Types Of Tuberculosis:
The lung is the main organ affected in tuberculosis; amongst extra-pulmonary sites, lymph node involvement is most common. Depending upon the type of tissue response and age.
The infection with tubercle bacilli is of 2 main types:
Read And Learn More Infammation And Repair Pathology
- Primary Tuberculosis and
- Secondary Tuberculosis
Their salient differences are given Below
1. Primary Tuberculosis: Infection of an individual who has not been previously infected or immunised is called primary tuberculosis or Ghon’s complex or childhood tuberculosis.
- Primary complex or Ghon’s complex is the lesion produced in the tissue of the portal of entry with foci in the draining lymphatic vessels and lymph nodes. Most commonly involved tissues for primary complex are lungs and hilar lymph nodes.
- Other tissues which may show primary complexity are tonsils and cervical lymph nodes, and in the case of ingested bacilli the lesions may be found in small intestine and mesenteric lymph nodes.
- The incidence of disseminated form of progressive primary tuberculosis is particularly high in immunocompromised host for example, In patients of AIDS.
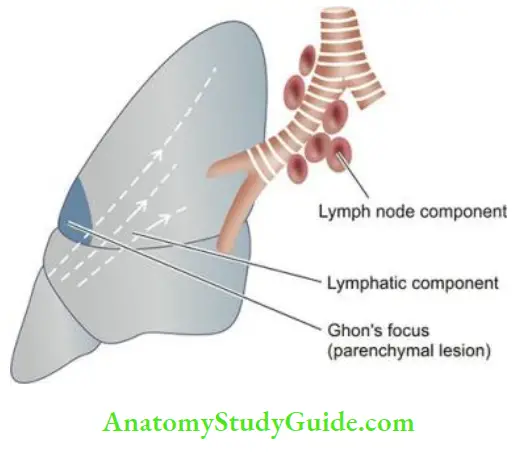
Primary complex or Ghon’s complex in lungs consists of 3 components:
- Pulmonary component: Lesion in the lung is the primary focus or Ghon’s focus. It is 1-2 cm solitary area of tuberculous pneumonia located peripherally under a patch of pleurisy, more often as subpleural focus in the interlobar fissure in the region of upper part of lower lobe and lower part of upper lobe.
- Lymphatic vessel component: Lymphatics draining the lung lesion contain macrophages containing bacilli and may develop beaded, miliary tubercles along the path of hilar lymph nodes.
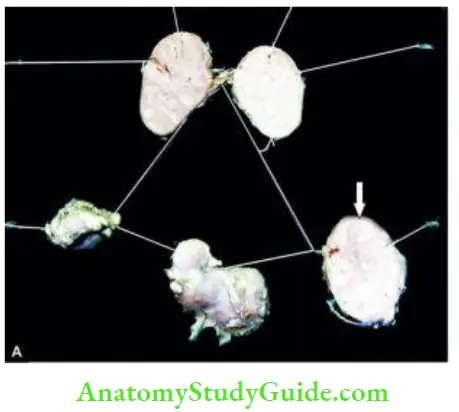
- Lymph node component: This consists of enlarged hilar and tracheo-bronchial lymph nodes in the area drained. The affected lymph nodes are matted and show caseous necrosis. Nodal lesions are a potential source of re-infection later.
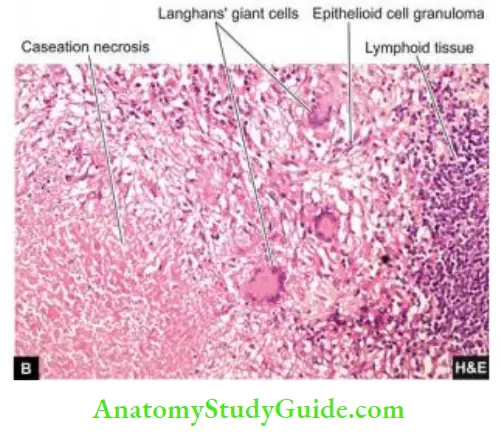
Microscopically, the lesions of primary tuberculosis have the following features
- Tuberculous granulomas with peripheral fibrosis.
- Extensive caseation necrosis in the centres of granulomas.
- Older lesions have fibrosis and may have calcification.
In the case of primary tuberculosis of the alimentary tract due to ingestion of tubercle bacilli, a small primary focus is seen in the intestine with enlarged mesenteric lymph nodes producing tabes mesenterica (page 594). The enlarged and caseous mesenteric lymph nodes may rupture into the peritoneal cavity and cause tuberculous peritonitis.
