Gastroenterology
Symptomatology And Evaluation Of Gastrointestinal Disease
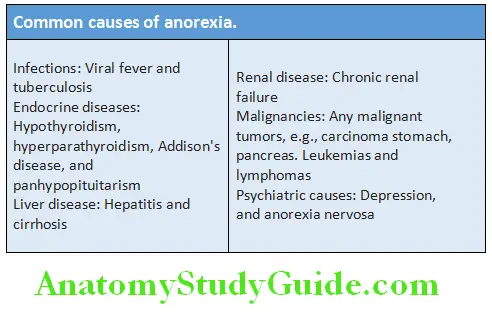
Anorexia:
Table of Contents
Question 1. List common causes of loss of appetite (anorexia).
(or)
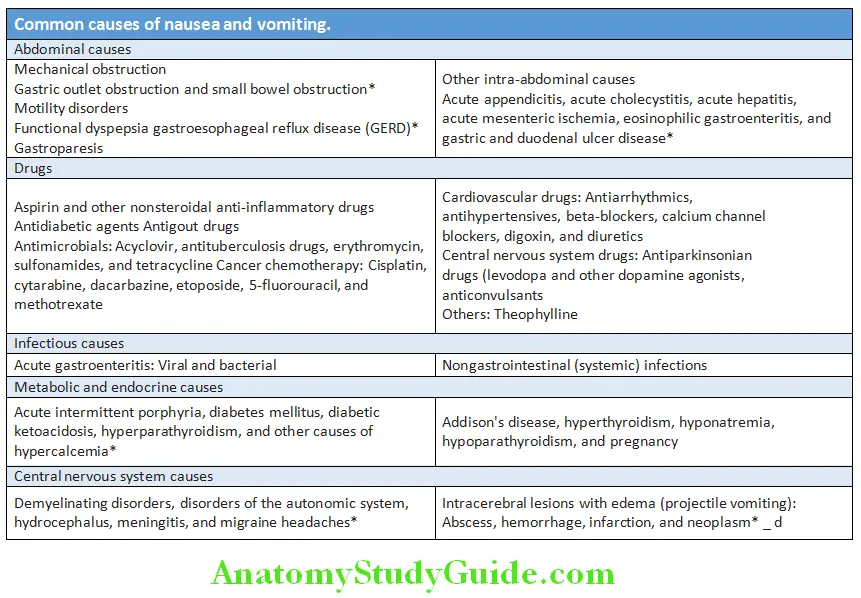
List common causes of persistent vomiting.
Answer:
Persistent Vomiting:
- Vomiting is the forceful oral expulsion of gastric contents. It is a complex reflex and involves both autonomic and somatic neural pathways.
- Nausea is a feeling of wanting to vomit and often precedes actual vomiting.
- Retching is a strong involuntary unproductive effort to vomit. It is associated with contraction of abdominal muscles but without expulsion of stomach contents through the mouth.
Read And Learn More: General Medicine Question And Answers
Mechanism of vomiting: Synchronous contraction of the diaphragm, intercostal muscles, and abdominal muscles raises intra-abdominal pressure. This is combined with relaxation of the lower esophageal sphincter and causes forcible ejection of contents of the stomach.
Rumination Syndrome/Merycism:
Features of rumination syndrome:
- Rumination is a functional disorder resembles vomiting but does not involve an integrated somatovisceral response coordinated by the emetic center
- It consists of the repetitive effortless regurgitation of small amounts of recently ingested food into the mouth followed by rechewing and re swallowing or expulsion
Complications of Chronic Vomiting:
Emetic injuries to the esophagus and stomach:
- Lesions may range from mild erythema to erosions and ulcerations
- Abrupt retching or vomiting episodes may produce longitudinal mucosal and even transmural lacerations at the level of the gastroesophageal junction. When the lacerations are associated with acute bleeding and hematemesis, the clinical condition is described as the Mallory-Weiss syndrome.
- Boerhaave’s syndrome refers to spontaneous rupture of the esophageal wall, with free perforation and secondary mediastinitis.
- Dental caries and erosions may result from chronic vomiting.
Spasm of the glottis and aspiration pneumonia:
In patients with diminished consciousness, or in an older person or patient with a depressed cough reflex, may be associated with aspiration of gastric contents into the bronchi, resulting in acute asphyxia and a subsequent risk of aspiration pneumonia.
Fluid, electrolyte, and metabolic alterations:
Hypochloremic alkalosis is usually the first metabolic abnormality to develop and is attributable to loss of fluid and hydrogen and chloride ions. Hypokalemia, hypernatremia, and dehydration can occur.
Nutritional Deficiencies:
Nutritional deficiencies may result from reduced caloric intake or loss of nutrients in the vomitus.
Question 2. Discuss treatment of persistent vomiting.
Answer:
Persistent vomiting Treatment:
1. Supportive measure: Correction of fluid and electrolyte balance
2. Medication:
- Phenothiazines and related drugs: Prochlorperazine 5–10 mg thrice daily
- Dopamine antagonists: Metoclopramide 10 mg 30 minutes before meals and at bedtime. Side effects include drowsiness and extrapyramidal effects. Domperidone (10 mg thrice daily) has no central nervous system (CNS) side effects
- Antihistaminic agents, e.g., diphenhydramine
- Serotonin 5-HT3 receptor antagonists: Useful in chemotherapy-associated emesis.
- Examples ondansetron and granisetron
- Neurokinin-1(NK-1) receptor antagonists, e.g., aprepitant (oral) and fosaprepitant (parenteral) indicated only in chemotherapy-induced nausea and vomiting
- Motilin receptor agonists: Erythromycin intravenously in boluses of 200–400 mg every 4–5 hours
- Muscarinic receptor agonist: Bethanechol
- Synthetic cannabinoids: Nabilone and dronabinol
- Glucocorticoids: Especially in raised intracranial tension (ICT), and chemotherapy-induced emesis
- Gastric electrical stimulation in refractory cases
Hiccough
Question 3. List the common causes of hiccoughs.
Answer:
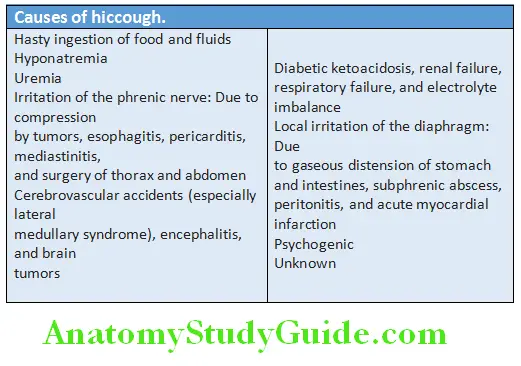
The symptom of hiccups (hiccoughs, singultus) is an involuntary, intermittent, and spasmodic contraction of the diaphragm and intercostal muscles and glottic closure.
Its causes are listed in Table:
Hiccups Symptomatic treatment:
- Advised to drink cold water, swallowing a teaspoon of dry sugar
- Apply pressure over the eyeballs
- Perform Valsalva maneuver
- Rebreathing into a paper bag
- Drugs
- Local infiltration of phrenic nerve with procaine
- Acupuncture
Drugs used for the treatment of hiccough:
- Chlorpromazine 25–50 mg orally or intramuscularly
- Domperidone 10 mg thrice daily
- Metoclopramide 10 mg thrice daily
- Xylocaine viscus 15 mL thrice a day
- Baclofen 5–10 mg thrice a day
- Nifedipine, haloperidol, phenytoin, olanzapine, nefopam, and gabapentin can be used
Constipation:
Question 4. Define constipation (Rome IV criteria). List the common causes.
Answer:
Constipation Definition: Constipation is defined as persistent, difficult, infrequent passage of hard stools, or seemingly incomplete defecation/evacuation. Many patients may also complain of excessive straining or lower abdominal fullness/discomfort.
Criteria for Functional Constipation:
Constipation Risk factors: Advanced age, female gender, low level of physical activity, low socioeconomic status, nonwhite ethnicity, and use of certain medications.
Rome IV criteria for functional constipation:
1. Two or more of the following six must be present*
- Straining during at least 25% of defecations
- Lumpy or hard stools in at least 25% of defecations
- Sensation of incomplete evacuation for at least 25% of defecations
- Sensation of anorectal obstruction/blockage for at least 25% of defecations
- Manual maneuvers to facilitate at least 25% of defecations (e.g., digital evacuation, support of the pelvic floor)
- Fewer than three defecations/week
2. Loose stools are rarely present without the use of laxatives
3. There are insufficient criteria for irritable bowel syndrome (IBS)
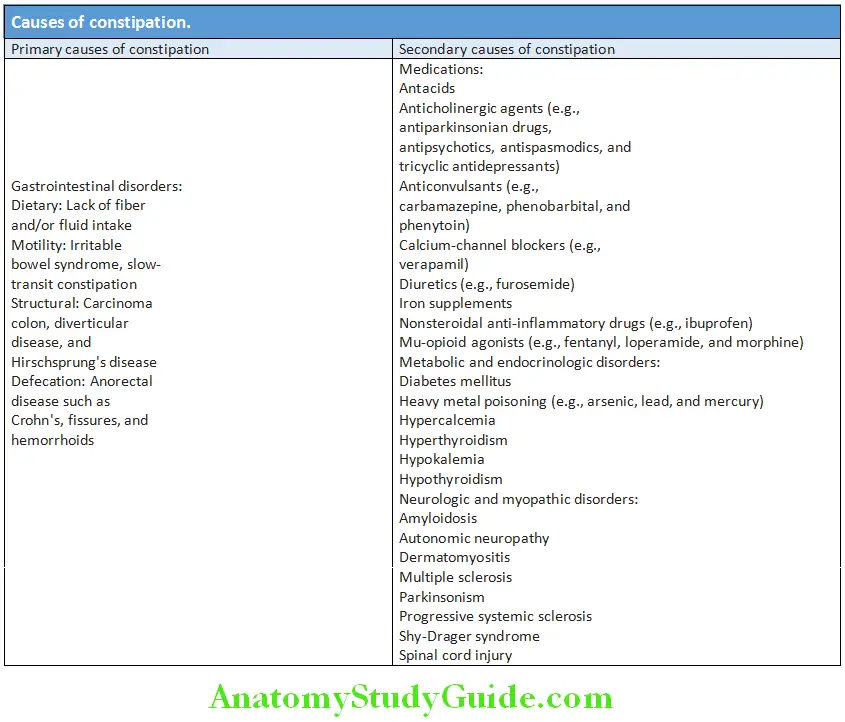
Causes of Constipation:
Constipation Investigations:
It is neither possible nor appropriate to investigate all patients with constipation.
Constipation Initial visit:
- Routine biochemistry: Serum calcium, serum glucose, and thyroid function tests
- Complete blood count
- Examination of stool including occult blood
- Digital rectal examination
- Proctoscopy and sigmoidoscopy or colonoscopy: To detect anorectal disease or exclude carcinoma colon (in patients older than 50 years or those with alarm situations such as blood in stool or anemia or weight loss or new onset of symptoms).
If these investigations are normal, a 1 month trial of dietary fiber and/or laxatives is advised.
Constipation Next visit: If symptoms persist, barium studies or CT colonography is indicated to look for structural disease. Colonic transit studies, anorectal manometry, and defecography are performed in only in resistant cases without a structural disease.
Question 5. Discuss management of constipation.
Answer:
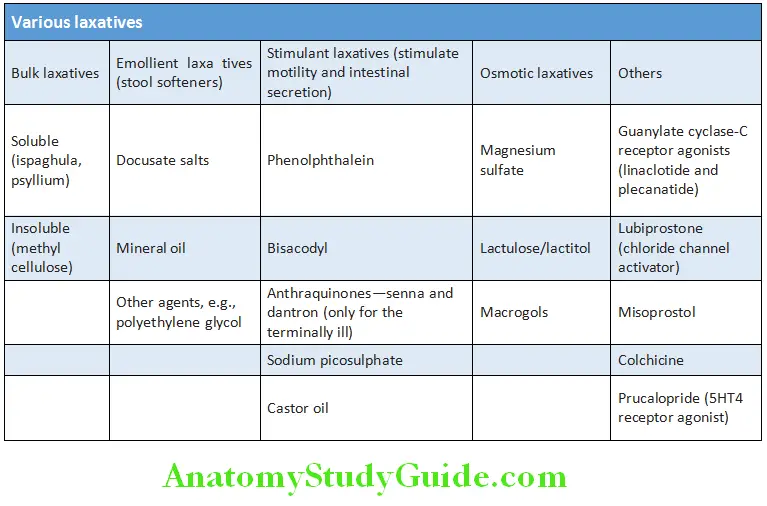
Constipation Treatment:
- Regular exercise and adequate fluid intake
- Treat the underlying cause or eliminate offending medication
- Fiber supplementation: If there is no secondary cause, increasing the fiber content of the diet and fluid intake. A fiber supplement such as wheat bran or psyllium and mucilaginous seeds and seed coats (e.g., ispaghula husk) with water two to four times per day
- Laxatives: They should be restricted to severe cases. Osmotic laxatives act by increasing colonic inflow of fluid and electrolytes by osmotic activity. This softens the stool and stimulates colonic contractility. The stimulatory laxatives act by stimulating colonic contractility and by causing intestinal secretion. Prucalopride is effective in refractory constipation
Chronic Blood and Mucus in the Stools:
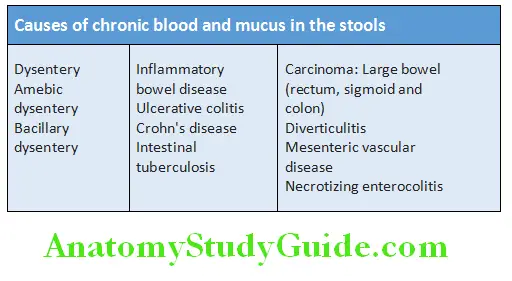
Question 6. List causes of chronic blood and mucus in the stools. How will you investigate such a case?
Answer:
Chronic Blood Causes:
Chronic Blood Investigations:
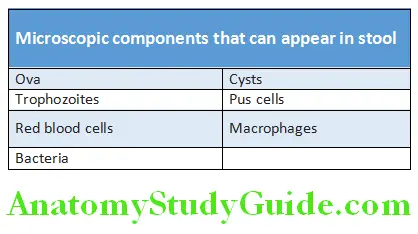
- Stool examination
- Macroscopy: Fresh blood/altered blood/foul smelling/bulky/floats in water/mucus
- Microscopy
- Stool culture and sensitivity: Grows the organism
- Proctoscopy: To detect any ulcers or tumors of rectum and hemorrhoids
- Sigmoidoscopy: To detect any ulcers/tumors in the sigmoid colon
- Colonoscopy: To visualize colon
- Barium enema: To identify any growth or filling defects, strictures, ulcers, and diverticula
- Biopsy: Of an ulcer or growth
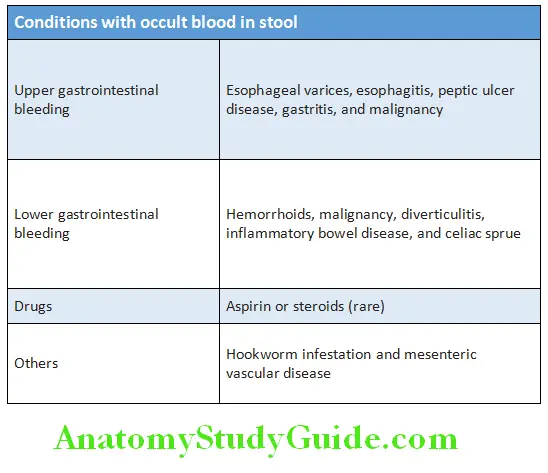
Occult Blood in the Stool:
- Stool may appear normal (i.e., no melena) in patients with gastroduodenal bleeding of up to 50–100 mL/day.
- Blood loss in stool of a normal individual varies from 0.5 mL/day to 1.5 mL/day. Occult blood tests begin to become positive usually when blood loss is around 2 mL/day.
- Test for detection of occult blood in stool:
- Guaiac test: Gastrointestinal tract bleeding is often intermittent. Hence, this test should be performed for several successive days. This test is negative in a person on iron or bismuth.
- Other tests: Fecal immunochemical tests and heme-porphyrin test.
Conditions with Occult Blood in Stool:
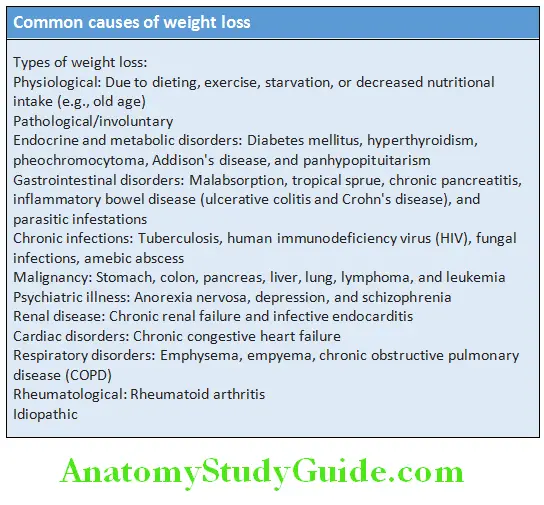
Common Causes Weight Loss:
Glossitis:
Question 7. List the causes of glossitis.
Answer:
Glossitis Definition: Glossitis is defined as inflammation of the tongue.
Glossitis Clinical Features:
- Patients may complain of lingual pain (glossodynia) or burning sensation (glossopyrosis).
- Atrophic glossitis is a sign of protein-calorie malnutrition and muscle atrophy and is commonly found in older adults.
- Median rhomboid glossitis manifests as an asymptomatic, well-defined erythematous patch in the mid-posterior dorsum of the tongue.
Glossitis Causes:
- B-complex deficiency, megaloblastic anemia (pernicious anemia), oral candidiasis, herpes, cirrhosis, iron deficiency anemia, pellagra, scarlet fever, syphilis, chemical irritants, drug reactions, amyloidosis, sarcoidosis, infections, and vesiculo-erosive diseases.
Dyspepsia:
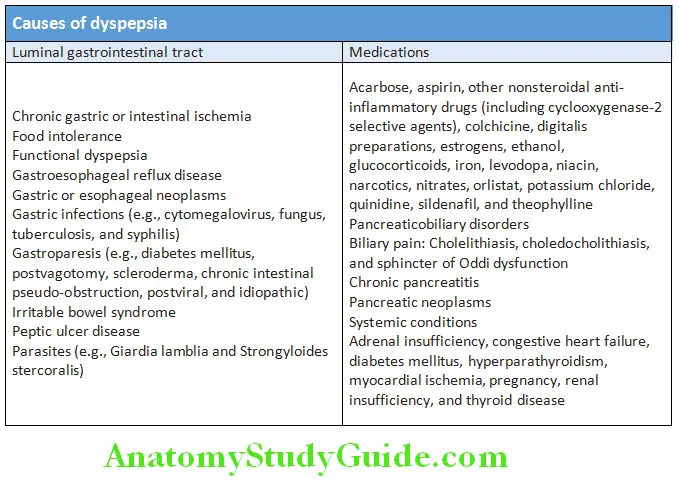
Question 8. List the causes and differential diagnosis of dyspepsia.
Answer:
Dyspepsia is derived from the Greek words dys and pepse and literally means “difficult digestion”.
- Dyspepsia is a collective description of a variety of gastrointestinal symptoms.
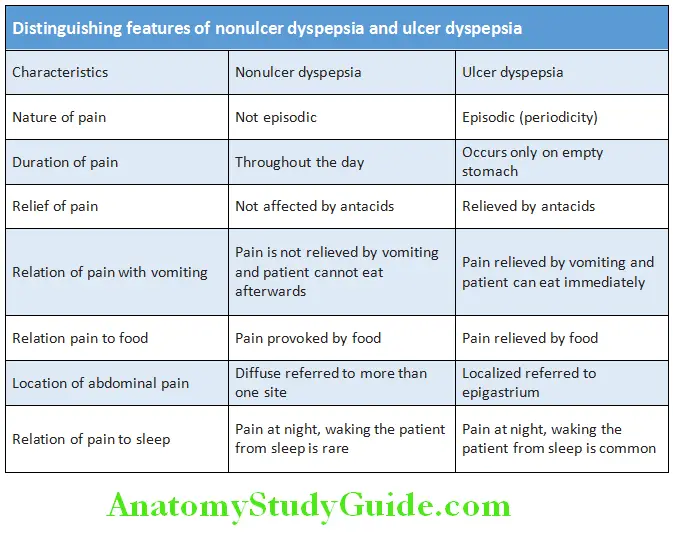
- Ulcer dyspepsia: Dyspeptic symptoms associated with peptic ulcer
- Non-ulcer dyspepsia (functional dyspepsia): No cause can be found
- Flatulent dyspepsia: Usually due to a functional disorder
- Symptoms include early satiety, flatulence, bloating, and belching predominate.

Dyspepsia Causes:
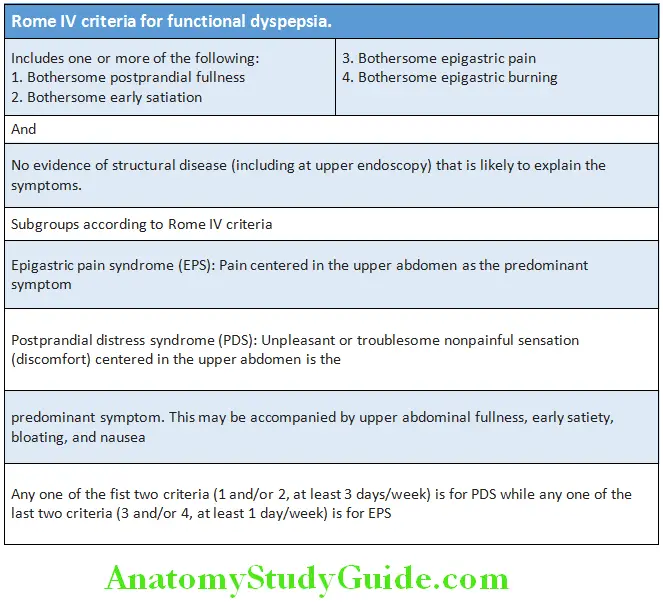
Nonulcer Dyspepsia (Functional Dyspepsia, Nervous Dyspepsia; Nonorganic Dyspepsia):
Question 9. Discuss the etiology clinical features, investigations, and management of nonulcer dyspepsia.
Answer:
Nonulcer Dyspepsia Definition: Chronic dyspepsia in the absence of organic disease.
Second most common functional gastrointestinal disorder (after irritable bowel syndrome).
Nonulcer Dyspepsia Etiology:
- It is dyspepsia in the absence of organic disease and even on detailed investigation, no cause can be found.
- Etiology is poorly understood but probably due to a spectrum of mucosal, motility and psychiatric disorders.
- Symptoms are probably due to disturbances in the motor function of the gastrointestinal tract similar to that occurring in the irritable bowel-syndrome. Both irritable bowel syndrome and nonulcer dyspepsia often exist together in the same patient.
- Helicobacter pylori infection should be excluded, because it may be responsible for symptoms in few patients.
Nonulcer Dyspepsia Clinical Features:
- Usually occurs in young (<40 years of age) females.
- Symptoms and subtypes are described.
- Morning symptoms of pain and nausea on walking are characteristic.
- Features suggestive of irritable bowel syndrome such as pellet-like stools and feeling of incomplete evacuation after defecation may be observed.
- History may reveal stress factors such as worries, financial problems, employment, and family affairs.
- On examination, no diagnostic signs, except for inappropriate abdominal tenderness on abdominal palpation.
- All the organic causes of dyspepsia such as peptic ulcer disease (PUD), drug ingestion, depression, pregnancy, alcohol abuse, etc., should be excluded.
- In older patients intra-abdominal malignancy should be excluded which may present with alarming features such as weight loss, anorexia, dysphagia, and hematemesis or melena.
Nonulcer Dyspepsia Investigations:
The history often suggests the diagnosis:
- Helicobacter pylori infection should be serologically excluded in all patients.
- Exclusion of organic causes by following investigations:
- Blood count, erythrocyte sedimentation rate (ESR) and occult blood in stools
- Liver function tests (to exclude alcoholism)
- Pregnancy test
- Barium meal
- Ultrasound scan may detect gallstones.
- Indications for endoscopy in patients with chronic dyspepsia/red flags are listed.
Indications for endoscopy in patients with chronic dyspepsia/red flags:
- Age >60 years
- Dysphagia/previous peptic ulcer disease and odynophagia
- Clinically significant weight loss (>5% usual body weight over 6–12 months)
- Protracted vomiting
- Melena
- Anemia
- Palpable mass
- Jaundice
- Family history of stomach cancer
Nonulcer Dyspepsia Management:
- Explanation, reassurance, and lifestyle changes
- Advice to avoid cigarette smoking and alcohol use
- Symptoms if associated with an identifiable cause of stress resolve with appropriate counseling
- Psychological factors influencing on gut function should
be explained and may require psychological treatment - Idiosyncratic and restrictive diets are not beneficial, but reducing intake of fat and coffee may help
- If endoscopy is noncontributory, empirical treatment is advised
- Prokinetic drugs, such as metoclopramide (10 mg three times daily) or domperidone (10–20 mg three times daily), may be given before meals for nausea, vomiting, or bloating
- Mosapride or itopride may also be tried
- H2-receptor antagonists or proton-pump inhibitors if night pain or heartburn is troublesome
- Helicobacter pylori eradication therapy, if test is positive and may be effective in some patients with functional dyspepsia
- Selective serotonin reuptake inhibitors may be effective in some patients
- Low dose tricyclic agents (e.g., amitriptyline) may be of help in up to two-thirds
- SSRI (selective serotonin re-uptake inhibitor) medication is tried in refractory cases
Distinguishing Features of Nonulcer Dyspepsia and Ulcer Dyspepsia:
Gastrointestinal Bleeding:
Upper Gastrointestinal Bleeding:
Question 10. Enumerate the etiology/causes and investigations of hematemesis upper gastrointestinal bleeding. Discuss how you will manage a case of esophageal varices.
Answer:
Hematemesis is the bleeding proximal to the duodenojejunal junction (ligament of Treitz).
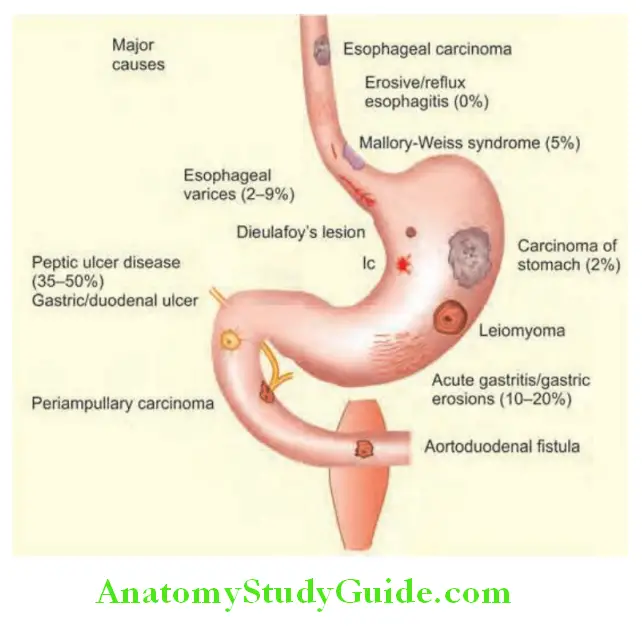
Gastrointestinal Bleeding Etiology:
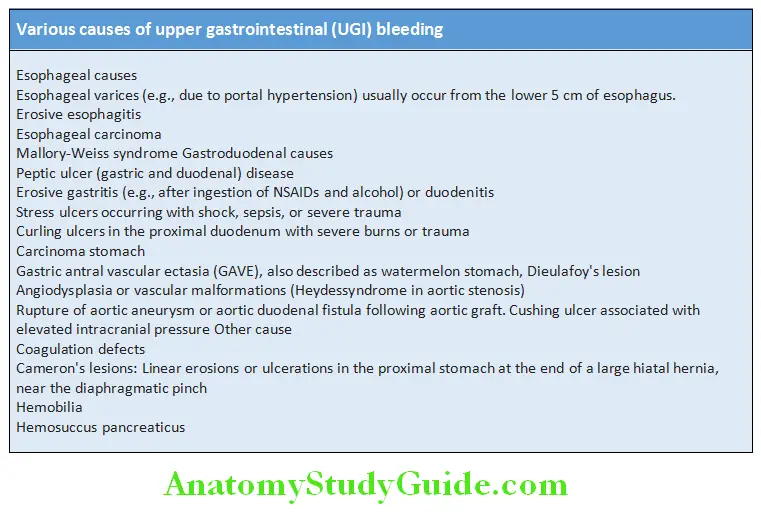
Peptic ulcers are the most common cause of upper gastrointestinal (UGI) bleeding (up to about 50%).
Presenting Symptoms And Clinical Features:
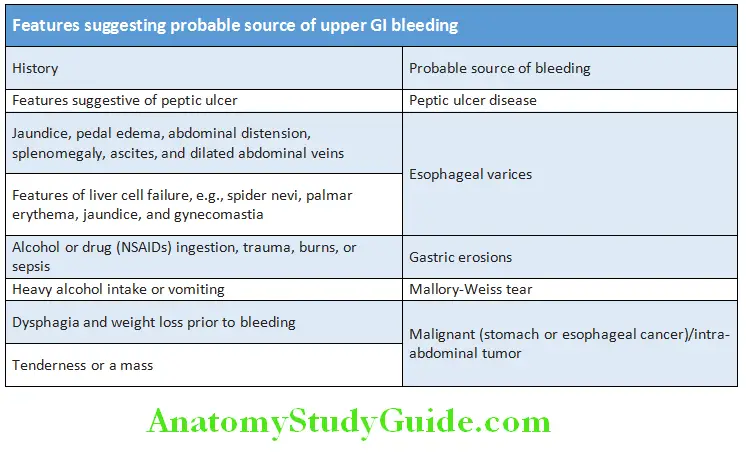
Question 11. Discuss the appropriate history and clinical features that identify the source of bleeding, quantity, volume loss, etiology, and risk factors of UGI bleed.
