near the junction of SVC and atrium.
Atrial Septal Defect Treatment:
Open heart surgery with CPB and closure of defect directly with sutures or with pericardial or synthetic patch.
4. Ventricular Septal Defect VSD is of four types:
- Perimembranous defect (in membranous septum): 70–80%
- Muscular defect (multiple): 10%
- Atrioventricular defect: 5%
- Subarterial defect: 5–10%
- O/E: Pansystolic murmur
Ventricular Septal Treatment:
Surgical repair: Open heart surgery with patch.
Coronary Artery Bypass Surgery
Coronary Artery Bypass Surgery Introduction:
Often simply called bypass surgery, it is the most commonly performed open heart surgery all over the world the incidence of coronary artery disease is rapidly rising in developing countries. A vein graft from the lower limb or an arterial graft (internal mammary artery or the radial artery) is used to bypass the obstructed coronary artery. The bypass is done from the root of the aorta to the distal coronary artery.
- The obstruction or the block is not touched.
Risk Factors for Coronary Artery Disease:
Incidence:
Least in Japan and highest in Finland.
Indications for Surgery:
- Usually indicated in symptomatic or for prognostic reasons (i.e. balance between expectant benefit and risk faced by the patient).
- >50% stenosis of left main stem artery
- >70% stenosis of the proximal left anterior interventricular artery
- Triple vessel disease
- Poor ventricular function associated with CAD.
- Chronic stable angina
- Acute coronary syndrome
- Surgery for complications of MI such as ventricular septal rupture, et
Coronary Artery Bypass Surgery Investigations:
- ECG/cardiac enzymes—Trop T and Trop I
- 2D echocardiogram—new stress ECHO
- Holter monitoring, thallium scan-201 or 99mTc
- Stress test (exercise tolerance test)
- Coronary angiogram
- Radionucleotide studies and cardiac MRI
- CT (multislice high resolution)
Contraindications of CABG:
- Small, diffusely diseased arteries
- Diffuse disease and heart failure
- Acute myocardial infarction over 6 hours old
- Moribund patients after resuscitation
Surgery:
- Bypass surgery with vein or artery graft
- Endarterectomy
- Venous patch
Bypass Surgery:
1. Techniques of bypass:
- Cold cardioplegia with moderate hypothermia and cardiopulmonary bypass.
- Ischaemic cross-clamp with moderate hypothermia with cardiopulmonary bypass.
- Empty beating heart, normothermic with cardiopulmonary bypass.
- Beating heart surgery, no heart lung machine.
2. Grafts:
- Veins—lower limbs (long saphenous vein)
- Upper limb (cephalic vein) rarely used
- Arteries—radial
- Internal mammary artery both right and left
- Gastroepiploic
- Inferior epigastric
- Inferior mesenteric
3. Nonautogenic conduits:
- Cryopreserved human saphenous vein allograft
- Processed bovine sacral artery
- Polytetrafluoroethylene graft (Gore-Tex)
Standard Surgical Procedure:
- Median sternotomy
- Internal mammary artery dissection done
- Pericardium opened
- Systemic heparinisation 3 mg/kg
- Aortic and venous cannulation.
- Cardiopulmonary bypass started
- Aorta cross-clamped and cold K+ rich solution given in the aortic root
- Heart arrested in diastole to achieve immobile surgical field
- Distal anastomosis completed
- Proximal anastomosis done with the heart beating
- Weaned off CPB
- Protamine given and decannulation carried out
- Sternum closed, extubation 6–8 hours later.
Complications of Surgery:
- Perioperative MI (2–3%)
- Stroke
- Arrhythmias (30%)
- Sinus tachycardia
- Atrial fibrillation
- Reinfarct
- Wound infection
- Bleeding
- General weakness
- Mortality (2–3%)
- Persistent poor cardiac output requiring inotropes or mechanical support
Mechanical support to low cardiac output patients post-CABG Intra-aortic balloon pump (IABP):
- Inserted percutaneously in the common femoral artery, threaded into the aorta till its tip lies in distal arch vessels.
- The balloon is triggered by the ECG, deflating during ventricular systole (decreasing afterload) and inflating during diastole (increasing diastolic pressure and blood flow to coronaries).
Coronary Artery Bypass Surgery Prognosis:
- Ability to return to normal lifestyle
- Improvement in ventricular function
- Work capacity better than preoperative
- The risk of arrhythmias is unchanged
- Minimal medications
- Complete and dramatic relief of chest pain.
Patency:

Recent Advances:
- Age limitation changed (CABG done in 80 years old also)
- Improved myocardial preservation
- Composite arterial grafts
- Sutureless anastomosis
- Endoscopic vein harvesting
- Intracoronary injections of vascular endothelial growth factor (VEGF)
Composite Arterial Grafts:
- Arterial grafts have long-term patency.
- Patients with total arterial grafts may not require future surgery.
