Cranial Cavity Anatomy Notes And Important Questions With Answers
Question: Why the bleeding or pus collection beneath the pericranium is not extensive?
Table of Contents
Answer: Pericranium is attached to sutures and does not cross the sutural line.
Therefore, it is restricted to underlying bone.
Read And Learn More: Face Anatomy Notes And Important Questions
Question 2: Why is it not advisable to feel both the carotid pulsations simultaneously?
Answer: Feeling the pulsations of both carotid arteries simultaneously may block the blood supply to the brain.
This can prove to be fatal.
Hence, pulsations of both common carotid arteries are not palpated simultaneously.
Question 3: Cephalohydrocoele
Answer: Cephalohydrocoele: Serous or watery accumulation under the pericranium. The CSF accumulates beneath the pericranium due to tear of dura and arachnoid mater.
It is called traumatic meningocoele.
Such swellings are restricted to the bones of vault and take the shape of underlying bone.
Question 4: Cephalhaematoma
Answer: Definition: It is the collections of pus or blood beneath the pericranium.
Dura mater is firmly attached to the sutural lines.
Therefore, it takes the shape of underlying bone.
It is particularly seen in birth injuries as a result of trauma.
Define venous sinuses and enumerate different venous sinuses.
1. Venous
These are the spaces in the cranium lined by endothelium, present In between two layers of dura mater (endosteal and meningeal) except inferior sagittal and straight sinuses which are in between two meningeal layers.
Non-compressive in nature, without Valves and Smooth muscles,
Absorbs cerebrospinal fluid through arachnid granulations,
Receives valveless emissary veins, which Equalize venous pressure within and outside the skull.
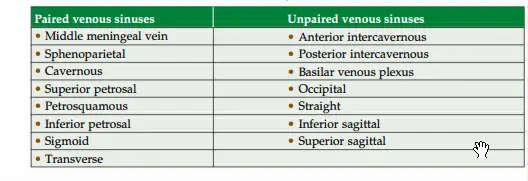
2. Venous Classification
- Paired
- Unpaired
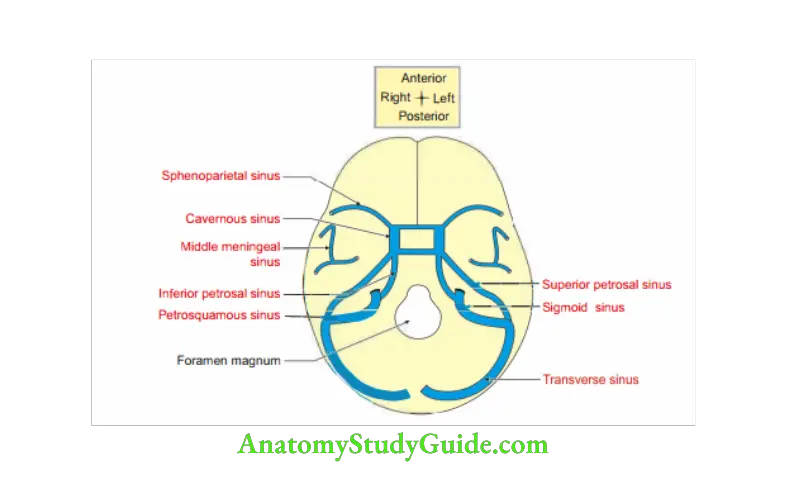
The paired sinuses can be recollected by visualizing interior of skull and starting in th middle cranial fossa as the sequence below and take the help of th diagram.
Describe cavernous sinus under the following heads:
1. Formation,
2. Relations,
3. Extent,
4. Contents,
5. Communications, and
6. Applied anatomy
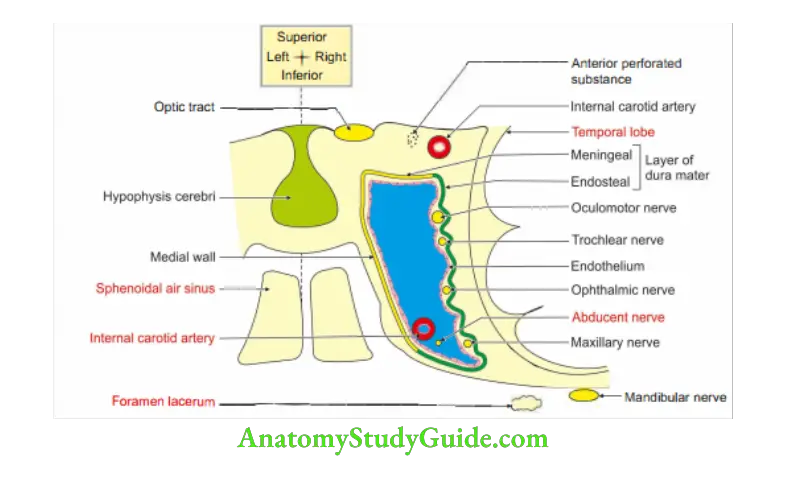
1. Cavernous Sinus Formation
- Roof and lateral wall: Meningeal layer of dura mater.
- Floor: Endosteal layer of dura mater.
- Medial wall
Meningeal layer of dura mater, and
Endosteal layer of dura mater.
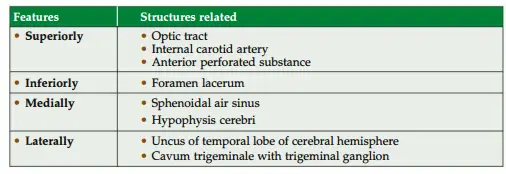
2. Cavernous Sinus Relations
3. Cavernous Sinus Extent: Apex of orbit to the apex of petrous part of temporal bone.
4. Cavernous Sinus Contents: True content is blood.
- Other structures are separated by a layer of endothelium.
- Structures passing through the sinus
Internal carotid artery with sympathetic nerve and venous plexus.
Note: This is only artery in the body lined inside and outside by endothelium.
Abducent (VI) nerve (below and lateral to internal carotid artery).
Structures in the lateral wall (from below upwards) I. …O.I
Maxillary nerve-2nd division of trigeminal nerve-5th cranial nerve
Oculomotor nerve-3rd cranial nerve
Irochlear nerve-4h cranial nerve
Ophthalmic nerve-1st division of trigeminal nerve-5th cranial nerve.
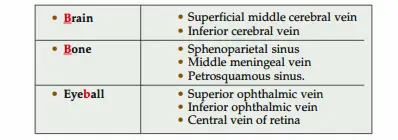
Cavernous Sinus Incoming channel: From
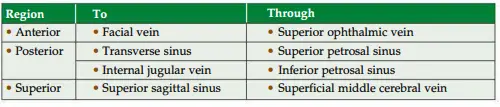
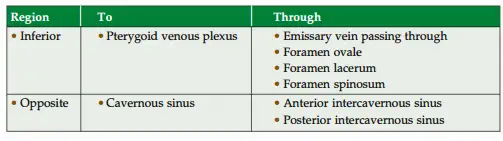
5. Cavernous Sinus Communications
6. Cavernous Sinus Applied anatomy
- Thrombosis of cavernous sinus is caused by septic infections of the dangerous area of face.
