Geriatric Endodontics
Geriatric is a Greek word where geras means old and iatro means doctor. Geriatric dentistry is providing dental care to older adults involving diagnosis, prevention, management, and treatment of problems associated with older age.
Table of Contents
In general, geriatric dental treatment starts at the age of 65 years. With improvement in health care facilities and awareness, not only older age group is going to increase but also their dental needs will continue to increase.
By this age, teeth have experienced decades of dental disease, restorative and periodontal procedures. They all have an adverse effect on the pulp, periarticular, and surrounding tissues.
The combination of an increase in pathosis and dental needs along with greater expectations has resulted in more endodontic procedures for older adults.
Before considering endodontic treatment in older teeth, we will discuss age changes in teeth and surrounding tissues.
Read And Learn More: Endodontics Notes
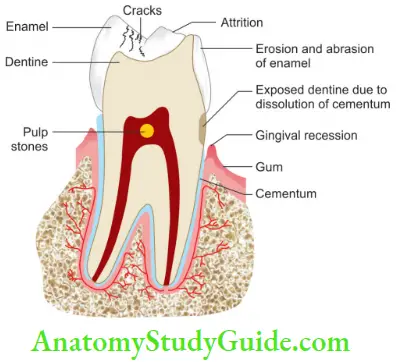
Age Changes In The Teeth
- Macroscopic Changes
- Changes in form and color
- Wear and attrition of teeth
- Causes for change in color of teeth:
-
-
- Decrease in thickness of dentin
- General loss of translucency
- Pigmentation of anatomical defects
- Corrosion products
- Inadequate oral hygiene
-
-
- Age Changes in Enamel
- Changes in enamel are based on ionic exchange mechanism
- Decrease in permeability of enamel
- Enamel becomes more brittle with age
- Enamel exhibits attrition, abrasion, and erosion
- Age Changes in Cementum
- The thickness of cementum increases with age
- It becomes more susceptible to resorption
- There is increased fluoride and magnesium content of cementum with age
- Age Changes in Dentin
- Physiologic secondary dentin formation
- Gradual obliteration of dentinal tubules
- Dentin sclerosis
- Occlusion of dentinal tubules by a gradual deposition of the peritubular dentin
- Clinical Implications of Age Changes in Dentin
- Obliteration of the tubules leads to a reduction in the sensitivity of the tissue
- Reduction in dentin permeability prevents the ingress of toxic agents
- The addition of more bulk to the dentin reduces pulpal reactions and chances of pulp exposures
- Clinical Implications of Age Changes in Dentin
- Age Changes in Pulp
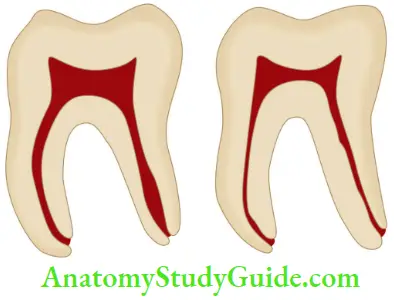
- Size of the pulp cavity decrease due to secondary dentin formation
- The difference between the dental pulp of old individuals and young teeth is due to more fires and less cells
- Blood supply to teeth decreases with age
- The prevalence of pulp stones increases with age
- Age Changes in Oral Mucosa
- Oral cavity is lined by stratified squamous epithelium which forms a barrier between the internal and external environment, thus providing protection against entry of noxious substances and organisms, mechanical damage, and fluid exchange.
- Clinical Changes in Epithelium
- With age, oral mucosa becomes increasingly thin, smooth, and dry with loss of elasticity and stippling and thus becomes more susceptible to injury.
- Tongue exhibits loss of filiform papillae and deteriorating taste sensation and occasional burning sensation.
- Histological Changes in Oral Mucosa
- These are seen in the epithelium and connective tissue.
- Epithelial Changes
- Decreased thickness of epithelial cell layer
- Reduced keratinization
- Alteration in the morphology of epithelial–connective tissue interface
- Decrease in the length of rete pegs of oral epithelium have been reported with age
- The rate of cell renewal in human oral epithelia decreases with aging
- Connective Tissue Change
- There is an increase in the number and density of elastin fibers
- Cells shrink in size and number and tend to become inactive
- Clinical Changes in Epithelium
- Oral cavity is lined by stratified squamous epithelium which forms a barrier between the internal and external environment, thus providing protection against entry of noxious substances and organisms, mechanical damage, and fluid exchange.