(or)
List the differential diagnosis for UGI bleed based on presenting symptoms and clinical features.
Answer:
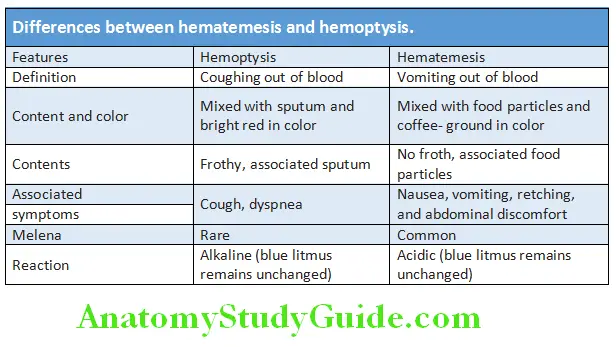
Presentation: Patient usually presents with either hematemesis (vomiting of blood or coffee-ground material) and/or melena
(black, tarry stool).
- Hematemesis: Color of the vomitus depends on how long the blood has been in the stomach and the severity of bleeding.
- Red with clots when bleeding is severe and bright red indicates rapid and sizeable bleeding.
- Black (“coffee grounds”) when less severe and bleeding is small.
- Melena: It is the passage of black, tarry, foul-smelling stools containing altered blood. The characteristic color and smell are due to the action of digestive enzymes and bacteria on hemoglobin. It usually occurs when more than 60 mL blood is lost and blood has been present in the UGI tract for at least 14 hours (and as long as 3–5 days). Occasionally, it develops due to hemorrhage from the right side of the colon.
- Severe/massive acute UGI bleeding can sometimes cause maroon or bright red stool due to passage of frank blood per-rectum (hematochezia).
- Occasionally, presentation with symptoms of blood loss only.
- These include:
- Acute loss with intravascular volume depletion: Dizziness, extreme pallor, and shock.
- Chronic loss: With symptoms of anemia Differences between hematemesis and hemoptysis are presented in Table.
Question 12. Discuss evaluation and treatment/management of upper gastrointestinal bleeding.
Answer:
Upper Gastrointestinal Bleeding History:
Physical Examination: Look for
- Vital signs, orthostatic hypotension
- Abdominal tenderness
- Skin, oral examination
- Stigmata of liver disease
- Rectal examination:
- Objective description of stool/blood
- Assess for mass, hemorrhoid
Question 13. Distinguish between upper and lower GI bleed based on clinical features.
Answer:
Differences between upper and lower GI bleed are presented in Table:
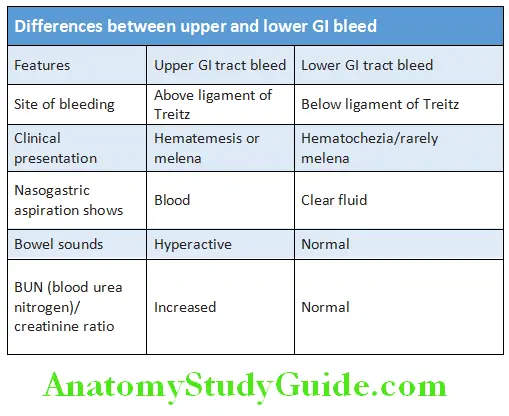
GI Bleed Basic Investigations:
- Complete blood count:
- Chronic bleeding leads to anemia, but the hemoglobin concentration and the hematocrit level may be normal after sudden, major bleeding until hemodilution occurs.
- Low platelet count: Suggests chronic liver disease, dilution, or hematologic disorder.
- Blood urea nitrogen (BUN) and creatinine: The blood urea nitrogen level increases to greater extent than the creatinine level because of increased intestinal absorption of urea after breakdown of blood proteins. An elevated blood urea with normal creatinine concentration implies severe bleeding.
- Liver function tests. They may show evidence of chronic liver disease.
- Prothrombin time: It may be prolonged in patients with chronic liver disease or in coagulation disorders or patients on anticoagulated therapy.
- Cross-matching: Potential infusion of packed red blood cells.
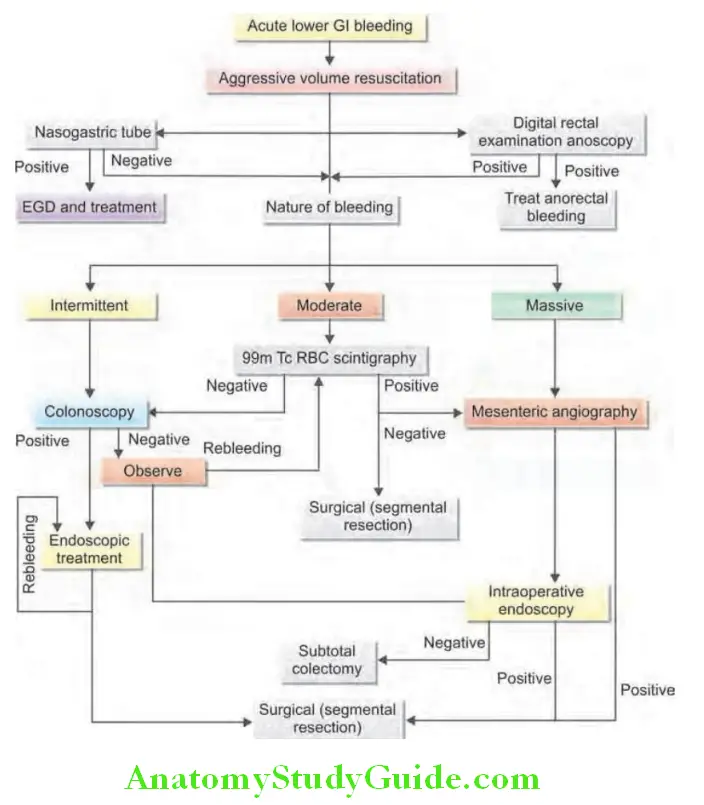
Question 14. Write short essay on management and drugs used in upper gastrointestinal bleeding.
Answer:
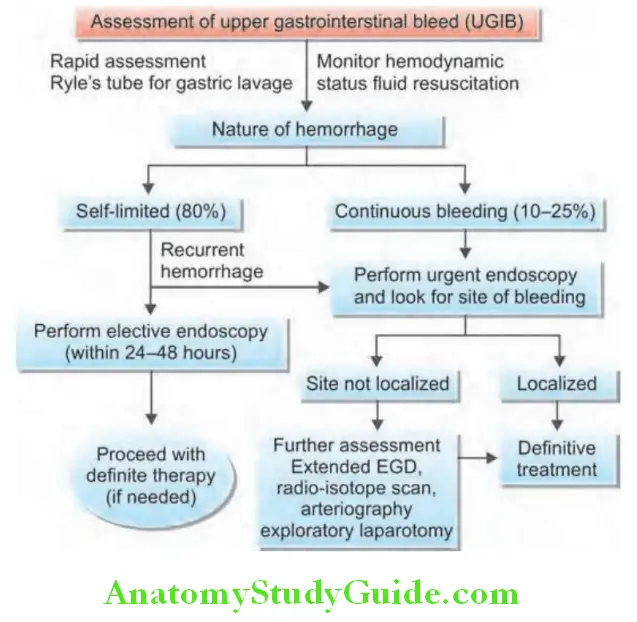
Assessment of upper GIT bleed is presented in Flowchart:
Gastrointestinal bleeding Management:
Medical resuscitation and replenishment of intravascular volume: In case of massive bleeding, resuscitation measures should be initiated simultaneously with the initial assessment
- Intravenous access: The first step is to gain intravenous access using at least one large-bore (14- or 16-gauge) intravenous catheters for essentially all patients so that normal saline can be infused as fast as necessary to maintain hemodynamic stability
- Fluid resuscitation: Adequate resuscitation and hemodynamic stabilization are essential prior to endoscopy (saline). Vasopressors if persistent hypotension
- Blood product transfusions: Initiate blood transfusions if the hemoglobin is <7 g/dL to maintain the hemoglobin at a level of ≥9 g/dL.
- Patients with active bleeding and a low platelet count (<50,000/μL) should be transfused with platelets. Patients with a coagulopathy with a prolonged prothrombin time with INR >1.5 should be transfused with fresh frozen plasma (FFP).
Initial clinical assessment:
- Circulatory status: Severe bleeding causes tachycardia, hypotension, and oliguria. Closely observe with hourly pulse, blood pressure, postural hypotension urine output, and level of consciousness
- Evidence of liver disease: May be present in patients with decompensated cirrhosis
- Comorbidity: Such as cardiorespiratory, cerebrovascular, or renal may be worsened by acute bleeding and also increase the hazards of endoscopy and surgical operations
Gastric lavage: This procedure has been abandoned in present day
- Procedure: Gastric lavage is performed by instilling 500 mL of ice-cold or tap water every 30–60 minutes
- Advantages of nasogastric or orogastric tube help to localize the site of upper GI bleeding. Determine the type of material whether red blood or coffee-ground. Assess the rate, severity, persistency, and recurrence of the bleeding. Clear the blood from stomach for better endoscopic visualization prior to endoscopy. Remove blood → reduces the risk of encephalopathy in patients with liver disease. Dilute acid-pepsin in stomach → reduces bleeding from erosions. Minimize the risk of aspiration
- Prognostic score: Rockall score is based upon age, the presence of shock, comorbidity, diagnosis, and endoscopic stigmata of recent hemorrhage
Gastrointestinal bleeding Endoscopy:
Pre-endoscopic pharmacotherapy:
For nonvariceal UGIB (upper gastrointestinal bleeding):
- IV proton pump inhibitor: 80 mg bolus, 8 mg/h drip (esomeprazole)
- Rationale: Suppress acid, facilitate clot formation, and stabilization
Goal of endoscopic therapy: To stop acute bleeding and reduce the risk of recurrent bleeding
- Early endoscopy (within 24 hours) is recommended for most patients with acute UGIB
- Achieves prompt diagnosis, provides risk stratification and hemostasis therapy in high-risk patients
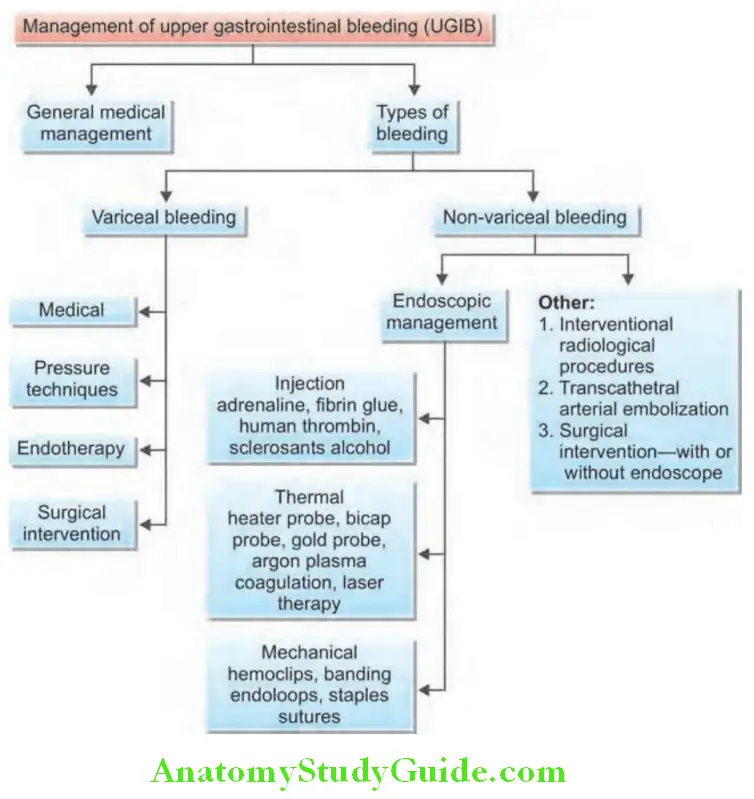
Endoscopic hemostasis therapy:
Gastrointestinal bleeding It includes:
- Epinephrine Injection
- Thermal Electrocoagulation
- Mechanical (hemoclips).
Combination therapy is superior to monotherapy Nonvariceal UGIB: Postendoscopy management
Postendoscopy management of nonvariceal UGIB:
- Patients with ulcers requiring endoscopic therapy should receive PPI x 72 hours
- Determine H. pylori status in all ulcer patients
- Discharge patients on PPI (once to twice daily), duration dictated by underlying etiology and need for nonsteroidal anti-inflammatory drugs (NSAIDs)/aspirin
- In patients with cardiovascular disease on low dose aspirin: Restart as soon as bleeding has resolved
Management of upper GI tract bleeding is summarized in Flowchart:
Question 15. Enumerate the indications for endoscopy, colonoscopy, and other imaging modalities in the investigation of Upper GI bleed.
Answer:
Upper GI bleed Endoscopy: It is the diagnostic modality of choice for acute upper GI bleeding. Endoscopy has a high sensitivity and specificity for locating and identifying bleeding lesions in the upper GI tract. Therapeutic endoscopy can in most cases achieve acute hemostasis and prevent recurrent bleeding once a bleeding lesion has been identified. Early endoscopy, within 24 hours is recommended for most patients with acute upper GI bleeding. For patients with suspected variceal bleeding, endoscopy should be performed within 12 hours of presentation.
Colonoscopy: It is indicated in patients with hematochezia and a negative upper endoscopy. It is also frequently performed in patients with melena and a negative upper endoscopy, to rule out right-sided colonic lesions which may also present with melena.
Imaging: Plain radiographs may be useful to demonstrate bowel obstruction/perforation in patients who present with pain abdomen and distention. Barium studies are contraindicated in the acute setting of UGI bleed as it may interfere with the subsequent endoscopy/surgery. USG abdomen is particularly useful in patients with suspected liver disease with clinical signs of portal hypertension.
Variceal Bleeding:
Occurs in one-third of patients with cirrhosis. In one-third initial bleeding episodes are fatal. Among survivors, one-third will rebleed within 6 weeks. Only one-third will survive 1 year or more. Management of variceal bleed is discussed..
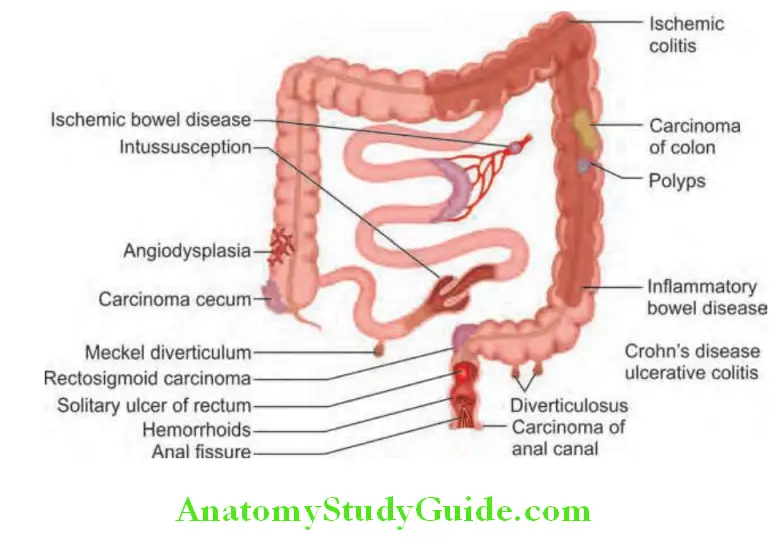
Lower Gastrointestinal Bleed:
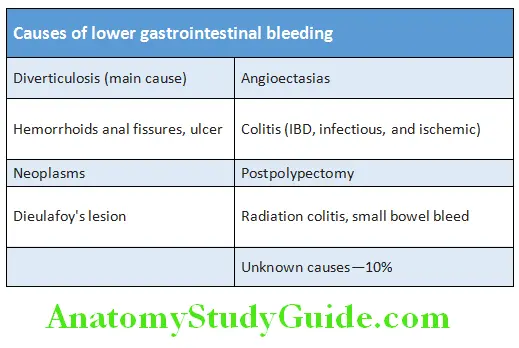
Question 16. List causes of lower gastrointestinal bleeding.
Answer:
Lower GI bleeding generally signifies bleeding from the colon or anorectum. In patients with severe hematochezia, first consider possibility of UGIB. About 10–15% of patients with presumed LGIB are found to have upper GIB.
Lower Gastrointestinal Bleed Etiology:
Management of LGI Bleed:
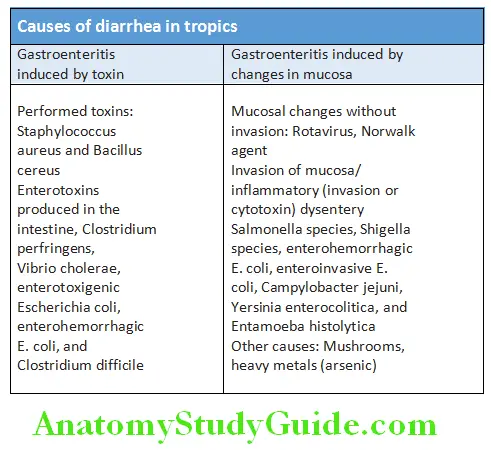
Approach To Diarrhea:
Question 17. Enumerate the common cause of diarrhea in the tropics.
Answer:
Approach To Diarrhea Definition: Daily bowel movements of three or more times are considered to be abnormal. The upper limit of stool weight is 200 g daily. Although stool weight usually considered as a “scientific” definition of diarrhea, diarrhea should not be defined solely in terms of fecal weight.
- Acute diarrhea is defined as abrupt onset of increased frequency and/or fluidity of bowel movements.
- Chronic diarrhea is defined as passage of loose stools with or without increased stool frequency for more than 4 weeks.
Large-volume versus Smallvolume Diarrhea:
- Normal rectosigmoid colon functions as a storage reservoir.
- Left colonic disorders: Inflammatory or motility disorders involving the left colon compromises this rectosigmoid
reservoir capacity and results in frequent small-volume bowel movements. - Right colonic or small bowel disorders: In diarrhea due to disorders of the right colon or small bowel and if the rectosigmoid reservoir is intact, individual bowel movements are less frequent and larger.
Frequent, small, painful stools may point to a source in the distal colon, whereas painless large-volume stools suggest a right colonic or small bowel source.
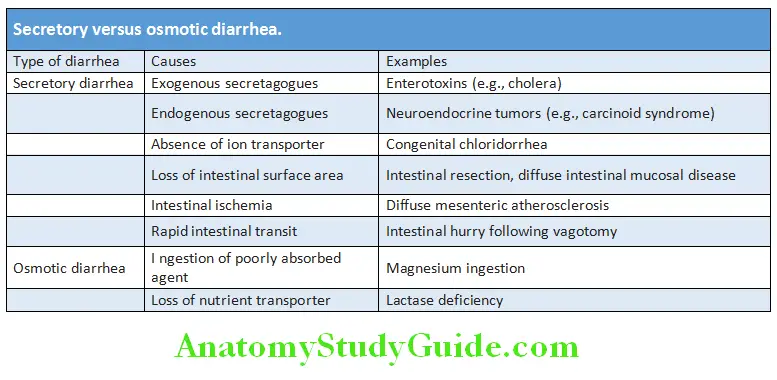
Secretory versus Osmotic Diarrhea:
- Secretory diarrhea: It results from malabsorption or secretion of electrolytes (secretory diarrhea).
- Osmotic diarrhea: It results from intestinal malabsorption of ingested nonelectrolytes.
- Osmotic diarrhea constitutes small number of cases whereas secretory diarrhea forms the much larger number of cases.
- In secretory diarrhea, sodium, potassium, and accompanying anions account almost entirely for stool osmolality. In contrast, in osmotic diarrhea poorly absorbable solutes within the lumen of the intestine account for much of the osmotic activity of stool water.
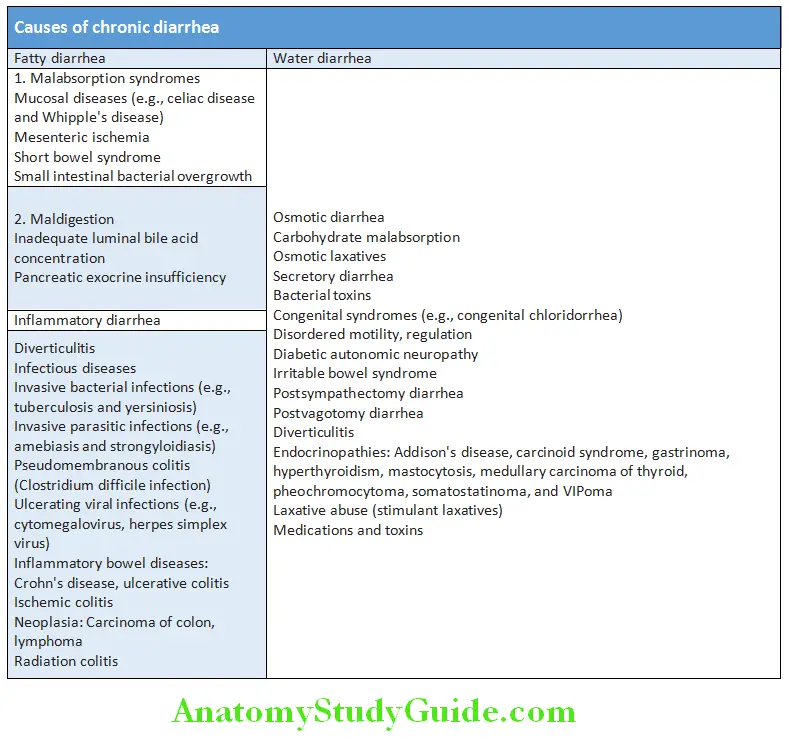
Watery versus Fatty versus Inflmmatory Diarrhea:
- Watery diarrhea: It implies a defect primarily in water absorption as a result of increased electrolyte secretion or reduced electrolyte absorption (secretory diarrhea) or ingestion of a poorly absorbed substance (osmotic diarrhea).
- Fatty diarrhea: It implies defective absorption of fat and perhaps other nutrients in the small intestine.
- Inflammatory diarrhea: It implies the presence of one of a limited number of inflammatory or neoplastic diseases involving the gastrointestinal tract.
Causes of Diarrhea in the Tropics:
Causes of Chronic Diarrhea:
Question 18. Write short note on causes of chronic diarrhea.
Answer:
Causes of chronic diarrhea:
Approach to the Patient with Acute Diarrhea:
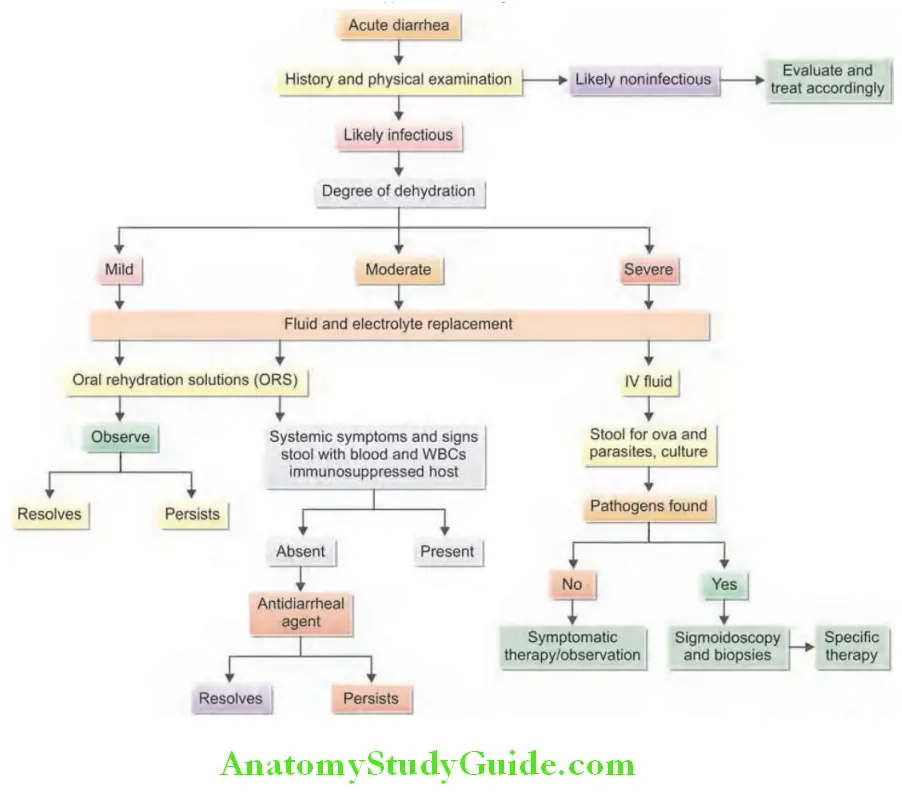
Question 19. Discuss the evaluation and management of acute diarrhea.
Answer:
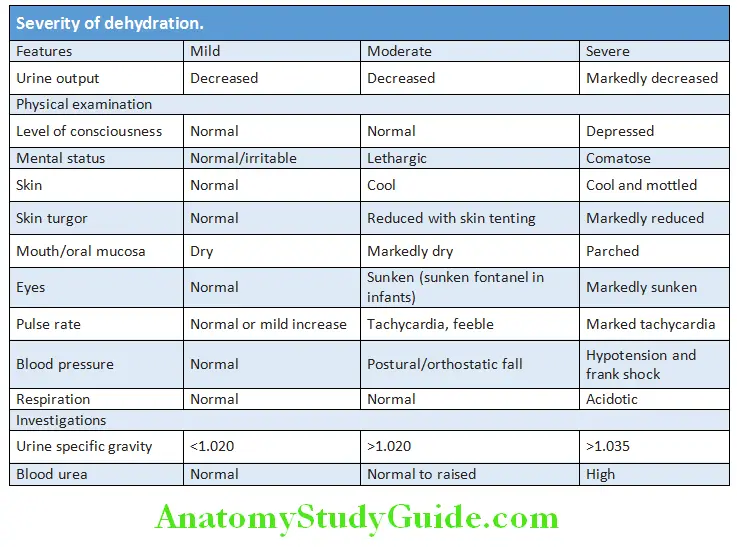
Assessment of the Patient:
- Degree of dehydration
- Evidence of specific cause
- Necessity of any diagnostic tests
- Requirement for any treatment
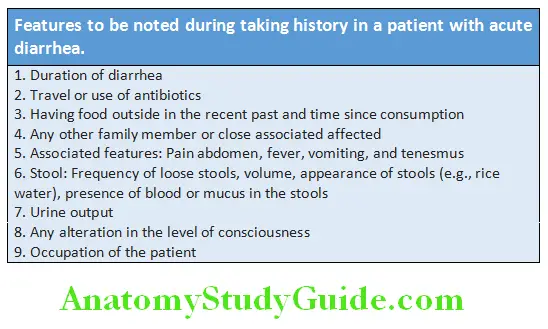
History Physical Examination:
- Examine for signs of dehydration to assess the severity of the diarrhea. These include examination of pulse, blood pressure (including postural change), skin turgor, dryness of mucous membranes (e.g., mouth), mental status, and breathing.
- Severity of dehydration.
- Electrolyte imbalances: Assess muscle strength and muscle reflexes which may be reduced in hypokalemia.
- Examination of abdomen to exclude any surgical cause (e.g., intestinal obstruction).
Question 20. Enumerate the indications for stool cultures and blood cultures in acute diarrhea.
Answer:
Laboratory Investigations:
Laboratory investigations usually do not help in the management acute diarrhea.
- Total white blood cell (WBC) count: Presence of high leukocyte count with shift to left suggests invasive bacterial infection.
- Electrolytes and acid-base status: It should be done in patients with severe dehydration. Severe diarrhea produces metabolic acidosis.
- Blood cultures: To be performed when bacteremia or a systemic infection is suspected.
- Stool examination: Grossly bloody or mucus in the stool suggests an inflammatory process. In severe cases stool should be examined for the presence of leukocytes, red cells, and cysts or trophozoites/parasites. In cholera V. cholerae show the characteristic darting motility. Stool with leukocytes considers inflammatory causes (Shigella, Salmonella, Campylobacter, E. coli, Entamoeba, and Clostridium difficile).
- Stool culture: Specific indications for stool cultures include bloody stools, stools that test positive for occult blood or leukocytes, prolonged course of diarrhea that has not been treated with antibiotics, immunocompromised host, or for epidemiologic purposes, such as cases involving food handlers.
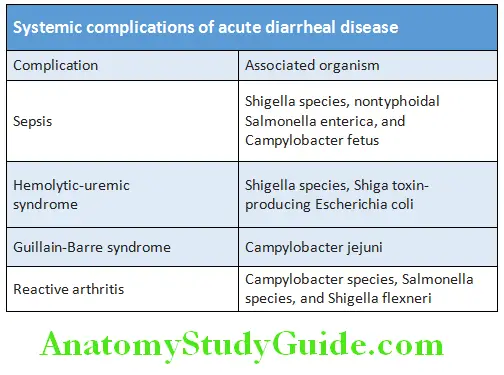
Question 21. Describe and discuss the acute systemic consequences of acute diarrhea including its impact on fluid balance.
Answer:
Systemic complications of acute diarrheal disease are presented in Table:
Effect on fluid balance:
- Usually, more than 90% of the fluid entering the small intestine is absorbed. Only about 1 liter reaches the large intestine. Further absorption occurs in the large intestine and only 100–200 milliliters of water is excreted each day in formed stools.
- When there is increased secretion and/or decreased absorption in the small intestine, large volumes enter the large intestine.
- Diarrhea occurs when this volume exceeds the absorptive capacity of the large intestine. Diarrhea stools contain large amounts of water, sodium, chloride, bicarbonate, and potassium.