These areas are Septum of nose and nasal cavities.
Adjoining area of cheek and paranasal air sinus. - Clinical manifestations of thrombosis in cavernous sinus are
Ophthalmoplegia and diplopia, if III, IV and VI nerves are involved.
Severe pain in the area of distribution.
Oedema of eyelids, and
Papilloedema
Exophthalmos.
There will be loss of vision, if central vein and artery are involved. - Arteriovenous aneurysm is caused by rupture of internal carotid artery and results in
Loud systolic thrill.
Unilateral pulsatile exophthalmos.
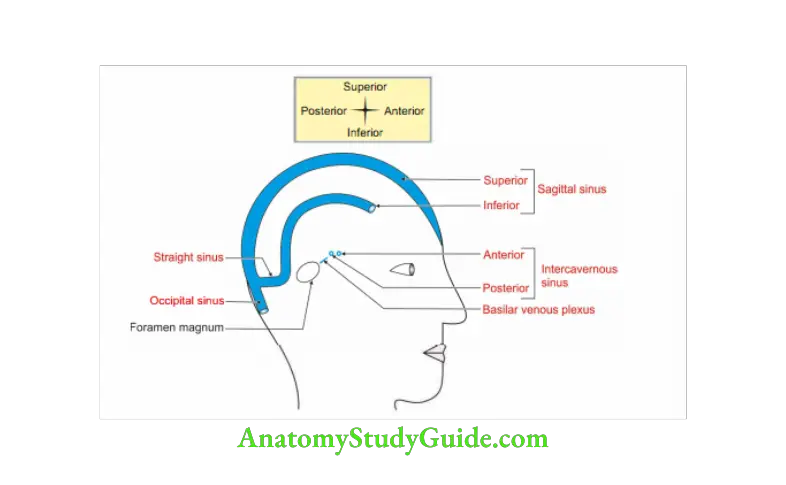
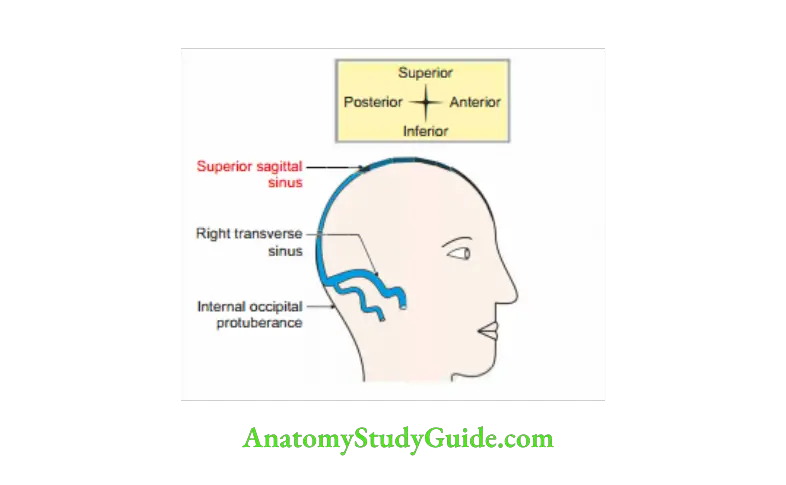
Superior Sagittal Sinus
Venous sinus situated at convex margin of falx cerebri between its two layers.
1. Extent: Crista galli (crista-crest or tuft of hair on an animal’s head, galli-cock) to internal occipital protuberance.
2. Course: Above the foramen caecum> crista galli> inner surface of frontal sagittal margins of parietal and squamous part of occipital.
3. Size: It becomes progressively larger as it passes backward to internal occipital protuberance.
4. Fate: Usually ends in right transverse sinus.
5. Shape: lar in cross-section
6. Superior Sagittal Sinus Features
- Arachnoid granulations are projected in superior sagittal sinus.
- There are numerous fibrous strands at inferior angle.
7. Superior Sagittal Sinus Tributaries
- Veins from nose.
- Superior cerebral veins which are 8 to 12 in number and collects blood from
Superolateral, and
Medial surface of cerebral hemisphere. - Diploic and emissary veins through venous lacunae.
8. Superior Sagittal Sinus Communicates with
- Veins of scalp through parietal emissary vein.
- Veins of nose passing through foramen caecum.
- Cavernous sinus through
Superior anastomotic vein (Trolard’s vein).
Superficial middle cerebral vein.
9. Superior Sagittal Sinus Applied anatomy
Thrombosis of superior sagittal sinus is caused by infection of nose, scalp and diploe.
The manifestations are
- Signs and symptoms of increased intracranial tension.
- Paraplegia (due to involvement of paracentral lobule).
- Convulsions due to compression of motor area.
Question 5: What is the clinical importance of sigmoid sinus?
Answer:
1. The infection of the scalp behind the ear can spread through the mastoid emissary vein to the sigmoid venous sinus.
It can be dangerous or fatal.
2. Infections from posterior cranial fossa can reach internal jugular vein through sigmoid sinus.
3. The sigmoid and transverse sinuses are often together termed the lateral sinus by clinicians. The sigmoid sinus is closely related to the mastoid air cells and middle ear cavity.
Hence, these sinuses liable to infective thrombosis secondary to otitis media.
Sigmoid Sinus
Sigmoid Sinus Introduction: It is a space lined by endothelium present in cranium. It is between two folds of dura mater (endosteal and meningeal layers), which are non-compressive in nature. It devoids smooth muscles and valves.
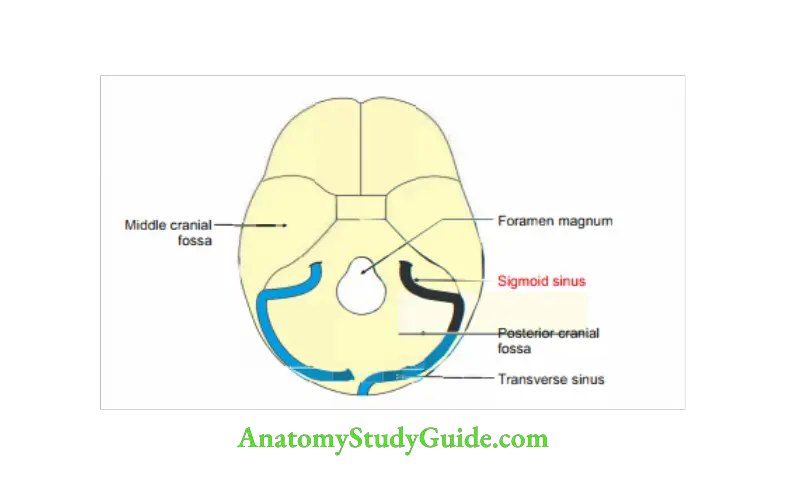
1. Site: Posterior cranial fossa on parietal, temporal and occipital bones.
2. Shape: “S” shape.
3. Termination: It continues as internal jugular vein through the jugular foramen.
4. Extent: Extends from anterior end of transverse sinus to posterior end of jugular foramen.
5. Tributaries: Connects to
- Pericranial veins through mastoid and condylar foramen.
