Extraocular Muscles under the following heads
Table of Contents
Extraocular Muscles Attchments (origin and insertion),
Extraocular Muscles Action,
Extraocular Muscles Nerve supply, and
Extraocular Muscles Applied anatomy
The extraocular muscles are voluntary and involuntary.
Voluntary muscles are
- Four recti,
- Two obliqui, and
- Levator palpebrae superioris.
Four recti:
- Superior rectus,
- Inferior rectus,
- Medial rectus, and
- Lateral rectus.
Obliqui
- Superior oblique
- Inferior oblique
Levator Palpebrae Superioris
Involuntary: Orbitalis
1. Extraocular Muscles Attachments
- Origin of recti:The recti muscles arise from the respective positions of a common I tendinous ring.
The ring is attached to the orbital surface of the apex of the orbit.
The lateral rectus has an additional small tendinous head, which arises from the orbital surface of greater wing of sphenoid bone. - B. Insertion of recti:
The recti are inserted into the sclera in front of the equator.
They are inserted few mmposteriorto thesclerocomeal junction.
The approximate distances of the insertion are I. 5, 6, 7, 8 mm MILSI
- Medial rectus: 5 mm behind the sclerocomeal junction.
- Inferior rectus: 2 mm behind the sclerocomeal junction.
- Lateral rectus: Z mm behind the sclerocomeal junction.
- Superior rectus: . mm behind the sclerocomeal junction.

Note: Visualise a clock. The 12 O’clock position represents superior rectus, 3 O’ clock medial rectus, the 6 O’ clock inferior rectus and 9 O’ clock positions represent lateral rectus.
Now focus at 6 O’clock position, the digit 6 of 6 O’ clock represents th insertion of inferior rectus behind sclerocorneal junction.
The digit prior to 6 is 5 and represents the insertion of medial rectus.
The digits after 6 are 7 and 8 which represent the insertion of lateral rectus and superior rectus.
1. Two obliqui:
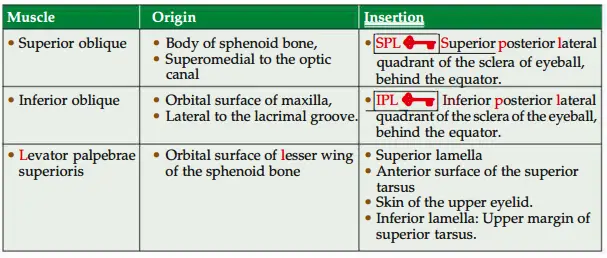
All extraocular muscles arise from apex of orbit except inferior oblique which arises from floor of orbit.
Involuntar muscles
- Superior tarsal muscle is the deep part of levator palpebrae superioris. It is inserted on the upper margin of superior tarsus.
- Inferior tarsal muscle connects the inferior tarsus of the lower eyelid to the fascia! sheath of the inferior rectus and inferior oblique. It helps in depression of lower lid.
- Orbitalis muscle bridges the inferior orbital fissure.
2. Involuntar muscles Action
- Action of individual muscles.
- Superior rectus: Elevation, adduction, intorsion.
- Inferior rectus: Depression, adduction, extorsion.
- Inferior oblique: Elevation, abduction, extorsion.
- Superior oblique: Depression, abduction, intorsion.
- Medial rectus: Adduction.
- Lateral rectus: Abduction.
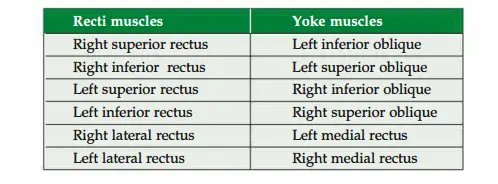



Muscles bringing particular action
- Adduction: Medial rectus, superior rectus and inferior rectus.
- Abduction: Lateral rectus, inferior oblique and superior oblique.
- Elevation: Superior rectus and inferior oblique.
- Depression: Inferior rectus and superior oblique.
- Intorsion: Superior rectus and superior oblique.
- Extorsion: Inferior rectus and inferior oblique.
3. Extraocular Muscles Nerve supply
- All the extaculaI socular muscle superior oblique,of supplied the eyeball by are trochlear supplied nerve by oculomotor(4th cranialnerve exceptnerve) and ateral rectus supplied by abducent nerve (6th cranial nerve) (superior,inferior and medial recti, inferior oblique and levator palpebrae superioris are supplied by oculomotor nerve).
S04, LR6 and R3-superior oblique by 4th (trochlear nerve), lateral rectus by 6th (abducent) and rest all muscles by 3rd
cranial nerve (oculomotor). - Tarsal muscles are supplied by carotid nerve. The fibres of the nerve are postganglionic sympathetic fibres arising frm superior cervical sympathtic ganglion.
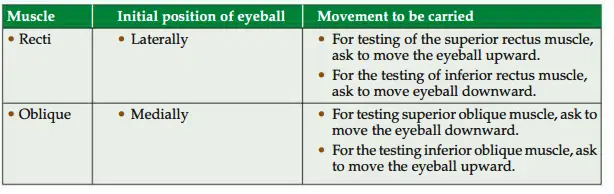
Extraocular Muscles Applied anatomy
The muscles of eyeball are tested in following ways .
Oculomotor Nerve Lesion Produces
Lateral strabismus,
In complete ophthalmoplegia
- There is paralysis of the muscles of the eyeball.
- Ptosis of the eyelid.
- Pupil is dilated (mydriasis).
- Loss of accommodation reflex.
Trochlear nerve lesion produces diplopia (double vision) when looking downwards.
Individuals with diplopia usually experience difficulty and
apprehension on descending staircase.
Abducent nerve lesion produces medial strabismus {squint (to have eyes that look in different direction)}.
In this condition, the two eyes appear to look in different directions. Diplopia is minimal when looking to the opposite side of the lesion.
- Nystagmus is characterized by involuntary, rhythmical oscillatory movements of the eyes. This is due to incoordination of the ocular muscles. It may be either vestibular or cerebellar in origin.
Leave a Reply