- These losses cause dehydration (due to the loss of water and sodium chloride), metabolic acidosis (due to the loss of bicarbonate), and hypokalemia (due to potassium depletion).
- Among these, dehydration (negative fluid balance) is the most dangerous because it can cause decreased blood volume (hypovolemia), cardiovascular collapse, acute renal failure, mental confusion, and death if not treated promptly.
Small Bowel versus Large Bowel Diarrhea:
Acute Diarrhe Management:
Most of acute diarrhea is self-limited and fluid and electrolyte replacement are of most important in all cases
Rehydration:
- Severe diarrhea produces dehydration especially in the very young and very old
- Toxin-induced diarrhea produces stools that are usually isotonic. Concentrations of sodium and chloride are slightly less than that of plasma while bicarbonate concentration is double that of plasma. The stools also contain significant amount of potassium
- In inflammatory diarrhea the electrolyte loss is of less compared to toxigenic diarrhea
Oral rehydration solution (ORS):
Used for mild-to-moderate dehydration:
Intravenous fluids:
- Used when there is moderate-to-severe dehydration
- Usually Ringer’s lactate is administered
- In severe cases, fluids are administrated at a rate of 20 mL/kg/hour for the first 2–3 hours. If the patient improves, reduce the rate to 10 mL/kg/h for the next 2–4 hours
- Concurrently start oral rehydration therapy
Absorbents:
Kaolin absorbs the toxin and may be of use in few patients. However, it does not affect the course of the disease
Antimotility drugs:
- Used for symptomatic treatment of toxin-induced diarrhea in adults only. It should not be used in young children and elderly
- It can be given in inflammatory diarrhea along with antibiotics.
- These include:
- Opiates (e.g., morphine and codeine): They may cause respiratory depression
- Diphenoxylate/atropine combination: May cause respiratory depression and anticholinergic side effects
- Loperamide: Dose is two tablets of 4 mg each initially, then 2 mg after each unformed stool, not to exceed 16 mg/day for ≤2 days
- Bismuth subsalicylate: It acts as an antisecretory agent. Dose is one tablet every 30 minutes for a total of eight doses or 60 mL every 6 hourly
Antisecretory agents Racecadotril:
- Reduces the hypersecretion of water and electrolytes into the intestinal lumen
- Inhibits enkephalinase (an enzyme that degrades enkephalins)
- Dose: 100 mg thrice daily. To be given to patients with acute, watery diarrhea only
- Contraindication: Renal insufficiency, pregnancy, and breastfeeding
Antispasmodics:
Mild antispasmodics such as dicyclomine, hyoscine may be used in patients with significant abdominal cramps
Antibiotics Indications:
- Symptomatic patients with inflammatory diarrhea (high fever, toxicity, and abdominal pain)
- Acute febrile dysentery illness
- Diarrhea caused by Campylobacter jejuni. Early use of erythromycin or azithromycin limits the duration of illness
- Commonly used antibiotics: Quinolones (norfloxacin 400 mg and ciprofloxacin 500 mg both given twice daily or levofloxacin 500 mg given once a day) for 3–5 days
- Cholera: Doxycycline in a dose of 300 mg as single dose. Alternatives include trimethoprim-sulfamethoxazole, furazolidone, and norfloxacin
Specific treatment once cause identified:
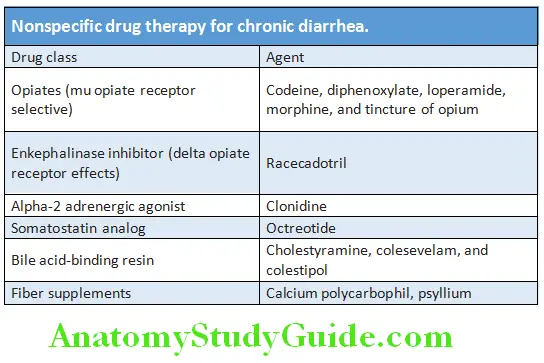
Nonspecific drug therapy for chronic diarrhea is presented in Table:
Traveler’s Diarrhea:
Question 22. Write short note on traveler’s diarrhea.
Answer:
Traveler’s diarrhea is the leading cause of illness in travelers. Usually a short-lived and self-limited.
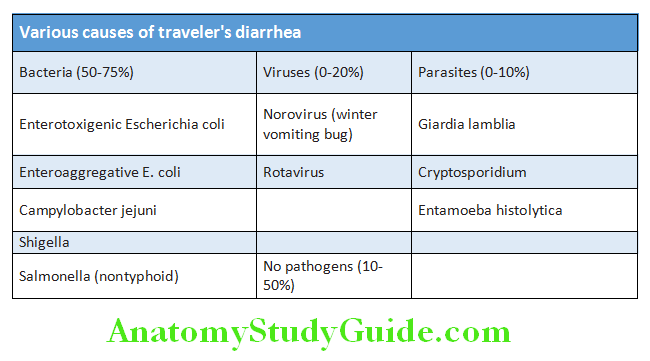
Traveler’s Diarrhea Etiology:
- Causative agents: Various pathogens causing travelers’ diarrhea are listed in Table 10.27. Most important pathogens are Escherichia coli and Enteroaggregative E. coli: rotavirus and norovirus.
- Source of infection: Main sources of infection are food and water contaminated with fecal matter.
Traveler’s Diarrhea Clinical Features:
- Usually involves intercontinental travelers.
- Symptoms: Abrupt in onset, watery diarrhea lasting 2–5 days, abdominal cramps, nausea, vomiting, anorexia, and fever.
- Signs: Diffuse tenderness over abdomen.
Diseases Of The Esophagus:
Dysphagia:
Question 23. Discuss causes and investigation (evaluation) and management of dysphagia.
Answer:
Dysphagia, from the Greek dys (difficulty, disordered) and phagia (to eat), refers to the sensation that food is hindered in its passage from the mouth to the stomach.
Causes of Dysphagia:
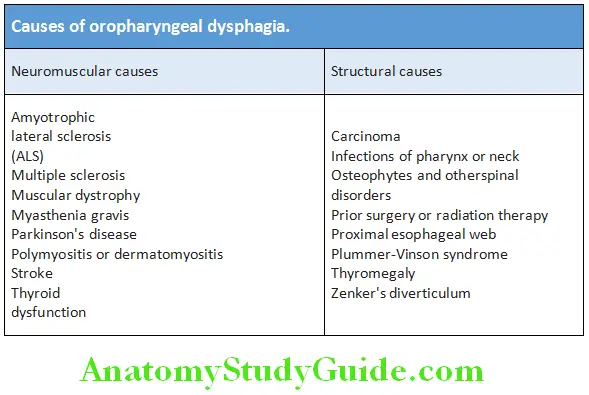
Oropharyngeal dysphagia:
Processes that affect the mouth, hypopharynx, and upper esophagus. The patient often is unable to initiate a swallow and repeatedly has to attempt to swallow. Patients frequently describe coughing or choking when they attempt to swallow. Causes of oropharyngeal dysphagia are listed in Table
Dysphagia Treatment:
- Usually self-limited and requires no treatment
- Dehydration is corrected by oral rehydration supplements
- Drugs:
- Antidiarrheal agents and antibiotics are only rarely required
- If there is fever or bloody diarrhea advise norfloxacin or ciprofloxacin. Azithromycin is used in patients who are allergic to quinolones
- Rifaximin (a poorly absorbed rifampicin derivative) is very effective against noninvasive bacterial pathogens
Prevention:
- Drugs: Doxycycline 100 mg/day for a few weeks. Norfloxacin/ ciprofloxacin/rifaximin once a day
- Probiotics may be useful
Esophageal dysphagia:
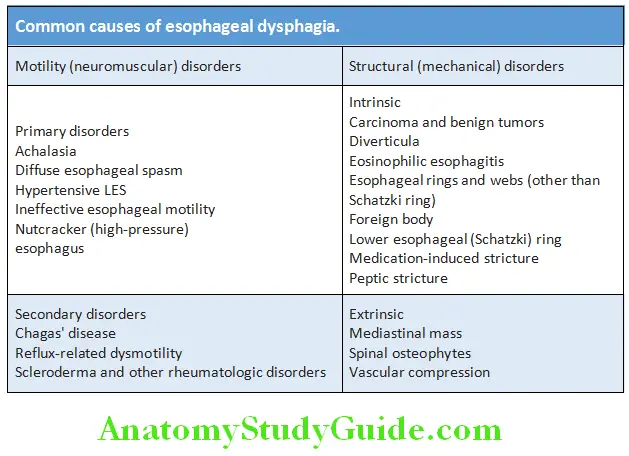
Differential Diagnosis of Dysphagia:
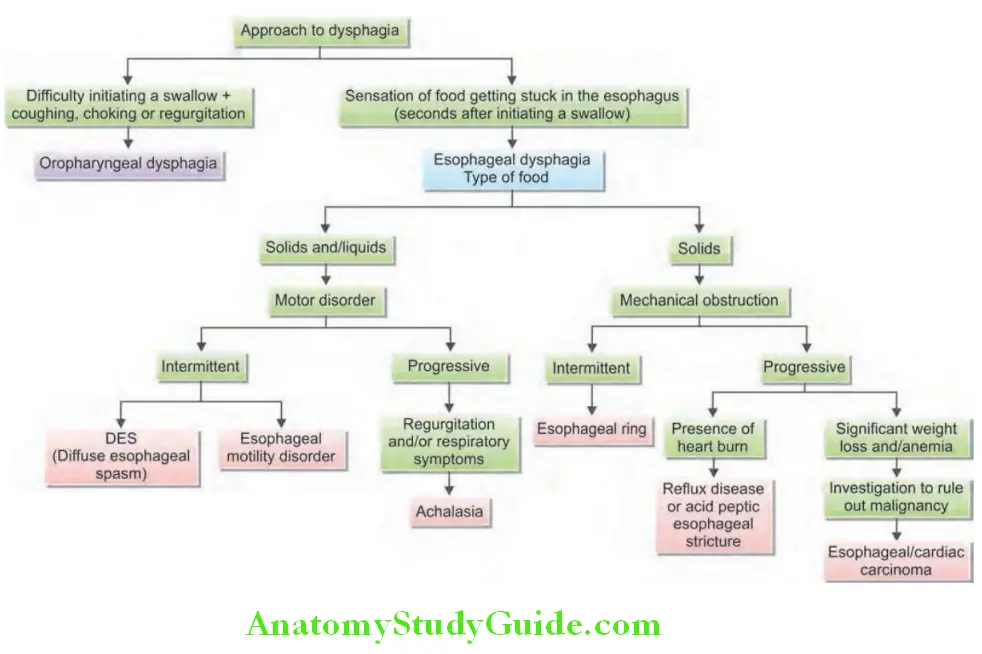
Approach to the patient with dysphagia is presented in Flowchart.
Dysphagia Investigations:
- Hemoglobin and peripheral smear for anemia
- Chest radiograph detects retrosternal goiter, mediastinal lymph nodes, aortic aneurysms, and primary and secondary malignancy of lungs.
- Esophagoscopy allows removal of foreign body, visualization and biopsy of tumors, ulcers, strictures, etc.
- Computed tomography (CT) scan of thorax
- Biopsy from the growth, ulcer, or inflamed mucosa
- Barium swallow detects tumors as filling defects or strictures (rat tail appearance).
- Esophageal motility studies (esophageal manometry)
Odynophagia:
Question 24. Write short note on the causes for odynophagia.
Answer:
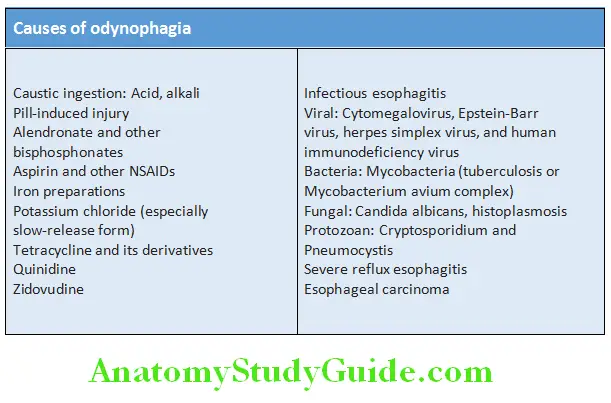
Odynophagia, or painful swallowing, is specific feature for esophageal involvement. It usually reflects an inflammatory process in the esophageal mucosa. Its severity varies. It may be a dull retrosternal ache on swallowing to a stabbing pain with radiation to the back so severe that the patient cannot eat or even swallow their own saliva.
Causes of Odynophagia:
Odynophagia Treatment:
- Iron deficiency anemia is treated with iron. It may resolve dysphagia
- Endoscopy:
- Dysphagia may require endoscopic dilatation
- Follow-up endoscopy at regular intervals to detect development of carcinoma
Gastroesophageal Reflx Disease:
Question 25. Describe the etiopathogenesis, complications, and management of gastroesophageal reflux disease (GERD).
(or)
Write short essay on reflux esophagitis and its management.
Answer:
Gastroesophageal Reflx Disease Definition:
Gastroesophageal reflux disease (GERD) is a consequence of the failure of the normal antireflux barrier to protect against frequent and abnormal amounts of gastroesophageal reflux (GER; i.e., gastric contents moving retrograde effortlessly from the stomach to the esophagus).
Spectrum of injury to the esophagus includes esophagitis, stricture, Barrett’s esophagus, and adenocarcinoma.
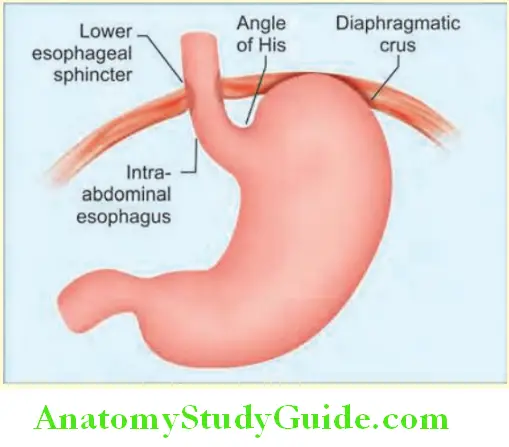
Gastroesophageal Reflx Pathophysiology:
Normal defense mechanisms preventing reflx and reflx esophagitis Several defense mechanisms prevent the reflux of gastric contents into the esophagus.
- Antireflux barrier at the gastroesophageal junction: This consists of lower esophageal sphincter (LES), at the
- Lower end of esophagus, below the diaphragm
- Striated muscles of the crural diaphragm
- Phrenoesophageal ligament
- Oblique entrance of the esophagus into the stomach (angle of His)
- Attachment of the lower esophageal sphincter (LES) to the crural diaphragm.
- Intra-abdominal:
- Pressure reinforces the LES tone.
- Esophageal clearance mechanisms: Reflux of gastric contents into the esophagus occurs in healthy persons and is normally cleared by esophagus in a two-step process.
- Volume clearance by peristaltic function: After acid reflux from stomach, the esophageal peristalsis returns the refluxed fluid to the stomach.
- Neutralization of acid by bicarbonate in the swallowed saliva: The small amounts of residual acid refluxed into the esophagus are neutralized by weakly alkaline (bicarbonate) contained in swallowed saliva.
- Epithelial defensive factors: The esophageal mucosa contains mainly three lines of defense.
- Pre-epithelial barrier: Consisting of
- Small Unstirred Water Layer
- Bicarbonate From Swallowed Saliva
- Secretions of submucosal glands.
- Epithelial defense: Consisting of cell membranes and tight intercellular junctions, buffers, and ion transporters.
- Postepithelial defense: Consists of the blood supply to the esophagus.
- Pre-epithelial barrier: Consisting of
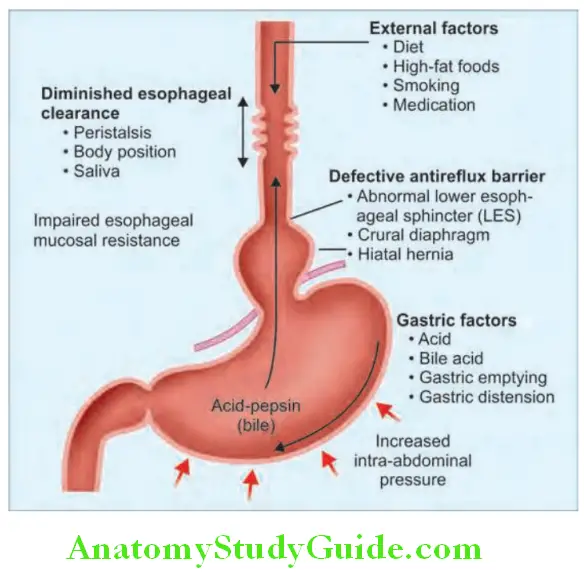
Causes of Disruption of Normal Defense:
Mechanisms:
- Defective antireflux barriers:
- Hiatus hernia (sliding type): This is characterized by sliding of the esophagogastric junction through the diaphragm. This results in increased exposure of the esophagus to acid and may lead to esophagitis, Barrett’s esophagus or peptic strictures.
- Abnormalities of lower esophageal sphincter (LES): Transient relaxation and reduced tone of LES can result in regurgitation, especially when intra-abdominal pressure is increased.
- Cigarette smoking, chocolate, alcohol, fatty foods, and caffeine cause relaxation and reduction of tone of LES.
- Cardiomyotomy and vagotomy reduce the efficiency of the LES.
- Drugs (aminophylline, β-agonists, nitrates, and calcium channel blockers) reduce the tone of LES.
- Crural diaphragm
- Increased the intra-abdominal pressure: It may occur during pregnancy, obesity, ascites, weight lifting, and straining.
- Prolonged/delayed esophageal clearance of refluxed acid: It may be due to
- Impaired Peristalsis
- Reduced Salivation
- Body position: Poor esophageal clearance leads to increased acid exposure time. Impaired production of saliva may be observed in smokers and Sjogren’s syndrome.
- Defective gastric emptying: It increases the gastric content available for reflux. It may be due to gastric outlet obstruction, anticholinergic drugs, and fatty food.
Gastroesophageal Reflx Disease Clinical Features:
Classical triad of symptoms is:
- Heartburn
- Acid Regurgitation
- Epigastric pain.
- Heartburn: It is the classic symptom of GERD. Patients usually complain of a burning feeling, rising from the stomach or lower chest and radiating toward the neck, throat, and occasionally the back. It occurs postprandially, particularly after large meals or after ingesting spicy foods, citrus products, fats, chocolates, and alcohol. The supine position and bending over may exacerbate heartburn.
- Acid regurgitation: Effortless regurgitation of acidic fluid, especially after meals and worsened by stooping or the supine position is highly suggestive of GERD.
- Epigastric pain: Sometimes radiating through to the back.
Other symptoms:
- Odynophagia (painful swallowing)
- Dysphagia: Dysphagia is reported by more than 30% of individuals with GERD. Transient to solids (due to esophageal spasm) or persistent dysphagia to solids (due to strictures).
- Less common symptoms associated with GERD include water brash, burping, hiccups, nausea, and vomiting.
- Iron deficiency anemia may occur due to blood loss.
Extraesophageal symptoms:
- Atypical chest pain which may be severe and can mimic angina.
- Upper respiratory tract: Hoarseness, sore throat, sinusitis, otitis media, chronic cough, and laryngitis
- Pulmonary: The prevalence of GERD in asthmatics is estimated between 34% and 89%. Other pulmonary diseases associated with GERD include aspiration pneumonia, interstitial pulmonary fibrosis, chronic bronchitis, and bronchiectasis.
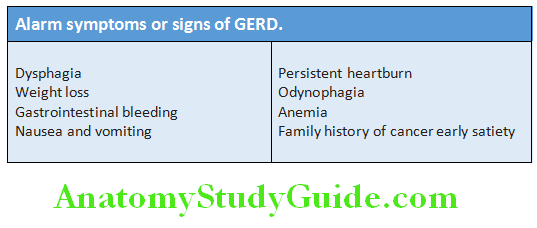
Alarm symptoms or signs:
Associated conditions: Pregnancy (reducing LES pressure due to the effects of estrogen and progesterone and possibly mechanical factors from the gravid uterus), scleroderma, achalasia cardia, and Zollinger–Ellison syndrome.
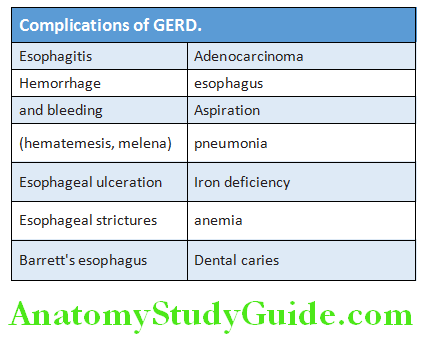
Complications of GERD:
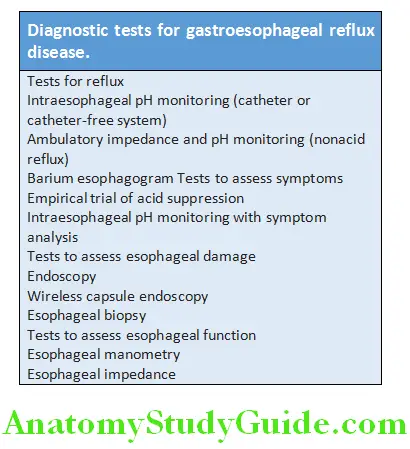
Gastroesophageal Reflx Disease Investigations:
Diagnostic endoscopy should be performed in patients who fail to respond to therapy or have alarm symptoms or signs.
- Endoscopy: It is useful for the detection of:
- Erosive esophagitis which would be visualized and confirmed by biopsy.
- Complications: Peptic stricture and Barrett’s esophagus (confirmed by biopsy)
- Barium radiography: It has no role in the diagnosis of GERD. Barium swallow and meal examination is useful for appreciation of gastroesophageal anatomy and may be important in the diagnosis of hiatus hernia.
- 24-hour pH recording: It is the “gold standard” for diagnosis of GERD.
- Prolonged measurement of pH is the most accurate method for the diagnosis of gastroesophageal reflux particularly in patients with atypical symptoms and with normal endoscopies.
- Esophageal manometry: Useful to exclude achalasia and other motility disorders.
- Resting ECG and stress ECG: To rule out ischemic heart disease (IHD).
Question 26. Write short note on management/treatment of gastroesophageal reflux disease (GERD)/reflux esophagitis.
Answer:
Gastroesophageal reflux disease Treatment:
General measures:
These are lifestyle modifications as listed.
Gastroesophageal reflux disease Medical treatment: Inhibition of gastric acid secretion is the cornerstone of the treatment of acute GERD.
Antacids: Liquid antacids buffer acid and increase LESP. They are used in the dose of 10–15 mL, 1 and 3 hours after meal and at bedtime or as needed. They relieve heart burn in mild cases.
Histamine (H2)-receptor antagonists: They decrease acid secretion. These drugs include cimetidine (800 mg bid, 400mg qid) or ranitidine (150 mg qid), or famotidine (20–40 mg bid) daily to be given with meals and before bed time, for at least 6 weeks (in mild cases).
Proton-pump inhibitors (PPIs):
- They decrease acid secretion and gastric volume. They are superior to histamine (H 2)-receptor antagonists. These include omeprazole (20–40 mg/day), lansoprazole (15–30 mg/day), pantoprazole (40 mg/day), esomeprazole (20–40 mg/day), and rabeprazole (10–20 mg/day). Maintenance doses may be necessary for 6–8 months.
- Present evidence does not support the common practice of using metoclopramide or domperidone 10 mg thrice daily either as monotherapy or an adjunct to acid suppression therapy. Its significant adverse effects argue against the use of this drug in GERD.
- Helicobacter pylori eradication does not have any therapeutic value.
- Dilatation of esophageal strictures
- Anemia is treated with oral iron or blood transfusion.
Gastroesophageal reflux disease Surgical treatment:
Indications:
- Failure to respond to medical therapy
- Patients not willing to take long-term PPIs or intolerant to PPIs,
- Patients with severe symptom, and
- Patients with regurgitation.
Gastroesophageal reflux disease Surgical measures:
Surgical resection of esophageal strictures: For patients with PPI-refractory GERD, anti-reflux mucosectomy (ARMS) or anti-reflux mucosal ablation (ARMA) can be tried.
Antireflux surgery: Laparoscopic fundoplication for patients with PPI-refractory GERD, anti-reflux mucosectomy (ARMS) or anti-reflux mucosal ablation (ARMA) can be tried. (additional valve mechanism) yields results comparable to continued PPI therapy.
Lifestyle modifications in the treatment of GERD:
- Avoid foods such as fatty food, alcohol, mint, tomatobased foods, spicy foods, coffee, tea, and acidic foods
- Avoid late night meals before retiring
- Avoid weight lifting, stooping, and bending at waist
- Elevation of the head of the bed in patients with regurgitation or heartburn during night
- Weight reduction
- Stop smoking, alcohol
- Frequents feeds of small volume
Barrett’s Esophagus:
Question 27. Write short answer on Barrett’s esophagus.
Answer:
Barrett’s esophagus is a premalignant condition, in which the normal squamous lining of the lower esophagus is replaced by columnar mucosa (columnar lined esophagus; CLO). The columnar mucosa may show areas of intestinal metaplasia (with goblet cells). It is an adaptive response to chronic gastroesophageal reflux and is often asymptomatic.
The risk of esophageal cancer depends on the severity and duration of reflux and it may be detected when the patient presents with esophageal cancer. It is more common in men, obese, and above the age of 50. It is weakly associated with smoking but not with alcohol intake.
Barrett’s Esophagus Diagnosis: It needs multiple systematic biopsies which may show intestinal metaplasia and/or dysplasia.
Barrett’s Esophagus Management:
Regular endoscopic surveillance to detect dysplasia at an early stage.
Currently recommendation are as follows:
- Barrett’s esophagus with intestinal metaplasia, but without dysplasia:
- Should undergo endoscopy at 3–5 yearly intervals, if the length of the Barrettic segment is 3 cm and at 2–3 yearly intervals if the length is >3 cm.
- Low-grade dysplasia: It should be endoscoped at 6-monthly intervals.
- Treatment is indicated only for symptoms of reflux or complications (e.g., stricture).
Endoscopic therapies: Such as radiofrequency ablation or photodynamic therapy, can induce regression. However, they are used only for patients with dysplasia or intramucosal cancer.
High-grade dysplasia or intramucosal carcinoma: Treatment options are either esophagectomy or endoscopic therapy, with a combination of endoscopic resection of any visibly abnormal areas and radiofrequency ablation of the remaining Barrett’s mucosa, as an “organ-preserving” alternative to surgery.
Hiatus Hernia
Question 28. Write short note on hiatus hernia.
Answer:
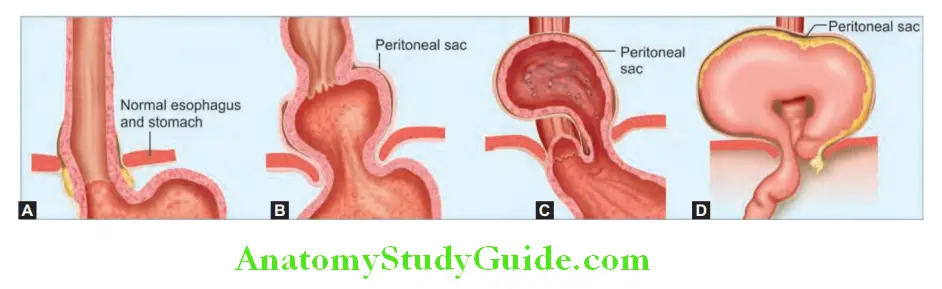
It is the herniation of elements of the abdominal cavity (part of stomach) through the diaphragm into the thoracic cavity.
Hiatus Hernia Types:
- Sliding or type I hiatus hernia: It is the most common type. In this type, the gastroesophageal junction and the fundus of stomach slide upward above the diaphragmatic hiatus.
- True paraesophageal (rolling) or type II hiatus hernia: It is uncommon. In this type, location of gastroesophageal junction is in its normal position, but the fundus and parts of the greater curvature of the stomach herniate into the mediastinum alongside the esophagus.
- Mixed paraesophageal hernia or type III: In this type, gastroesophageal junction and a large part of the stomach herniate into the mediastinum.
Predisposing factors: Obesity, pregnancy and ascites. Occurs in 33% of normal adults and 50% of elderly.
Hiatus Hernia Clinical Features:
- Majority of hiatus hernia are asymptomatic. Hiatus hernia predisposes to gastroesophageal reflux disease (GERD), and hence, symptoms of GERD may be present.
- Type I: Usually asymptomatic or present with symptoms of heartburn or acid regurgitation.
- Type II and III may present with epigastric pain, chest pain, substernal fullness, shortness of breath, nausea, or vomiting.
Hiatus Hernia Investigations:
Plain radiograph of the chest: Hernia may be visible as a gas bubble, often with a fluid level behind the heart.
Barium swallow/meal: It is the best method of diagnosis and demonstrates the presence of gastroesophageal junction in the thorax.
Hiatus Hernia Investigations Endoscopy
Hiatus Hernia Investigations Management:
- Asymptomatic hiatus hernias do not require any treatment. Surgical repair of hernia is required in selected cases with gastroesophageal reflux
- Symptomatic rolling hiatus hernias require surgical repair because it is potentially liable to undergo volvulus as a dangerous complication.
Hiatus Hernia Investigations Surgical treatment:
- Repair of the diaphragmatic defect
- Fixing the stomach in the abdominal cavity (fundoplication) combined with an antireflux procedure
Achalasia of the Esophagus:
Question 29. Write short note on achalasia cardia and its diagnosis/investigations.
Answer:
Achalasia is characterized by esophageal aperistalsis and results from progressive degeneration of ganglion cells in the myenteric plexus in the esophageal wall, causing failure of relaxation of the hypertonic lower esophageal sphincter in response to the swallowing wave. Failure of propagated esophageal contraction results in progressive dilatation of the gullet.
