Nasociliary nerve
Nasociliary nerve Introduction:
Table of Contents
Nasociliary nerve is the branch of ophthalmic division of trigeminal nerve. It is sensory nerve to the Whole eyeball (eye, cornea, iris and ciliary body but not conjunctiva), Paranasal air sinus, mucous membrane of the nasal cavity, and Skin of the external nose.
1. Nasociliary nerve Course and relations
- Runs through the tendinous ring between the two divisions of oculomotor nerve.
- Passes by sitting on optic nerve I ON optic nerve)! and below superior rectus.
- Enters anterior ethmoidal foramen as anterior ethmoidal nerve.
- Runs in the roof of middle and anterior ethmoidal air cells.
Read And Learn More: Face Anatomy Notes And Important Questions
2. Nasociliary nerve Branches of nasociliary nerve
1. Communicating branches to ciliary ganglion: It forms sensory root to ciliary ganglion.
2. Nasociliary nerve Collateral branches
Long ciliary nerve:
It is sensory to
- Cornea,
- Iris, and
- Ciliary body.
It is sympathetic to dilator pupillae.
- Posterior ethmoidal nerve: It is sensory to following air sinuses
- Posterior ethmoidal sinus, and Sphenoidal air sinus.
3. Nasociliary nerve Terminal branches
Infratrochlear nerve (smaller terminal branch): It is sensory to
- Conjunctiva,
- Lacrimal sac,
- Caruncle,Medial end of eyelids, and
- Upper half of the external nose.
Anterior ethmoidal nerve (larger terminal branch): It is sensory to
- Anterior ethmoidal sinus,
- Middle ethmoidal sinus.
- Dura mater of anterior cranial fossa
- Mucosa of nose, and
- Skin of the lower half of the nose.
3. Applied anatomy: A lesion of the nasociliary nerve at the superior orbital fissure causes Paraesthesia in the forehead and nose, and Loss of corneal blink reflex.
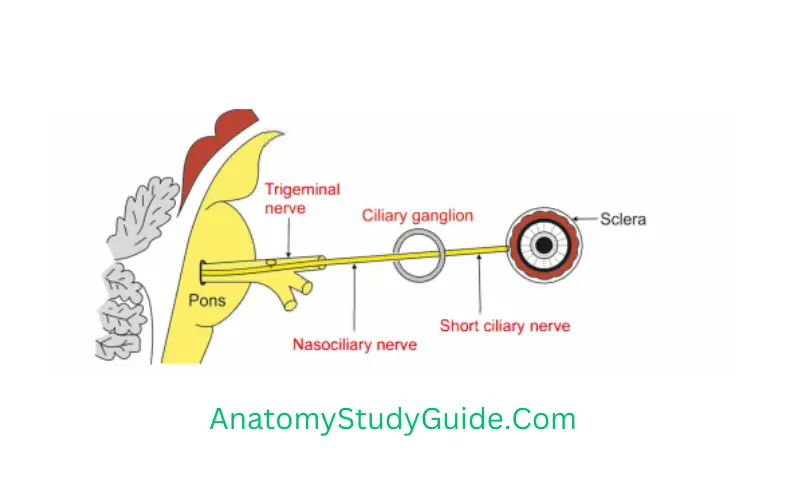
Short Ciliary Nerves
1.Short Ciliary Nerves Origin: Arise from ciliary ganglion. They are 15 to 20 in number.
2. Short Ciliary Nerves Course: They pass with the optic nerve to the back of the eyeball.
3. Short Ciliary Nerves Distribution: They supply
- Ciliary body (oculomotor nerve fibres), which is concerned with accommodation.
- Circular muscle of iris (oculomotor nerve fibres), which constricts the pupil.
- Radial fibres of iris (sympathetic nerve fibres), which dilate the pupil.
Question1: What is squint (strabismus)?
Answer 1. It is weakness or paralysis of muscles of eyeball.
2. squint may be concomitant or paralytic.
- Concomitant squint is congenital.
Movements are not affected and there is no diplopia. - In paralytic squint, movements are limited.
There is diplopia and vertigo.
The head is turned in the direction of the function of paralysed muscle.
There is a false orientation of the field of vision.
What is Tenon’s capsule?
1. Tenon’s capsule Definition:
It forms a thin, loose membranous sheath around the eyeball.
2. Tenon’s capsule Extent:
It extends from the optic nerve to the sclerocorneal junction.
3. Tenon’s capsule Function:
Free movement of eyeball within the sheath.
4. Tenon’s capsule Structures piercing
- Tendons of the various extraocular muscles.
- Ciliary vessels.
- Ciliary nerves.
5. Tenon’s capsule Expansions
- A tubular sheath covers each orbital muscle.
- The medial check ligament is a strong.lar expansion of medial rectus muscle.