- Cerebellar vein.
- Internal auditory vein.
6. Sigmoid Sinus Applied anatomy
- Infections from posterior cranial fossa can reach internal jugular vein through sigmoid sinus.
- It is closely related to mastoid air cells. Hence, the infection from middle ear or mastoid antrum can spread to sigmoid sinus and other venous sinuses.
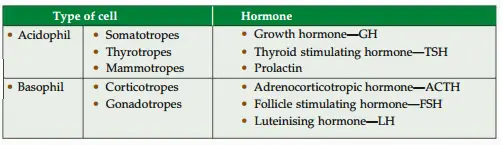
Question 6: State the types of cells in adenohypophysis and their secretions.
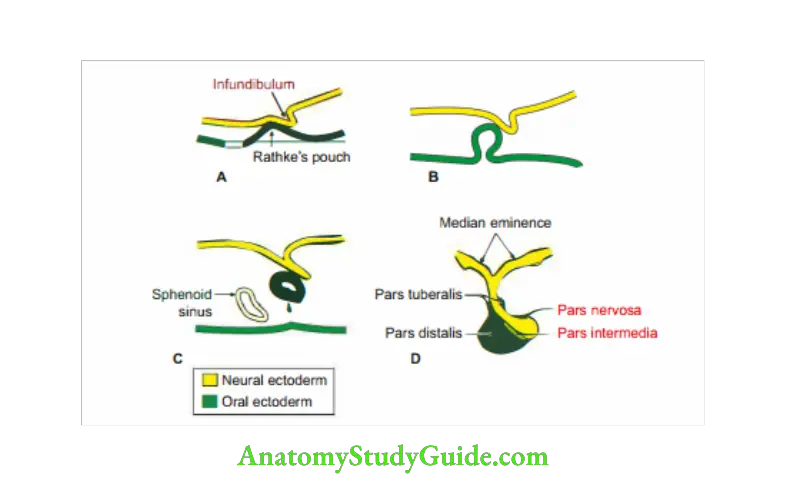
Development of hypophysis cerebri
1. Hypophysis Cerebri Development
- Chronological age: It develops in the middle of the 4th week of intrauterine life.
- Germ layer: Ectoderm.
- Site: Roof of the stomodeum.
- Source
- Rathke’s pouch: It is a blind pouch arising from surface ectoderm of the stomodeum. It grows upwards and comes in contact with the diverticulum arising from the floor of diencephalon.
- Neuroectoderm:I. … gownward giverticulum frm flor ofgiencephalon.
- Derivatives
Rathke’s pouch gives rise to
- Pars distalis (pars anterior): Anterior lobe
- Pars intermediate lobe
- Pars tuberalis
Neuroectoderm gives rise to
- Pars nervosa (posterior lobe), and
- Stalk.
Hypophysis Cerebri Anomalies
- Craniopharyngiomas: It is a tumour growing from the hypphyseal stalk or
Rathke’s pouch. The Rathke’s pouch may persist, forming a benign cystic tumour in the body of sphenoid.
It is associated with increased intracranial pressure and showing deposition of calcium in the capsule.
Compressioncauses hyppituitarism, hydrocephaly and personality changes. - Hyperplasia: More than normal growth.
- Aplasia
- Hypoplasia: Less than normal growth of the gland.
- Accessory pharyngeal hypophysis: It is present in the roof of nasopharynx.
Hypophysis Cerebri Applied anatomy
- Pituitary tumour gives rise to two main types of symptoms.
General symptoms: Due to pressure over the surrounding structures.
Specific symptoms: Pressure over optic chiasma. It causes bilateral hemianopia. - Acidophilic adenoma causes acromegaly in adult and gigantism in young individual.
- Basophilic adenoma causes Cushing’s syndrome. The damage of the posterior lobe causes diabetes insipidus.
Pressure over hypothalamus gives rise to hypothalamic symptoms.
Describe hypophysis cerebri under the following heads:
1. Gross anatomy,
2. Blood supply,
3. Histology, and
4. Applied anatomy
1. Gross anatomy
Situation: It is an endocrine gland situated in the pituitary fossa of the body of sphenoid bone.
Shape: Oval
Size: 8 mm x 12 mm
Weight: 500 mg
Relations
Superior
- Diaphragm. sellae,
- Optic chiasma,
- Tuber cinereum (grey coloured), and
- Infundibular recess of 3rd ventricle.
Inferior
- Body of sphenoid, and
- Sphenoidal air sinus
Lateral: Cavernous sinus.
2. Blood supply: It is site of portal circulation.
1. Arterial supply: Arterial supply is divided into arteries of
- Neurohypphysis, and
- Adenohypophysis.
- Neurohypophysis
- Superior hypophyseal artery
- Inferior hypophyseal artery } Internal carotid artery
Each superior hypophyseal artery supplies
- Ventral part of hypothalamus
- Upper part of infundibulum through trabecular artery
Each inferior hypphyseal artery divides into
- Medial branch and
- Lateral branch.
They form anarterial ring aroun posterior lobe. Branches of thse circles supply posterior lobe.
Adenohypophysis: It is supplied exclusively by portal system. They arise from capillary tufts formed by the superior hypphyseal arteries.
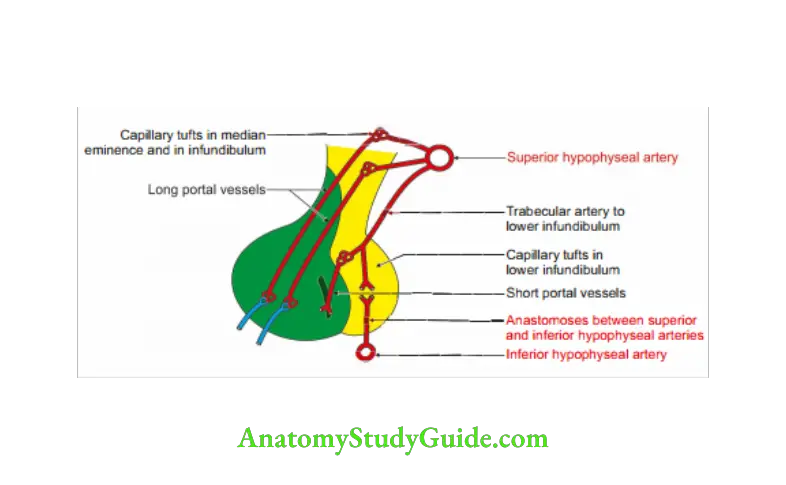
The long portal vessels drain the
- Median eminence, and
- Upper infundibulum.
