Ephebodontics Introduction
In 1933, Stone and Church classified children on the basis of their age as follows:
Table of Contents
- 0–1 year – Infant
- 1–2 years – Toddler
- 2–4 years – Pre-schooler
- 4–6 years – Early childhood
- 6–12 years – Childhood
- Above 12–19 years – Adolescent
Children from 10 to 19 years have been classified as adolescents by Paul Cassamassino, Jimmy Pinkham and Daniel.
The American Academy of Pediatric Dentistry (AAPD) and Society for Adolescent Medicine have emphasised that this age group needs special attention in paediatric medicine and dentistry.
Read And Learn More: Paediatric Dentistry Notes
The AAPD also instituted a Task Force to define the needs and formulate recommendations for adolescent dentistry.
The first scientific monologue on Adolescent Dentistry, Dental Clinics of North America, was published in 1969.
The term ‘pedodontics’ was coined to refer to adolescent dentistry.
The interaction between adolescents and their micro-environment (family and peers) and macroenvironment (society) is more complex when compared to that of a child who is younger and an adult who is older.
A child is shaped by receiving directions and assertions from the micro- and macro-environment.
On the other hand, adults can assert and even command the micro- and macro-environment in their circle.
But adolescents are at a crossroads. This makes their social interaction more complex and attracts special attention to their psychological and healthcare needs.
Changes Encountered In The Adolescent Period
The father of psychology, G. Stanley Hall, studied adolescence and wrote a book in 1904.
He concluded that individuals have specific psychological needs during the adolescent period.
The psychosexual theory says that by around 12 years of age, a child’s orientation is centred on the genital organs (genital stage).
The psychosocial theory points out that during this age, a child may create an identity or get confused while facing a social task (identity versus role confusion).
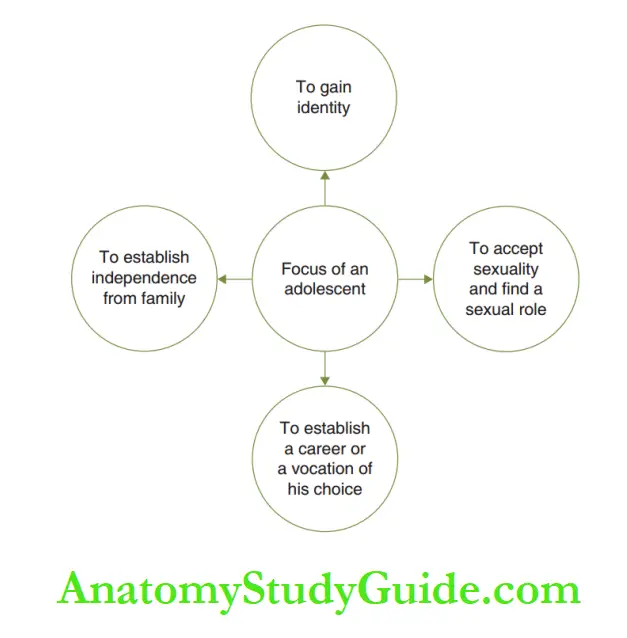
The adolescents focus their attention on four basic needs as depicted.
An individual may undergo psychological, emotional and cognitive changes during adolescence.
Adolescence is also associated with a surge in endogenous steroids in the body.
This surge in steroids is usually coherent with the onset of puberty
It is usually around 12 years in Indian girls and 14 years in Indian boys. With the onset of puberty, the secondary sexual characters develop.
These changes make the adolescent an ‘emotionally turbulent’ or a highly ‘sensitised’ individual.
The cognitive development of the adolescent is explained by Piaget’s cognitive theory. He identifies three specific features in adolescents.
They are as follows:
1. Hypothetic deductive reasoning: The individual is able to solve problems by a chosen solution, after a systematic evaluation of the available solutions.
2. Adolescent egocentrism: The individuals feel that the entire world is looking at them. They are highly conscious of themselves. This is also termed ‘imaginary audience’.