- It is attached to the lacrimal bone.
- The lateral check ligament is a stronglar expansion from the sheath of the lateral rectus muscle.
It is attached to zygomatic bone. - The lower part of Tenon’s capsule is thickened and is named the suspensory ligament of the eye or the suspensory ligament of Lockwood.
It is expanded in the centre and narrows at its extremities and is slung like a hammock below the eyeball. - It is formed by union of margins of sheaths of Inferior rectus and Inferior oblique muscles with Medial and lateral check ligaments.
Question 2: What is the mode of blood supply of optic nerve?
It is divided into arterial supply and venous return.
1. Optic Nerve Arterial supply:
The arteries form plexus. They are derived from two sources
Plexus formed by the
- Superior hypophyseal artery, branch of internal carotid artery,
- Ophthalmic artery,
- Posterior ciliary artery (branch of ophthalmic artery), and Extraneural branches of central artery. Branches of the central artery.
2. Venous return: Central vein.
Palpebral (canthal) ligaments
These ligaments connect the tarsal plates to the orbits. They are medial and lateral palpebral ligaments.
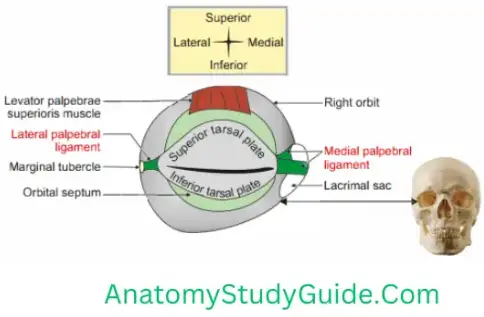
Medial palpebral ligament
- It is well-developed.
- It is superficially situated.
- It conncts medial ends of two tarsal plates to the anterior lacrimal crest and frontal process of maxilla.
- At its insertion, it splits into tarsal plates to surround lacrimal canaliculi. It lies in front of nasolacrimal sac and the orbital septum.
Lateral palpebral ligament
- It is poorly developed.
- It extends from the lateral ends of tarsal plates to small tubercle on the zygomatic bone (Whitnall’s tubercle).
- It is deeply situated.
- It lies deep to orbital septum and lateral palpebral raphe of orbicularis oculi.
Question 3: Describe extraocular muscles under the following heads:
1. Attchments (origin and insertion),
2. Action,
3. Nerve supply, and
4. Applied anatomy
The extraocular muscles are voluntary and involuntary.
Voluntary muscles are
- Four recti,
- Two obliqui, and
- Levator palpebrae superioris.
Four recti:
- Superior rectus,
- Inferior rectus,
- Medial rectus, and
- Lateral rectus.
Obliqui
- Superior oblique
- Inferior oblique
Levator palpebrae superioris
Involuntary: Orbitalis
1. Attachments
- Origin of recti:The recti muscles arise from the respective positions of a common I tendinous ring.
The ring is attached to the orbital surface of the apex of the orbit.
The lateral rectus has an additional small tendinous head, which arises from the orbital surface of greater wing of sphenoid bone. - B. Insertion of recti:
The recti are inserted into the sclera in front of the equator.
They are inserted few mmposteriorto thesclerocomeal junction.
The approximate distances of the insertion are I. 5, 6, 7, 8 mm MILSI
- Medial rectus: 5 mm behind the sclerocomeal junction.
- Inferior rectus: 2 mm behind the sclerocomeal junction.
- Lateral rectus: Z mm behind the sclerocomeal junction.
- Superior rectus: . mm behind the sclerocomeal junction.

Note: Visualise a clock. The 12 O’clock position represents superior rectus, 3 O’ clock medial rectus, the 6 O’ clock inferior rectus and 9 O’ clock positions represent lateral rectus.
Now focus at 6 O’clock position, the digit 6 of 6 O’ clock represents th insertion of inferior rectus behind sclerocorneal junction.
The digit prior to 6 is 5 and represents the insertion of medial rectus.
The digits after 6 are 7 and 8 which represent the insertion of lateral rectus and superior rectus.
1. Two obliqui:
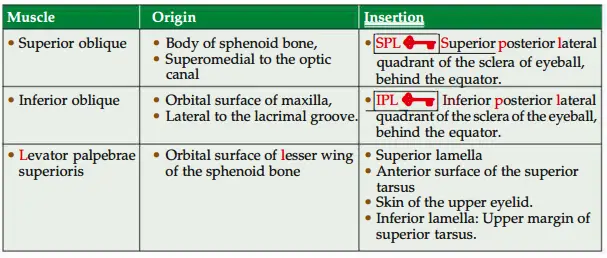
All extraocular muscles arise from apex of orbit except inferior oblique which arises from floor of orbit.
Involuntar muscles
- Superior tarsal muscle is the deep part of levator palpebrae superioris. It is inserted on the upper margin of superior tarsus.
