Surgical Complications Of Enteric Fever
During the third week of enteric fever, Salmonella typhi, paratyphi (enteric bacilli) multiply in Peyer’s patches and can give rise to the following problems:
Table of Contents
1. Haemorrhage is seen in about 5–10% of cases due to ulceration of Peyer’s patches. It can be occult, obvious or rarely massive bleeding. It is managed conservatively in majority of cases.
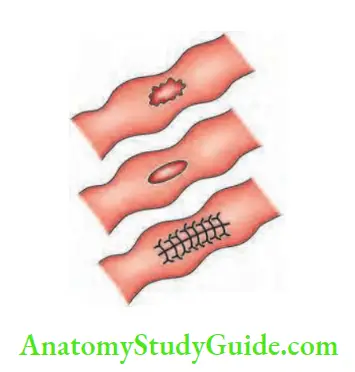
2. Perforation of terminal ileum: An oval, vertical perforation results in peritonitis. Enteric perforation need not give rise to all signs of peritonitis. Guarding and rigidity can be minimal because of poor, immunocompromised nature of the disease and due to Zenker’s degeneration of abdominal wall muscles.
It is a single perforation in about 85% of the cases. It is situated in the antimesenteric border of the terminal ileum. Typically, it occurs in the third week of enteric fever. Bradycardia, dehydration, toxicity are the other features.
- Hyperplasia of reticuloendothelial system including lymph nodes, liver and spleen is characteristic of typhoid fever.
- Diagnosis of perforation is based clinically on the acute abdominal pain, bleeding per rectum with/ without guarding and rigidity. High grade fever, toxicity and bradycardia are other features that help in the diagnosis.
- A plain X-ray abdomen may not reveal gas because of small sealed off performation.
- The most useful investigation is CT scan which can reveal not only pneumoperitoneum but also pericolic collection, which can be missed by ultrasound (see the clinical notes).
Surgical Complications Of Enteric Fever Treatment:
- Third-generation cephalosporins are used.
- Emergency laparotomy, resection of bowel and end-to-end anastomosis or closure of the perforation by using non-absorbable sutures. Abdomen is closed with a tube drain kept in the right iliac fossWound infection is common in such cases. Multiple fistulae are also common .
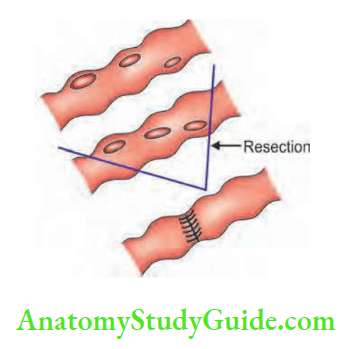
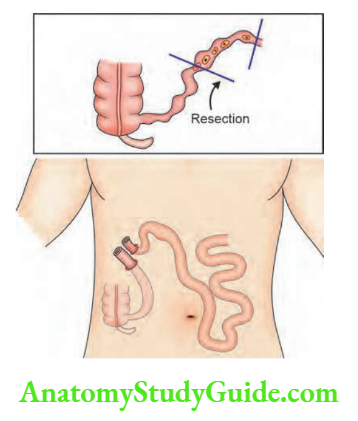

- Small bowel exteriorisation: This can be considered in cases after resection when both ends of the intestine are friable. This is a very safe option. After 1–4 weeks, relaparotomy and anastomosis of resected ends is done.
3. Paralytic ileus due to toxic dilatation of intestine results in distension of abdomen. It is managed by drip and suction.
4. Typhoid cholecystitis is not uncommon. Its starts within 2 to 4 days fever. Chances of gallbladder perforation are present.
5. Typhoid pyelonephritis, cystitis, epididymo-orchitis.
6. Typhoid osteomyelitis
7. Typhoid conjunctivitis
8. Thrombosis of the common iliac vein occurs probably due to sluggish blood flow.
9. Perforation of large intestine can occur in paratyphoid ‘B’ infections.
Most of these complications occur due to bacteraemia produced in the early septicaemic phase of enteric fever. The liver, spleen, bone and bowel are commonly affected. Metastatic abscesses are common.
Intestinal Amoebiasis
- This disease is caused by Entamoeba histolytica and transmitted mainly by contaminated drinking water.
- After the cysts are swallowed, they are broken down in the intestine by trypsin into trophozoites which produce inflammation of the colon. Trophozoites swallow red blood cells and multiply by mitosis. They enter into crypts of Lieberkuhn. They produce multiple submucous loculi which later result in multiple ulcers. These ulcers are flask-shaped (bottle neck) ulcers with healthy intervening mucosa.
- Some trophozoites are transformed into cysts and excreted outside.
- Lower sigmoid and upper rectum are involved in 75% of cases.

Surgical Complications Of Enteric Fever Clinical Features:
1. Amoebic typhlitis: Inflammation of the caecum by amoeba is described as amoebic typhlitis. It produces pain in the right iliac fossa and it can be confused for appendicitis. However, in this condition, there is also tenderness in the left iliac fossA point on the left side corresponding to McBurney point on the right side is called Sir Philip Manson-Bahr’s amoebic point of tenderness and is suggestive of involvement of rectosigmoid.
2. Amoebic dysentery: It can be acute or chroniAn acute attack is associated with gripping pain abdomen with blood and mucus in stool, an urgency to pass stools. High grade fever and tenesmus are the other features. Chronic dysentery is more common with 2–4 foul-smelling stools per day and mild to moderate colicky abdominal pain.


3. Amoeboma: Chronic, low grade, persistent inflammation of the caecum produces granulomatous hyperplasia of the caecum, with thickening of the pericaecal tissue (producing mass in the right iliac fossa). Amoeboma can also occur in rectosigmoid junction. This is, however, uncommon nowadays because of effective treatment with metronidazole.
- Clinically, this manifests as mass in the right iliac fossa causing dull aching pain, vague ill health, tender palpable caecum with guarding. It can be confused for ileocaecal tuberculosis or carcinoma caecum.
- It responds very well to metronidazole.
4. Amoebic perforation of the caecum or sigmoid can occur resulting in pericolic abscess. Peritonitis needs emergency surgery.
5. Massive bleeding per rectum is rare. It occurs due to separation of the slough.
Surgical Complications Of Enteric Fever Treatment:
- Metronidazole 400–600 mg, 3 times a day for 10 days. It acts on amoebae present in the lumen and tissue.
- Diiodohydroxyquin 650 mg, 3 times a day for 20 days is another alternative.
- Diloxanide furoate is ideal for chronic cases in the dose of 500 mg, 3 times a day for 10 days. It acts on luminal amoebae. It is the drug of choice in chronic cyst passers. Supportive treatment in the form of hospitalisation, correction of dehydration, antispasmodics and bedrest is also adviseStool culture must be done before and after treatment with antiamoebic drugs.
Leave a Reply