Achalasia of the Esophagusb Cause: Unknown. Autoimmune, neurodegenerative, and viral etiologies have been suggested. Reduction in nitric oxide synthase containing neurons is detected by immunohistochemical staining in the lower esophageal sphincter. There is degeneration of ganglion cells within the sphincter and the body of the esophagus. Infection with Trypanosoma cruzi in Chagas’ disease causes a syndrome that is clinically similar to achalasia.
Achalasia of the Esophagus Clinical Features:
- Age and gender: Occurs equally in males and females and at all ages but is rare in childhood.
- Dysphagia: It develops slowly, is initially intermittent and characteristically for both liquids and solids from the onset (worse for solids). Dysphagia is eased by drinking liquids, and by standing and moving around after eating.
- Episodes of chest pain: Spontaneous chest pain occurs due to esophageal spasm which may be misdiagnosed as cardiac.
- Regurgitation of food from the dilated esophagus: As the disease progresses, dysphagia worsens and caused poor emptying of the esophagus. This may produce nocturnal pulmonary aspiration and aspiration pneumonia.
- Heartburn does not occur because the closed esophageal sphincter which prevents gastroesophageal reflux.
- Achalasia predisposes to squamous carcinoma of the esophagus.
Achalasia of the Esophagus Investigations:
- Chest X-ray: It shows a dilated esophagus. Sometimes fluid level may be observed behind the heart. There is absence of fundic gas shadow.
- Barium swallow: There is absence of peristalsis and often synchronous contractions in the body of the esophagus. There is tapered narrowing of the lower esophagus producing a “bird’s beak” appearance due to failure of the sphincter to relax.
- Manometry shows high-pressure, nonrelaxing lower esophageal sphincter with poor contractility of the esophageal body.
- Endoscopy: It should be performed because carcinoma of the cardia can mimic the presentation and radiological and manometric features of achalasia (“pseudo-achalasia”).
Achalasia of the Esophagus Management:
Treatment for achalasia is palliative
Achalasia of the Esophagus Endoscopic:
- Endoscopic dilatation of the LES (lower esophageal sphincter)
- Endoscopically directed injection of botulinum toxin into the lower esophageal sphincter (intersphincteric injection)
Achalasia of the Esophagus Surgical:
- Surgical myotomy (Heller’s operation)
- Peroral endoscopic myotomy (POEM)
Eosinophilic Esophagitis
Question 30. Write short note on eosinophilic esophagitis.
Answer:
- Eosinophilic esophagitis is characterized by eosinophilic infiltration of esophageal mucosa.
- Atopy (allergic rhinitis, eczema, and asthma) is common, and food allergens may trigger the process.
- Dysphagia is prominent, but symptoms can also mimic GERD.
- Endoscopy reveals—include corrugated mucosa, longitudinal mucosal furrows, fixed esophageal rings or trachealization whitish mucosal plaque or exudate, stricture, and mucosal friability giving the appearance of crepe paper.
- Biopsy ≥15 eosinophils per HPF
- Treatment:
- First-line therapy consists of PPIs, which also treats concomitant GERD.
- Topical steroids (swallowed fluticasone, 880–1760 μg/d in two to four divided doses, or swallowed budesonide, 1–2 mg/d in two to four divided doses) are options; prednisone is an alternate option if topical steroids are ineffective.
- Six food elimination diet (SFED) (eggs, milk, soy, gluten, tree nuts, and seafood).
- If no response higher doses of topical steroids, systemic steroids, elimination diet trials, or cautious esophageal dilation

Diseases Of The Stomach And Duodenum:
Peptic Ulcer Disease:
Question 31. Discuss the etiology, pathogenesis, pathology, clinical features, investigations, and management of peptic ulcer disease or acid peptic disease.
Answer:
Peptic Ulcer Disease Definition:
An ulcer in the gastrointestinal (GI) tract may be defined as a break in the lining of the mucosa, with appreciable depth at endoscopy or histologic evidence of involvement of the submucosa.
Sites of Peptic Ulcer:
Any portion of the GI tract exposed to acidic gastric juices
- Duodenum: More common in the first portion of the duodenum (anterior or posterior wall) than in the stomach. Occasionally occurs at both anterior and posterior sites (“kissing” ulcers)
- Stomach: Lesser curvature near the junction (transitional zone) of the body and antrum
- Proximal ulcers: Located in the body of the stomach
- Distal ulcers: Located in the antrum and angulus of the stomach
- Gastroesophageal junction of esophagus
- Anastomotic site: Occurs in patients who have undergone a distal gastric resection. Occur at margins of the gastroduodenal anastomosis/gastrojejunostomy (anastomotic ulcer)
- Multiple ulcers: In the duodenum, stomach, and/or jejunum in Zollinger-Ellison syndrome
- At metaplastic or heterotopic gastric mucosa, e.g., Meckel diverticulum within an ileum having ectopic gastric mucosa
Incidence: ~12% in males and 10% in females.
Peptic Ulcer Disease Etiology:
Question 32. Write short essay/note on risk factors for peptic ulcer disease.
Answer:
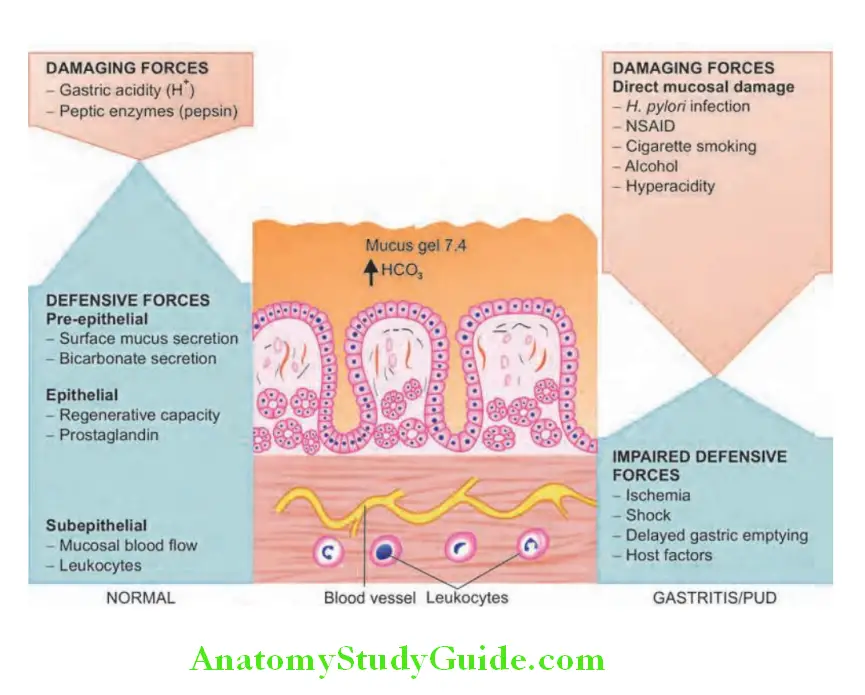
Normal process in the stomach:
Two opposing sets of forces keep stomach in a normal state:
- Damaging forces
- Defensive forces.
1. Peptic Ulcer Damaging forces: Capable of inducing mucosal injury are two gastric secretory products hydrochloric acid pepsinogen.
2. Peptic Ulcer Defensive forces is a three-level barrier composed of pre-epithelial, epithelial, and subepithelial elements.
Pre-epithelial barrier is a mucus-bicarbonate layer of the stomach.
- Surface mucus secretion: Mucin is secreted by surface foveolar cells.
- Actions of mucus are:
- Mucus layer promotes formation of an “unstirred” protective layer of fluid on the mucosa.
- Prevents the direct contact of large food particles with the epithelium.
- Impedes the diffusion of ions and molecules such as pepsin.
- Bicarbonate secretion into mucus by surface epithelial cells → diffuse into the unstirred mucus → buffer the hydrogen ions entering from the luminal aspect → result in a pH gradient, ranging from 1 or 2 at the gastric luminal surface, and reaching to a neutrality of 6–7 along the epithelial cell surface.
Peptic Ulcer Epithelial barrier: Consists of surface epithelial cells act through several factors, such as
- Production of mucus,
- Epithelial cell ionic transporters that maintain intracellular pH,
- Bicarbonate production
- Intracellular tight junctions.
Subepithelial barrier:
- Rich gastric mucosal blood flow: Provides
- Bicarbonate (Hco3–), Which Neutralizes The Acid Generated By Parietal Cell
- An Adequate Supply Of Nutrients And Oxygen, And
- Removes toxic metabolic by-products.
Pathogenesis of Peptic Ulcer:
Question 33. Write short essay/note on Helicobacter pylori and its role in pathogenesis (pathophysiology) of gastric ulcer.
Answer:
The imbalances between mucosal defensive forces (disruption of any of protective mechanisms) and damaging forces (direct mucosal injury) cause chronic gastritis and also PUD.
Direct mucosal injury/increased damage:
Majority of PUD (both gastric and duodenal ulcers) can be attributed to NSAIDs and H. pylori.
- Helicobacter pylori is a gram-negative spiral bacteria with multiple unipolar flagella that allow them to move freely through the gastric mucus layer, where they remain protected from low gastric pH. It is one of the most important, common, primary causes of PUD. It is associated with ~85–90% of duodenal and ~65% of gastric ulcers. Helicobacter pylori infection remains one of the most common chronic bacterial infections in humans more than 50% of the world’s population is infected with the bacterium. H. pylori also plays a role in the development of gastric and duodenal ulcer, gastritis, MALT (mucosal-associated lymphoid tissue) lymphoma, and gastric adenocarcinoma.
- Mode of spread: Oral-oral or feco-oral route either by kissing or ingestion of contaminated vomitus.
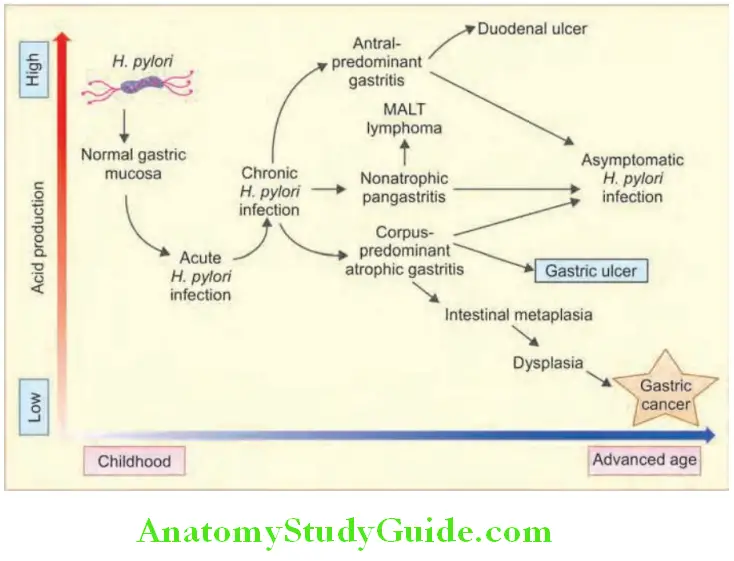
- Lesions produced: H. pylori may attach to gastric epithelium causing damage to the mucosa. Causes chronic antral gastritis with high acid production → may progress to pangastritis → resulting multifocal atrophic gastritis → increased risk of gastric adenocarcinoma. Natural history of H. pylori infection is shown.
- Nongastric diseases and H. pylori infection: Raynaud’s, scleroderma, idiopathic urticaria, acne rosacea, migraine, thyroiditis, Guillain-Barré syndrome, coronary artery disease, immune thrombocytopenic purpura.
- Mechanism of action by H. pylori:
- Flagella: It makes them motile, allows them to burrow and live beneath the mucus layer above the epithelial surface.
- Urease: It is produced by H. pylori→ converts urea into ammonia (strong alkali) → raises the local gastric pH, acts on the antral G cells → release of gastrin → hypergastrinemia → result in hypersecretion of gastric acid.
- Adhesion molecule: It helps it to bind to gastric epithelial (surface foveolar) cells.
- Enzymes: These include proteases and phospholipases act on the mucous gel → reduce the mucosal defense.
- Cytotoxins: Two genes namely cytotoxin-associated gene A (CagA) and vacuolating agent (vacA) gene cause gastritis, peptic ulceration, and cancer.
- Cytokine induces inflammatory response: Normally H. pylori does not invade the cells/tissues. It causes increased production of proinflammatory cytokines [interleukin (IL)-1, IL-6, tumor necrosis factor (TNF) and IL-8] by the mucosal epithelial cells → activation of neutrophils and macrophages (inflammatory response to gastric mucosa) → release of lysosomal enzymes, leukotrienes, and reactive oxygen species → impairs mucosal defense. The cytokines also stimulate gastrin release → increased acid production.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) and aspirin:
- Causes:
- Direct Chemical Irritation Of Mucosa
- Suppresses Mucosal Prostaglandin Synthesis
- Reduces the bicarbonate secretion.
- Cigarette smoking impairs blood flow to the mucosa and healing of mucosal damage.
- Alcohol, radiation therapy, and chemotherapy: Direct injury to mucosal cells.
- Ingestion of chemicals: Such as acids or bases cause direct injury.
- Gastric hyperacidity: It is induced by H. pylori infection, parietal cell hyperplasia, and Zollinger–Ellison syndrome.
- Others: High-dose corticosteroids that suppress prostaglandin synthesis and impair healing, other drugs (e.g., bisphosphonates, cocaine, and amphetamines), hypercalcemia, psychological stress, duodenal gastric reflux, Crohn’s disease, and systemic mastocytosis.
- Stress ulcers: They occur with shock, sepsis, or severe trauma.
- Curling ulcers: They develop in the proximal duodenum with severe burns or trauma.
- Cushing ulcers: They develop in the stomach, duodenum, and esophagus in patients with intracranial disease. Highly prone for perforation.
Pathogenesis of Peptic Ulcer Clinical Features:
Recurrent episodes of abdominal pain: It is the most common presentation and has three notable characteristics:
1. Localization to the epigastrium: Pain is referred to epigastrium and the patient will be able to localize the site with one finger (pointing sign). The characteristics of pain are:
- Nature: Usually burning in character or gnawing discomfort.
- Radiating pain: May radiate to the back, thorax, and other parts of abdomen.
- Nocturnal: Pain in duodenal ulcer occurs 90 minutes to 3 hours after a meal. May occur at night (most specific) and wakes the patient from sleep between midnight and 3 AM, and is relieved by food, milk, or antacids.
- Hunger pain: Pain occurs on empty stomach (painful hunger) relieved by food or antacids.
2. Relationship to food:
- Pain is usually relieved by food, milk, antacids, belching, or vomiting in duodenal ulcer.
- In contrast, in few patients with gastric ulcer food may precipitate the pain.
3. Periodicity (episodic pain):
- In untreated patients, pain tends to occur in episodes. Each episode consisting of daily pain lasting 2–8 weeks, separated by prolonged asymptomatic intervals.
- Between episodes (periods of remission) patient may be perfectly well and may be able to eat even heavy or spicy meals without apparent discomfort.
- During the initial stages, the episodes tend to be of short in duration and less frequent. Later, the episodes become longer in duration and more frequent. More symptomatic during winter and spring. Relapses are more common in smokers compared to nonsmokers.
Pathogenesis of Peptic Ulcer Other symptoms:
Retrosternal burning (heartburn), water-brash (excessive salivation), loss of appetite, and acidic regurgitation into the throat and vomiting. Persistent daily vomiting suggests gastric outlet obstruction. Fullness, bloating, anorexia, nausea, and dyspepsia. Tarry stools or coffee-ground vomitus indicate bleeding. Rarely, with anemia due to chronic blood loss, abrupt hematemesis, acute perforation, or gastric outlet obstruction.
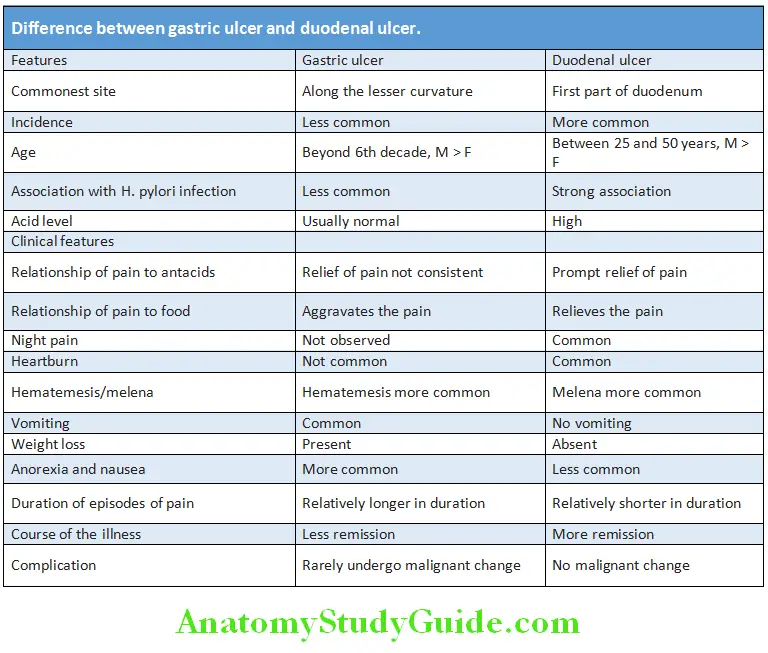
Difference between gastric ulcer and duodenal ulcer is shown in Table:

Complications:
Question 34. List complications of peptic ulcer disease.
Answer:
Complications of peptic ulcer:
- Upper gastrointestinal bleeding (20%)
- Perforation of ulcer (6–7%)
- Gastric outlet obstruction 1–2% (with fluid and electrolyte imbalance), gastrocolic or duodenocolic fistulas
- Rarely malignant transformation
- Rarely pancreatitis due to posterior penetration of ulcer
Investigations/Diagnosis:
Question 35. Discuss diagnosis of peptic ulcer disease.
Answer:
Anatomic diagnosis: Documentation of a peptic ulcer needs either a radiographic (barium study) or an endoscopic examination.
- Endoscopy: It is most sensitive and specific for the detection of ulcer disease of the upper GI tract. Typical location of peptic ulcer is duodenal bulb and lesser curvature of stomach.
- Advantages of endoscopy are:
- Direct visualization of mucosa (to determine if an ulcer is a source of blood loss) and the ulcer (even lesions too small to detect by radiographic examination),
- Useful for photographic documentation of a mucosal defect
- Biopsy can be taken to rule out malignancy (about 10% of gastric ulcers are malignant) or H. pylori.
- Endoscopic ultrasound: It may be useful in detecting an unsuspected submucosal component or enlarged lymph nodes (e.g., in gastric malignancies such as lymphoma and linitis plastica).
- Etiologic diagnosis: The cause of the ulcer must be established. The major risk factor for peptic ulcers is either H. pylori or NSAID
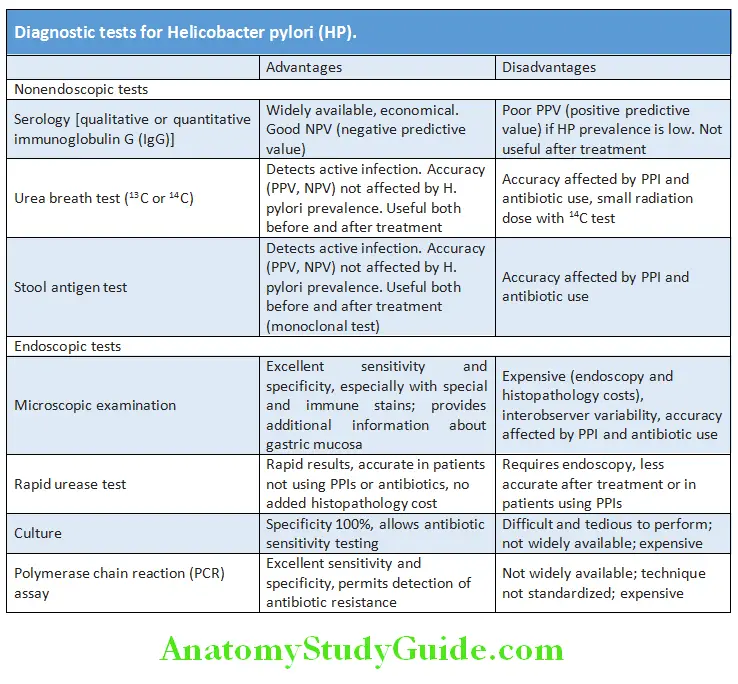
- Tests for Helicobacter pylori.
Question 36. Discuss the investigation done in Helicobacter pylori infection.
Answer:
- Nonsteroidal anti-inflammatory drugs: Diagnosis is established based on history of drug use and symptoms of pain.
- Hypersecretory syndromes: Zollinger-Ellison syndrome should be considered in patients with multiple ulcers. Serum gastrin and gastric acid analysis should be performed in these patients.
Question 37. Discuss the medical management of peptic ulcer disease and mention the new drugs used in its treatment.
(or)
Discuss management of Helicobacter pylori infection/Helicobacter pylori eradication regimens.
Answer:
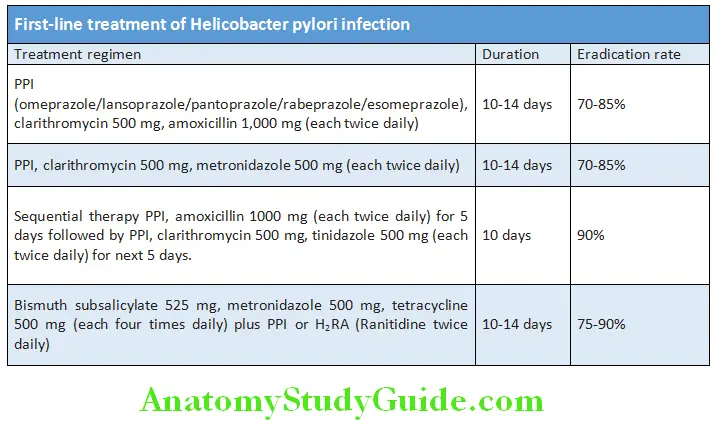
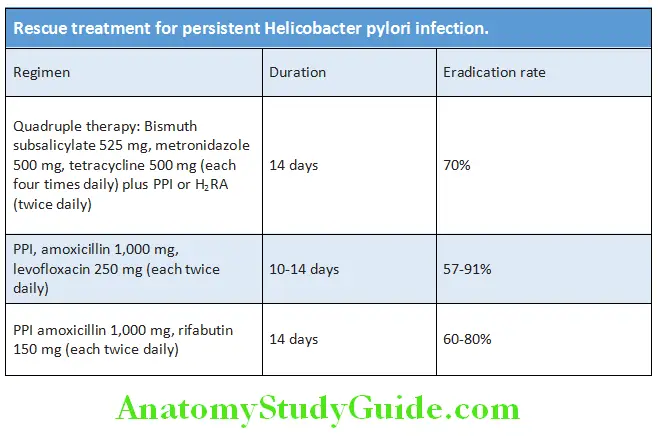
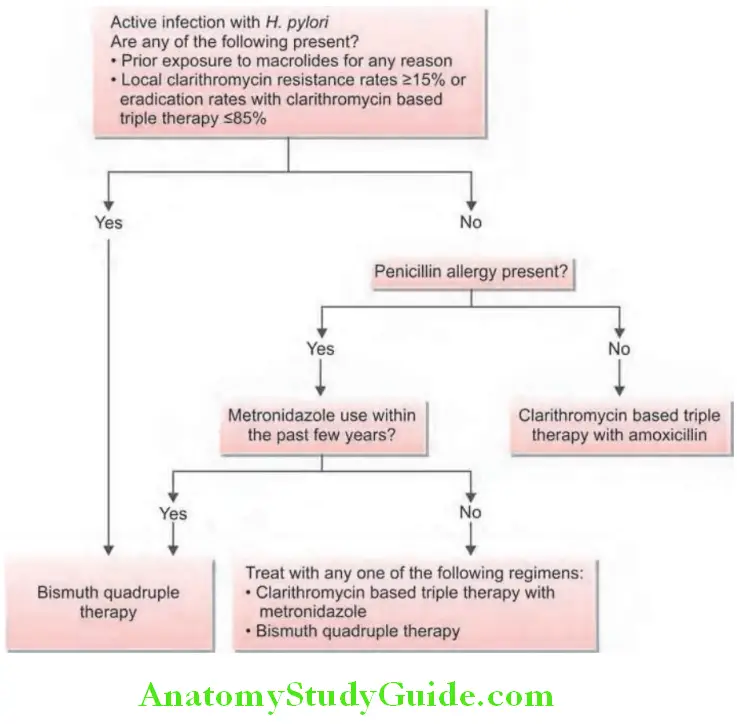
Helicobacter Pylori Treatment/Management:
Treatment may be divided into short-term management and long-term management (intermittent, maintenance, and surgical treatment).
1. Short-term management:
- General measures:
- General measures in peptic ulcer disease:
- Avoid: Cigarette smoking, aspirin, and NSAIDs
- Alcohol to be avoided
- No special dietary advice is necessary
- Acid neutralizing/inhibitory drugs
- Antacids: Neutralizes the secreted acid and rarely used at present.
- Mainly used for symptomatic relief of dyspepsia.
- Preparation: Tablet or liquid preparations
- Dose: 15–30 mL liquid antacid 1 and 3 hours after food and at bed time for 4–6 weeks.
- Commonly used antacids: Combination of aluminum hydroxide and magnesium hydroxide. Others include calcium carbonate and sodium bicarbonate.
- Side effects:
- Aluminum compounds cause constipation, and phosphate depletion and interfere with the absorption of digoxin and tetracycline
- Magnesium compounds cause diarrhea, hypocalcemia, and hypermagnesemia.
- Calcium carbonate causes milk-alkali syndrome and sodium bicarbonate produces systemic alkalosis.
- Histamine H2-receptor antagonists:
- Drugs: These include four agents namely cimetidine (400 mg BD or 800 mg at night), ranitidine (150 mg BD or 300 mg at night), famotidine (20 mg BD or 40 mg at night), and nizatidine (150 mg BD or 300 mg at night). All are equally effective.
- Mechanism of action: Inhibit acid and pepsin secretion by blocking H 2-receptors.
Duration of treatment: - Duodenal ulcer: Usually for 4 weeks. Smokers and patients with recent major complications (e.g., hematemesis, perforation), treatment is prolonged to 6–8 weeks.
- Gastric ulcer: For 6 weeks, followed by endoscopy and further treatment if necessary.
- Proton pump (H +, K+-ATPase) Inhibitors (PPIs):
- These agents are substituted benzimidazole derivatives that covalently bind and irreversibly inhibit H +, K+-ATPase.
- They include omeprazole (20 mg/d), esomeprazole (20–40 mg/d), lansoprazole (15–30 mg/d), rabeprazole (20 mg/d), and pantoprazole (40 mg/d). All have similar efficacy in the treatment of various acid-peptic disorders.
- Mechanism of action:
- Proton-pump inhibitors are lipophilic compounds that cross the parietal cell membrane and enter the acidic parietal cell canaliculus.
- Upon entering the acidic parietal cell, the PPIs are protonated, and trapped within the acid environment of the tubulovesicular and canalicular system. They become activated and bind covalently with the H +/K+ ATPase enzyme and potently inhibit all phases of gastric acid secretion by the proton pump.
- Side effects: Headache, diarrhea, abdominal pain, and nausea. The use of PPI may predispose to an increased risk of Clostridium difficile infection, community acquired pneumonia, hip fracture, and vitamin B12 deficiency.
- Advantages: Superior healing rates, shorter healing time, and faster relief of symptom compared to H 2-blockers.
- Indications:
- Indications for proton pump inhibitors (PPIs):
- GERD and reflux esophagitis
- Peptic ulcer not responding to other medical measures.
- As an adjunct to anti-H. pylori treatment.
- Zollinger-Ellison syndrome
- Cytoprotective agents:
- Sucralfate: It is a complex sucrose salt insoluble in water and becomes a viscous paste within the stomach and duodenum. It binds to sites of active ulceration. Sucralfate acts as a protective barrier, over the ulcer and increases the mucosal defense and repair. Standard dose 1 g qid.
- Bismuth-containing preparations: Colloidal bismuth subcitrate (CBS) and bismuth subsalicylate are used to induce healing of peptic ulcers. Side effects include black stools, constipation, darkening of the tongue, and neurotoxicity. They are commonly used as one of the agents in an anti-H. pylori regimen.
- Prostaglandin analogs: They enhance mucosal defense and repair and useful in preventing NSAID-induced mucosal injury. Dose (e.g., Misoprostol) is 200 µg qid.
- Treatment for H. pylori infection.
- Indications: Consensus of opinion is that all patients with proven acute or chronic duodenal ulcer and those with gastric ulcers who are H. pylori-positive should be administered drugs against H. pylori (even without documenting the presence of bacteria).
- Advantages: It reduces the risk of recurrence of ulcer.
- Type of therapy: Triple or quadruple therapy.
- Avoid: Cigarette smoking, aspirin, and NSAIDs
2. Long-term management:
1. Intermittent treatment: When the symptoms relapses < four times a year, 4 weeks course of one of the ulcer-healing agents are prescribed.
2. Maintenance treatment:
- Continuous maintenance treatment is not required after successful eradication of H. pylori.
- If symptoms relapses for more than four times per year or history of complications (e.g., repeated bleeding or perforation) require the lowest effective dose of PPI.
- Long-term maintenance is with H 2-receptor antagonists (cimetidine 400 mg at night, ranitidine 150 mg at night, famotidine 20 mg at night or nizatidine 150 mg at night).