3. Personal fable: The individual feels that his/her opinions and feelings are the most special and highly unique.
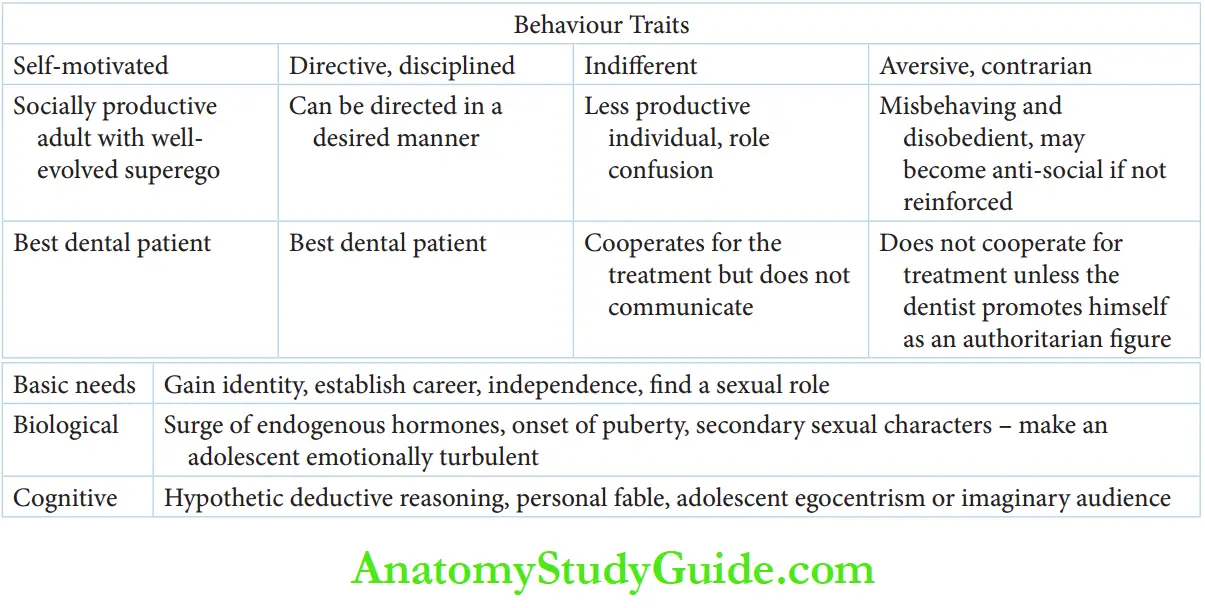
He/She has a prince/princess-like attitude. Four distinct behaviour traits are exhibited during adolescence,
Which is as follows:
1. Self-motivated: The adolescent has a very well-evolved superego. His vision and mission are clear. He adopts a strategy to achieve the same.
He lives a purposeful, focused life and most likely transforms into a socially, highly productive adult.
2. Directive, disciplined: The adolescent is not self-motivated but may be directed to act/behave in a desired manner.
His value code is framed on the social quality of his ‘director’ (the individual who guides the adolescent).
3. Indifferent: The adolescent is in a phase of ‘role Confusion’.
He exhibits neither focus nor a specific purpose in life. The productivity is very low and the individual is absolutely indifferent about enhancing the same.
He needs serious counselling and has to adopt a mentor with a sound authoritarian figure for a transition from this behaviour.
4. Aversive, contrarian, experimentalist: The adolescent is misbehaving and disobedient.
He has no code of values or ethics. He acts like a contrarian by doing things when prohibited and does not comply with instructions.
He experiments with ‘forbidden acts’ to check out the reasons for forbidding the act.
This may include smoking, alcohol consumption, taking drugs and sexual indulgence.
His behaviour needs reprimanding and negative reinforcement to prevent him from becoming an anti-social element.
Self-motivated and directive adolescents (categories 1 and 2) make the best dental patients.
The indifferent adolescent (category 3) cooperates with treatment but does not socialise or communicate during dental appointments.
Aversive adolescents (category 4) do not cooperate with dental treatment unless the dentist promotes himself as a strong authoritarian.
Factors Affecting The Dental Health Of Adolescents
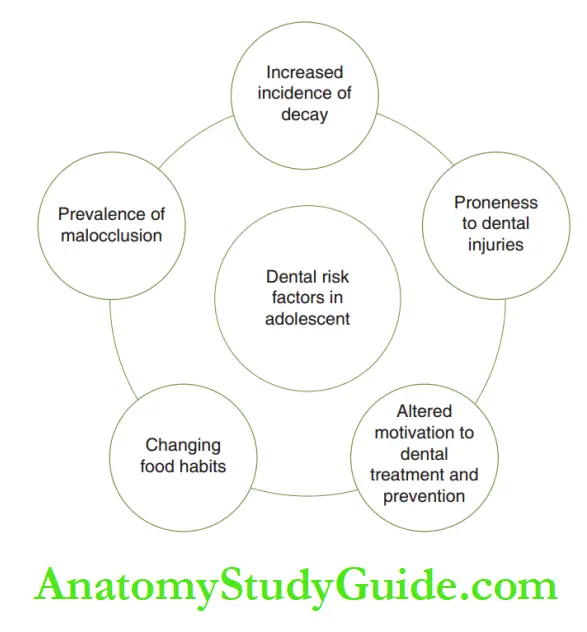
The risk factors that can affect the dental health of adolescents are increased incidence of dental decay, changing food habits, altered motivation of adolescents towards dental prevention and treatment, proneness to traumatic injuries and the prevalence of malocclusion.
Food Habits And Decay Prevalence:
The phase of adolescence shows increasing decay incidence and prevalence pandemically.
The main reason could be the change in food habits during adolescence.
Poor motivation to maintain oral hygiene and incidence of malocclusion making maintenance of oral hygiene more challenging are other reasons.
The variety of activities during adolescence including academics, sports, fine arts and outdoor entertainment raises the individual’s calorific requirement substantially.