The short portal vessels drain the lower infundibulum.
portal vessels carry hormone releasing factors.
2. Venous drainage: Short veins emerge on the surface of gland and drain into cavernous sinuses.
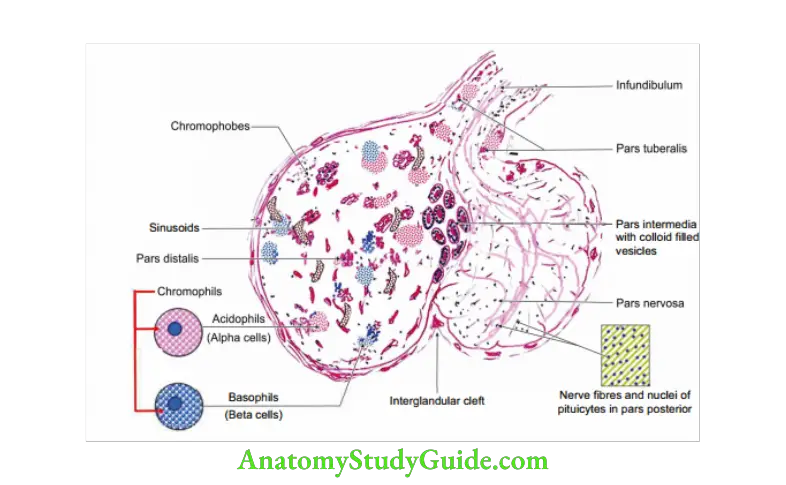
3. Histology:
1. Anterior lobe: It forms 3/4th of the gland. It consists of
Chromophil cells (50% of the cells have affinity to colours).
- Acidophils (alpha cells, about 43% of cells).
- Basophils (beta cells, about 7% of cells).
Chromophobe cells (50% of the cells do not take colour).
2. Intermediate lobe: It is made up of numerous basophil cells and chromophobe cells. They surround colloid material. I
3. Posterior lobe: It consists of
- Large number of non-myelinated nerve fibres.
- Modified neuroglial cells, called pituicytes.
4. Applied anatomy: Pituitary tumours produce signs and symptoms of both pressure effects and disturbances in endocrine function.
1. Pressure effects
- Pressure on the optic chiasma causes bitemporal hemianopia.
- Pressure on nerves in the cavernous sinus and its contained nerves produces ophthalmoplegia and may cause exophthalmos.
- Pressure on the 3rd ventricle causes increased intracranial tension.
2. Endocrine effects
- Acromegaly or gigantism in case of adenoma of acidophil cell.
- Cushing’s syndrome in case of adenoma of basophil cells.
Question 7: Lesions of optic chiasma
Answer: 1. Pressure over the central part of optic chiasma causes bitemporal hemianopia.
2.Lesion in peripheral part of optic chiasma leads to binasal hemianopia.
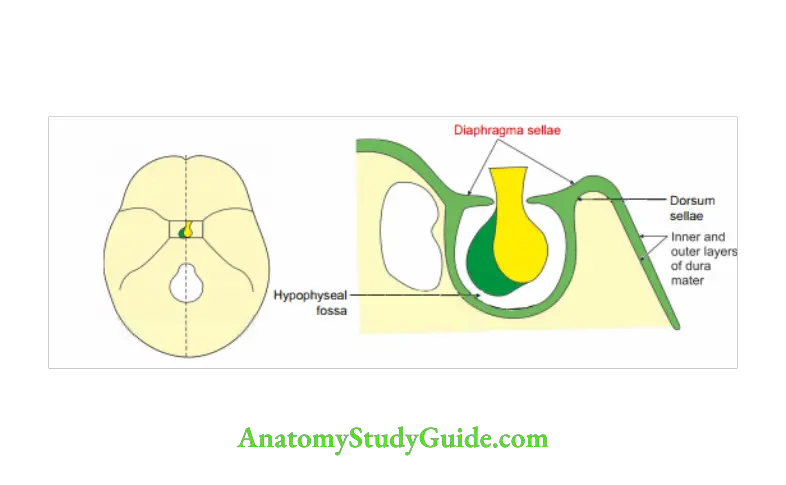
Diaphragma sellae
(Diaphragm-partition, sellae-saddle)
Diaphragma Sellae Introduction: It is the inner layer of dura mater covering the pituitary fossa .
1. Diaphragma Sellae Features
- It forms the roof of the pituitary fossa.
- It is fibrous in nature.
2. Diaphragma Sellae Attachments
- Anteriorly: Tuberculum sellae
- Posteriorly: Dorsum sellae
- On both sides, it is continuous with dura mater of middle cranial fossa.
3. Diaphragma Sellae Perforations: It is perforated
- Centrally by pituitary gland
- Anteriorly by optic nerve.
4. Diaphragma Sellae Blood supply: It has little blood supply by
- Middle meningeal artery cessory memngea. 1 artery } branch of 1st part of maxillary artery)
- Meningeal branch of ascending pharyngeal artery (branch of external carotidartery).
5. Diaphragma Sellae Nerve supply: Meningeal branch of maxillary nerve.
Faix Cerebelli
(Faix-sickle ) shaped)
Faix Cerebelli Introduction: It is a fold of dura mater projecting into posterior cerebellar notch.
1. Formation: It is formed by duplication of inner dural layer.
2. Faix Cerebelli Extent: It extends from internal occipital protuberance along the internal occipital crest to the posterior margin of the foramen magnum.
3. Faix Cerebelli Content: Occipital sinus
4. Faix Cerebelli Features: It has
- Base: It isattachedto th posterior part ofinferior surface of th tentorium cerebelliin the median plane.
- Apex has two parts which surround the foramen magnum.
- Posterior margin: It is convex and attached to internal occipital crest. It encloses the occipital venous sinus.
- Anterior margin is free.
5. Faix Cerebelli Functions
- It partly separates two cerebellar hemispheres.
- It minimizes the rotator displacement of the brain.
Note: The tentorium cerebelli is an insensitive structure.
Faix cerebri
Introduction: It is sickle J ‘haped fold of dura mater present between the right and left cerebral hemispheres.
1. Faix cerebri Features
Attachments
- Anteriorly to frontal crest of frontal and crista galli of ethmoid bone.
- Posteriorlyto internal occipital protuberanceand posteroinferiorly to tentoriumcerebelli
- Superiorly to the sagittal sulcus.
- Inferiorly it has free margin.
Surfaces: It has two surfaces and related to medial surface of cerebral hemisphere.
Faix cerebri Contents
- Superior sagittal sinus
- Inferior sagittal sinus
- Straight sinus
Tentorium cerebelli
(Tentorium-tent)
Tentorium Cerebelli Introduction: It is tent-like fold of dura mater separating occipital lobe of cerebrum
from cerebellum .
