Case History Introduction
A complete case history of the child is obtained from the parents during his first dental visit. The child is encouraged to participate if he/she has the cognitive ability to do so. A complete case history comprises many parameters, including the demographic details of the patient and the chief complaint recorded in the patient’s own words.
Table of Contents
It also includes a prenatal, natal and post-natal history of the patient, past treatment history and personal history. Each parameter is discussed in detail in this chapter. In case of emergency, complete history cannot be obtained. The details pertaining to the chief complaint are recorded. After obtaining the case history, the child is thoroughly examined.
Read And Learn More: Paediatric Dentistry Notes
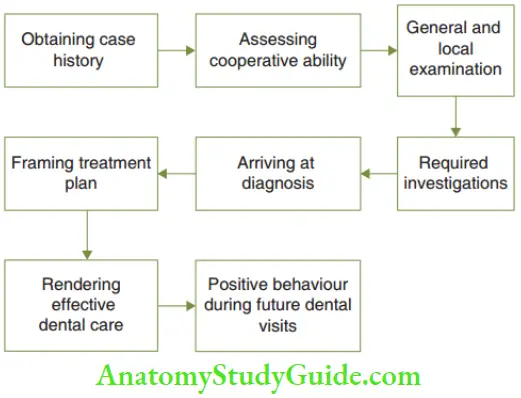
General examination of the child and local examination of the orofacial structures are conducted to decide the appropriate investigations. In addition, an assessment of the cooperative ability of the child is also required to arrive at the diagnosis. The treatment plan is based on an accurate diagnosis.
A clearly drawn treatment plan is necessary for the successful delivery of dental care to children. The effective and efficient treatment creates positive behaviour in the patient during his future visits.
Demographic Data
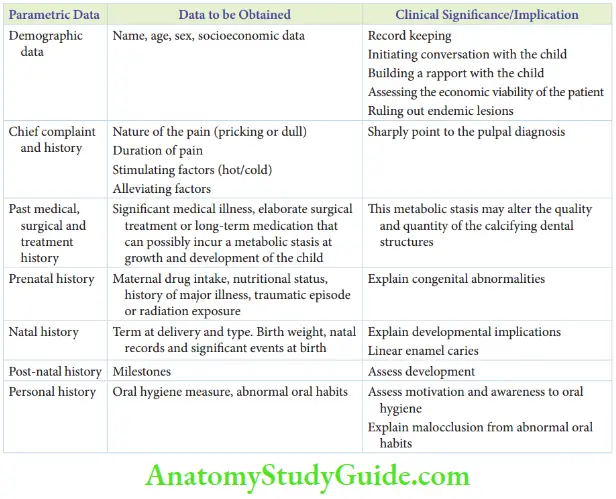
Demographic data consists of the name, age, sex and socioeconomic status of the patient. It is useful for initiating conversation and building a rapport with the child. The possibility of endemic diseases can be identified and the economic status of the patient can be assessed. Demographic details are also important to record the cases and refer to during future visits.
- Name: The name of the child is used for record purposes. Enquiring the pet name of the child prior to the appointment creates familiarity with the child. The dentist becomes a known person and calling by the pet name allays the stranger anxiety in the child.
- Age and sex: The chronological age is the number of years since the birth of the child. The dental age is based on the eruption of teeth. The other means of expressing age are listed.
- Socioeconomic data: The address of the child and the occupation of the parents can throw light on the socioeconomic viability of the patient/guardian to obtain rehabilitative care. Also, the address will help in diagnosing endemic lesions such as fluorosis. The level of education of the parents and assessment of their awareness on dental diseases can help in deciding the type of awareness programme and oral hygiene motivation exercise required.
- Different Means of Expressing Age
- Skeletal age: The age based on the skeletal maturation, indicated on a hand–wrist radiograph or vertebrae.
- Biological age: It refers to the biological maturation of the child.
- Mental age: The age corresponding to the IQ of the child. It is calculated with the following formula:
- Circumpubertal age: The age is based on the growth spurt of the child. There are four growth spurts:
- Prenatal growth spurt: Period before birth
- Post-natal growth spurt: 1 year after birth
- Mixed dentition or pre-pubertal growth spurt
- 7–9 years in girls
- 8–10 years in boys
- Pubertal growth spurt
- 9–11 years in girls
- 11–13 years in boys
Chief Complaint
The chief complaint is the presenting complaint of the patient in his/her own words. If the child is unable to communicate, it can be recorded in the parent’s words. The chief complaint has to be specific and lucid.
The history of presenting illness should include the details of the chief complaint. For instance, if the child complains of pain, the nature (pricking or dull) and duration of pain have to be enquired about. Some factors such as hot or cold food may aggravate the pain while some medication may relieve the pain. All these have to be recorded.
If there is more than one complaint, the order of occurrence has to be noted.
Past Treatment History
Past treatment history includes past medical, surgical and dental history.
- Past medical history: Earlier episodes of chronic systemic illness and the medication administered have to be recorded. These may have dental implications. For instance, a child may have been affected by exanthematous fever at the age of 5 years. This may influence the calcification of the middle and cervical regions of premolars and second molars. Later, it may manifest as enamel hypoplasia. Hypoplastic bands around the premolars and second molars at the age of 13 years must be correlated with the exanthematous fever that occurred at the age of 5 years. Tetracycline antibiotics may have been administered to a child, younger than 8 years, suffering from recurrent respiratory infections. The region of permanent teeth calcifying at that time may exhibit tetracycline stains.