New Treatments:
- Cholecystokinin 2 receptor antagonists (CCK2): Itriglumide
- Potassium competitive acid blockers (P-CABs): Revaprazan
3. Surgical treatment:
- Most of peptic ulcers are cured by H. pylori eradication therapy and by acid-suppressing drugs. Elective surgery is reserved for the treatment of medically refractory disease (recurrence of ulcer following surgery, gastric outlet obstruction), or urgent/emergency surgery for the treatment of an ulcer-related complication (e.g., perforation and hemorrhage).
- Indications for surgery
- Chronic non-healing gastric ulcer: Persistent ulceration despite adequate medical therapy. The procedure of choice is partial gastrectomy with a Billroth I anastomosis, in which the ulcer and the ulcer-bearing area of the stomach are resected.
- Gastric outflow obstruction
- Recurrent ulcer following gastric surgery
- Duodenal ulcer: Most commonly performed procedures are:
- Vagotomy and drainage (by pyloroplasty, gastroduodenostomy, or gastrojejunostomy)
- Highly selective vagotomy (which does not require a drainage procedure)
- Vagotomy with antrectomy
- As an emergency for complications namely perforation and hemorrhage.
Dumping Syndrome:
Question 38. Write a short note on dumping syndrome.
Answer:
- It is a series of vasomotor and GI signs and symptoms that occur when food reaches the small bowel too rapidly and usually develops in patients who have undergone vagotomy and drainage (especially Billroth procedures).
Triggering factor: It usually occurs after meals rich in simple carbohydrates (especially sucrose) and high osmolarity. Ingestion of large amounts of liquids may also contribute.
- Phases: There are two phases of dumping namely early and late.
1. Early dumping:
- Time of occurrence: Occurs 15–30 minutes after meals.
- Signs and symptoms: Consists of crampy abdominal discomfort, nausea, diarrhea, belching (bloating), borborygmi, tachycardia, palpitations, diaphoresis, light-headedness, and, rarely, syncope.
- Mechanism: The signs and symptoms are due rapid emptying of hypertonic gastric contents into the small intestine that draws the fluid into lumen of the gut and leads to distension of small intestine. This leads to reduced volume of plasma and acute intestinal distention. Release of vasoactive GI hormones (vasoactive intestinal polypeptide, neurotensin, and motilin) may also play a role.
2. Late phase of dumping:
- Time of occurrence: Occurs 90 minutes to 3 hours after meals.
- Signs and symptoms: Consists of vasomotor symptoms such as light-headedness, diaphoresis/sweating, palpitations, tachycardia, and occasionally syncope.
- Mechanism: Possibly secondary to hypoglycemia from excessive insulin release.
Provocative Test:
- After an overnight fast, a solution of 50–75 g glucose given orally.
- Measure blood glucose, hematocrit, pulse rate, and blood pressure at 30 minutes intervals, immediately before and up to 180 minutes after ingestion of glucose.
- Positive test: Characterized by an early (30 minutes) increase in pulse rate (>10/minutes) or hematocrit >3% and late (120–180 minutes) hypoglycemia.
Dumping Syndrome Treatment:
- Patient should be asked have small, multiple (six) meals and avoid simple carbohydrates and liquids during meals.
- Antidiarrheals and anticholinergic drugs are complementary to diet.
- Guar and pectin: They increase the viscosity of intraluminal food contents, thereby slowing down gastric emptying.
- Acarbose: It is an α-glucosidase inhibitor that delays digestion of ingested carbohydrates. It appears beneficial in the treatment of the late phases of dumping.
- Octreotide: It is a somatostatin analog given subcutaneously (50 g tid), before the meal may be used in diet-refractory cases. A long-acting octreotide may be given once every 28 days.
Diseases Of The Intestine:
Malabsorption Syndrome:
Question 39. Discuss the classification, etiology, clinical features, investigations (diagnosis), and management of malabsorption syndrome.
(or)
List the investigation of a case of steatorrhea.
Answer:
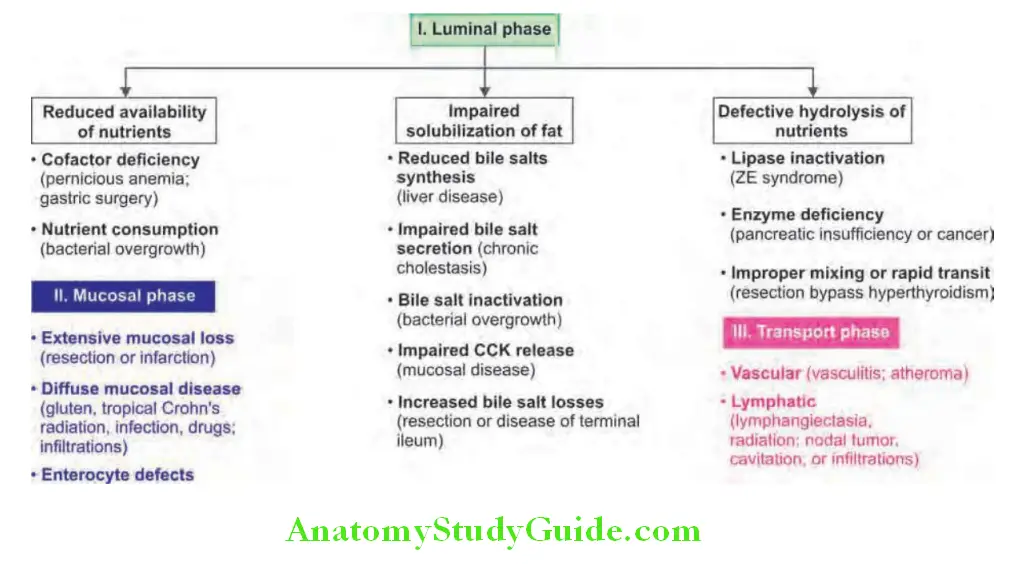
Diseases Of The Intestine Definition: Malabsorption is defined as defective/diminished intestinal absorption of one or more dietary nutrients.
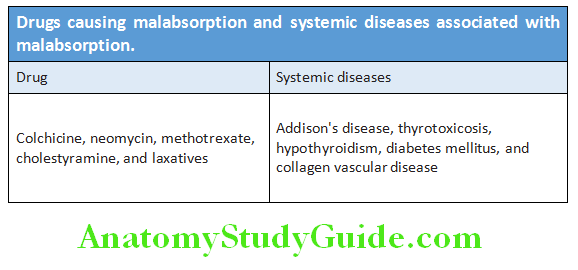
Diseases Of The Intestine Classifiation and Etiology:
Drugs causing malabsorption and systemic diseases associated with malabsorption are presented in Table.
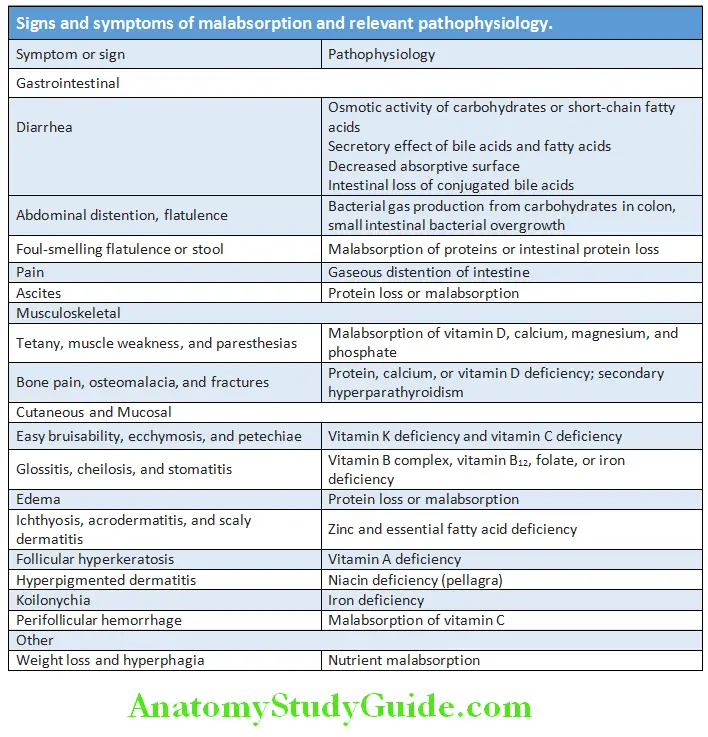
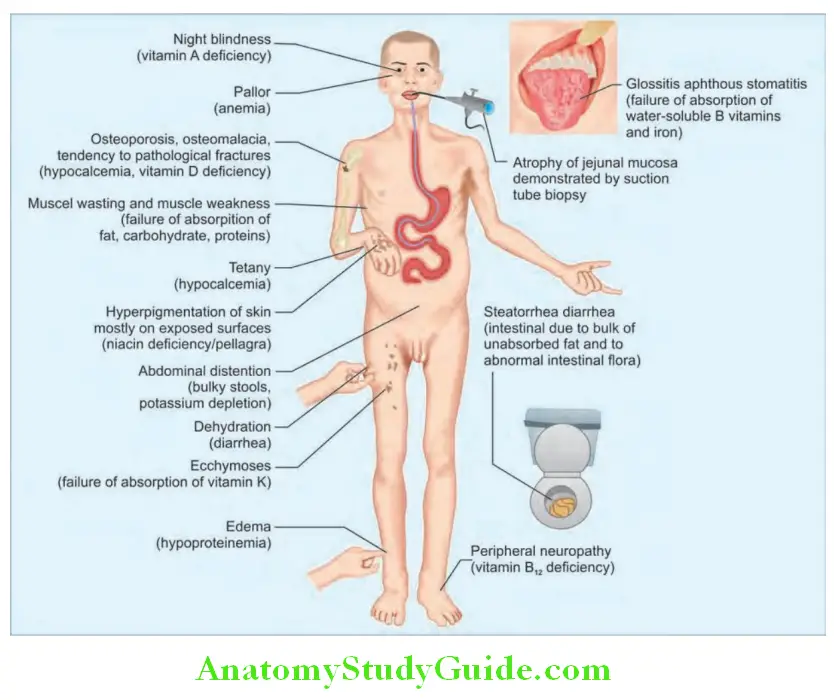
Diseases Of The Intestine Clinical Features:
- Onset: Insidious and gradually progresses.
- General features: Diarrhea, abdominal pain, distension, loss of weight, and anemia.
- Symptoms and signs and relevant pathophysiology are presented.
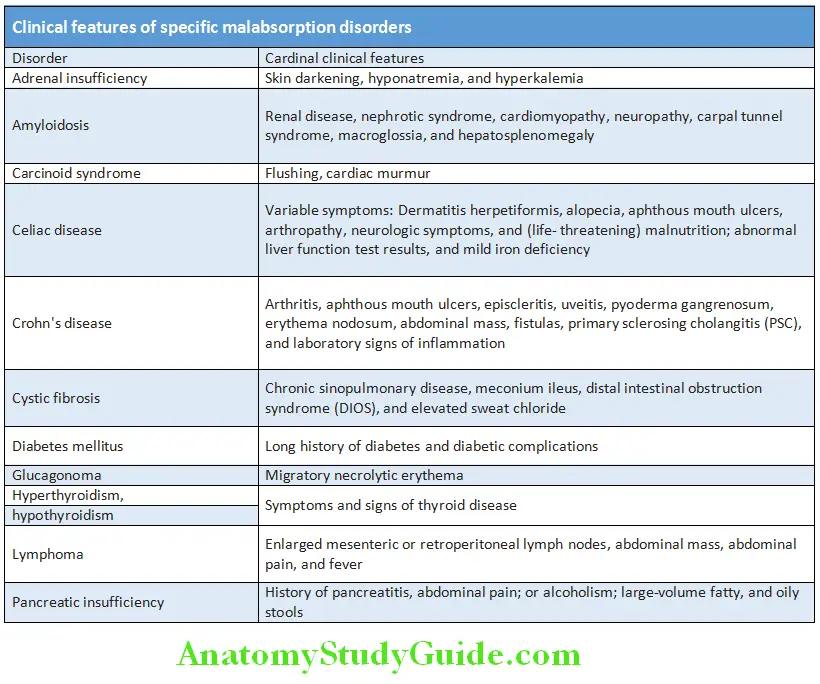
Question 40. Discuss the chronic effects of diarrhea including malabsorption.
Answer:
Clinical features of specific malabsorption disorders are presented in Table:
Malabsorption Investigations:
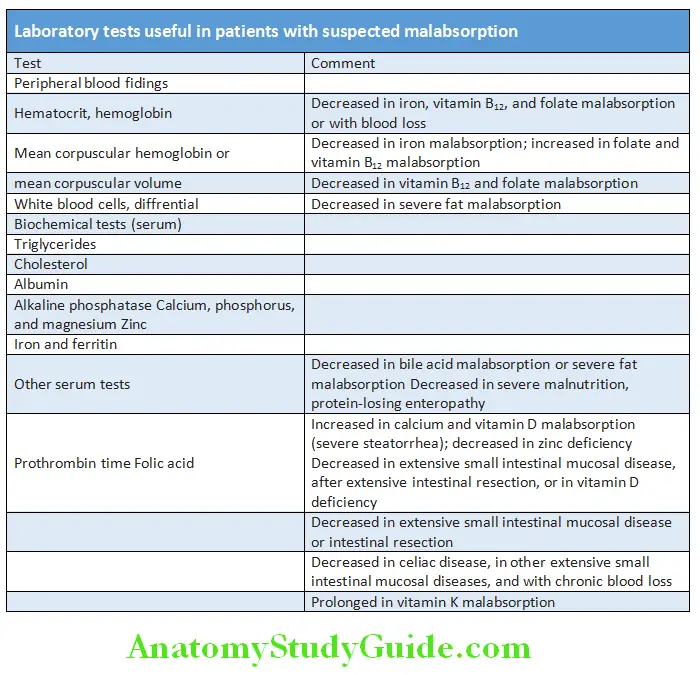
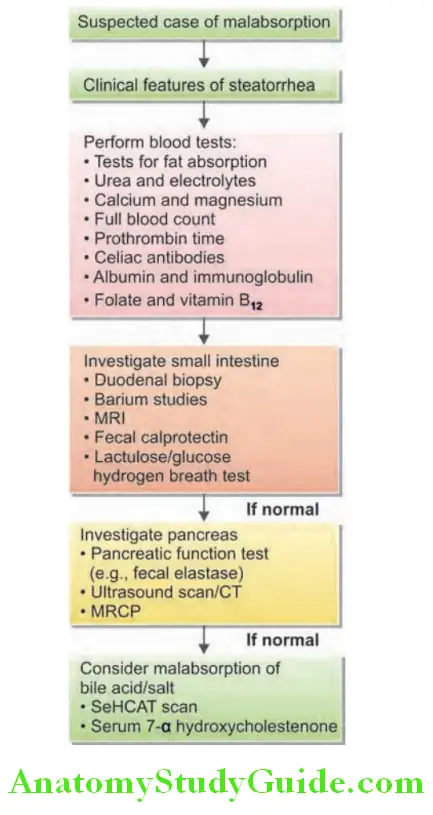
Tests for fat absorption:
Quantitative test:
- 72-hour-stool fat collection: Gold standard
- 6 g/day: Pathologic, patients with steatorrhea >20 g/day.
Qualitative tests:
- Sudan III stain for fat globules in stool: Detect clinically significant steatorrhea in >90% of cases. Acid steatocrit: A gravimetric assay. Sensitivity
- 100%, specificity—95%, PPV—90%
- NIRA (near infrareflectance analysis): Equally accurate with 72 hours stool fat test. Allows simultaneous measurement of fecal fat, nitrogen, and CHO (carbohydrate)
- Measurement of blood levels of fat-soluble vitamins (A, D, E, and K); prothrombin time.
- Plasma vitamin A level after 2–3 days of oral retinol: It will be lower than normal.
Tests for carbohydrate absorption:
- Glucose tolerance test: It reveals absence of rise in blood glucose levels.
- Blood sugar level: Low
- D-xylose absorption test: D-xylose is a pentose monosaccharide absorbed exclusively at the proximal small intestine. This test is used to assess proximal small intestine mucosal function. The procedure is as follows:
- After overnight fast, administer 25 g D-xylose perorally.
- Urine collected for next 5 hours and urinary excretion of D-xylose is estimated.
- Abnormal test: <4.5 g is abnormal and suggest intestinal malabsorption (duodenal/jejunal mucosal disorders) and excludes pancreatic cause.
- Lactose tolerance test (LTT):
- Orally 50 g of lactose is given.
- Blood glucose levels measured at 0, 60, and 120 minutes.
- Normally, blood glucose shows a rise of >20 mg/dL.
- Blood glucose <20 mg/L + development of symptoms favor diagnosis.
- Hydrogen breath test: It is used for the diagnosis of lactase deficiency. 50 g lactose given orally and breath hydrogen measured every hour for 4 hours. Normal value is <10 ppm increase above baseline.
Tests for protein absorption:
- Serum albumin: Low
- Nitrogen in the 24-hour stool: >2.5 g.
- α1-Antitrypsin content in stool: Normally no antitrypsin in stool. A 3 days collection of stools is estimated for α 1-antitrypsin content.
Test for bile acid malabsorption:
- Selenium-homocholic acid taurine (SeHCAT) test: In this test, Se-labeled bile acid is given orally. After 7 days, total body retention is measured with a gamma camera.
- Retention value of <10% is abnormal.
Tests for absorption of other substances:
- Serum B12 level: Reduced
- Schilling test for absorption of B12: To determine the cause of cobalamin (B12) malabsorption.
Test for bacterial overgrowth:
- Quantitative bacterial count from aspiration from small intestine. Normal count is <10 U/mL (jejunum), >10 U/mL (ileum).
- Breath tests: Cholyl-14 C-glycine, e.g., bacterial overgrowth. Lactose H2 for lactose intolerance, e.g., in bacterial overgrowth.
- Small intestinal biopsy (duodenal or jejunal): Lesions seen can be classified into three:
- Diffese and specifi, e.g., Whipple’s disease
- Patchy and specific, e.g., Crohn’s disease, lymphoma, and infectious causes
- Diffese and nonspecific, e.g., celiac sprue, tropical sprue, and autoimmune enteropathy
Barium studies: Important information about the gross anatomy and morphology of small intestine.
Treatment of Malabsorption Syndrome:
- General measures:
- Dehydration and electrolyte deficiency is treated by intravenous infusion
- Replacement therapy for anemia, bone disease and coagulation defects. Vitamin D, B complex, and calcium supplements
- Specific therapy depending on the cause:
- Celiac disease: Gluten-free diet
- Pancreatic insufficiency: Pancreatic supplements
- Bile acid deficiency/malabsorption: Low-fat diet and cholestyramine (bile acid binder)
Celiac Disease:
Question 41. Write short essay/note on celiac disease (nontropical sprue/gluten-induced enteropathy).
Answer:
Celiac Disease Defiition:
Celiac disease is characterized by small intestinal malabsorption of nutrients after the ingestion of wheat gluten or related proteins from rye and barley, villus atrophy of the small intestinal mucosa, prompt clinical and histologic improvement following strict adherence to a gluten-free diet, and clinical and histologic relapse when gluten is reintroduced.
Celiac Disease Etiology:
Exact etiology is not known, but environmental, immunologic, and genetic factors play important role.
- Environmental factor: Gluten is the protein present in the cereals wheat, barley and rye. Gliadin is a component of gluten. There is a clear cut association of the celiac disease with gliadin. Gluten restriction results in morphologic changes within hours in patient with celiac disease.
- Immunologic factor: It involves both adaptive and innate immune responses. Presence of serum antibodies such as IgA antigliadin, IgA antiendomysial (90–95% sensitivity and specificity), and IgA anti-tTG antibodies in patients with celiac disease. It is not known whether they represent primary or secondary to the tissue damage.
- Genetic factor(s): Increased incidence of celiac disease is observed within families but the exact mode of inheritance is unknown. All patients express the HLA-DQ2 or HLA-DQ8 allele.
Celiac Disease Pathology:
- Site of lesion: Biopsy from the second portion of the duodenum or proximal jejunum (which are exposed to the highest concentrations of dietary gluten) is diagnostic.
- Microscopic changes: Characterized by increased numbers of intraepithelial CD8+ T lymphocytes (intraepithelial lymphocytosis), crypt hyperplasia, and villous atrophy. Increased numbers ofplasma cells, mast cells, and eosinophils within the upper part of the lamina propria.
Celiac Disease Clinical Features:
Age and gender: It can manifest at any age. Usually manifests early in childhood at about 2 years of age (after wheat is introduced into the diet), or later in the second to fourth decades of life with a female preponderance.
Celiac Disease Symptoms: Many patients are asymptomatic (silent). The symptoms are very variable and often nonspecific.
- Symptoms due to malabsorption of multiple nutrients, with diarrhea, steatorrhea, weight loss, and the consequences of nutrient depletion (i.e., anemia and metabolic bone disease).
- Symptoms due to the depletion of a single nutrient (e.g., iron or folate deficiency or vitamin B12 deficiency, osteomalacia, edema from protein loss, and tetany).
Associated diseases:
Diseases associated with celiac disease:
- Insulin-dependent diabetes mellitus (2–8%)
- Thyroid disease (5%)
- Primary biliary cirrhosis (3%)
- Sjögren’s syndrome (3%)
- IgA deficiency (2%)
- Pernicious anemia
Associated diseases Complications:
Complications of celiac disease:
- Gastrointestinal malignancies: An increased incidence of both gastrointestinal (e.g., carcinoma of the esophagus) and nongastrointestinal neoplasms as well as enteropathy associated T cell lymphoma (EATCL)
- Development of intestinal ulceration independent of lymphoma (ulcerative jejunitis ), refractory sprue, and collagenous sprue
- Nonresponsive celiac disease: Few patients do not improve on a strict diet
- Refractory celiac disease (RCD)
- Pneumococcal infections
- Dermatitis herpetiformis
- Osteomalacia
Treatment/Management of Celiac Disease:
- Diet: Lifelong gluten-free diet. Avoid wheat, rye, and barley. Oats not contaminated with flour are tolerated by most patients. Rice, meat, dairy products, vegetables, and fruits are safe. Completely avoid beer and whisky obtained from malt distillation procedures.
- Lactose-free diet is advisable because of secondary lactase deficiency associated with celiac disease
- Supplementation of vitamins and minerals in cases patients with these deficiencies, folic acid supplements for women of childbearing age
- Pneumococcal vaccinations (because of splenic atrophy) once in every 5 years
- Corticosteroids: They are rarely required. Used in critically ill patients who present with acute celiac crisis characterized by severe diarrhea, dehydration, weight loss, acidosis, hypocalcemia, and hypoproteinemia. May be used in gliadin shock after a gluten challenge
Serologic tests in celiac disease:
Serologic tests:
- IgA antiendomysial antibody
- IgA antitissue transglutaminase antibody (anti-tTG)
- IgA antigliadin antibody
- IgG antigliadin antibody
Tropical Sprue:
Question 42. Write short essay on tropical sprue (idiopathic tropical malabsorption syndrome).
Answer:
Tropical Sprue Definition: Tropical sprue is a condition presenting with chronic diarrhea and malabsorption (of two or more substances) that occurs in residents or travelers to certain, but not all tropical areas (especially India and Southeast Asia) in the absence of other intestinal diseases or parasites.
Tropical Sprue Etiology:
- Etiology and pathogenesis of tropical sprue are unknown.
- Role of infectious agents: Because tropical sprue responds to antibiotics, it is possible that it may be caused by one or more infectious agents (e.g., Klebsiella pneumoniae, Enterobacter cloacae, or E. coli) or a toxin produced by these agents.
- Role of folic acid deficiency: Folic acid is absorbed in the duodenum and proximal jejunum, and most patients with tropical sprue show evidence of folate malabsorption and depletion.
Tropical Sprue Clinical Features:
- Clinical features vary in different parts of the world.
- Intensity: Vary and consist of diarrhea, anorexia, abdominal distension fatigue, and weight loss.
- Onset:
- Acute: Sometimes acute with sudden severe diarrhea and accompanied by fever. It occurs either a few days or many years after being in the tropics.
- Chronic phase: Onset may also be insidious, with chronic diarrhea and evidence of nutritional deficiency. Features of megaloblastic anemia (folic acid malabsorption) and other deficiencies, including ankle edema, glossitis, and stomatitis, are common. Remissions and relapses may occur.
Treatment of Tropical Sprue:
- Broad-spectrum antibiotics: Tetracycline or oxytetracycline 1 g daily in four divided doses for up to 6 months and produces improvement within 1–2 weeks
- Folic acid: A dose of 5 mg daily along with tetracycline is most often curative. It induces a hematologic remission and improvement in appetite, weight gain, and also morphological changes in small intestinal biopsy
- Correction of deficiencies: Severely ill patients require resuscitation with fluids and electrolytes for dehydration. Nutritional deficiencies should be corrected such as vitamin B (1,000 μg)
- Symptomatic treatment for diarrhea
- Prognosis: Excellent. Mortality is usually due to water and electrolyte depletion
Diagnosis and Investigations:
- Abnormal jejunal mucosal biopsy: It shows partial villous atrophy and mononuclear cell infiltrate in the lamina propria.
- The lesion is less severe than that of celiac disease.
- Stool examination
- Demonstration of malabsorption
Lactose Intolerance:
Question 43. Write a short note on lactose intolerance.
Answer:
Lactose Intolerance Etiology:
- Lactose is the disaccharide present in milk and it is digested to monosaccharides (glucose and galactose) by the brush border lactase.
- Classification: There are two types of lactase deficiency namely primary and secondary.
- Primary lactase deficiency: It is due to genetic deficiency or absence of lactase and both intestinal absorption and brush border enzymes are normal.
- Secondary lactase deficiency: It occurs in association with both structural and functional disorders of brush border enzymes and transport processes, e.g., celiac disease, tropical sprue, and Crohn’s disease.
- Lactose intolerance develops due to the deficiency of lactase and lactose present in the milk cannot be hydrolyzed. Hence, lactose gets fermented by bacteria causing gastrointestinal symptoms.
Lactose Intolerance Clinical Features:
- Diarrhea, abdominal pain, cramps, and/or flatus develops after ingesting milk or milk products.
- Symptoms improve on withdrawal of milk or milk products.
Lactose Intolerance Investigations:
- Hydrogen breath test: This is used as a screening test to measure transit time and detect bacterial overgrowth in the small intestine. Appearance of breath hydrogen peak after
- Measurement of lactase activity in a jejunal biopsy.
Lactose Intolerance Treatment:
Lactose free diet. Avoid milk and dairy products. However, it may lead to nutritional deficiencies, particularly calcium deficiency.
Administration of exogenous β-galactosidase:
- Enzyme replacement therapy with microbial exogenous lactase (obtained from yeasts or fungi)
- Enzymes supplement to milk and dairy products
- Use of yogurt and probiotics (source of β-g oral lactulose indicates that the undigested lactose is fermented by the colonic microflora and produces hydrogen which can be detected in expired air.
Whipple’s Disease:
Question 44. Write short note on Whipple’s disease and its important clinical features.
Answer:
Whipple’s disease is a chronic, rare, multisystemic infectious bacterial disease caused by Tropheryma whipplei (grampositive).
Whipple’s Disease Clinical Features:
- Gender: More common in males than in females.
- Whipple’s disease is a chronic multisystem disease associated with diarrhea, steatorrhea, weight loss, arthralgia, and central nervous system (CNS) and cardiac problems.
- Migratory arthralgias of the large joints
- Dementia and other CNS findings (such as supranuclear ophthalmoplegia, nystagmus, and myoclonus)
- Cardiac disease (dyspnea, pericarditis, and culture-negative endocarditis)
- Pleuropulmonary (pleural effusion)
Whipple’s Disease Investigations:
Biopsy: Jejunal biopsy and biopsy of other involved tissues show numerous PAS—positive macrophages with small bacilli. In the small intestine, these macrophages produce lymphatic blockade in the lamina propria causing malabsorption.
Treatment: Trimethoprim-sulfamethoxazole (double strength tablet): Dose twice a day for 1 year. This should be preceded by a 2-week course of parenteral therapy with ceftriaxone (2 g daily) or by meropenem.
Giardiasis:
Question 45. Write short essay/note on clinical features, diagnosis, and treatment of Giardiasis.
Answer:
- Giardiasis is an infection caused by flagellate Giardia lamblia (Giardia intestinalis).
- Giardiasis is found worldwide and is one of the most common parasitic diseases in both developed and developing countries, causing intestinal disease, and diarrhea.
- It mainly affects children, tourists and immunosuppressed individuals (agammaglobulinemia).
- Incubation period: 1–3 weeks
- Mode of infection: By ingesting contaminated water. In cystic form, it is viable in water for up to 3 months.
- Malabsorption may develop due to loss of brush–border enzyme activities and few patients may show flattering of villi.
Giardiasis Clinical Features:
- Range from asymptomatic carrier stage to fulminant diarrhea and malabsorption.
- After ingestion of flagellar trophozoite form, it attaches to the mucosa of duodenum and jejunum and causes inflammation. It produces disease of small intestine.
- Acute giardiasis: Starts as diarrhea, abdominal pain, nausea, vomiting, anorexia, belching, flatus, weakness, and abdominal pain. Fever and blood in stool are rare. The duration is usually >1 week.
- Chronic giardiasis: May present with or without having experienced antecedent acute episode. Diarrhea may not be a prominent symptom and they may have increased flatus, and loose stools. It may produce steatorrhea; malabsorption if illness is prolonged may result in marked weight loss. Symptoms may be continuous or episodic and can persist for years.
- Chronic giardiasis in children from developing countries may develop retardation of growth.
- Severe disease: Giardiasis may be severe in patients with hypogammaglobulinemia, resulting in malabsorption, weight loss, growth retardation, and dehydration.
- Physical examination may reveal abdominal distension and tenderness.
- Extraintestinal manifestations: These include urticaria, anterior uveitis, and arthritis.