1. Tentorium Cerebelli Features
Surfaces
- Upper surface supports the occipital lobe.
- Lower surface roofs the cerebellum.
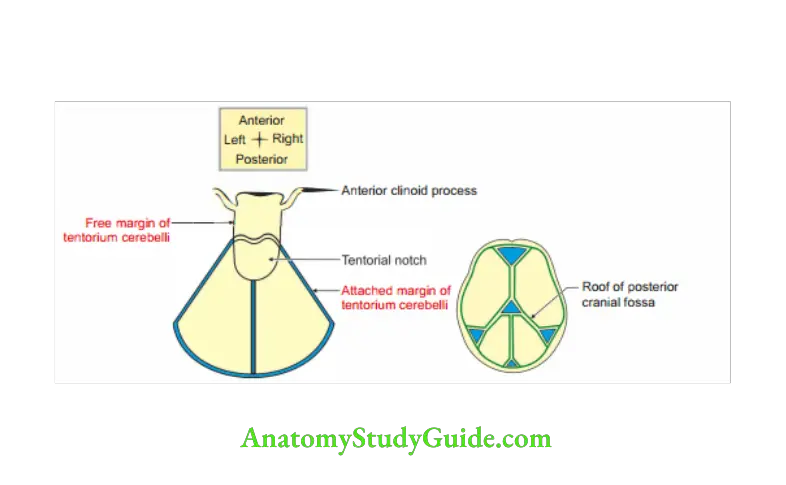
Tentorium Cerebelli Margins
1. Attached margin: It is convex. At periphery, it is attached to
- Lips of transverse sulci,
- Superior border of petrous part of temporal bone.
- Posterior clinoid process.
2. Free margin: It is U shaped and free. It is attached to anterior cranial fossa.
2. Tentorium Cerebelli Structures piercing
- Great cerebral vein pierces the dura mater and joins the inferior sagittal sinus to form the straight sinus.
- Trochlear nerve pierces before crossing the free and attached margin of tentorium cerebelli.
- Oculomotor nerve pierces after crossing the fre and attached margin of tentorium cerebelli.
3. Tentorium Cerebelli Contents
- The following venous sinuses are enclosed in the tentorium cerebelli. (There isno venous sinus in the free margin of tentorium.)
Transverse sinus,
Superior petrosal sinus, and
Straight sinus. - Other contents
Trigeminal ganglion
Sensory and motor root of trigeminal nerve with covering of pia mater andarachnoid mater that contains CSF.
4. Tentorium Cerebelli Recess: Trigeminal cave is formed by the folds of dura mater.
- Above by 2 meningeal layers of dura mater
- Below by 1 meningeal and one endosteal layer of dura mater.
5. Blood supply
Arterial: Meningeal branches of
- Ascending pharyngeal artery
- branch of external carotid artery
- Vertebral artery (branch of 1st part of subclavian artery).
Venous: Drain into meningeal vein and the dural venous sinus.
6.Tentorium Cerebelli Nerve supply: Sensory nerve supply: Recurrent meningeal branch of ophthalmicdivision of trigeminal nerve.
7. Tentorium Cerebelli Functions
- Stabilization of brain: They play important role in stabilizing the brain in caseof sudden movements of head.
- It absorbs the stress.
- It bears the weight of occipital lobe without transmitting to cerebellum.
8. Tentorium Cerebelli Applied anatomy
- Supratentorial and infratentorial compartments are communicated through the narrow space around midbrain and tentorial notch.
In case of obstruction of the communication, there is dilatation of ventricles and subarachnoid space of posterior cranial fossa. - Inflammation of the supratentorial compartment gives rise to frontal or parietal headache since it is innervated by ophthalmic division of trigeminal nerve.
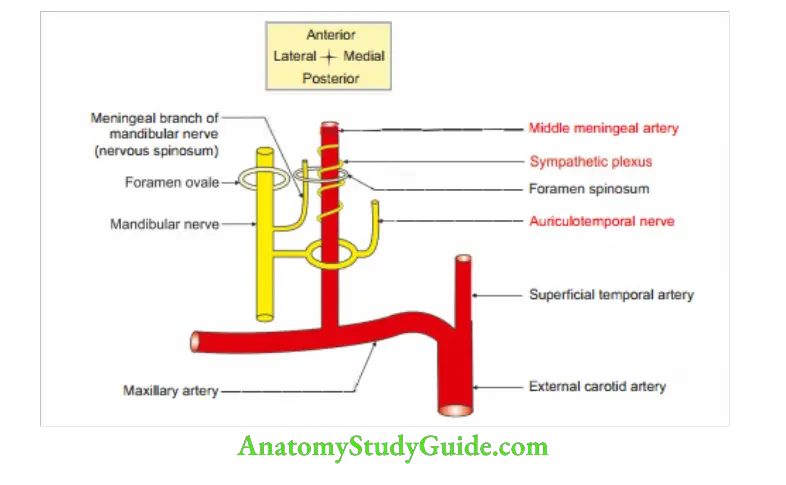
Middle meningeal artery
Middle Meningeal Artery Introduction: It is the main source of blood to the bones of vault of the skull.
1. Middle Meningeal Artery Origin: It is th 1stbranch of th 1st part ofmaxillary artery given in th infrtemporal fossa.
2. Middle Meningeal Artery Relations: It is superficial to sphenomandibular ligament and deep to lateralterygoid muscle. It is accompanied by
- Plexus of sympathetic nerves.
- Middle meningeal vein, a loyal friend.
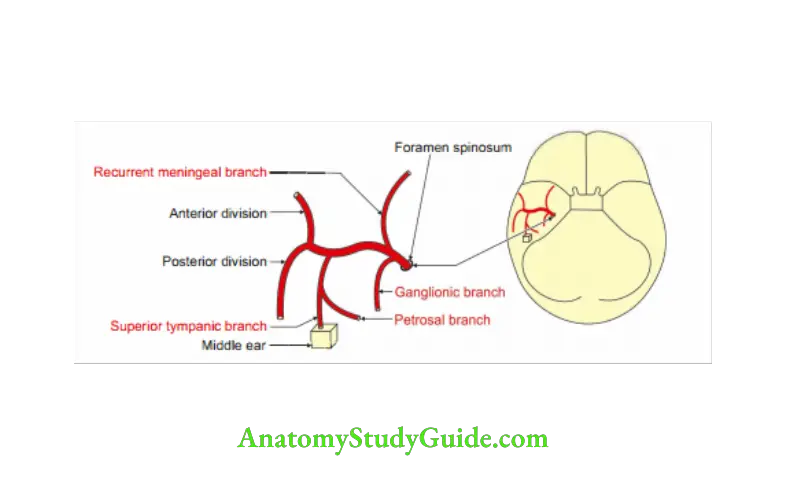
3. Middle Meningeal Artery Branches: The major branches of middle meningeal artery run between periostea and meningeal layers of dura mater.
The small branches are within periosteal layers.