- Age Changes in Periodontal Connective Tissue
- Gingival connective tissue becomes denser and coarsely textured upon aging
- Decrease in the number of fibroblasts
- Decrease in the fier content
- Increase in the size of interstitial compartments containing blood vessels
- Evidence of calcification on and between the collagen fibers
- Age Changes in Salivary Glands
- There is a diminished function of salivary glands with aging resulting in reduced salivation or xerostomia.
- This causes xerostomia, mouth soreness, burning or painful tongue, taste changes, chewing difficulty, problems with swallowing and talking.
- Age Changes in Bone Tissue
- Cortical thinning
- Loss of trabeculae
- Cellular atrophy
- Sclerosis of bone
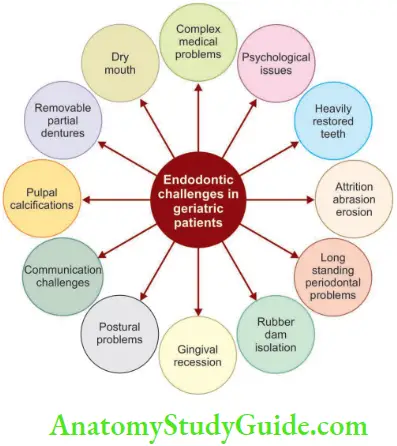
Endodontic Challenges In Geriatric Patients
The primary function of teeth is mastication, thus the loss of teeth leads to detrimental food changes and a reduction in health.
The needs, expectations, desires, and demands of older
Endodontic challenges in geriatric patients thus exceed for those of any age group.
Quality of life for older patients can be improved by preventing the loss of teeth through endodontic treatment and can add a large and impressive value to their overall dental, physical, and mental health.
Root canal treatment can be offered as a favorable alternative to the terms of extraction and cost of replacement.
Diagnosis And Treatment Plan
1. Chief Complaint of Geriatric Patients
- The most common reason for pain in old age patients is a pulpal or periapical problem that requires either root canal treatment or extraction.
- Older patients are more likely to have or already had root canal treatment and have a more realistic perception about treatment comfort.
- By and large, the pain associated with vital pulps seems to be reduced with aging and severity seems to diminish over time suggesting a reduced pulp volume.
- Patient explains regarding complaint, stimulus, or irritant that causes pain, the nature of pain, etc.
- This information is useful in determining whether the source is pulpal or periapical and if these problems are reversible or not.
2. Past Dental History
- Dentists should ask the patient’s past dental history so as to access the patient’s dental status and plan future treatment accordingly.
- From dental history, the clinician can assess the patient’s knowledge about dental treatment and his psychological attitude, and expectations from dental treatment.
3. Medical History
- Dentists should recognize that the biological or functional age of an individual is far more important than chronological age.
- As most of old-aged people suffer from one or other medical problems, a medical history should be taken prior to starting any treatment for geriatric patients.
- A standardized form should be used to identify any disease or therapy that would alter the treatment plan or its outcome.
- Aging usually causes changes in the cardiovascular, respiratory, and central nervous systems that result in most drug therapy needs.
- The renal and liver function of the patients should be considered while prescribing drugs as they have some action on these organs.
4. Examination of the Patient
- The extraoral and intraoral clinical examination provides the dentist useful information regarding the disease and previous treatment done.