Treatment/Management:
- Tinidazole 40 mg/kg (2 g/day) once by mouth and repeated after 1 week
- Metronidazole 2 g daily for 3 days or metronidazole 200 mg thrice daily for 5–7 days is usually curative in >90% of cases
- Nitazoxanide 500 mg twice a day for 3 days. Other drugs include mepacrine and albendazole
- Paromomycin is an oral aminoglycoside and is not well absorbed. It can be given to symptomatic pregnant patients
- Refractory cases: Prolonged therapy with metronidazole 800 mg thrice daily for 3 weeks
Giardiasis Investigations/Diagnosis:
- Stool examination: Demonstration of protozoal parasite
- Duodenal or jejunal aspiration by endoscopy or with a luminal capsule gives a higher diagnostic yield.
- String test: In this one, end of a piece of string is passed into the duodenum by swallowing and retrieved after an overnight fast. The fluid is expressed from this and examined for the presence of G. lamblia trophozoites.
- Biopsy: Biopsy and histological examination of jejunal mucosa may show G. lamblia on the epithelial surface.
- Stool antigen detection tests: Detection of parasite antigens in the feces is sensitive and specific and easier to perform.
- Other tests: Chronic cases may show steatorrhea, malabsorption of xylose, and vitamin B12 and lactose intolerance.
Carcinoid Tumors (Neuroendocrine Tumors):
Question 46. Write short note on carcinoid tumors (neuroendocrine tumors) and carcinoid syndrome.
Answer:
- Neuroendocrine cells are amine- and acid-producing cells located throughout the body.
- Neuroendocrine tumors (NETs) are tumors derived from the diffuse neuroendocrine system of the GI tract.
- Location of carcinoid tumors: Appendix (25%), small intestine (25%), and rectum (15%). Stomach (5%) and lung (15% of all carcinoid tumors).
Classifiation of Carcinoid Tumors:
According to their anatomic area of origin:
- Foregut (lungs, bronchi, and stomach)
- Midgut (small intestine, appendix, and proximal large bowel
- Hindgut (distal large bowel, rectum).
Ultrastructurally, they possess electron-dense neurosecretory granules which may contain various substances.
These include: 5-hydroxytryptamine (serotonin), histamine, tachykinins, motilin, prostaglandins, bradykinins, adrenocorticotropic hormone, and corticotropin-releasing factor.
Carcinoid Syndrome:
It is symptom complex in which systemic symptoms are produced when the vasoactive substances are secreted by carcinoid tumors into the systemic circulation. Carcinoid syndrome occurs in only 8–10% of patients.
- Midgut carcinoids (usually ileal carcinoid) with hepatic metastasis can produce carcinoid syndrome. Because, normally liver is able to metabolize these secretory products into inactive forms and with hepatic metastasis the product can reach systemic circulation.
- Foregut (bronchial and extraintestinal) carcinoids can present with carcinoid syndrome without hepatic metastases.
- This is because bioactive products can bypass liver and can be released directly into systemic circulation.
- Hindgut carcinoids seldom produce syndrome since they do not secrete these products.
- Intestinal carcinoids have an increased tendency for liver metastasis.
Carcinoid Tumors Clinical Features:
Characterized by cutaneous flushing, involving head and neck (blush area) associated with lacrimation, sweating, bronchospasm, colicky abdominal pain, diarrhea, and right-sided cardiac valvular fibrosis.
Carcinoid Tumors Diagnosis:
Diagnosed by measuring urinary or plasma serotonin or its metabolites in the urine.
- Measurement of 5–hydroxyindoleacetic acid (5-HIAA): Increased (>9 mg) urinary excretion in 24-hour sample collection.
- Serum chromogranin A levels are elevated in 56–100% of patients.
- Serotonin level in blood and platelets is high, because it is overproduced in 92% of patients.
- Plasma neuron-specific enolase levels are increased but are less sensitive than chromogranin A.
- Others: CT, MRI, and somatostatin receptor scintigraphy, PET (positron emission tomography) with radiolabeled 5-hydroxytryptophan may be helpful.
Carcinoid Tumors Treatment:
- Avoid conditions and diets that precipitate flushing and diarrhea
- Supplementation of diet with nicotinamide
- Wheezing is treated with oral bronchodilators
- Treatment of heart failure with diuretics
- Control of the diarrhea with antidiarrheal agents (e.g., loperamide and diphenoxylate). If not controlled advise serotonin receptor antagonists (cyproheptadine, methysergide, and ondansetron) to control diarrhea
- Analogs of somatostatin (e.g., octreotide and lanreotide) to control flushing
- Surgical resection of the carcinoid tumor
- Excision of liver metastases or hepatic artery embolization with or without chemotherapy
Ischemic Colitis:
Question 47. Write short note on ischemic colitis.
Answer:
Ischemic Colitis Etiology:
- Transient nonocclusive hypoperfusion of a segment of the colon, e.g., systemic hypoperfusion
- Occlusion of the inferior mesenteric artery or its branches, e.g., atherosclerotic or thrombotic occlusion
- Less common causes, e.g., hypercoagulable states (in young persons), iatrogenic ligation of the inferior mesenteric artery (e.g., with aortic surgery), embolism, vasculitis, and colonic obstruction (e.g., colonic cancer).
- Drugs and chemicals: Medications, illicit drugs, and chemicals may also produce chemical picture identical or similar to ischemic colitis (e.g., digitalis, vasopressin, pseudoephedrine, amphetamines, cocaine, estrogens, ergot alosetron, etc.).
Ischemic Colitis Clinical Features:
- Age: Occur in persons older than 60 years without any apparent cause.
- Onset: Many cases are acute and self-limited.
- Symptoms: Colicky lower abdominal pain (mostly left lower quadrant), diarrhea, and passage of bright red blood per rectum, nausea, and vomiting. Though the blood loss is not usually enough to require transfusion, some patients may progress to shock because of loss of blood and fluid.
- Physical examination: Abdominal tenderness and guarding over the affected portion of the colon (especially left iliac fossa), and abdominal distention fever and tachycardia.
Laboratory Findings/Investigation:
- Nonspecific findings such as leukocytosis and hemoconcentration
- Plain radiographs of the abdomen: It may show “thumbprinting” at splenic flexure and descending colon or may be normal.
- Computed tomography (CT) scanning of abdomen: Useful to exclude other disorders.
- Double contrast barium enema demonstrates involvement of splenic flexure and descending colon. Mucosal abnormalities are thumbprinting and ulceration.
- Colonoscopy has replaced barium studies as it is more sensitive. Sigmoidoscopy shows normal rectal mucosa and bleeding descending from above.
- Arteriography confirms the diagnosis in patients with obstructive lesions.
Ischemic Colitis Treatment:
- For right-sided ischemic colitis: It requires visceral angiography which is needed for both diagnosis and intra-arterial administration of vasodilators (e.g., papaverine as a 60-mg intravenous bolus followed by an infusion of 30–60 mg/hour). Some patients may need urgent surgery
- Left-sided acute ischemic colitis: It accounts for most cases and most cases resolve within hours to a few days with supportive therapy.
- Therapy includes volume replacement, correction of any low-flow state, broad-spectrum antibiotics (similar to those recommended earlier for patients with small bowel ischemia), avoidance of vasoconstrictive medications, and rarely, blood transfusion. Surgery is required only in patients with signs and symptoms of transmural necrosis, perforation, or massive bleeding
- Conservative management: Intravenous fluids, hemodynamic stabilization, discontinuation or avoidance of vasoconstrictive agents, bowel rest, and empiric antibiotics
- Surgical treatment: Peritonitis and strictures
Pseudomembranous Colitis:
Question 48. Write short note on pseudomembranous colitis (antibiotic-associated colitis).
Answer:
Pseudomembranous colitis also referred to as antibiotic-associated colitis or antibiotic-associated diarrhea, generally caused due to toxin produced by Clostridium difficile, when the normal bacterial flora is altered or suppressed by antibiotics.
- Antibiotic-associated diarrhea may also be caused by other organisms such as Salmonella, C. perfringens type A, or Staphylococcus aureus but only C. difficile causes pseudomembranous colitis.
- In the colon, the vegetative form of C. difficile multiplies and produces two major toxins namely toxin A (an enterotoxin) and toxin B (a cytotoxin).
Pseudomembranous Colitis Clinical Features:
- Age: Pseudomembranous colitis usually develops in adults and about 80% of cases occur in people over 65 years of age.
- Patient is on antibiotics or has received antibiotics within last 8 weeks. Clinical symptoms range from asymptomatic to severe and sometimes life-threatening fulminant pseudomembranous colitis.
- Diarrhea: It is the most common manifestation.
- Stool: Soft and unformed to watery or mucoid in consistency and has a characteristic odor. Stools are almost never grossly bloody.
- Frequency: Patients may have as many as 20 bowel movements/day.
- Profuse watery diarrhea with abdominal cramps
- Substantial fluid and protein losses combined with fever, cramps, hypoalbuminemia, leukocytosis, and hypotension.
- Laboratory findings: Leukocytosis is common (observed in up to 50% of patients) and is a marker of severe disease. Leukocytosis often >15,000/mm3 white blood cells (WBCs)/L. Extremely high level (>50,000/mm3 indicates fulminant and potentially fatal illness.
- Complications: Dehydration, electrolyte disturbances, hypoalbuminemia, toxic megacolon, bowel perforation, hypotension, renal failure, hypotension, lactic acidosis sepsis, and death.
Pseudomembranous Colitis Investigations and Diagnosis:
- Enzyme immunoassay for C. difficile glutamate dehydrogenase
- Enzyme immunoassay for C. difficile toxins A and B
- Real-time PCR tests detect the critical gene is tcdB.
- Stool culture for C. difficile
- Sigmoidoscopy or colonoscopy: Endoscopy is a rapid diagnostic tool in seriously ill patients and characteristically shows erythema, white plaques or an adherent pseudomembrane. Biopsy can be done.
Pseudomembranous Colitis Treatment/Management:
Treatment consists of:
- Discontinuation Of The Implicated Antibiotic
- Supportive Care
- Avoidance of antiperistaltic agents and opiates
- Withdraw/discontinue the precipitating antibiotic/antimicrobial drug and isolate the patient
- Supportive care: Oral or intravenous rehydration
- Mild-to-moderate cases: Oral metronidazole 500 mg thrice daily for 10–14 days. Rifaximin can be added
- Severe cases: Oral vancomycin 125 mg 6 hourly for 14 days
- Severe complicated or fulminant cases: Vancomycin (500 mg orally or via nasogastric tube) plus intravenous metronidazole (500 mg q8h) plus consider rectal instillation of vancomycin (500 mg in 100 mL of normal saline as a retention enema q6–8h).
- Intravenous vancomycin not effective. Newer drug fidaxomicin (200 mg twice daily) is as efficacious as vancomycin. If ileus develops vancomycin administered by enema
- Oral probiotic therapy: Use of live nonpathogenic bacteria to re-establish the gut flora often used in resistant or relapsed cases. Probiotics use organisms resistant to gastric acid. However, its clinical benefits are not proved
- Avoidance of antiperistaltic agents and opiates: Antiperistaltic drugs such as loperamide or diphenoxylate should not be administered because they can precipitate toxic megacolon
- Colectomy may be necessary in severely ill and refractory cases
- Newer treatment modalities: Fecal microbiota transplantation (fecal enemas or infusion of donor feces through a nasoduodenal tube)
Psychosomatic Disorders of the Gastrointestinal Tract:
Pseudomembranous Colitis Classifiation:
Irritable Bowel Syndrome:
Question 49. Write short essay/note on irritable bowel syndrome, its clinical features and management.
Answer:
Irritable Bowel Syndrome Definition:
- Irritable bowel syndrome (IBS) is a functional disorder of the gastrointestinal tract characterized by abdominal pain or discomfort and altered bowel habits in the absence of detectable structural, infective or biochemical abnormalities.
- Irritable bowel syndrome is benign, chronic symptom complex of altered bowel habits, and abdominal pain.
Pathophysiology:
Exact cause not known and pathogenesis of IBS is poorly understood. However, the following factors have been proposed.
Gastrointestinal motor abnormalities: GI motility is quantitatively different in 25–75% of IBS patients compared with healthy controls.
- Patients with diarrhea as a predominant symptom exhibit rapid jejunal contraction waves, rapid intestinal transit, an increased number of colonic contractions (colonic transit is accelerated), and rectosigmoid motor activity.
- Patients with predominant constipation have decreased orocecal transit and a reduced number of colonic contraction waves.
Visceral hypersensitivity: IBS is associated with increased sensory responses to visceral stimulation induced by intestinal distension. The mechanism for visceral hypersensitivity is not known. This is more common in females and in diarrheapredominant IBS.
Central neural dysregulation: There is a clinical association of emotional disorders and stress with symptom exacerbation in IBS. MRI has shown that in response to distal colonic stimulation, the mid-cingulate cortex (brain region concerned with attention processes and response selection) shows greater activation in IBS patients. This cerebral dysfunction may lead to the increased perception of visceral pain.
Abnormal psychological features: Abnormal psychiatric features are found in up to 80% of IBS patients. These include anxiety, tension, depression, excessive worry, somatization, and neurosis. Altered intestinal flora: Bacterial overgrowth (shown by positive lactulose hydrogen breath test) in the small bowel has been observed in IBS patients and may contribute to symptoms.
Abnormal serotonin pathways: Serotonin is a neurotransmitter that plays an important role in the regulation of GI motility and visceral perception.
Post-infectious IBS: IBS may be induced by initial GI infection by Campylobacter, Salmonella, and Shigella.
Immune activation and mucosal inflammation: Certain diet/foods may precipitate an attack.
Irritable Bowel Syndrome Clinical Features:
- Age: IBS affects all ages. Most patients present before age 45 (20–40 years).
- Gender: More common in women compared to men (3:1).
- Abdominal pain is the most common key symptom (prerequisite clinical feature) for the diagnosis of IBS. Characteristics of pain:
- Location: Pain is most typically referred to the lower abdomen (left or right iliac fossa) or hypogastrium.
- Aggravation: Pain may be aggravated by emotional stress or poor sleep, and intake of food.
- Relief: Abdominal symptoms are relieved by defecation or passage of flatus, but this relief may be temporary.
- Altered bowel habits: Most consistent clinical feature in IBS. Bowel pattern subtypes/variants are.
- Irritable bowel syndrome-constipation predominant (IBS-C): Patient reports that abnormal bowel movements are usually constipation (>25% Bristol stool types 1 or 2; <25% Bristol stool types 6 or 7).
- Irritable bowel syndrome-diarrhea predominant (IBS-D): Patient reports that abnormal bowel movements are usually diarrhea (>25% Bristol stool types 6 or 7; <25% Bristol stool types 1 or 2).
- Mixed IBS (IBS-M): They have features of alternating diarrhea and constipation (>25% Bristol stool types 1 or 2; >25% Bristol stool types 6 or 7).
- Irritable bowel syndrome-unclassified (IBS-U) includes those patients who meet the diagnostic criteria for IBS but cannot be accurately categorized into one of the other three subtypes.
Most common alteration in the bowel habit is constipation alternating with diarrhea.
- Diarrhea: Frequent defecation, often painless, but produce low-volume stools and rare/never at night. Diarrhea usually consists of small volumes of loose stools. Sense of incomplete evacuation, leading to repeated attempts at defecation in a short time span.
- Constipation: Pass infrequent pellet-like (ribbon-like or pencil-like) stools usually in association with abdominal pain or proctalgia.
- Stools: Usually hard with narrowed caliber. May be accompanied by passage of large amounts of mucus.
- Gas and flatulence: Abdominal distention and increased belching or flatulence more common among female patients. Postprandial tenesmus is common and is due to an exaggerated gastrocolic reflex.
- Other symptoms: Dyspepsia, heartburn, nausea, and vomiting
- Extraintestinal symptoms: Headache, back pain, fatigue myalgia, dyspareunia, and urinary frequency are often observed.
- Physical examination: Usually unremarkable, except for abdominal tenderness (most often in the left lower quadrant) or a tender, palpable sigmoid colon. In IBS-C, rectal examination may show paradoxical contraction of the puborectalis muscle or decreased descent of the pelvic floor when simulating a bowel movement.
Irritable Bowel Syndrome Investigations:
Aim of investigations is to exclude organic gastrointestinal diseases.
- Full blood count
- Stool examination: For parasites, ova, leukocytes, and occult blood.
- Sigmoidoscopy: Usually normal. There may be difficulty in negotiating rectosigmoid curve due to spasm. There may be marked motor activity of bowel and may show abundant mucus.
- Colonoscopy: Should be performed to exclude colorectal cancer, in older patients and those with history of rectal bleeding.
- Barium enema: Usually normal but may show spasticity of sigmoid, exaggerated haustral markings and a tubular appearance of the descending colon.
- In diarrhea-predominant patients investigations to exclude microscopic colitis, lactose intolerance, bile acid malabsorption, celiac disease, and thyrotoxicosis.
Diagnostic Criteria:
Rome IV diagnostic criteria for irritable bowel syndrome are presented in Table.
Red flag signs of IBS are presented.
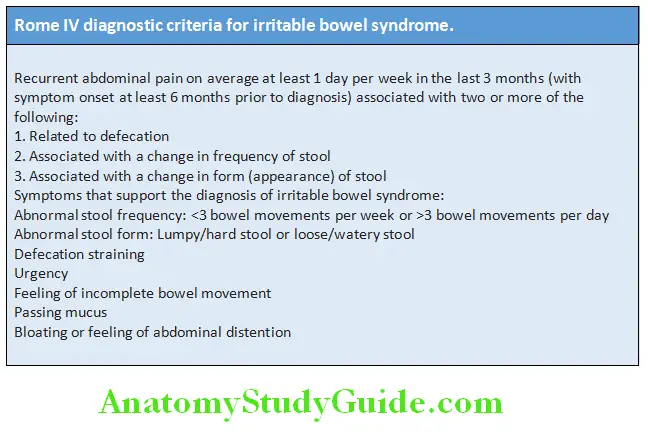
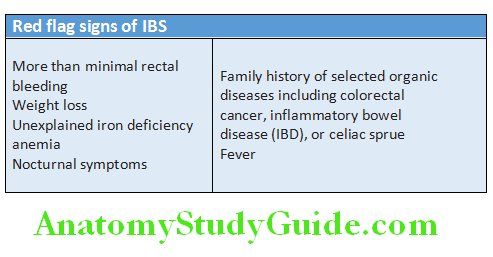
Irritable Bowel Syndrome Treatment:
Patient counseling and dietary alterations:
- Reassurance and thorough careful explanation of the functional nature and benign prognosis of the disorder
- Dietary modification: Avoid obvious foods that precipitate symptoms. The role of probiotics is not well established
- Many IBS patients have nonspecific intolerance to foods
- The dietary restriction of fermentable carbohydrates popularly termed the low FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diet
- Exclusion of gas-producing foods/foods that increase flatulence (e.g., beans, onions, celery, carrots, raisins, bananas, apricots, prunes, brussels sprouts, wheat germ, pretzels, and bagels), alcohol, and caffeine
- Irritable bowel syndrome patients should avoid foods that trigger an onset of their symptoms, consume a minimum of high fat foods, and take part in regular physical activity
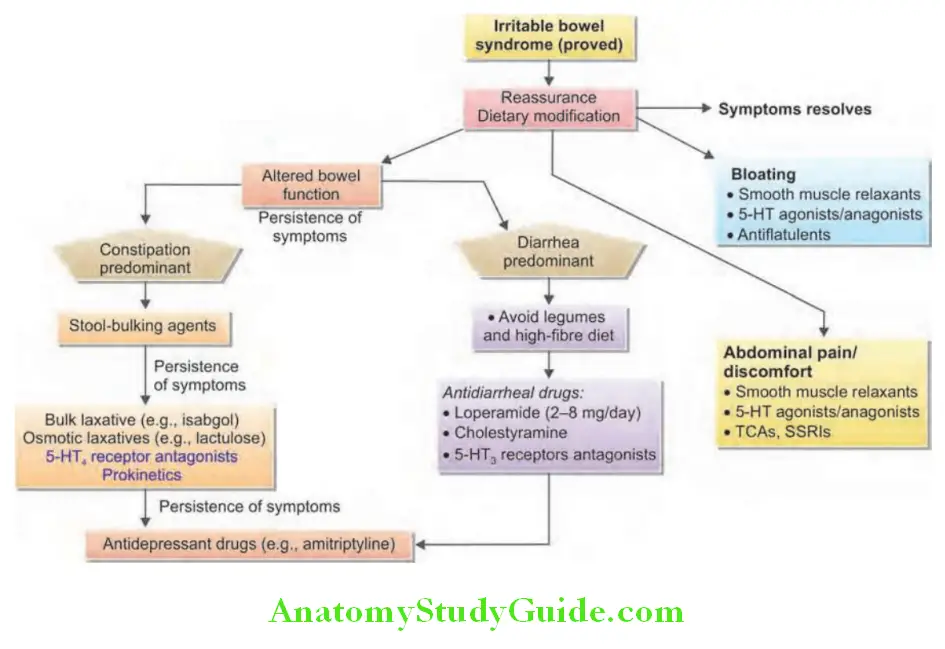
Constipations-predominant IBS:
Stool-bulking agents: High-fiber diets and bulking agents (e.g., bran or hydrophilic colloid) increase the roughage content of the diet (increases the fecal output of bacteria) and delay colonic transit. If symptoms persist add a bulk laxative (methylcellulose, isabgol husk, psyllium fiber supplement, and corn fiber). Osmotic laxatives (e.g., polyethylene glycol, lactulose, and milk of magnesia) or secretory stimulators (e.g., lubiprostone) may be tried, if high-fiber supplementation fails.
Prokinetic agents:
Tegaserod is a 5-HT4 receptor agonist and a prokinetic drug, stimulates intestinal peristalsis. However, tegaserod has been withdrawn from the market; because of serious cardiovascular events.
Cisapride and mosapride are not useful in most patients.
Antispasmodics: If abdominal pain is not adequately relieved, synthetic anticholinergic agent (dicyclomine 10 mg TID) or an antispasmodic (mebeverine 135 mg TID) may be given.
Antidepressant drugs: Patients with intractable symptoms may be benefited from tricyclic antidepressant drugs such as amitriptyline (10–25 mg orally at bedtime) or desipramine (10–25 mg orally at bedtime).
Antiflatulence therapy: Advised to eat slowly and avoid chew gum or carbonated beverage drinks. Antibiotic rifaximin (400, three times a day) may also help in relieving bloating.
Chloride-channel activators: Lubiprostone activates chloride channels in the intestinal epithelial cells. This in-turn induces passive movement of sodium and water into the lumen of the intestine and improves bowel function.
Diarrhea-predominant IBS:
- Advised to avoid legumes and high-fiber diet.
- Anti-diarrheal drugs
- Loperamide (2–4 mg up to four times a day maximum of 12 g/day).
- Cholestyramine resin is a bile acid-binding agent used as a second-line agent (4 g four to six times a day).
- Serotonin receptor antagonists: Serotonin acts on 5-HT3 receptors and increases the sensitivity of afferent neurons of the gut. Alosetron (others drugs include ondansetron, granisetron, alosetron, and cilansetron) is a 5-HT3 receptor antagonist reduces abdominal visceral pain, induces rectal relaxation, increases rectal compliance, and delays colonic transit. But it is of little use because of danger of producing ischemic colitis.
- Antispasmodics: For the control of pain.
- Antibiotics: Nonabsorbable antibiotics such as rifaximin 400 mg BID for 5–6 weeks has been tried.
- Probiotics use: The bifidobacteria, Saccharomyces boulardii, and other combinations of probiotics demonstrate some efficacy in IBS.
- Asimadoline: Kappa-opioid receptor agonist has been in trials for IBS.
Abdominal Tuberculosis:
Question 50. Describe the etiology, pathology, clinical features, complications, differential diagnosis, investigations, and treatment of abdominal tuberculosis.
Answer:
It includes gastrointestinal tuberculosis, peritoneum, and abdominal lymph nodes, either individually or in combinations.
Gastrointestinal Tuberculosis:
Intestinal tuberculosis commonly involves ileocecal region (about 70% of cases) probably because this region has:
- Increased Rate Of Absorption Of Fluid And Electrolyte;
- Increased Physiological Stasis
- Prominent Lymphoid Tissue
- Minimal digestive activity.
Abdominal Tuberculosis Other rare regions: These include ascending colon, jejunum, sigmoid colon, rectum, duodenum, stomach, and esophagus.
Abdominal Tuberculosis Etiology:
- Causative agent: Mycobacterium tuberculosis human or bovine strain.
- Routes of spread of intestinal tuberculosis
- Hematogenous spread: Primary or secondary tuberculosis of lung may spread through blood into the intestine.
- Ingestion: Mycobacteria in sputum from active pulmonary focus may be ingested and cause intestinal tuberculosis.
- Direct spread: From nearby or adjacent organs.
- Through lymphatics: From infected lymph nodes
- Routes of spread of peritoneal tuberculosis: Infection may spread to peritoneum from lymph nodes or intestinal lesions or tuberculous salpingitis (fallopian tube) in females.
Abdominal Tuberculosis Pathology:
Intestinal tuberculosis:
Three types:
1. Ulcerative (60%): More often observed in malnourished adults.
- Gross:
- Characteristics of tuberculous ulcers are:
- Multiple superficial ulcers mainly found in the ileocecal region
- Long axis of ulcers is perpendicular to the long axis of the intestine (in typhoid fever, long axis of ulcers lies parallel to the long axis of the intestine).
- Consequences: Fibrosis occurring during healing of ulcers produces strictures. Rarely, endarteritis may lead to massive bleeding.
2. Hypertrophic (10%): This is a variant of secondary tuberculosis observed in ileocecal region. More often found in relatively well-nourished adults.
- Gross: The lesions are seen mainly in cecum and/or ascending colon. These regions become thick-walled due to scarring, fibrosis, and local hypertrophy) and show mucosal ulceration.
- Clinically, the lesion present as a palpable and may be mistaken for carcinoma.
3. Ulcerohypertrophic (30%):
- It represents combination of both ulcerative and hypertrophic types.
- Right iliac fossa mass due to hypertrophic ileocecal region, and involved mesenteric fat and lymph nodes.
Peritoneal Tuberculosis:
- Gross appearance of peritoneum: Shows multiple yellow-white tubercles. Peritoneum is thick and hyperemic with a loss of its shiny appearance. Omentum is also thickened.
- Forms:
- Wet type: It presents with ascites.
- Encysted (loculated) type: It presents with a localized abdominal swelling.
- Fibrotic type: It presents with abdominal masses. Thy consist of thickening of mesentery and omentum with matted bowel loops. Adhesions may produce intestinal obstruction.
A combination of above types is also can be seen.
Solid Organ Tuberculosis:
These include:
- Spleen
- Liver
- Adrenal Tuberculosis
- Genitourinary tuberculosis.
Tuberculosis of Mesenteric Lymph Nodes:
Usually observed in young adults. Involves mesenteric lymph nodes and these nodes may become palpable as rounded mass (tabes mesenterica). May be confused with lymphoma.
Abdominal Tuberculosis Clinical features:
- Usually found in young adults.
- It may present as acute, chronic, or acute on chronic condition.
- Common symptoms: Fever, abdominal pain, anorexia, malaise, weight loss, diarrhea, constipation, alternating constipation and diarrhea, and gastrointestinal bleeding or obstruction.
- Abdominal pain may be either colicky (due to luminal compromise) or dull and continuous when there is involvement of mesenteric lymph nodes.
- Physical examination of the abdomen: It is described as “doughy” because matted loops of bowel may be palpable. A well-defined, firm, mobile mass may be found in the right lower quadrant of the abdomen. Mesenteric lymphadenitis produces mass. Abdominal distention due to ascites.
Complications and differential diagnosis are described.
Complications of intestinal tuberculosis:
- Intestinal hemorrhage
- Subacute intestinal obstruction
- Fistula formation (between skin and intestine or between loops of intestines)
- Intestinal perforation
- Malabsorption: Ileocecal tuberculosis is the common cause of malabsorption in India
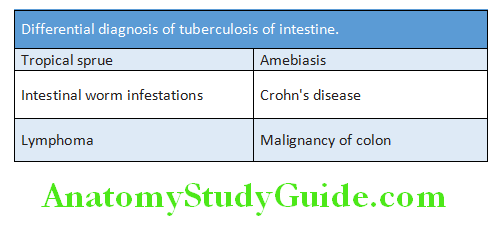
Abdominal Tuberculosis Investigations:
Hematological investigations: ESR is raised, anemia, and hypoalbuminemia.
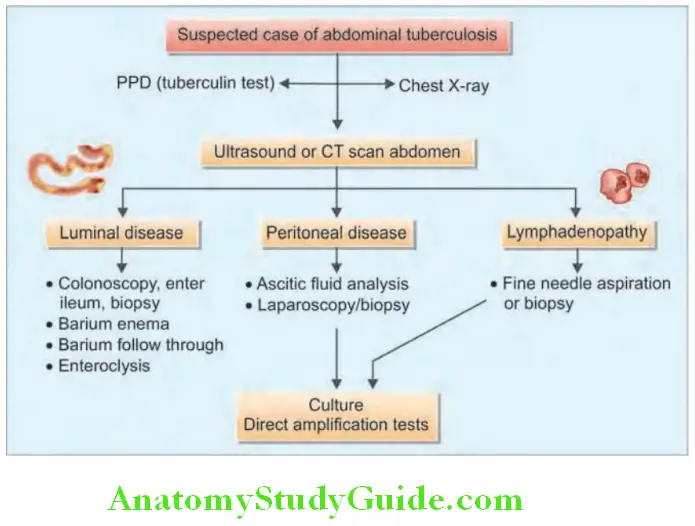
Radiological investigations:
- Chest X-ray: May show evidence of active or old tuberculosis.
- Plain X-ray of abdomen: It may reveal calcified lymph nodes.
- If there is intestinal obstruction: Dilated bowel loops with multiple air-fluid levels may be seen.