- Ganglionic branches to trigeminal ganglion,
- Petrosal branch,
- Superior tympanic branch,
- Temporal branch, and
- Anastomosing branch.
Note: The major branches of middle meningeal artery run between periosteal and meningeal dura layers.
The small branches are within periosteal layers.
4. Middle Meningeal Artery Course
- Ascends between two roots of auriculotemporal nerve.
- Enters the middle cranial fossa through foramen spinosum.
- Runs upwards and forwards on greater wing of sphenoid bone and divides into anterior and posterior divisions.
- Anterior division is closely related to motor area of brain.
- Posterior division runs backwards on superior temporal sulcus of brain.
It ends at posteroinferior angle of parietal bone by dividing into frontal and parietal branches.
5. Middle Meningeal Artery Applied anatomy
- Fracture of the skull may cause injury to the middle meningeal artery producing extradural haemorrhage.
The resultant extradural haematoma compresses the motor area of the cerebral cortex and causes paralysis of the muscles of opposite side of body. The paralysis of muscles depends upon the extent of compression by haematoma.
- Talk and diesyndrome: Injury atpterionbysmall stone results in rupture of middle meningeal artery.
The patient gets transient unconsciousness.
He becomes conscious, talks for sometime and again becomes unconscious.
The duration of consciousness between two consciousness periods is called lucid interval.
Patient dies before the condition is diagnosed.
So in case of any head injury, th patient should be kept 24 hours for observation to rule out extradural haemorrhage. - The rupture of middle meningeal artery is a surgical emergency.
The symptoms of brain compression occur within 3 hours.
It should be explored immediately to arrest the bleeding and to remove the blood clot. - Rupture of posterior division of middle meningeal artery results in contralateral deafnss.
- The anterior division is approached by making a hole at pterion (4 cm above midpoint of zygomatic arch)
Note: Intracranial haemorrhagemay be arterial or venous. It is rememberedas arterialvenous-arterial
- Between bone and endosteal layer of dura mater (extradural or epidural haemorrhage-arterial)
- Between dura mater and arachnoid mater (subdural haemorrhage-venous)
- Between arachnoid mater and pia mater (subarachnoid haemorrhage-usually arterial)
- Intracranial haemorrhage never separates the ‘two layers’ of the dura mater and it never separates pia mater from the underlying cortex.
Question 8: Describe oculomotor nerve under the following heads:
1. Origin,
2. Course,
3. Distribution, and
4. Applied anatomy
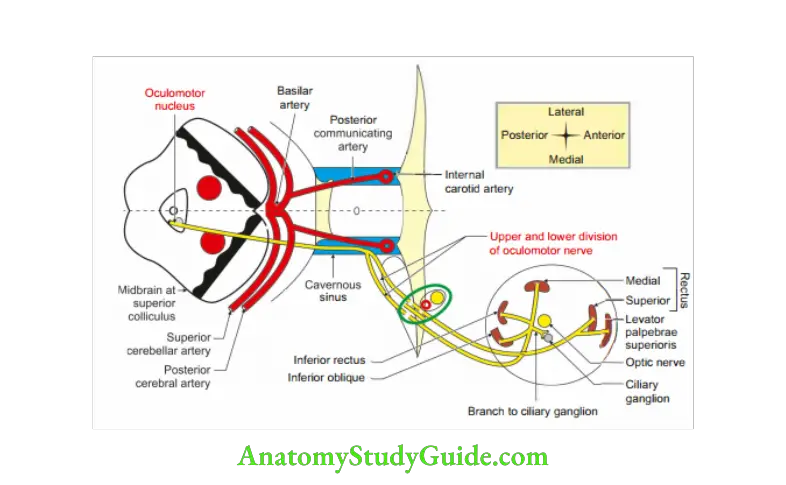
Answer: 1. Oculomotor Nerve Origin: The oculomotor nerve arises from oculomotor nucleus, present in the grey matter of midbrain at the level of superior colliculus.
2. Oculomotor Nerve Course
Nuclei:
- Median unpaired central nucleus for
Convergence, and
Accommodation. - Paired lateral motor nucleus for all extraocular muscles of eyeball except lateral rectus and superior oblique.
- Paired small nucleus (Edinger-Westphal nucleus) for parasympathetic pupillary fibres for pupil constriction and ciliary body.
Oculomotor Nerve Intraneuronal: Oculomotor nucleus — +egmentum — +ed nucleus — medial part of substantia nigra and emerges out of brainstem on medial side of crus cerebri through oculomotor sulcus.
Oculomotor Nerve Extraneuronal: It pierces the pia mater and lies in the subarachnoid space in the posterior cranial fossa.
Oculomotor Nerve Posterior cranial fossa: It passes between posterior cerebral artery and superior
cerebellar artery.
- It lies posterior to posterior cerebral artery and
- Superior and anterior to superior cerebellar artery and passes
- Lateral and parallel to posterior communicating artery.
- It pierces
- Arachnid mater and lies in the interval between free and attached margin of tentorium cerebelli.
- Dura mater lateral to posterior clinoid process.
- Cavernous sinus and traverses the roof and descends in the lateral wall of cavernous sinus.
It receives a few filaments from internal carotid artery and communicates with ophthalmic division of trigeminal nerve.
Cavernus sinus: The relations from above downwards are 3rd and 4th cranial 1 nerves, ophthalmic and maxillary division of trigeminal nerve.
The nerve divides into upper and lower divisions at anterior end of,cavernous sinus.
Superior orbital fissure: It divides in two divisions.
3. Distribution Motor
Upper-division
Levator palpebrae superioris
Superior rectus
Note: Superior rectus only has crossed innervation.
Lower-division
- Inferior rectus
- Inferior oblique
- Medial rectus
Parasympathetic branch to ciliary ganglion. It supplies sphincter pupillae and ciliaris muscle, through the branch of inferior oblique.
Oculomotor Nerve Applied anatomy
Infranuclear paralysis of oculomotor nerve results into Loss of accommodation.
Pftosis.
Pfrotrusion of eyeball-proptosis
Lateral squint.
Ebolus in cavernous sinus is one of the causes of paralysis of 3rd nerve.
Diplopia.
Dilatation of pupil.
Complete division of oculomotor nerve is manifested as
- Eyeball is depressed and abducted. “Down and out”. External strabismus: Due to unopposed action of lateral rectus.
- Ophthalmoplegia > Diplopia where false image is higher than true image.
- Ptosis: Drooping of eyelid due to involvement of levator palpebrae muscle.
- Sphincter pupillae is not functioning. It results into dilatation of pupil (mydriasis)
- Dilated and fixed pupil.
- Loss of accommodation reflex because of paralysis of three muscles.
- Medial rectus-medial convergence of eyeball is lost.
- Sphincter pupillae-pupillary constriction is lost.
- Ciliaris muscle-thickness of lens will increase.
- Apparent protrusion of eyeball due to flaccid paralysis of most of ocular muscles.