- Past surgical history: A relatively elaborate surgery during childhood may be followed by a phase of recuperation, rest and metabolic stasis. This metabolic stasis may alter the quality and quantity of the calcifying dental structures.
- Past dental history: History of the earlier dental appointment, the chief complaint and the treatment performed may guide the prospective requirement of necessary investigations. The number of visits and the behaviour displayed by the child may indicate the expected behaviour/dental attitude of the child in the present situation.
Prenatal History
The presence of the mother is mandatory during the appointment for obtaining the prenatal history of the child. It is obtained under file headings reflecting the events during gestation.
- Drug intake: Any drug with an appropriate size and ionic charge can cross the placental barrier and cause teratogenicity. Tetracyclines, immunosuppressant drugs and phenytoin are some examples. Alcohol can also cross the placental barrier. High intake of alcohol during the second trimester of pregnancy can cause foetal facial malformations. Foetal alcohol syndrome produces typical facies with proneness to clef palate, saddle nose, hypoplastic maxilla and hypertelorism.
- Major illness: A major illness of the mother during gestation can affect the foetus. For instance, maternal rubella (German measles) is a major cause of cardiovascular malformations in children. Sexually transmitted diseases such as syphilis and AIDS can be vertically transmitted from the mother to the foetus.
- Nutrition: Good nutrition is essential to the mother as high metabolic activity prevails during gestation. Poor quality of nutrition can affect the growth and maturation of the calcifying structures of the foetus including teeth. Vitamins A, E and D and trace elements are highly essential nutrients.
- Trauma: Physical and psychological trauma of the expecting mother during gestation can lead to higher levels of stress hormones (catecholamines) in her. The increased hormone levels can cause metabolic alteration in the foetus.
- Radiation exposure: Th foetus is at high risk when an expectant mother is irradiated as the proportion of undifferentiated totipotential cells is more. A lead apron is mandatory for the expecting mother if investigative dental radiographs are required. Acute distress/demise of the foetus or serious congenital malformations may result following irradiation.
Natal History
Events during the birth of a child constitute the child’s natal history. The following data is recorded in the natal history.
- Gestational age at delivery: Th gestational age of delivery can have an influence on the dental structures.
- 38 weeks of gestation – Full term
- 34–38 weeks ofgestation – Borderline
- 28–38 weeks of gestation – Pre-term
- Less than 28 weeks – Foetus is not viable A child born during the pre-term period may experience the following disturbances in dental structures:
- Delayed eruption and exfoliation of primary teeth
- Delayed eruption of permanent teeth
- The neonatal line is the line of demarcation between calcifying structures formed before and after birth. It is exaggerated into a band called a neonatal band. It represents a longer period of stasis during the formation of dental structures.
- The neonatal band is hypoplastic and the progression of dental caries in this region is more rapid and linear in the pattern. It is termed linear enamel caries.
- Type of delivery: The delivery of a baby can be through normal vaginal delivery or C-section or facilitated with the help of a forceps. A baby born by forceps delivery has an increased risk of temporomandibular joint damage. This is because the forceps is applied at the pre-tragus area during delivery.
- Birth weight:
- Normal birth weight – 2.5 to 3.5 kg
- Low birth weight (LBW) – 1.8 to 2.5 kg
- Very low birth weight (VLBW) – Less than 1.8 kgLBW or VLBW babies are associated with delayed biological and dental ages. Primary teeth eruption, their exfoliation and permanent teeth eruption are expected to be delayed in these cases. The orthodontic treatment may have to be appropriately timed in such cases.
- Head circumference and C-R length: Head circumference at birth and the crown-rump length are obtained from the prenatal records. The normal head circumference at birth is 33½ cm. A larger head circumference may indicate hydrocephalus and a smaller head circumference may indicate microcephaly.
- Other significant events at birth such as blue baby, cyanosis, kernicterus and erythroblastosis are recorded. The birth events cause metabolic insult to the system. It leads to a transient halt in the calcification or significant alteration in the matrix formation/mineralisation curve of all the developing teeth, especially primary teeth and permanent first molars.
Erythroblastosis and kernicterus result in intrinsic staining of the developing teeth when the matrix formation is altered.
The presence of natal teeth is also recorded.
Post-Natal History
From the birth of a child, various milestones indicate his growth. The correct order of significant milestones is turning on the back, balancing on all four limbs, crawling, standing with support and standing alone and walking with support and walking alone. The age of occurrence of every milestone has to be recorded. A child should be able to walk with or without support by the end of1 year.
A delay in the attainment of biological milestones would implicate/suggest a prospected delay in dental development also. Development of speech and language is more rapid during the second half of the second year. By 18 months, the child will be able to say around 50 words. The vocabulary upsurges to 2000 words by the age of 2 years.
Personal History
- Oral hygiene history: Oral hygiene measures followed by the child including the frequency and technique of tooth brushing are enquired. It is appropriate if the child brushes twice a day with a prescribed kid-sized toothbrush and paediatric toothpaste. Fone’s technique is the best toothbrushing technique for children. Unit 6 discusses oral hygiene of children.
- Habit history: Children may have some abnormal oral habits such as thumb/finger sucking, tongue thrusting, mouth breathing and bruxism. The frequency and duration of performing the habit are recorded. The intensity or oral force with which it is performed is also noted.
- Diet history: A 1-day diet chart can be recorded to assess the cariogenicity or number of dietary sugar exposures to the child. Obtaining a diet chart and diet counselling are elaborate.
Summary
During the first dental visit of a child, a complete case history is obtained from the parents to assess the clinical implications.
Leave a Reply