- If intestinal perforation: Air under diaphragm and dilated loops.
- Barium meal:
- May show hypermotility (accelerated intestinal transit)
- Hypersegmentation of the barium column (“chicken intestine”)
- Precipitation, flocculation, and dilution of the barium
- Luminal stenosis with smooth but stiff contours (“hour-glass stenosis”)
Multiple strictures with segmental dilatation of bowel loops:
Stierlin sign: A defect characterized by failure of the diseased segment to retain barium that is otherwise normally retained by adjacent uninvolved segments. Appears as a narrowing ileum with rapid emptying into a shortened cecum.
String sign: A thin stream of barium seen in the terminal ileum.
- Barium enema:
- Wide gaping of ileocecal valve with narrowing of the terminal ileum (“Fleischner” or “inverted umbrella sign”). Fold thickening and contour irregularity or terminal ileum shrunken in size (“conical cecum”).
- Pulled up cecum due to contraction and fibrosis of the mesocolon.
- Loss of normal ileocecal angle and dilated terminal ileum, appearing suspended from a retracted, fibrosed cecum.
- Localized stenosis opposite the ileocecal valve with a rounded off smooth cecum and a retracted fibrosed cecum.
- Abdominal ultrasound
- Intra-abdominal fluid (free or loculated; with or without debris and septae).
- Localized fluid between rapidly oriented bowel loops due to local exudation from the inflamed bowel (interloop ascites; “club sandwich” or “sliced bread” sign).
- Lymphadenopathy, discrete or matted with heterogeneous echotexture due to caseation.
- Uniform and concentric bowel wall thickening in the ileocecal region (versus eccentric thickening at the mesenteric border found in Crohn’s disease and variegated appearance of malignancy).
- Contrast-enhanced CT scan
- Symmetric circumferential thickening of cecum and terminal ileum. Ulceration or nodularity within the terminal ileum, along with narrowing and proximal dilatation
- Regional lymph nodes: Caseating lymph nodes with hypodense centers and peripheral rim enhancement.
- Retroperitoneal nodes (periaortic and pericaval) almost never seen in isolation, unlike lymphoma.
- Mesenteric thickening: Omental thickening seen as an omental cake appearance.
- Thickened peritoneum and enhancing peritoneal nodules.
- Ascitic fluid of high-attenuation value
- Ascitic fluid examination lymphocytic ascites with serum-ascites albumin gradient (SAAG) (1.1 g/dL and elevated ascites ADA level)
- Biopsy of peritoneum: Punch or laparoscopic biopsy
- Colonoscopy: It may show mucosal nodules and ulcers in colon and is used for taking biopsy from the edge of ulcers.
- Biopsy from other organs involved: Liver, lymph node
Abdominal Tuberculosis Treatment:
- Antitubercular treatment similar to treatment of pulmonary tuberculosis
- Surgery
- Strictureplasty for strictures that reduce the lumen by 50% or more and that cause proximal dilation
- Resection of segment having multiple strictures
Ulcers in Intestine:
Question 51. Write short note on ulcers in intestine.
Answer:
Conditions causing ulcers in intestine are presented in Table.
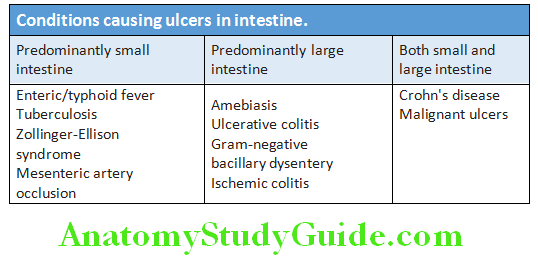
Inflammatory Bowel Disease:
Question 52. Describe the etiology, pathology, clinical features, investigations, and management of inflammatory bowel diseases (ulcerative colitis and Crohn’s disease).
Answer:
Inflammatory bowel disease (IBD) is an immune-mediated chronic intestinal condition. It results from inappropriate mucosal immune activation.
These include several conditions:
Inflammatory Bowel Disease Most important:
- Ulcerative colitis (UC)
- Crohn disease (CD)
- Others (uncommon) nonspecific inflammatory bowel disease: Indeterminate colitis (15% patients with IBD) microscopic ulcerative, microscopic lymphocytic, and microscopic collagenous colitis.
Etiology and Pathogenesis of IBD:
Genetic Factors:
Genetic predisposition/susceptibility contributes to IBD:
1. Familial:
- Crohn’s disease: Genetic factors play a prominent role. The concordance rate for monozygotic twins is about 50%.
- Ulcerative colitis: Genetic factors are less prominent than in Crohn’s disease. The concordance of monozygotic twins is only 16%. Concordance for dizygotic twins for both Crohn’s disease and ulcerative colitis is less than 10%.
2. Susceptibility genes:
Genes associated with innate immunity and autophagy (e.g., NOD2/CARD15, ATG16L1, and IRGM):
Actions of NOD2/CARD15 protein are:
- Prevents The Entry Of Microbes Into The Wall Of The Intestine
- Regulates Innate Immune Responses; And
- Prevents Excessive Immune Response By Luminal Microbes.
Environmental Factors:
Include both the local microenvironment (intestinal microflora) and the nutritional environment.
1. Intestinal microflora/microbiota:
- Hygiene hypothesis: The gut lumen contains abundant commensal bacteria and its composition within individuals remains stable for several years. This intestinal microflora can be modified by diet and disease. IBD is associated with an alteration in the bacterial flora.
- Improved food storage conditions and decreased food contamination: It has reduced frequency of enteric infections, with “clean” environment in the intestinal lumen → the immune system may not be exposed to microorganisms (pathogenic or non-pathogenic) → inadequate development of regulatory processes to limit mucosal immune responses.
2.Smoking: CD patients are more likely to be smokers, and smoking exacerbates CD. In contrast, an increased risk of UC is observed in non- or ex-smokers.
Host Factors:
These include epithelial defects, impaired mucosal barrier, abnormal intestinal defensins, and immune dysregulation.
Psychosocial Factors:
It can contribute to worsening of symptoms in IBD. Major life events (For Example, illness or death in the family, divorce, or separation) are associated with an increase in symptoms such as pain, bowel dysfunction, and bleeding.
Ulcerative Colitis:
Inflammatory Bowel Disease Definition:
Ulcerative colitis is a severe ulcerating inflammatory disease. It is limited to the large intestine (the colon and rectum). It is characterized clinically by recurrent attacks (exacerbations and remissions) of bloody diarrhea. Pathologically, the inflammatory response is found only in the mucosa and submucosa of the intestinal wall and shows chronic destruction of crypts.
Inflammatory Bowel Disease Pathology:
Site: Ulcerative colitis primarily involves the colonic mucosa. Usually involves the rectum (involved in 95% of cases) and extends proximally for a variable distance in a continuous fashion to involve part or the entire colon. Skip lesions are not seen in UC.
- Pancolitis: If entire colon is involved by the disease, then it is termed pancolitis.
- Left-sided colitis: When disease involves only the left-side of colon.
- Extensive colitis: When disease involves colon up to the hepatic flexure.
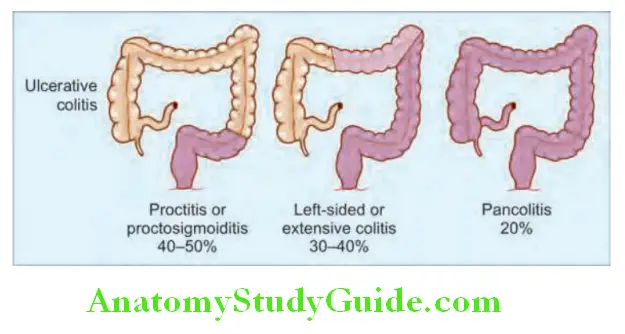
- Proctitis/proctosigmoiditis: When the disease is limited to the rectum alone, then it is known as ulcerative proctitis. When the process involves rectum and sigmoid colon, then it is termed ulcerative proctosigmoiditis.
- Backwash ileitis: The small intestine is normal. However, in severe cases of pancolitis mild mucosal inflammation of the distal ileum may be present and is termed as backwash ileitis.
Inflammatory Bowel Disease Microscopy:
- Chronic inflammatory infiltrates: Lymphocytes, plasma cells, and macrophages in the lamina propria. The density of plasma cells is more in the basilar region of the lamina propria (basal plasmacytosis) and extends into the muscularis mucosae.
- Changes in the crypt: These include cryptitis, crypt abscesses, destruction of crypts, and distortion of crypt architecture. Chronic UC may show epithelial dysplasia.
- Toxic megacolon: In severe cases (fulminant disease-toxic megacolon), inflammation may damage the muscularis propria and disturbs neuromuscular function and leads to colonic dilation and toxic megacolon that can undergo perforation. The colon is dilated, walls are thin, and with denuded mucosa and colon may rupture.
Clinical Features of UC:
Question 53. Write short essay/note on clinical features of ulcerative colitis.
Answer:
- Major symptoms of UC: The first attack is usually the most severe and the disease is later characterized by relapses and remissions.
- Diarrhea: Colonic motility is altered due to inflammation. When the disease is severe, patients develop diarrhea and pass liquid stool containing blood, mucus, pus, and fecal matter. Diarrhea is often nocturnal and/or postprandial.
- Rectal bleeding: Patients with proctitis usually pass fresh blood. When the disease extends beyond the rectum, blood is usually mixed with stool or grossly bloody diarrhea may be noted.
- Tenesmus or urgency with a feeling of incomplete evacuation.
- Passage of mucus
- Crampy abdominal pain: Severe pain is not a prominent symptom, but some patients with active disease may present m with vague lower abdominal discomfort or mild central abdominal cramping. Severe cramping and abdominal pain can develop when the attack is severe.
- Others: These include anorexia, nausea, vomiting, malaise, fever, and weight loss. There may be symptoms and signs of dehydration and anemia. In severe cases, the patient is toxic with fever, tachycardia, and signs of peritoneal inflammation.
Severity of symptoms: It reflects the extent of disease and the intensity of inflammation.
Duration of symptoms: Although UC can present acutely, symptoms are usually present for weeks to months.
Exacerbations and remissions: They are characteristic features. Relapses are provoked by emotional stress, intercurrent infection, gastroenteritis, antibiotics, or NSAID therapy.
Question 54. Write short note/essay on extraintestinal manifestations of ulcerative colitis.
Answer:
Extraintestinal manifestations:
Risk of carcinoma colon: The incidence is high, especially in patients with total colitis, disease of more than 10 years duration and early age of onset.
Signs:
- Tenderness on palpation directly over the colon, especially in the left iliac fossa.
- Signs of proctitis include tender anal canal and blood on rectal examination.
- Signs of toxic megacolon: It is a serious complication and its signs include severe pain and bleeding, and signs of peritonitis, if there is associated perforation.
Investigations:
Question 55. Write short essay/note on investigation of ulcerative colitis.
Answer:
They are required for confirmation of the diagnosis, know the distribution and activity, and identify complications.
Laboratory findings:
- Anemia: Decrease in hemoglobin may be due to blood loss or malabsorption (nutritional deficiencies) of iron, folic acid, or vitamin B12. It may be associated with raised platelet count.
- Raised ESR and acute-phase reactants [C-reactive protein (CRP)], are nonspecific serum inflammatory markers and are observed during exacerbations. They are sometimes used to monitor the activity of disease.
- Total WBC count: Moderate leukocytosis is observed in active disease, but a marked leukocytosis suggests an abscess or another suppurative complication.
- Hypoalbuminemia: Reduced serum albumin concentration may be due to protein-losing enteropathy, inflammatory disease, or malnutrition (poor nutrition).
- Stool examination
- Stool microscopy and culture: To exclude infective pathology and C. difficile toxin.
- Blood cultures in patients with septicemia.
- Serological tests: These are supportive and not used independently as markers for diagnose IBD.
- Anti-Saccharomyces cerevisiae antibodies (ASCA): These are antibodies to yeast. They are observed in 40–70% of patients with Crohn’s disease and in less than 15% of patients with ulcerative colitis. Presence of raised ASCA immunoglobulin A (IgA) and IgG titers is highly specific for Crohn’s disease.
- Perinuclear antineutrophil cytoplasmic antibodies (pANCA): They are detected in 10–20% of colon-predominant Crohn’s disease, and in 55–70% of patients with ulcerative colitis.
- Antigoblet cell autoantibodies: Found in 30–40% cases of ulcerative colitis and Crohn’s disease.
- Other tests:
- Fecal lactoferrin: It is a very sensitive and specific marker for detecting intestinal inflammation.
- Fecal calprotectin: Its levels correlate with inflammation and helpful in predicting relapses.
Ulcerative colitis Endoscopy:
Endoscopy with mucosal biopsy is the gold standard investigation for ulcerative colitis.
Colonoscopy: For mild-to-moderate disease and patient not having an acute flare, colonoscopy is preferable to flexible sigmoidoscopy because it can assess the disease extent and activity. Colonoscopy helps in assessing the extent and activity of ulcerative colitis.
Sigmoidoscopy:
- During early phase of the mild disease:
- Uniform continuous involvement of the mucosa
- Diffuse Mucosal Erythema/Hyperemia,
- Loss Of The Normal Mucosal Vascular Pattern, Granularity, And Edema
- Exudate of mucus, pus and blood on the mucosa.
- As the disease becomes severe: Mucosa becomes more friable, bleeds easily on touch, and may ulcerate. Pseudo-polyps represent epithelial regeneration and may develop after recurrent attacks in patients with long-standing disease.
Ulcerative colitis Biopsy:
Histological changes develop more slowly than clinical features. Biopsies help in diagnosis and to know the disease extent. Rectal biopsy shows mucosal inflammation and histological abnormalities are most severe in the distal colon and rectum.
Chromoendoscopy: Used for diagnosis of dysplasia in patients with long-standing UC.
Radiological features:
- Plain abdominal X-ray: Useful to exclude toxic dilatation of colon.
- Barium enema in ulcerative colitis:
- Earliest change in UC: Fine mucosal granularity
- Later, the mucosa shows thickening and superficial ulcers. Deep ulcers appear as ‘collar-button’ ulcers, which indicate that the ulcer has penetrated the mucosa.
- Haustral folds may be normal in initial phase of the disease, but later become edematous and thickened.
- Long-standing disease may show loss of haustration, pseudopolyps, narrowing and shortening of the colon.
- CT scan: It is not so helpful when compared to endoscopy and barium enema in UC. CT scanning shows: mild mural thickening (<1.5 cm), inhomogeneous wall density, no thickening of small bowel, increased perirectal and presacral fat and target appearance of the rectum.
Biochemical abnormalities:
- Electrolyte abnormalities
- Abnormal liver function tests
Question 56. Discuss severity staging of ulcerative colitis.
(or)
Write short essay/note on management of ulcerative colitis.
(or)
Describe and enumerate the indications, pharmacology, and side effects of pharmacotherapy in UC, including immunotherapy.
Answer:
Treatment of Ulcerative Colitis:
Whenever possible, IBD should be approached by a multidisciplinary team consisting of physicians, surgeons, radiologists, and dietitians. IBDs are life-long conditions and have psychosocial implications. Truelove and Witts’ severity index of ulcerative colitis is presented in Table.
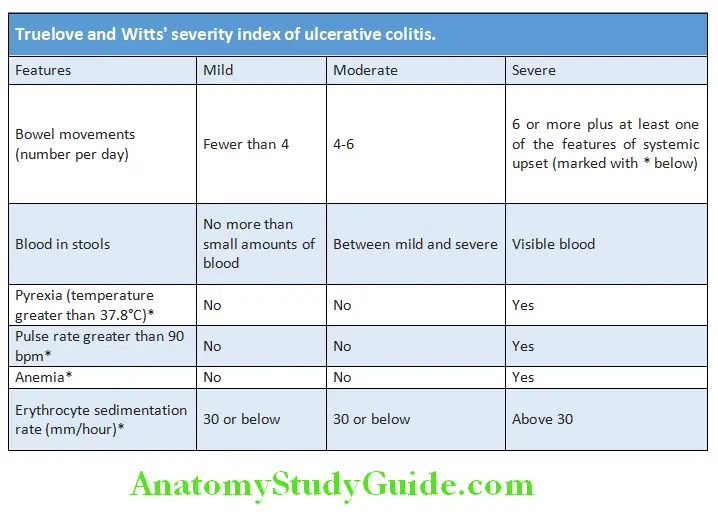
Medical Management of UC:
Aims of medical therapy:
Aims of medical therapy in ulcerative colitis:
- Treat acute attacks and reduce inflammation
- Prevent relapses and maintain clinical remission
- Detect carcinoma at an early stage
- Select patients for surgery
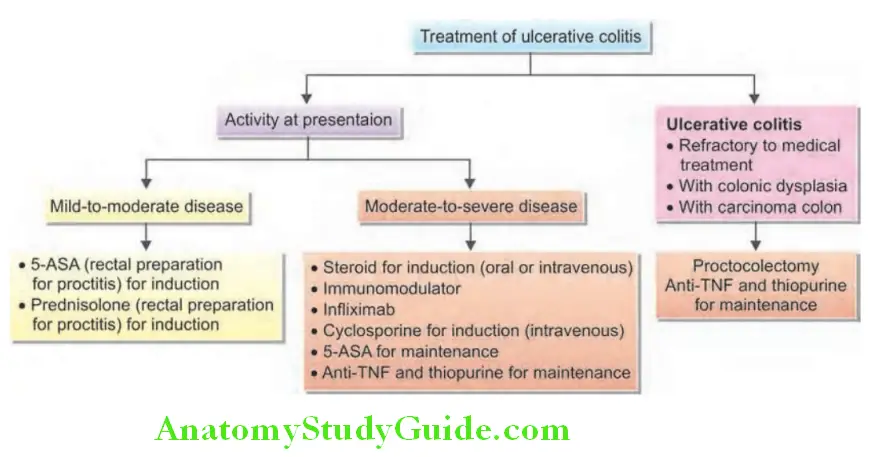
- 5-Aminosalicylate (5-ASA) agents:
- Available as oral tablets or topical (enema/suppository) preparation (for rectal and sigmoid disease).
- These agents include 5-aminosalicylic acid (5-ASA) or mesalazine alone, or combination of 5-ASA with a carrier which releases 5-ASA after splitting by bacteria in colon (sulfasalazine, olsalazine, and balsalazide).
- Topical mesalazine is the initial preferred agent in mild-to-moderate Ulcerative proctitis/proctosigmoiditis, for induction as well as maintenance of remission. It acts as a topical anti-inflammatory within the lumen of the intestine, controls acute exacerbation, maintains remission, and prevents relapses. Maintenance therapy may decrease the risk of colorectal cancer.
- Patients who are unwilling or unable to tolerate topical mesalazine can be started an oral 5-ASA medication. Oral 5-ASA should also be added in those patients who do not show remission after 4 weeks of topical therapy.
- For patients with left-sided or extensive mildly-to-moderately active UC a combination of an oral 5-ASA agent plus rectal mesalazine is used. Sulfasalazine and high dose mesalazine are the most frequently used oral agents. Sulfasalazine is the combination of a sulfapyridine (acting as a “carrier” that allows 5-ASA to be delivered into the colon) with 5-ASA (active agent).
- Side effects include nausea, dyspepsia, hair loss, headache, worsening diarrhea, and hypersensitivity reactions.
- Sulfa-free aminosalicylate preparations (e.g., olsalazine and balsalazide): They deliver higher amounts of the active ingredient of sulfasalazine (5-ASA, mesalamine) to the site of active disease in the bowel and have limited systemic toxicity.
- Remission is usually within 2–4 weeks of therapy. If remission is not induced with oral/topical ASA combination within 2–4 weeks, then a topical steroid (Budesonide)
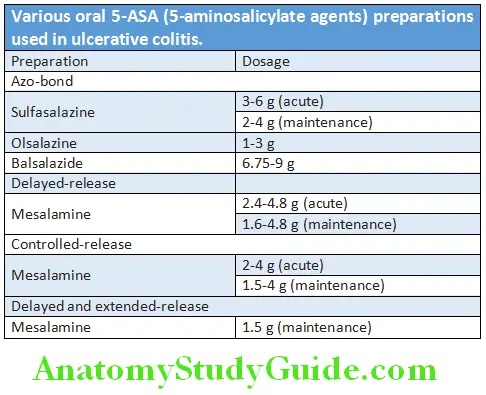
Corticosteroids:
- Oral or parenteral corticosteroids are beneficial in inducing remission in moderate-to-severe ulcerative colitis.
- They have no role in maintaining remissions. During clinical remission, steroids should be tapered according to the clinical activity.
Local Treatment:
- Topical applications of steroid are also beneficial for distal colitis and as an adjunct in patients with involvement of rectal involvement associated with involvement of proximal colon.
- Hydrocortisone or prednisolone enemas, suppositories or foam may control active disease. Budesonide-MMX uses colonic release technology to extend the application of budesonide throughout the colon.
- Duration of treatment: 3–6 weeks.
Systemic Treatment:
- Oral: Active UC that is unresponsive to 5-ASA therapy is treated with oral prednisone at doses of 40–60 mg/day for 3–6 weeks.
- Parenteral:
- Intravenous: Hydrocortisone 300 mg/day or methylprednisolone, 40–60 mg/day are given as a constant infusion in severe cases.
- Intramuscular or subcutaneous injection: Long-acting corticotrophin is used in the treatment of relapses.
- Tapering of dose: Steroids once started are gradually tapered and withdrawn, normally at a rate of no more than 5 mg/week.
Antibiotics:
No role in the treatment of active or quiescent UC.
Immune Modulators:
Indications:
- Patients who remain symptomatic despite 5-ASA therapy.
- Patients who have moderate-to-severe ulcerative colitis.
Drugs:
1. Azathioprine and 6-mercaptopurine (6-MP):
- Usefulness are as follows:
- Patients who require two or more corticosteroid courses within a year.
- Relapse of disease as the dose of prednisolone is reduced below 15 mg.
- Relapse within 6 weeks of stopping corticosteroid.
- Dosage: Azathioprine 2–3 mg/kg/day and 6-mercaptopurine 1.5 mg/kg/day.
- Disadvantage: Slow clinical response and may not be evident for as long as 12 weeks.
- Side effects: These include allergic reactions, pancreatitis, myelosuppression, infections, hepatotoxicity, and malignancy (lymphoma).
2. Methotrexate: It is a folic acid antagonist useful in patients who do not respond to azathioprine.
3. Cyclosporine (CSA): It inhibits both the cellular and humoral immune systems. CSA blocks the production of IL-2 by T-helper cells. CSA prevents activation of T cells by inhibiting calcineurin and indirectly inhibits B cell function by blocking helper T cells.
4. Tacrolimus: It is a macrolide antibiotic with immunomodulatory properties similar to CSA.
Biologics:
Used to treat moderately to severely active ulcerative colitis that has responded inadequately to conventional therapy including corticosteroids and mercaptopurine or azathioprine, or who cannot tolerate, or have contraindications for, such therapies. Common side effects include headaches, nausea, vomiting, diarrhea, skin rash, weight gain from fluid retention, muscle aches, etc. Another important side effect is reactivation of TB. Hence, prior screening for dormant/active TB is mandatory. Screening is using Mantoux test or Quantiferon-TB Gold assay (in WHO—BCG Vaccine countries).
Drugs:
1. Ant-TNF agents: Infliximab (given IV) is the most commonly used agent. Antitumor necrosis factor (anti-TNF) therapy can prevent or reduce rates of colectomy. Other agents include adalimumab and golimumab (both given subcutaneously).
2. Vedolizumab—MAB against aplha4-beta7 integrin. Preferred in elderly (>65 years), and those with history of malignancy or infectious complications.
3. Ustekinumab—MAB against interleukin 12/23.
Small Molecule Drugs:
Tofacitinib—oral small molecule Janus kinase inhibitor, used for treating adults with moderate to severe UC who have failed or are intolerant to anti-TNF agent-based therapy.
General supportive measures:
Parenteral nutrition: It is necessary in seriously ill patients and parenteral broad-spectrum antibiotics may be required in septicemia.
Correction of dehydration and electrolyte imbalance
Antispasmodic medications and antidiarrheal (loperamide) for mild diarrhea (to be avoided in severe colitis).
Surgical management:
- Surgery involves removal of the entire colon (colectomy) and rectum and is a curative procedure. It is indicated UC does not responded adequately to medical therapy. Emergency colectomy may be necessary for toxic megacolon.
- Elective surgical procedure is either panproctocolectomy with ileostomy, or proctocolectomy with ileal-anal pouch anastomosis.
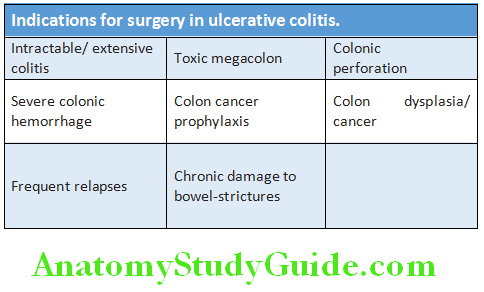
Follow-up:
- Extensive colitis of more than 10 years duration: Colonoscopy with multiple biopsies is recommended every 3 years to assess for dysplasia or malignant changes.
- UC for more than 20 years: Colonoscopy is recommended every 2 years. Biopsies from entire colon and samples from suspicious areas. If the biopsy shows high-grade dysplasia, total colectomy is performed.
Crohn’s Disease:
Question 57. Discuss the etiology, pathology, clinical features, investigations, and management of Crohn’s disease.
(or)
Write short note on Crohn’s disease.
Answer:
Etiology and Pathogenesis:
Pathology:
Gross:
- Site: It can involve any area of the gastrointestinal (GI) tract from mouth to anus. Unlike UC, rectum is spared in CD.
- Most commonly involved sites are:
- Terminal ileum and right side of colon (40–55%)
- Small intestine/bowel disease alone (30–40%): Terminal ileum alone or ileum and jejunum.
- Colon alone (15–25%)
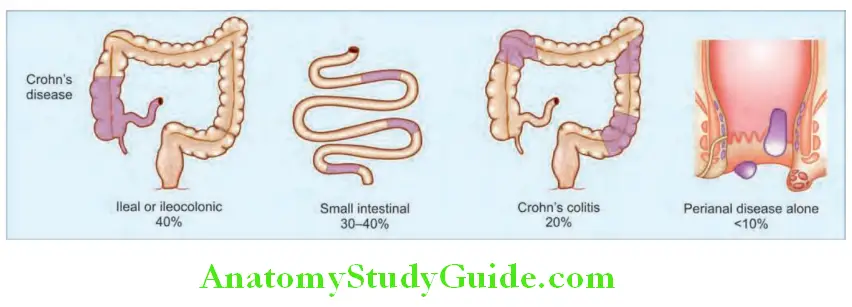
- Number of lesions: Usually, the lesions are multiple.
- Skip lesions: The intestinal involvement is discontinuous in which inflamed segments of intestine are sharply demarcated/separated by apparently normal intervening bowel/intestine in between.
- Intestinal wall: The involved intestinal wall shows fibrotic thickening and is rubbery and appears like a hosepipe and produces a characteristic radiological sign known as the “string sign”.
- Transmural inflammation: Inflammation involves all layers of the bowel wall.
- Mucosal lesions: The earliest lesion is the aphthous ulcer which becomes deeper, transmural, and discrete. Multiple lesions may coalesce longitudinally to form linear or serpentine (snake-like) ulcers and produce characteristic “cobblestone” appearance. Later the ulcer becomes deeper and form linear clefts or fissures. Similar to UC, pseudopolyps may also form in CD.
- External surface: The fat may encircle around the antimesenteric serosal surface producing a pattern known as creeping fat.
- Adhesion and fistulae: Involved loops of bowel are often adherent to each other. Fissures frequently develop between mucosal folds. They may extend deeply to become fistula tracts or sites of perforation. These fistulas may also penetrate from the bowel into other organs, including the bladder, uterus, vagina, and skin.
Microscopic features:
- Chronic inflammation by lymphocytes, plasma cells, and macrophages
- Mucosal ulcerations: Which are small, superficial (aphthous ulcers).
- Crypt abscesses: Clusters of neutrophils within a crypt and are often associated with crypt destruction.
- Noncaseating granulomas
Clinical Features of Crohn’s Disease:
Symptoms due to involvement of small intestine or ileum and right colon (ileocolitis).
CD present with one of two patterns of disease:
- Penetrating Fistulous Pattern
- Fibrostenotic obstructing pattern. The clinical manifestations depend on the site of disease.
- Crohn’s disease is a chronic disease with exacerbations and remissions.
- Major symptoms include abdominal pain (typically in the right lower quadrant), diarrhea, and weight loss (due to malabsorption and patients avoid food because eating provokes pain).
- Ileal Crohn’s disease may cause subacute or acute intestinal obstruction and patients present with recurrent episodes of colicky abdominal pain, abdominal distention, nausea, vomiting, and excessive borborygmi.
- Sparing of rectum and the presence of perianal disease are observed in about 30% of patients in the form of fistulas, abscesses, fissures, and skin tags. It presents with pain, discharge, and fever (if there is an abscess).
Physical examination:
- Signs depend on the location and severity of the disease process.
- Abdominal tenderness in the right lower quadrant (classical), accompanied by fullness, guarding, or a mass depending on the severity of inflammation.
- Palpable mass per abdomen and rectally reflects adherent loops of intestine and abscess.
- Features of malabsorption such as weight loss and anemia (iron, folic acid, and vitamin B12 malabsorption)
- Sodium, potassium, water, magnesium and zinc deficiency may develop due to chronic diarrhea.
- Stool usually does not show frank blood, mucus or pus unless colon is involved.
- Oral ulcers
Investigations:
- Anemia: Anemia may result from chronic disease, blood loss or nutritional deficiencies of iron, folate, or vitamin B12. It may be normochromic normocytic or macrocytic or hypochromic anemia depending on the deficiency/cause.