- Common observations in geriatric patients:
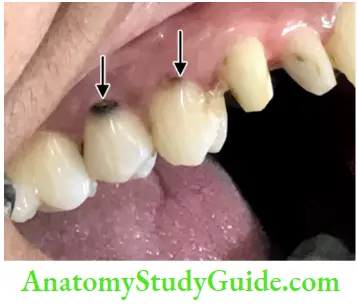
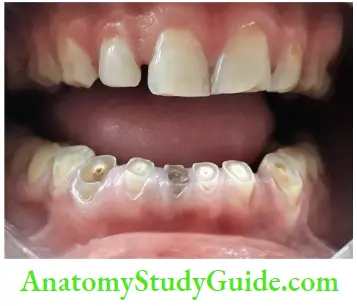
Missing teeth: In older patients, usually some of teeth get extracted. Missing teeth indicate a decrease in functional ability, resulting in loss of chewing ability. This reduced chewing ability leads to a higher intake of a more refined soft carbohydrate diet and sugar intake to compensate for loss of taste and xerostomia. All these lead to increased susceptibility to dental decay
Gingival recession: It results in exposure of cementum and dentin and thus making them more prone to decay and sensitivity

Root caries: It is very common in older patients and is difficult to treat; the caries excavation is irritating to the pulp and often results in pulp exposures or reparative dentin formation making the canal negotiation difficult
Attrition, abrasion, and erosion expose the dentin and allow the pulp to respond with dentinal sclerosis and reparative dentin which may completely obliterate the pulp

With increasing age, the size of pulp cavity decreases due to reparative dentin formation.
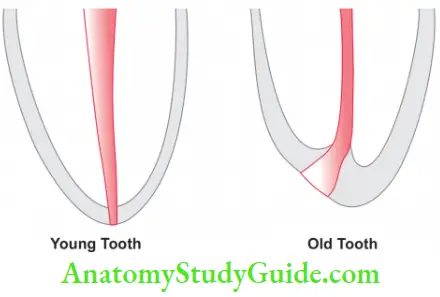
Continued cementum deposition is seen with increasing age thus moving cementodentinal junction (CDJ) farther from the radiographic apex.
Calcifications are observed in the pulp cavity which can be due to caries, pulpotomy, or trauma and is more of linear type. the lateral and accessory canals can be calcified, thus decreasing their clinical significance
Reduced tubular permeability is seen because dentinal tubules become occluded with advancing age
Missing and titled teeth in older patients result in changes in the molar relationship, a biting pattern that can cause temporomandibular joint (TMJ) disorders
Reduced mouth opening increases the working time and decreases the accessibility for treatment
Presence of multiple restorations indicates a history of repeated dental treatment. Pulpal injury in older age patients is the mainly because of marginal leakage and microbial contamination of cavity walls
5. Pulp Vitality Tests like a cold test, heat test, electric pulp test, and test cavity tell the status of the pulp, but these tests are not very accurate because of extensive calcification and the reduced size of the pulp cavity.
6. Radiographs
- Radiographs help the clinician to identify the status of the tooth and then plan the treatment.
- But while taking radiographs of geriatric patients, the following problems are encountered:
- The presence of tori, exostoses, denser bone requires increased exposure times for proper diagnostic contrast
- Older patients may be less capable of assisting in fim placement so fim holders should be used to secure the position of fim.
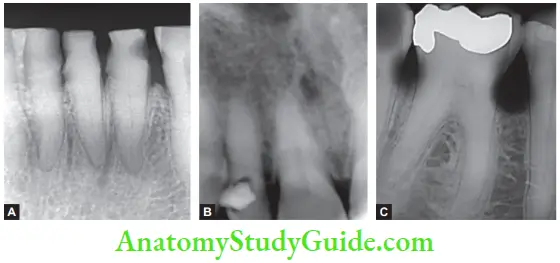
- Common Radiographic Observations in Geriatric Patients
-
-
- Receded pulp cavity which is accelerated by reparative dentin
- Presence of pulp stones and dystrophic calcification
- Receding pulp horns can be noted in the radiograph
- Deep proximal or root decay may cause calcification of the pulp cavity
- A midroot disappearance of a detectable canal may indicate bifurcation rather than calcification
- In cases where the vitality tests do not correlate with the radiographic findings, one should consider the presence of odontogenic and nonodontogenic cysts and tumors
- In teeth with root resorption along with apical periodontitis, shape of apex and anatomy of foramen may change due to inflammatory osteoclastic activity
- In teeth with hypercementosis, the apical anatomy may become unclear
-
7. Treatment Plan
- Considerations for endodontic treatment in geriatric patients:
- Irrespective of age, main aim of treatment is the removal of pain and infection so as to restore teeth to normal health and function
- For medically compromised or cognitively impaired cardiac patients and neuropsychiatric patients, it is safe and better to start treatment only after a valid consent is obtained from the particular doctors
- Depending on the length of the appointment, morning appointments are preferable though some patients prefer late morning or early afternoon visits to allow “morning stiffness” to dissipate
- Single-appointment procedures are better, as these patients may have physical problems and require transportation or physical assistance to get into the office
- Because of reduced blood supply, pulp capping is not as successful in older teeth as in younger ones, therefore, not recommended
- Endodontic surgery in geriatric patients is not as viable an alternative as for a younger patient
8. Anesthesia
- Older patients are less anxious about dental treatment because of low conduction velocity of nerves, limited extension of nerves into the dentin, and dentinal tubules are more calcified
- In older patients, the width of the periodontal ligament is reduced which makes the needle placement for intraligamentary injection more difficult.