- Patient finds difficulty in getting down the staircase and reading the books.
He gets diplopia while doing these activities.
- In paralysis of oculomotor nerve, patient cannot look upwards, downwards or medially.
- 3rd nerve is usually affected due to syphilitic periarteritis of posterior cerebral and superior cerebellar arteries as the nerve passes between the arteries.
- Weber’s syndrome: Ipsilateral paralysis of oculomotor nerve with contralateral hemiplegia.
Benedikt’s syndrome (tegmental mesencephalic paralysis): It involves lesion of oculomotor nerve an red nucleus.
Threis damage of corticospinl tract. It manifs as
Ipsilateral
- Paralysis of the muscles supplied by oculomotor nerve, and
- Ataxia
Contralateral
- Hyperkinesia
- Tremor of the arm and leg.
- In meningitisNEET, one of the dreadful complication is uncal herniation that affects oculomotor nerve.
- In uncal herniation or compressio n by the aneurysm of posterior communicating artery, the peripheral fibres of oculomotor nerve are first compressed.
These are parasympathetic fibres going to pupil.
They are first u affected and results in dilatation of pupil.
As the compression progresses, the extrinsic muscles of eyeball are also affected. - Unexplained fixed pupil with headache is a dictum of rupture of aneurysm 1 of posterior communicating artery in circle of Willis. It produces compression of Z peripheral fibres of oculomotor nerve. ,
- Paralysis of oculomotor nerve in diabetic patient, there is paralysis of muscles of eyeball.
There is no affection of parasympathetic fibres which spares pupillary reaction. - Internuclear ophthalmoplegia is due to lesion in medial longitudinal bundle (fasciculus).
There is weakness of adduction on the same side and contralateral abduction nystagmus. - One and half syndrome: It is lesion in parapontine reticular formation (PPRF)on same side.
Weber’s syndrome
1. Condition which includes
- Upper motor neuron lesion of corticospinal tract in crus cerebri of the midbrain,and
- Lower motor neuron lesion of third nerve, supplying the muscles of eyeball.
2. Clinical features: It results in
- Contralateral hemiplegia, and
- Ipsilateral paralysis of muscles of eyeball supplied by oculomotor nerve.
Question 9: Describe trochlear nerve under the following heads:
1. Course and distribution
2. Applied anatomy
Answer: 1. Trochlear Nerve Course and distribution
- Peculiarity: It is only cranial nerve emerging from dorsal aspect of brainstem.
- The trochlear nerve emerges from the superior medullary velum near the frenulum veli just below the inferior colliculus.
It winds two peduncles.
Superior cerebellar peduncle, and the
Cerebral peduncle just above the pons. - It passes between two arteries
Posterior cerebral artery, and
Superior cerebellar artery. It appears ventrally lateral to the cerebral peduncle. - It enters the cavernous sinus by piercing the posterior corner of its roof.
- It runs forwards in the lateral wall of the cavernous sinus between the
Oculomotor, and
Ophthalmic nerves. In the anterior part of the sinus, it crosses over the 3rd nerve. - It enters the orbit through the lateral part of the superior orbital fissure.
- In the orbit, it passes medially above the origin of levator palpebrae superioris and ends by supplying the superior oblique muscle through its orbital surface.
2. Trochlear Nerve Applied anatomy: When the trochlear nerveis damaged, diplopia occurson looking
downwards, vision is single, as long as the eyes look above the horizontal plane.
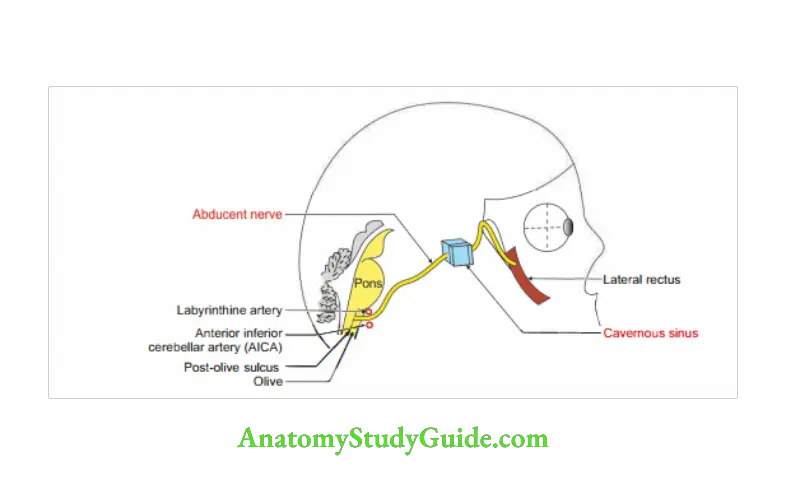
Question 10: Describe abducent nerve under the following heads:
Answer: 1. Origin and nuclei
2. Course and distribution
3. Applied anatomy
This is the 6th cranial nerve. It supplies the lateral rectus muscle of the eyeball.
1. Origin and nuclei:
- The abducent nerve has a motor nucleus.
It belongs general somatic efferent column supplying lateral rectus muscle.
It also belongs to general somatic afferent carrying proprioceptive sensations of lateral rectus to mesencephalic nucleus oftrigeminal nerve. - It arises from motor nucleus present in the dorsal part of lower part of pons. It lies deep to axons of facial nerve.
The motor nucleus of abducent nerve and axons of facial nerve collectively form a bulging in the floor of fourth ventricle.
The bulging is called facial colliculus.
2. Course and distribution
- The nerve emergs from brainstem at the pontomedullary junction.
- It passes between labyrinthine artery and anterior inferior cerebellar artery.
It runs upwards, forwards and laterally through the cisterna pontis. - It passes deep to petrosphenoidal ligament, and bends sharply forwards.
- It passes through Dollero’s canaLNEET The canal is situated at the junction of apex C1 of petrous part of temporal bone and clivus of occipital bone. I
It passes through the substance of cavernous sinus along with internal carotid artery. - The entry of abducent nerve in the cavernous sinus is at a point
Lateral to the dorsum sellae, and Superior to the apex of the petrous temporal bone. - It enters the orbit through the middle part of the tendinous ring of superior orbital fissure.
Here it lies inferolateral to the oculomotor and nasociliary nerves. - In the orbit, it ends by supplying the lateral rectus muscle. It enters the ocular surface of the muscle.
3. Trochlear Nerve Applied anatomy Paralysis of the abducent nerve results in:
- Medial (internal or convergent) squint, and
- Diplopia: Change in the visual axis of the two eyes leading to double vision due to paralysis of lateral rectus muscle.
Meckel’s cave (trigeminal cave)
Introduction: It is a diverticulum of inner layer of dura mater and arachnid mater.
1. Site: Anterior surface of apex of the petrous temporal bone in the middle cranial fossa.
2. Contents: Trigeminal ganglion.
3. Formation: It is formed by evagination of sensory and motor roots of trigeminal nerve.
Since these layers pierce subarachnoid space, they are bathed by CSP.