- Leukocytosis: Modestly raised leukocyte count indicates active disease, but a marked leukocytosis suggests an abscess or other suppurative complication.
- Raised ESR (erythrocyte sedimentation rate) and C-reactive protein: They are nonspecific serum inflammatory markers and may be used to monitor the activity of disease.
- Abnormal liver function tests
- Hypoproteinemia/hypoalbuminemia: Indication of malnutrition.
- Malabsorption: Ileal disease results in malabsorption of vitamin B12 (reduced serum vitamin B12 level) and Schilling test is done to determine the malabsorption of vitamin B12.
- Serologic markers: They are supportive but may not independently used for the diagnose IBD.
- Anti–Saccharomyces cerevisiae antibodies (ASCA): These are antibodies to yeast, are present in 40–70% of patients with Crohn’s disease (positive in only 10–15% cases of ulcerative colitis).
- Perinuclear antineutrophil cytoplasmic antibodies (pANCA): They are present in 20% of patients with CD (colon predominant disease), and in 55% of patients with ulcerative colitis.
- Antigoblet cell autoantibodies in 30–40% cases of Crohn’s disease.
- Antiglycan antibodies in about 40–50% cases (e.g., antilaminaribioside, antimannobioside antibodies).
- Stool examination: Stool microscopy and culture to exclude infectious causes of diarrhea.
- Sigmoidoscopy and colonoscopy in Crohn’s disease:
- Segmental inflammation with normal mucosa between (skip lesions).
- Discrete, aphthous, or deep ulcers and occasionally connected to one another, forming longitudinal stellate, serpiginous, and linear ulcers.
- Perianal disease (fissures, fistulas and skin tags) or sparing of the rectum.
- Strictures are common.
- Biopsy of involved region (e.g., colonic mucosa, ileal mucosa, anal skin tags, and perianal inflammatory lesions) shows typical noncaseating granulomatous inflammation (tuberculosis must be excluded) and infiltration by lymphocytes and plasma cell.
- Wireless capsule endoscopy (WCE) allows direct visualization and identification of inflammation in the entire small bowel mucosa. However, it should be avoided in the presence of small bowel strictures.
Radiological Findings in Crohn’s disease:
Barium meal follow thorough and barium enema:
- Early radiographic findings in the small bowel:
- Thickened folds and aphthous ulcerations
- Cobblestone appearance of mucosa resulting from longitudinal and transverse ulcerations.
- More advanced disease:
- Transmural inflammation leads to decreased luminal diameter and limited distensibility.
- Rigidity of involved segments and multiple strictures.
- As ulcers progress deeper, they can lead to fistula formation. Radiographic “string sign” is due to long areas of transmural inflammation and fibrosis, producing narrowing of lumen of involved small intestine.
- Segmental nature of CD: It results in wide gaps of normal or dilated bowel between involved segments (skip lesions).
- Inflammatory masses and abscesses may be found.
- Fistulous tracts
High-resolution ultrasound and spiral CT scanning:
- It helps in defining thickness of the bowel wall and intra-abdominal abscesses.
Radionuclide scan:
- Using gallium-labeled polymorphs or indium-labeled leukocytes identify intestinal and colonic disease and localize extraintestinal abscesses.
Question 58. Discuss Crohn’s disease severity index.
Answer:
Crohn’s Disease Activity Index:
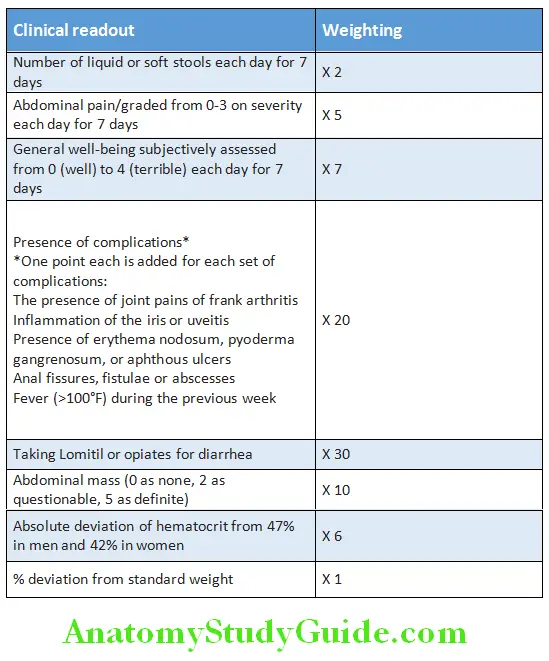
Treatment:
Medical Management of Crohn’s Disease:
General Considerations:
- Stop cigarette smoking
- Diarrhea can be controlled with loperamide, codeine phosphate, or cophenotrope.
- Long-standing diarrhea may be due to bile acid malabsorption and is treated with bile salt sequestrants (e.g., cholestyramine).
- Anemia: Due to vitamin B12, folic acid, or iron deficiency, should be treated accordingly.
Induction and Maintenance of Remission:
- Glucocorticosteroids: Used to induce remission in moderate and severe Crohn’s disease. Oral prednisolone 30–60 mg/day, which isgradually tapered and withdrawn. Mild-to-moderate ileocecal, CD should be treated by controlled-release steroids such as budesonide (9 mg by mouth once a day)
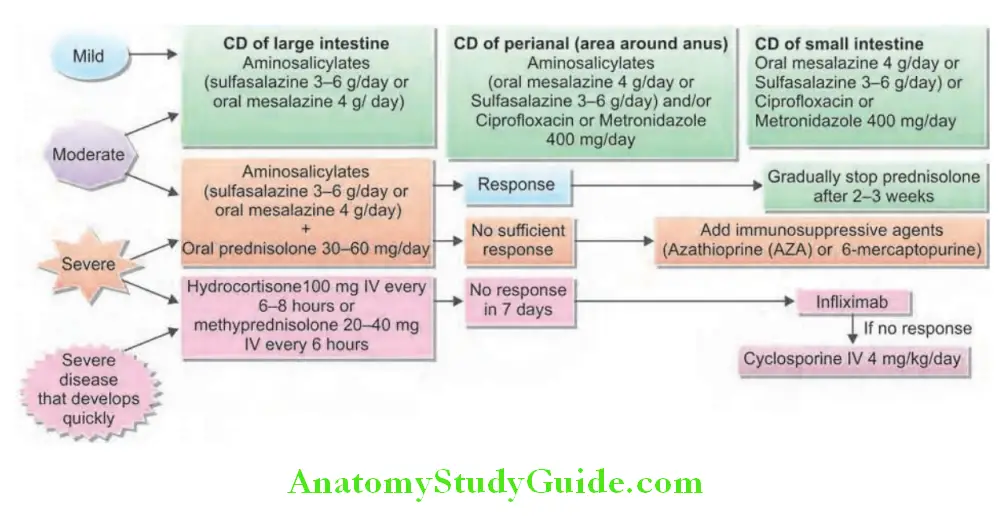
- Aminosalicylates: 5-ASA (e.g., mesalazine 4 g/day or sulfasalazine 3–6 g/day) as maintenance in mild-to-moderate ileocolonic disease. However, they are not effective for maintaining remission.
- Antibiotics: Ciprofloxacin and metronidazole 400 mg are used in abscess and perineal Crohn’s disease.
- Nutritional therapy: Dietary antigens may stimulate the immune response in the intestinal mucosa. Bowel rest and total parenteral nutrition (TPN) are effective in inducing remission but are not effective as maintenance therapy. Enteral diets with a low fat and a low linoleic acid content (not palatable) may induce remission are similar to steroids.
- Immunosuppressive agents: Azathioprine (AZA) and its metabolite 6-mercaptopurine (6MP) and newer drugs (e.g., mycophenolate mofetil) suppress the proliferation of T- and
B-lymphocytes. They are effective in inducing and maintaining remission and have steroid-sparing properties. - Biologic therapy: Anti-TNF therapy is reserved for moderateto-severe Crohn’s disease that failed to respond to other therapies (infliximab, adalimumab, and peg certolizumab) and in CD with refractory perianal and enterocutaneous fistulas.
- Vedolizumab an integrin antibody is preferred in elderly and in those with malignancies or infectious complications. Another MAB ustekinumab (anti IL 12/23) is used when standard AntiTNF therapy fails.
Maintenance of Remission:
- Aminosalicylates
- Azathioprine, 6MP, and mycophenolate mofetil
Surgical Management:
Small intestine: Strictures can be widened (stricturoplasty)/minimal resection and anastomosis.
Colorectal:
- Subtotal colectomy and ileorectal anastomosis, if rectum is spared.
- Pancolectomy with ileostomy, if whole colon and rectum are involved
Assessment of severity of Crohn’s disease is presented in Table 10.53.
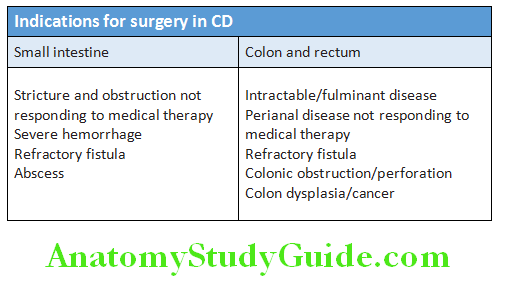
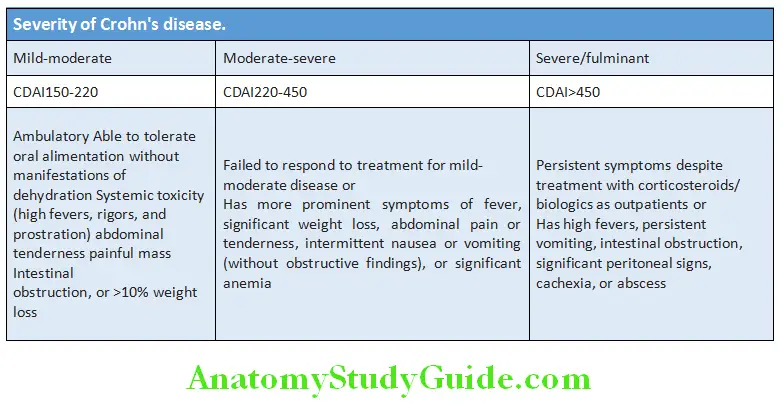
Toxic Megacolon:
Question 59. Give a brief account of toxic dilatation of colon (toxic megacolon).
Answer:
Toxic Megacolon Definition: Toxic megacolon is defined as a transverse or right colon with a diameter of greater than 6 cm, with loss of haustration.
Toxic Megacolon Causes:
- Ulcerative colitis: One of the most significant complications of UC. It can be triggered by electrolyte abnormalities, narcotics, antidiarrheal (diphenoxylate and loperamide) antispasmodics medications (reduce gastrointestinal motility), and barium enema.
- Other rare causes:
- Diarrheas are due to Clostridium difficile
- Campylobacter jejuni gastroenteritis
- Shigellosis
- Chagas’ megacolon
- Amebic colitis.
Toxic Megacolon Clinical Features:
- Features of severe colitis
- High fever, tachycardia, dehydration, electrolyte imbalance, and leukocytosis:
- Physical examination: Patient is toxic and ill, postural hypotension, colonic dilatation, abdominal tenderness over the involved colon, and absent or hypoactive bowel sounds.
- Plain radiograph of abdomen: Shows colonic dilatation with transverse colonic diameter greater than 6 cm. Air may be observed in the wall of the colon.
Complications:
Perforation is the most dangerous of the local complications.
Toxic Megacolon Treatment:
- Medical therapy: About 50% of cases will resolve with medical therapy alone
- Nil mouth, and nasogastric suction
- Intravenous fluids to replace water and electrolyte abnormalities
- Broad-spectrum antibiotics (e.g., ampicillinsulbactam) plus metronidazole
- Urgent colectomy may be necessary when there is no improvement with medical therapy
Complications of Inflmmatory Bowel Disease:
Question 60. Write short note on the complications of inflammatory bowel disease.
Answer:
It may be local and systemic (extraintestinal).
Local Complications:
Conditions that mimic inflammatory bowel disease (ulcerative or Crohn’s colitis) are presented in Table.
Extraintestinal Manifestations:
Question 61. Write short note/essay on extraintestinal manifestations of inflammatory bowel disease.
Answer:
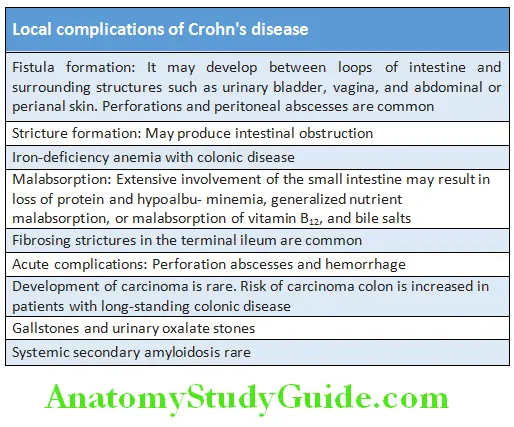
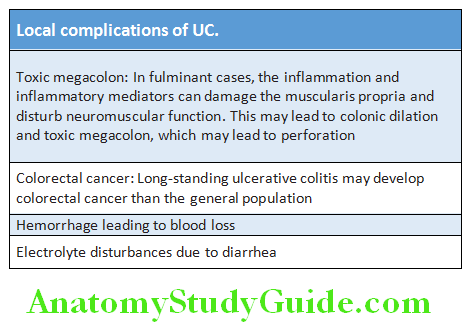
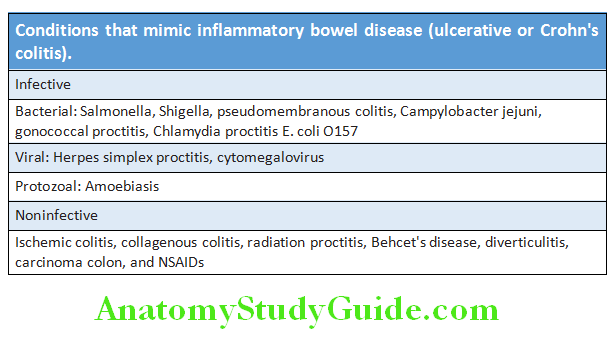
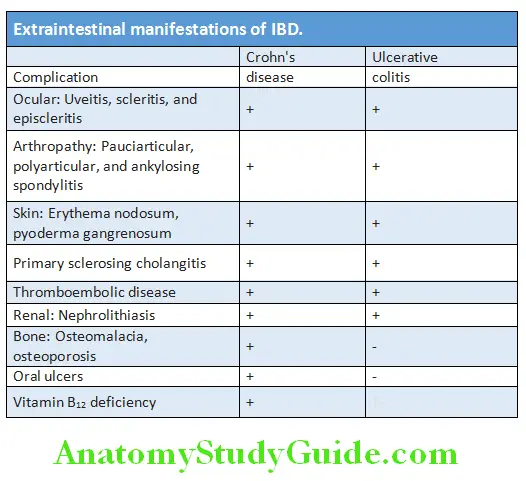
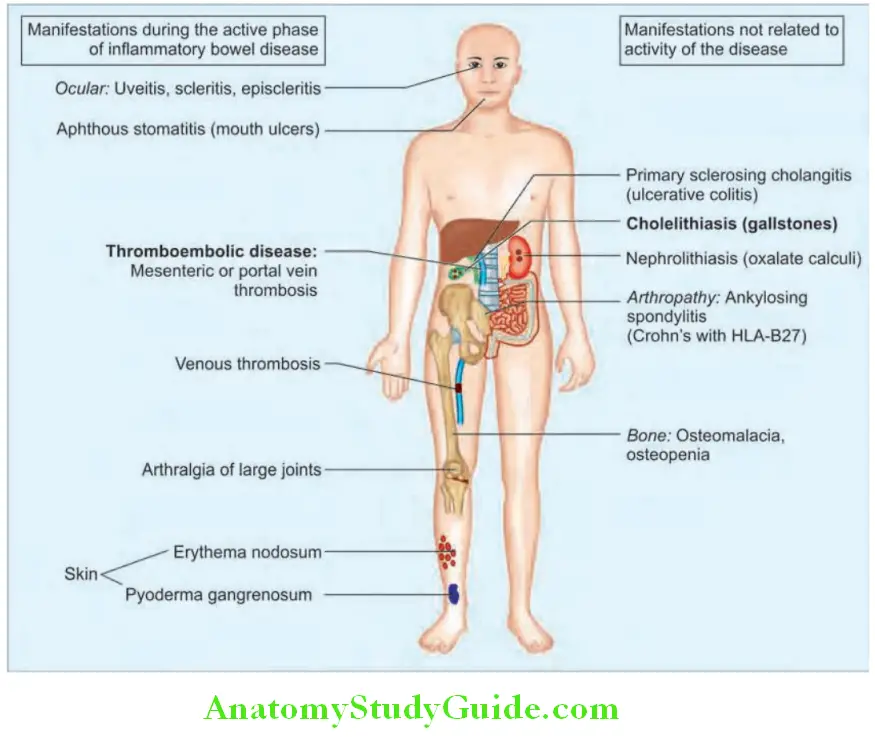
Diffrences between Ulcerative Colitis and Crohn’s Disease of the Colon:
Question 62. Write short note on the differences between ulcerative colitis and Crohn’s disease of the colon.
Answer:
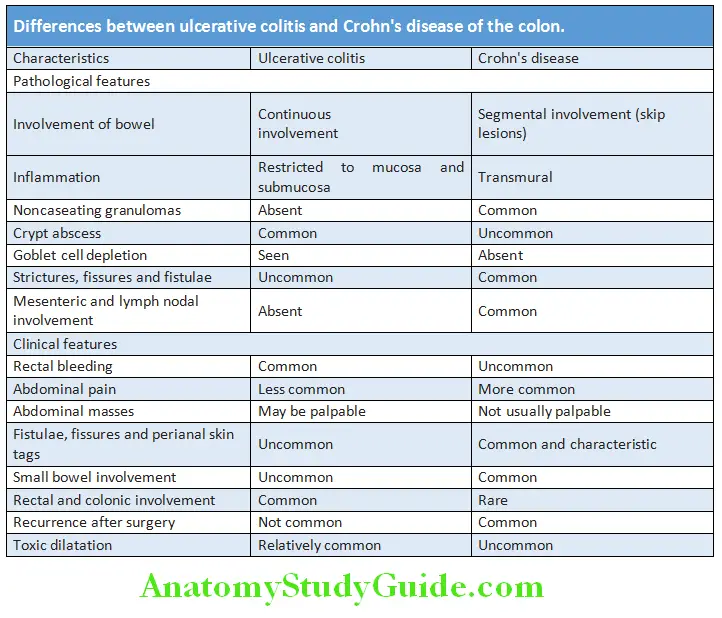
Probiotics And Prebiotics:
Question 63. Write short note on the differences between ulcerative colitis and Crohn’s disease of the colon.
Answer:
Discuss briefly about probiotics and prebiotics.
Probiotics:
Definition: Probiotics are defined as live microorganisms which are beneficial to its host. Throughout their journey in the digestive tract, they need to be intact, so they can reach the intestines where they act to give their beneficial effects to the body.
Nature:
- Bacteria: Probiotics are usually bacterial components of the normal intestinal flora of human beings (e.g., lactobacilli and Bifidobacterium infantis). They produce lactate and short-chain fatty acids (e.g., acetate and butyrate) as end products of metabolism.
- Yeast: Saccharomyces boulardii is yeast.
Preparation:
- Yogurt: It is commonly used probiotic in which is milk fermented by bacteria that convert lactose into lactic acid.
- Freeze-dried bacteria: Probiotics are also available as freeze-dried bacteria (in capsule, tablet, or powder form).
- Their composition varies and most of them contain:
- Lactobacillus acidophilus often with bifidobacteria. Other strains include Bacillus coagulans, L. Paracasei, and L. johnsonii.
Limitations: Problems with quality control and formulation restrict the clinical availability of some probiotics.
Probiotics And Prebiotics Uses:
- Malnutrition: Helps in normalizing the nutritional status of malnourished children. WHO suggested the use of yogurt in nutritional recovery.
- Lactose intolerance: Yogurt is preferred.
- Prevention and treatment of antibiotic-associated diarrhea: Probiotics containing
- Saccharomyces boulardii yeast may be useful to some extent.
- Irritable bowel syndrome (IBS) and colitis
- Improve immune function/immunity
- Necrotizing enterocolitis in neonates
- Speed treatment of certain intestinal infections
- Prevent and treat eczema in children
- Prevent or reduce the severity of colds and flu
- Prevent and treat vaginal yeast infections and urinary tract infections
- Reduce bladder cancer recurrence: Probably reduces the development of carcinoma of colon.
Prebiotics:
Probiotics And Prebiotics Defiition:
Prebiotics are referred to as a dietary fiber or carbohydrates that act as the food of probiotics. This is why it triggers bacterial growth and activity in the intestinal microflora. Therefore, it promotes good health of the host.
- Chemical substances (usually oligosaccharides) which beneficially nourish and act as a fertilizer to promote growth of the host’s intrinsic probiotic bacteria. They encourage their growth.
- Prebiotics are special form of dietary fiber.
- Prebiotics are not digested (nondigestible) by the small intestine and nonmetabolized by nonprobiotic gut flora such as Bacteroides species and Escherichia coli present in the host.
- Synthetic prebiotics are oligosaccharides containing fructose or galactose, known as fructose oligosaccharides (FOS) and galactose oligosaccharides (GOS), respectively. Lactulose is also a prebiotic.
- These oligosaccharides are enriched with the combination of inulin.
- They may be added to foods, or combined with a probiotic.
Potential uses of prebiotics:
- Relief of constipation
- Reduce intestinal pH
- Restore intestinal bacterial balance
- Increase in the absorption of calcium and magnesium
- Effect on blood cholesterol level
- Reduction of fasting glucose level in type 2 diabetes patients
- Reduce risk on colorectal cancer
- Effects on the immune system
- Better intestinal flora in infants
- Lactulose: Useful in hepatic encephalopathy
- Prevention of osteoporosis: Prebiotics may increase calcium absorption
- Chronic constipation
Synbiotics:
- Synbiotics refer to the combination of the prebiotics and probiotics within a single product.
- Prebiotics are targeted to act on the large intestines while the probiotics are most effective in doing its role in the small intestine.
- The two agents have been said to act synergistically. So, the term synbiotics is used.
Miscellaneous Topics:
Gardner’s Syndrome:
- Condition in which familial adenomatous polyposis (FAP) is associated with predominant extraintestinal manifestations.
- Autosomal dominant disorder
- Adenomatous polyps: Numerous in colon and few in the stomach and duodenum
- Extraintestinal lesions: These include:
- Osteomas of mandible, skull, and long bones
- Epidermal cysts, desmoid tumors, thyroid tumors, etc.
Probiotics And Prebiotics Treatment: Prophylactic total colectomy.
Peutz-Jeghers Syndrome:
- It is a rare autosomal dominant syndrome.
- Median age of presentation is 11 years
- It is characterized by:
- Multiple GI hamartomatous polyps: Involves the entire GIT but are most common in the small intestine. Usually, present in the dozens.
- Mucocutaneous hyperpigmentation: The melanotic pigmentation is seen in the mouth, buccal mucosa, and genitalia region.
- Peutz-Jeghers syndrome is associated with an increased risk ofseveral malignancies. These include cancers of the colon, pancreas, breast, lung, ovaries, uterus, and testicles.
- Genetics: Inactivation (loss-of-function mutations) of the STK11/LKB1 gene (tumor suppressor gene) detected in about 70% of affected families. The hamartomas are not preneoplastic precursor lesions.
- Clinical presentation: Abdominal pain, rectal bleeding, anemia, intestinal obstruction, and intussusception.
- Diagnosis and treatment: Intraoperative enteroscopy (IOE) and remove all small intestinal polyps by double balloon enteroscopy (DBE).
Indications, Contraindications and Complications of Upper Gastrointestinal Endoscopy:
Question 64. List indications, contraindications, and complications of upper gastrointestinal endoscopy.
Answer:
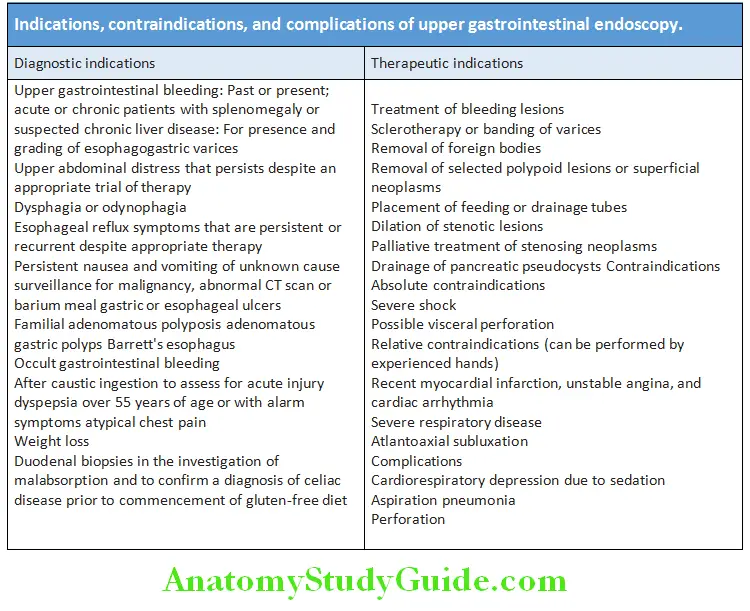
Indications for Colonoscopy:
Question 65. List indications for colonoscopy.
Answer:
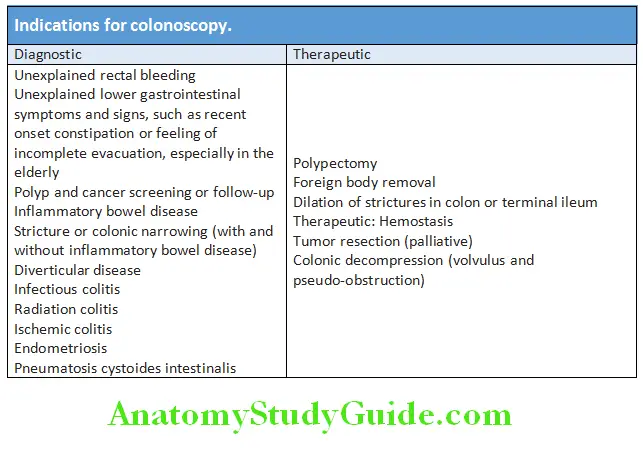
Protein-losing Enteropathy:
Question 66. Write short note on protein-losing enteropathy.
Answer:
It is characterized by excessive loss of protein into the gut lumen, sufficient to cause hypoproteinemia.
Protein-losing Enteropathy Causes: Most common in diseases with mucosal ulceration.
Protein-losing Enteropathy Clinical features: Peripheral edema and hypoproteinemia.
Protein-losing Enteropathy Investigations: Liver function tests are normal liver function and no proteinuria. Diagnosis can be confirmed by measuring fecal clearance of a1-antitrypsin or 51Cr-labeled albumin after intravenous injection. Other investigations depend on the underlying cause.
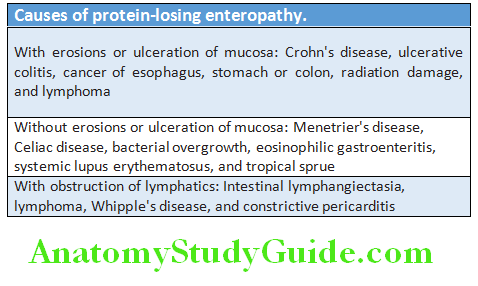
Treatment of the underlying disorder, with nutritional support and measures to control peripheral edema.
Generalized Abdominal Distension:
Question 67. List causes of abdominal distension.
Answer:
Causes of abdominal distension (7Fs):
Fat, fluid (ascites), flatus (obstruction/ileus), fetus (pregnancy), feces (constipation), full bladder, fatal neoplasm (organomegaly)
Diffrences between Diarrhea and Dysentery:
Question 68. Distinguish between diarrhea and dysentery based on clinical features.
Answer:
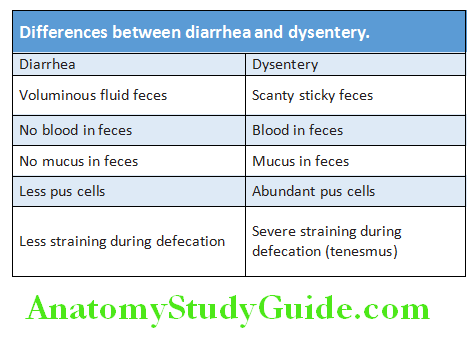
Causes of Oral Ulceration:
Question 69. List causes of oral ulceration and aphthous ulcer.
Answer:
Aphthous Ulceration:
Aphthous ulcers are superficial and painful ulcers which can develop in any part of the mouth. Recurrent ulcers are common in women prior to menstruation. The cause is unknown. Other causes of oral ulceration are presented in Table.
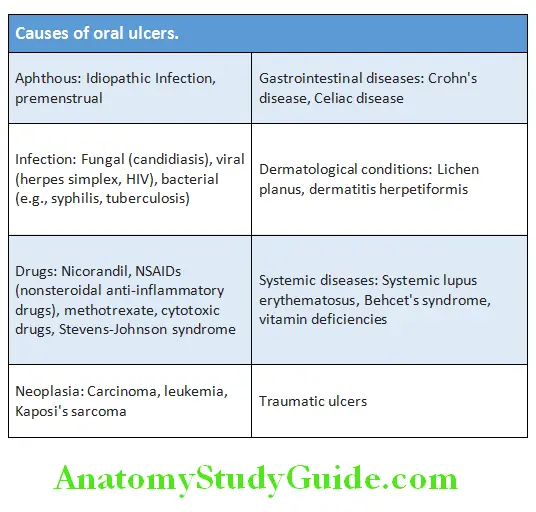
Leave a Reply