- Only smaller amounts of anesthetic should be deposited and the depth of anesthesia should be checked before repeating the procedure
- Intrapulpal anesthesia is difficult in older patients as the volume of the pulp chamber is reduced
9. Isolation
- Rubber dam is the best method of isolation. If the tooth is badly mutilated making the rubber dam placement difficult, then consider multiple tooth isolation with a saliva ejector
10. Access to Canal Orifice
- One of the most difficult parts in the treatment of older patients is the identification of the canal orifices
- Obtaining access to the root canal and making the patients to keep their mouths open for a longer period of time is a real problem in older patients
- A radiograph should be taken to determine canal position, root curvature, axial inclinations of root and crown, and extent of the lesion
- In case of compromised access for preparation, coronal tooth structure or restorations need to be sacrificed.
- Endodontic microscopes can be of greater help in identifying and treating narrow geriatric canals
11. Cleaning and Shaping
- Calcifid canals in geriatric patients are more difficult to locate and penetrate. Canals seem to be longer due to cementum deposition
- DG 16 explorer is used for the initial assessment of the orifice
- Use of broaches for pulp tissue extirpation is avoided in older patients because very few canals of older teeth have adequate diameter to allow safe and effective uses of broaches
- NiTi instruments are used for cleaning and shaping in crown down technique rather than stainless steel hand files.
- This saves time, provides the flexibility of NiTi, and avoids tiredness of hand while working in sclerosed canals
- One should prefer rotary NiTi files with no rake angle in the crown down technique
- It is difficult to locate apical constriction in these patients because of reduced periapical sensitivity in older patients, reduced tactile sense of the clinician, and limited use of apex locator in heavily restored teeth
12. Obturation
- For obturation, those obturation techniques are employed which do not require a large midfoot taper. The lateral compaction technique is preferred in these patients.
13. Prognosis of Endodontic Treatment
- In the case of vital pulp, the prognosis depends on many local and systemic factors.
- In case of nonvital pulp, the repair is slow because of
- Arteriosclerotic changes in blood vessels
- Decreased rate of bone formation and resorption
- Increased mineralization of bone
- Altered viscosity of connective tissue
14. Endodontic Surgery
- Indications
- Irrespective of age, indications are same as discussed.
- Medical history is important in older patients
- Following local anatomic considerations should be considered in elderly patients:
- Increased incidence of dehiscence of roots and exostoses
- Apically positioned muscle attachment
- Less resilient tissue
- Decreased resistance to reflection
- Ecchymosis and delayed healing are common postoperative findings
Geriatric Endodontics Conclusion
- Geriatric dentistry is a specialized multidisciplinary branch of general dentistry designed to provide dental services to elderly patients.
- With the increase in life expectancy, the demand for geriatric dentistry is increasing. It means the dental practitioners are expected to take care of more geriatric patients in the future.
- Due to the presence of age-related physiological and psychological changes, and medical conditions, the management of the elderly population differs from that of the general population.
- Since oral health is directly associated with the general well-being of patients, dental care should be included in the overall health management of all geriatric patients.
- Dentists should make an attempt to meet the needs of elderly patients, provide the necessary infrastructure, and offer them empathetic care to ensure satisfaction.
Leave a Reply