- Inferior tarsal muscle connects the inferior tarsus of the lower eyelid to the fascia! sheath of the inferior rectus and inferior oblique. It helps in depression of lower lid.
- Orbitalis muscle bridges the inferior orbital fissure.
2. Action
- Action of individual muscles.
- Superior rectus: Elevation, adduction, intorsion.
- Inferior rectus: Depression, adduction, extorsion.
- Inferior oblique: Elevation, abduction, extorsion.
- Superior oblique: Depression, abduction, intorsion.
- Medial rectus: Adduction.
- Lateral rectus: Abduction.



Muscles bringing particular action.
- Adduction: Medial rectus, superior rectus and inferior rectus.
- Abduction: Lateral rectus, inferior oblique and superior oblique.
- Elevation: Superior rectus and inferior oblique.
- Depression: Inferior rectus and superior oblique.
- Intorsion: Superior rectus and superior oblique.
- Extorsion: Inferior rectus and inferior oblique.
3. Nerve supply
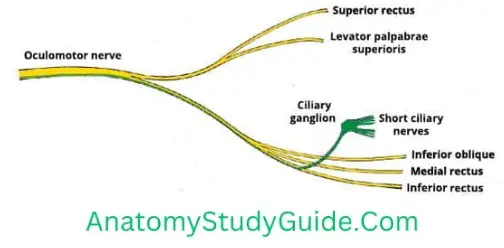
- All the extaculaI socular muscle superior oblique,of supplied the eyeball by are trochlear supplied nerve by oculomotor(4th cranialnerve exceptnerve) and ateral rectus supplied by abducent nerve (6th cranial nerve) (superior,inferior and medial recti, inferior oblique and levator palpebrae superioris are supplied by oculomotor nerve).
S04, LR6 and R3-superior oblique by 4th (trochlear nerve), lateral rectus by 6th (abducent) and rest all muscles by 3rd
cranial nerve (oculomotor). - Tarsal muscles are supplied by carotid nerve. The fibres of the nerve are postganglionic sympathetic fibres arising frm superior cervical sympathtic ganglion.
Applied anatomy
The muscles of eyeball are tested in following ways .
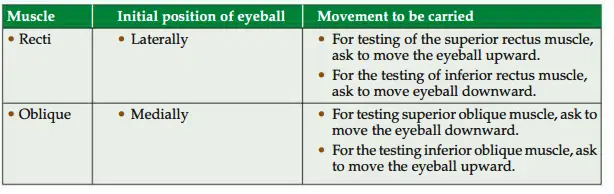
Oculomotor nerve lesion produces
Lateral strabismus,
In complete ophthalmoplegia
- There is paralysis of the muscles of the eyeball.
- Ptosis of the eyelid.
- Pupil is dilated (mydriasis).
- Loss of accommodation reflex.
Trochlear nerve lesion produces diplopia (double vision) when looking downwards.
Individuals with diplopia usually experience difficulty and
apprehension on descending staircase.
Abducent nerve lesion produces medial strabismus {squint (to have eyes that look in different direction)}.
In this condition, the two eyes appear to look in different directions. Diplopia is minimal when looking to the opposite side of the lesion.
- Nystagmus is characterized by involuntary, rhythmical oscillatory movements of the eyes. This is due to incoordination of the ocular muscles. It may be either vestibular or cerebellar in origin.
Ciliary ganglion
Introduction: It is collection of cell bodies of parasympathetic nerve. It supplies the
sphincter pupillae muscle.
1. Size: Pinhad.
2. Content: Cell bodies of multipolar neuron. @
3. Situation: Apex of the orbit in the angle made by optic nerve and lateral rectus “muscle.
4. Relations
- Medially: Optic nerve.
- Laterally: Lateral rectus muscle.
5. Connections: Three roots
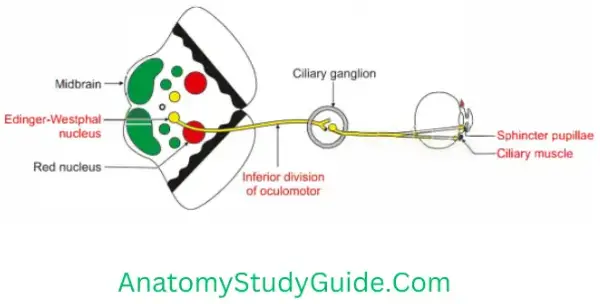
Motor (parasympathetic)
- Preganglionic fibres arise from Edinger-Westphal nucleus > lower division of 3rd nerve > ciliary ganglion > fibres are relayed into ciliary ganglion.
- Postganglionic fibres carried by short ciliary nerve and supply
- Sphincter pupillae, and
- Ciliaris muscle.