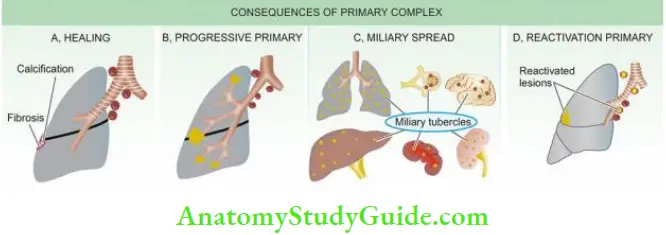
Fate Of Primary Tuberculosis:
- The primary complex may have one of the following consequences:
-
- The lesions of primary tuberculosis of the lung commonly do not progress but instead heal by fibrosis, and in time undergo calcification and even ossification.
- Less commonly, the primary focus in the lung continues to grow and the caseous material is disseminated through bronchi to the other parts of the same lung or the opposite lung. This is called progressive primary tuberculosis.
- Another uncommon outcome is entry of bacilli into the circulation through erosion in a blood
vessel and spread by haematogenous route to other tissues and organs. This is called primary miliary tuberculosis and the lesions may be disseminated to organs such as the liver, spleen, kidney, brain and bone marrow etc. - In conditions with lowered resistance and increased hypersensitivity of the host, the healed lesions of primary tuberculosis after having remained dormant for a long time, may get reactivated.
- The bacilli lying dormant in acellular caseous material or healed lesion get activated and cause progressive secondary tuberculosis. It affects children more commonly but immunocompromised adults may also develop this kind of progression.
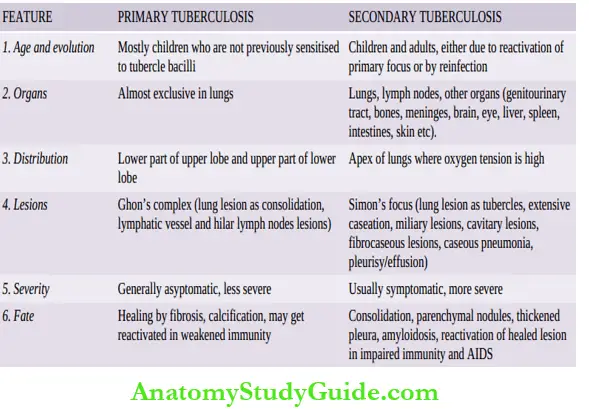
Differences between primary and secondary tuberculosis.
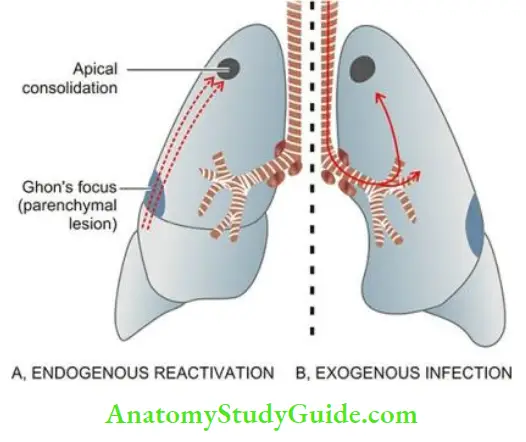
2. Secondary Tuberculosis:
Infection of an individual who has been previously infected or sensitised is called secondary, or
The routes of infection in secondary tuberculosis may be
- Endogenous source such as reactivation of dormant primary complex, or
- Exogenous source such as fresh doses of reinfection by the tubercle bacilli.
Secondary tuberculosis occurs most commonly in lungs. Other sites and tissues which can be involved are lymph nodes, tonsils, pharynx, larynx, small intestine and skin. Secondary tuberculosis of other organs and tissues is described in relevant chapters later while that of lungs is discussed here.
Secondary Pulmonary Tuberculosis:
The lesions in secondary pulmonary tuberculosis usually begin as 1-2 cm apical area of consolidation of the lung which subsequently develops central caseation necrosis and later may develop peripheral fibrosis.
It may occur by lymphohaematogenous spread of infection from reactivation of the primary complex to the apex of the affected lung where the oxygen tension is high and favourable for growth of aerobic tubercle bacilli, or the infection may be the result of direct reinfection. Microscopically, the appearance is typical of tuberculous granulomas with caseation necrosis.
Patients with HIV infection previously exposed to mycobacterial infection have particularly high incidence of reactivation of primary tuberculosis. The pattern of lesions in such cases is similar to that of primary tuberculosis i.e. with involvement of hilar lymph nodes rather than cavitary and apical lesions in the lung. In addition, infection with M. avium-intracellulare occurs
more frequently in cases of AIDS.
Leave a Reply