Meckel’s Cave Applied anatomy
- In trigeminl neuralgia, alcohol is injected into the trigeminal ganglion to alleviate the pain.
- The approach to sensory root of trigeminal nerve is avoided in the Meckal’s cave.
Failure of this approach may result into transient facial palsy.
It is explained as
- The greater petrosal nerve lies deep to trigeminal ganglion.
The stripping of th dura mater exerts pressure on facial nerve–eniculate ganglion-motor fires of facial nerve tht causes transient paralysis of muscles of face.
Trigeminal neuralgia (tic douloureux)
Trigeminal Neuralgia Introduction: It is a sensory disorder of the sensory root of trigeminal nerve, 5th cranial nerve. It occurs most often in middle-aged and elderly persons.
1. Manifestations
- It is characterized by sudden attacks of excruciating, lightening-like jabs(penetrating) of facial pain.
- A paroxysm (sudden sharp pain) can last for 15 min or more.
- The pain may be so intense that the person winces; hence the common term tic(twitch).
- In some cases, the pain may be so severe that psychological changes occur, leading to depression and even suicide attempts.
2. Nerves involved: Frequency of the nerves involved
- Maxillary-most common
- Ophthalmic-less common
- Mandibular-least common
3. The paroxysms of sudden stabbing pain are often set off by touching the face,brushing the teeth, shaving, drinking, or chewing. The pain is often initiated by touching a sensitive trigger zone.
4. Trigeminal Neuralgia Cause is not known.
5. Trigeminal Neuralgia Treatment: In maxillary nerve involvement, the temporary relief is given by blocking the infraorbital nerve.
The nerve is blocked at the infraorbital foramen by using alcohol.
This treatment usually relieves pain temporarily.
Question 11: Inferior sagittal sinus
Answer: 1. It is unpaired dural venous sinus.
2. Situation: Posterior two-thirds of the lower, concave free margin of the falx cerebri.
3. Termination: It ends in the straight sinus.
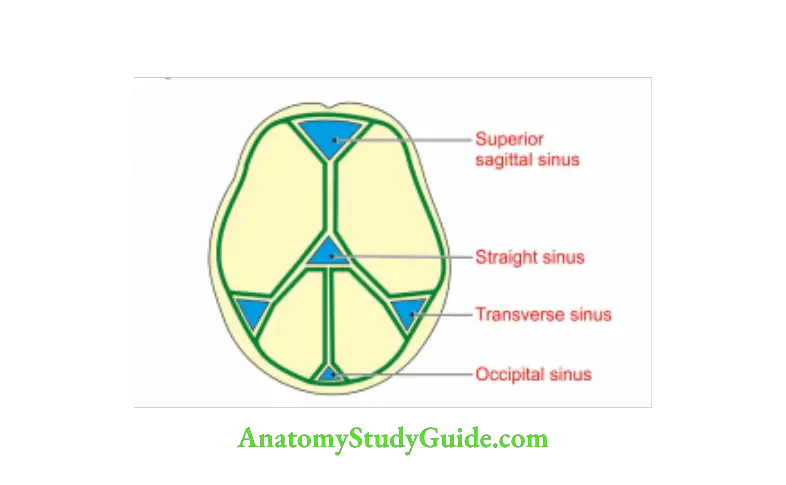
Question 12: Confluence of sinuses
Answer: 1. It is meeting point of 5 sinusesNEEr_ 1 paired and 3 unpaired sinuses.
2. Site: Internal occipital protuberance
3. Sinus opening
- Paired sinus-transverse sinus
- Unpaired sinuses:
Superior sagittal sinus
Straight sinus
Occipital sinus - Tributaries:
Cerebral vein
Cerebellar vein
Trigeminal ganglion (semilunar or gasserian ganglion)
Trigeminal Ganglion Introduction: It is sensory ganglion present in the course of trigeminal nerve.
1. Site: The trigeminal ganglion lies within a pouch of dura mater called the trigeminal cave.
It is present on trigeminal impression present on the anterior surface of petrous part of temporal bone.
2. Homologous to dorsal root ganglion of the spinal nerve.
It consists of pseudounipolar nerve cells with T-shaped arrangement of their processes.
One process arises from the cell body which then divides into a central and a peripheral process.
The ganglion is semilunar< in shape.
The three divisions of the trigeminal nerve emerge from the ganglion.
The posterior concavity of the ganglion receives the sensory root of the nerve.
3. Relations
Trigeminal Ganglion Medially
- Internal carotid artery.
- Posterior part of cavernous sinus.
Trigeminal Ganglion Laterally: Middle meningeal artery.
Trigeminal Ganglion Superiorly: Parahippocampal gyrus.
Trigeminal Ganglion Inferiorly
- Motor root of trigeminal nerve.
- Greater petrosal nerve.
- Apex of the petrous temporal bone.
- Foramen lacerum.
4. Associated roots: The central processes of the trigeminal ganglion cells enter the lateral aspect of the pons and divide into ascending and descending branches which terminate in one or another component of the sensory nucleus of V.
- The peripheral processes of the ganglion cells form three divisions of the trigeminal nerve, namely the ophthalmic, maxillar and mandibular.
5. Blood supply: The ganglion is supplied by twigs from:
- Internal carotid artery, one of two terminal branches of common carotid artery.
- Middle meningeal, branch of 1st part of maxillary artery.
- Accessory meningeal arteries, branch of 1st part of maxillary artery.
- By the meningeal branch of the ascending pharyngeal artery, medial branch of external carotid artery.
Surface anatomy: A little in front of pre-auricular point at a depth of 4.5 cm.
Trigeminal Ganglion Applied anatomy
- Trigeminal neuralgia is relieved by injecting 90% alcohol in the affected division of trigeminal ganglion.
- A herpes zoster virus infection may produce a lesion in the trigeminal ganglia. This occurs in 20% of cases. It is manifested of vesicles in one of the divisions of trigeminal nerve.
- Removal of trigeminal ganglion results in temporary loss of taste sensations of anterior two-thirds of the tongue.
Trigeminal Ganglion Treatment
Medical Surgical treatment.
- In maxillary nerve involvement
- For temporary relief: Block the infraorbital nerve at the infraorbital foramen by using alcohol. This treatment usually relieves pain temporarily.
- Avulsion or cutting of the branches of the nerve at the infraorbital foramen.
- Radiofrquency selective ablation of parts of the trigeminal ganglion by a needle electrode passing through the cheek and the foramen ovale.
- Rhizotomy: Sensory root of the trigeminal nerve may bepartially cut between the ganglion and the brainstem (rhizotomy).
- Tractotomy: Sectioning the spinal tract of fifth cranial nerve (tractotomy).
After this operation, the sensation of pain, temperature and simple (light) touch is lost over the area of skin and mucous me
Leave a Reply