Sensory: Nasociliary fibres pass through ciliary ganglion without relay.
Sympathetic fibres pass through the ciliary ganglion without relay.
- Preganglionic fibres arise from spinal nerve and reach to superior cervical sympathetic ganglion.
- Postganglionic fibres arise from the plexus around ophthalmic artery pass through short ciliary nerve and supply dilator pupillae.
6. Branches:8 toThe10 short ciliary nerves
7. Peculiarity: postganglionic parasympathetic fibres of ciliary ganglion are myelinated.
8. Applied anatomy
1. Complete division of oculomotor nerve is manifested as NEEr
- Eyeball is depressed and abducted. “Down and out”. External strabismus: Due
to unopposed action of lateral rectus.
Ophthalmoplegia >Diplopia where false image is higher than true image. - Ptosis: Drooping of eyelid due to involvement of levator palpebrae muscle.
- Sphincter pupillae is not functioning. It results into dilatation of pupil
(mydriasis) - Dilated and fixed pupil.
- Loss of accommodation reflex because of paralysis of three muscles.
Medial rectus-medial convergence of eyeball is lost.
Sphincter pupillae-pupillary constriction is lost.
Ciliaris muscle-thicknss of lens. - Apparent protrusion of eyeball due to flaccid paralysis of most of ocular muscles.
2. Neurosyphilis causes inflammation of posterior cerebral and superior cerebellar arteries. This compresses oculomotor nerve.
3. Weber’s syndrome: Contralateral hemiplegia (upper motor neuron lesion) and ipsilateral paralysis of muscles supplied by oculomotor nerve.
What happens in case of unilateral ocular muscle paralysis?
1. Paralysis of a muscle will cause limitation of movement of the eyeball. One will
have double vision when one attempts to use the muscle.
1.When the abducent nerve supplying the lateral rectus is paralyzed, the individual cannot abduct the eyeball on the affected side. The eyeball is fully adducted by the unopposed pull of the medial rectus.
2.In complete 3rd nerve paralysis, the
- Eye cannot be moved upward, downward or inward.
- At rest, the eye looks laterally (external strabismus) because of the activity of the lateral rectus, and
- Downward because of the activity of the superior oblique.
- The patient has double vision (diplopia).
Drooping of the upper eyelid (ptosis) occurs because of paralysis of the levator palpebrae superioris.
The pupil is widely dilated and non reactive to light because of the paralysis of the sphincter pupillae and the unopposed action of the dilator pupillae (supplied by the sympathetic). - Accommodation of the eye is lost.
3. In 4th nerve paralysis, the patient complains of double vision on looking straight downward.
This is because the superior oblique is paralyzed and the eye turns medially as the inferior rectus pulls the eye downward.
4. In 6th nerve paralysis, the patient cannot
- Tum the eyeball laterally.
- When looking straight ahead, the lateral rectus is paralyzed, and
- Unopposed medial rectus pulls the eyeball medially, causing internal strabismus.
Question4 : Why the paralysis of extraocular muscles causes diplopia?
1. The perception of two images of a single object is called diplopia.
2. The objects lying in different parts of the visual field produce images over different spots on the retina.
3. The brain judges the position of an object by the position at which its image is formed on the retina.
4. Normally, the movements of the right and left eyes are in perfect alignment, and an object casts an image on corresponding spots on the two retinae so that only one image is perceived by the brain.
5. When a muscle of the eyeball is weak, and a movement involving that muscle is performed, the movement of the defective eye is slightly less than that of the normal eye.
6. As a result, images of the object on the two retinae are not formed at corresponding points but over two points near each other.
The brain, therefore, ‘sees’ two images,one from each retina.
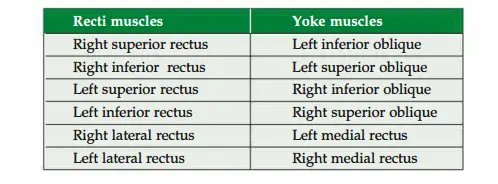
Question5 : What is conjugate movements of eyes?
Normally, movements of the two eyes are harmoniously coordinated.
Such coordinated movements of both eyes are called conjugate ocular movements.
Question6 : What is nystagmus?
Answer: 1. An involuntary rhythmical, oscillatory movement of eyeball is called nystagmus.
2. This is due to incoordination of the ocular muscles. It may be either
- Vestibular or
- Cerebellar, or even
- Congenital.
Orbital nerve
It is a branch of pterygopalatine ganglion. It is actually branch of maxillary nerve. It also carries parasympathetic and sympathetic fibres which pass through the ganglion.
1. Course: It passes through the inferior orbital fissure.
2. Distribution: It supplies the
- Periosteum of the orbit, and
- Orbitalis muscle.
- Mucous membrane of sphenoidal and ethmoidal air sinuses.
Leave a Reply