- Arterial grafts are used in the shape of T or Y.
- It can revascularise almost all blocked major vessels.
Endoscopic Vein Harvesting:
- Only two small incisions
- With help of a subcutaneous tunnel, the vein is dissected
- Requires expensive equipment
- Major branches are tied and smaller ones are controlled by pressure
- Cosmetic advantage
- Takes longer time
Off Pump Coronary Artery Bypass Surgery
Coronary Artery Bypass Surgery Procedure:
- Beating heart surgery, no heart-lung machine
- Sternotomy, stabilisation devices used
- Short-acting beta-blockers to reduce the heart rate.
- Proper positioning of the heart with mechanical stabilisation device for proper visual presentation
- CPB standby, all vessels can be bypassed by proper position of heart, quick recovery, early extubation
- No CPB, less trauma, reduced risk of bleeding and kidney failure, reduced hospital stay.
Coronary Artery Bypass Surgery Advantages:
- Avoids physiological stress associated with CPB.
- Aortic manipulation leading to neurological complications avoid whole body inflammatory response that occurs due to CPB is decreased.
- The incidence of postoperative renal failure due to CPB is decreased.
Future Developments/Recent Advances:
- Bypass graft coupling devices to facilitate anastomosis (clips, stents).
- Normalising left ventricular geometry with intracardiac devices.
- Myocardial protection during CPB (ventricular assist devices). Ischaemic preconditioning pharmacologically preoperatively.
- Vascular intimal hyperplasia: Important cause of graft occlusion. Gene-based therapies to prevent this before grafting the veins.
- Minimally invasive direct coronary artery bypass (MIDCAB) surgery: Anterior submammary incision. LIMA dissected down with the aid of a thoracoscope and grafted to the LAD.
Abdominal Aortic Aneurysms (AAA)
- Aneurysms are defined as a focal dilatation of at least 50% larger than the expected normal arterial diameter.
- For AAA—transverse diameter 3 cm or greater
Risk Factors for AAA:
Site:
95%—infrarenal aorta, 5%—suprarenal aorta.
Salient Features:
Fates of aneurysm:
- Infection, rupture (free/contained), thrombosis, embolism.
Growth Rates:
<5 cm diameter—0.3 cm/year >5 cm diameter—0.5 cm/ year.
Abdominal Aortic Aneurysms Clinical Features:
Incidental finding:
- Pulsatile abdominal mass on palpation, detected during evaluation for another abdominal pathology or detected at surgery for unrelated abdominal or pelvic operation.
Classical triad:
- Sudden-onset midabdominal or flank pain
- Shock
- Presence of a pulsatile abdominal mass (expansile pulsation).
Palpation findings:
Firm mass, expansile pulsation over the mass and if upper border is palpable, then the origin is probably infrarenal.
Abdominal Aortic Aneurysms Diagnosis:
1. Chest X-ray round opacity, eggshell pattern of calcification
2. Abdominal ultrasound:
- Detail of the vessel wall
- Presence of plaques
- Size
3. CT—most precise:
- The proximal and distal extent can be made out.
- Amount and location of mural thrombus
- Calcifications
- Adjacent structures


4. MRI/MRA:
- Less frequently used
- Used if the patient has renal failure
5. Contrast arteriography:
Less frequently used
Abdominal Aortic Aneurysms Complications:
Abdominal Aortic Aneurysms Management:
Low-risk AAAs
- Followed by serial size measurements. Reduce expansion rate and rupture risk by conservative treatment such as:
- Smoking cessation
- Blood pressure control
- Reduction of cholesterol
- Risk factor modifications
- Drugs used: α-blockers, NSAIDs—inhibit elastase
- MMP inhibitors—doxycycline
- Repair is indicated when it is symptomatic or >1 cm/ year growth.
High-risk patients:
- Delay in repair until larger diameter
- Endovascular aneurysmal repair (EVAR) can be trie
Techniques of Open Repair:
- Transperitoneal approach
- Retroperitoneal approach is indicated in cases of hostile abdomen, suprarenal aneurysm, horseshoe kidney, peritoneal dialysis, inflammatory aneurysm and in ascites.
- Minimal incision aortic surgery: 12 to 15 cm incision, 9 cm proximal to the umbilicus.
Endovascular Aortic Aneurysm Repair:
Stent-graft is introduced into the aneurysm through the femoral arteries and fixed in place to the nonaneurysmal aortic neck and iliac arteries with self-expanding or balloon-expandable stents (Palmaz stents), or with barbs, pins or hooks.
Special Considerations:
1. Inflammatory aneurysm:
- Incidence is about 5%
- Adherent to: Duodenum, IVC, left renal vein, ureters—the reason being lymphatic obstruction during aneurysm expansion and secondary fibrosis and infection from chronic contained rupture
- Rupture is uncommon (as it is often symptomatic and treated before rupture)
- A retroperitoneal approach is preferred.