On the other hand, skipping or missing meals is also common during adolescence.
This promotes snacking or an increased inclination towards consuming mid-meal snacks. Adolescents also restrict eating food to avoid weight gain.
This can lead to many conditions, collectively called ‘eating disorders’.
Two of them have been commonly identified, namely anorexia nervosa and bulimia.
Anorexia nervosa is characterised by immoderate food restriction due to fear of gaining weight and is associated with distorted body self-perception.
This condition is more common in females. The adolescent shows excessive weight loss.
Food restriction may also cause metabolic and hormonal disorders in the adolescent.
Bulimia nervosa was first described by the British psychiatrist Gerald Russell in 1979.
It is characterised by binge eating or consuming a large amount of food in a short duration.
The individual may then attempt to get rid of the food taken by vomiting, by taking laxatives or diuretics, or by doing extensive exercise.
This condition is also more common in women. Bulimia is also commonly accompanied by fasting over an extended period of time.
The majority of those with bulimia nervosa are of normal weight.
Adolescents give prime importance to their peer group who also influence their food habits.
This may lead to avoiding a particular conventional and nutritious food item and choosing to consume a favourite snack (refried junk food).
The food habits of adolescents are also influenced by media commercials. This is referred to as ‘fodder of media’. An adolescent requires thorough diet counselling.
The session should include awareness of their increased calorific demand and the nutritive qualities of various foodstuffs.
The risks associated with frequent intake of refined carbohydrate snacks, such as increased dental decay and obesity, should also be emphasised.
Diet counselling should also motivate the adolescent to follow a strategically balanced diet.
Traumatic Injuries:
The adolescents are involved in athletic sports activities and outdoor entertainment. This makes them prone to oral/dental injuries.
These injuries may be incurred by a fall or may happen during sports.
The points have to be emphasised to prevent sports injuries. The classification and treatment of traumatic injuries
Malocclusion:
Class I and class II malocclusion manifest during late mixed dentition, which is coherent with the adolescent phase.
Developing malocclusion predisposes teeth to two problems:
1. Teeth meal arrangement such as crowding makes oral hygiene difficult and predisposes to gingivitis
2. Teeth meal arrangement such as increased overjet, increased overbite and lip incompetence predisposes traumatic injuries to teeth
There is a psychological dimension to malocclusion in the adolescent.
The individual is highly sensitive to peer acceptance. The ‘self-image’ is not satisfying, this dissatisfaction takes centre stage during every act of this phase.
He/she spends longer time in front of the mirror, brooding over the ‘wrong element’ on his/her face.
When the peers identify the ‘wrong element’ (commonly protruded or large teeth), the adolescent focuses on getting it corrected at once.
Adolescence is also the right age to plan and commence orthodontic therapy if indicated.
Motivation And Awareness:
The adolescent requires more time and words to get motivated besides appropriate treatment. It is essential that the parents and the health care providers understand this.
The adolescents are primarily ‘attention seekers’. It should be made sure that they feel secure in the social environment.
Adolescence is the phase that decides the social outcome of the individual.
When the adolescents are made to feel that ‘they are being attended to/their presence is felt/they are important’, they will comply with the instructions given. Only then will the motivation towards oral hygiene and good dental upkeep bear fruit.
1. The adolescent should be made aware that the emotional turbulence he/she is undergoing is absolutely normal in this phase.
He/she should be instructed to talk to the parent of his/her sex with regard to the
feelings he/she has towards the opposite sex.
The parent should also be counselled about how to react and clear the doubts of their adolescent children.
2. The adolescent should be made aware of the increased risk of dental decay and gum disease.
Motivation towards good oral health can be achieved with clinical photographs of the teeth before and after oral prophylaxis.
Clinical photographs may be made at each review and compared with the earlier one.
3. The child should be made aware of more calories required to perform various activities and that snacks will not provide calories.
A clear explanation of a balanced diet and food guide pyramid is essential.
The adolescent has to understand from the counselling that missing meals may not pave the way to losing weight.
4. The adolescent should be made aware of the use of mouthguards during sports, and wearing them must be made compulsory during playing.
On the whole, the adolescent should be made to understand that he is going through a crucial phase of his life which would determine his social usefulness, and this phase is a determinant of his ultimate general and dental health.
Ephebodontics Summary
1. The adolescent phase is above 12–19 years according to Stone and Church.
2. Paul Cassamassino, Jimmy Pinkham and Daniel mentioned that the adolescent phase extends from 10 to 19 years.
3. Adolescent dentistry is termed ‘pedodontics’.
4. Children receive instructions from the micro- and macro-environment while adults command their micro- and macro-environment. Adolescents are at a crossroads, thus making their social interaction complex.
5. Changes during adolescence are as follows:
6. Factors affecting dental health during adolescence are increased decay prevalence, altered food habits, proneness to dental injuries and prevalence of malocclusion.
7. Adolescents require proper motivation and awareness of good dental health.
Leave a Reply