2. Aortocaval fistula:
- Continuous abdominal bruit +
- High-output cardiac failure
- ‘Steal’ phenomenon—ischaemia to the lower limbs.
- Treatment: Fistula closure followed by AAA repair.
3. Horseshoe kidney:
- The kidney usually fused anterior to the aorta
- Left retroperitoneal approach
- Endovascular repair is not possible.
Ruptured Abdominal Aortic Aneurysm
Types of Rupture:
- Anteriorly—into the peritoneal cavity.
- Posteriorly—into retroperitoneum.
Ruptured Abdominal Aortic Aneurysm Clinical Features:
Back and abdominal pain, pallor, diaphoresis and syncope. If untreated, it is fatal in all cases.
Ruptured Abdominal Aortic Aneurysm Treatment:
- Immediate surgical repair.
- If the patient is unstable + previously diagnosed or a pulsatile mass, he is transferred immediately to OT.
- If stable + questionable diagnosis, a CT and open surgical repair, control the haemorrhage + resuscitation + aneurysm repair. The early postoperative mortality rate is 45%.
Differential Diagnosis of Ruptured AAA:
- Angina pectoris, perforated peptic ulcer
- Acute pancreatitis, acute cholecystitis
- Acute diverticulitis, mesenteric vascular occlusion
- The prolapsed lumbar intervertebral disc, sciatica

Chest Trauma, Cardiothoracic Surgery Multiple Choice Questions
Question 1. Fracture of the following rib is a marker of severe trauma:
- First
- Fourth
- Eighth
- Tenth
Answer: 1. First
Question 2. Treatment of the posterior flail segment is:
- Strapping
- Open reduction and fixation
- No treatment is required
- External fixator application
Answer: 3. No treatment is required
Question 3. Posterior flail segment does not require treatment because:
- The scapula supports the flail segment
- It does not cause complications
- It heals by itself
- It has no physiological implications
Answer: 1. Scapula supports the flail segment
Question 4. ‘Internal pneumatic fixation’ for flail chest is the term used for:
- Insertion of a balloon into the chest
- Internal fixation with screws
- Endotracheal intubation and positive pressure ventilation
- Valsalva manoeuvre
Answer: 3. Endotracheal intubation and positive pressure ventilation
Question 5. Tension pneumothorax should immediately be treated with:
- Intercostal tube insertion
- Needle thoracostomy
- Thoracotomy
- Thoracoscopic drainage
Answer: 2. Needle thoracostomy
Question 6. Features of tension pneumothorax include all of the following except:
- Tachypnoea
- Hypotension
- Dull note on percussion
- Tachycardia
Answer: 3. Dull note on percussion
Question 7. Indications for thoracotomy in haemothorax include all of the following except:
- Drainage more than 1000 ml
- Drainage of more than 100 ml/hour for 4 hours
- If clotted, haemothorax is suspected
- Coagulation abnormalities
Answer: 4. Coagulation abnormalities
Question 8. The intercostal drain can be removed in all of the following situations except:
- Lung is fully expanded
- Drainage < 100 ml
- No air leak
- The patient is on a ventilator
Answer: 4. The patient is on a ventilator
Question 9. The following is the diagnostic of surgical emphysema:
- The lungs are emphysematous
- Always follows surgery
- Palpable crepitus
- Infiltrates on chest X-ray
Answer: 3. Palpable crepitus
Question 10. The following is true about mediastinal emphysema except:
- The emphysema is mainly suprasternal
- A mediastinal drain needs to be inserted
- Pericardial crunching sounds can be heard on auscultation
- Oesophageal and tracheal injury need to be ruled out
Answer: 2. Mediastinal drain needs to be inserted
Question 11. Nontraumatic rib fractures may be seen in all of the following except:
- Hypoparathyroidism
- Metastatic disease
- Older patients after violent coughing
- Osteogenesis imperfecta
Answer: 1. Hypoparathyroidism
Question 12. The classic ‘three’ sign of coarctation of aorta is formed by all of the following except:
- Dilated left subclavian artery
- Narrowing of coarctation
- Post-stenotic dilatation of aorta
- Dilated pulmonary artery
Answer: 4. Dilated pulmonary artery
Question 13. Most common type of aneurysm with a propensity to rupture:
- Abdominal aortic aneurysm
- Carotid artery aneurysm
- Radial artery aneurysm
- Cerebral artery aneurysm
Answer: 1. Abdominal aortic aneurysm
Question 14. The most common cause of noncardiac complication after abdominal aortic aneurysm repair is:
- Pulmonary insufficiency
- Cerebral insufficiency
- Renal insufficiency
- Hepatic insufficiency
Answer: 3. Renal insufficiency
Question 15. The most common cause of respiratory insufficiency following chest trauma is:
- Pulmonary contusion
- Pneumothorax
- Flail chest
- Haemothorax
Answer: 2. Pneumothorax
Leave a Reply