Human Internal Pulp Anatomy
Introduction
For the success of endodontic therapy, it is essential to have knowledge of the normal configuration of the pulp cavity. In addition to general morphology, variations in the canal system must be kept in mind while performing root canal therapy.
Table of Contents
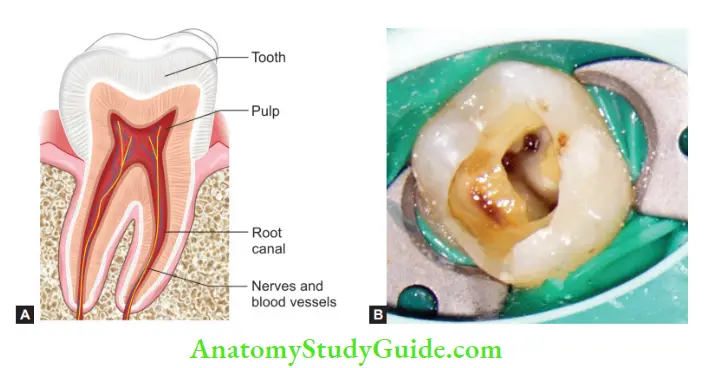
Pulp Cavity
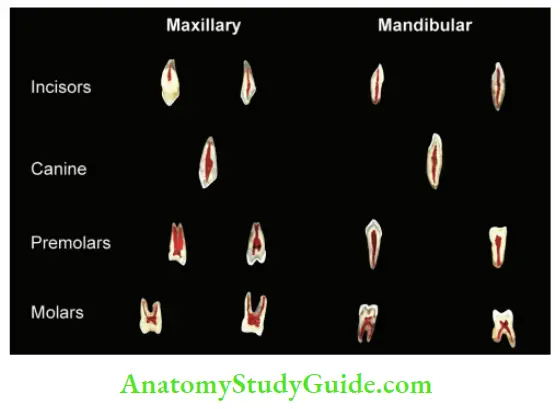
The pulp cavity is the central cavity of a tooth containing dental pulp and consists of the root canal and pulp chamber. It is enclosed by dentin all around, except at the apical foramen.
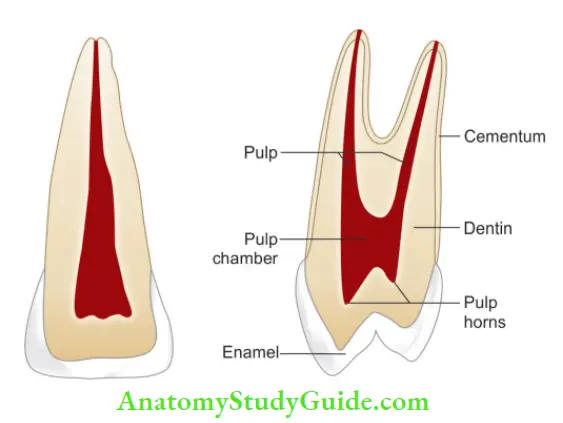
Pulp Chamber:
- It occupies the coronal portion of the pulp cavity and acquires the shape according to the external form of the crown of a tooth
- The roof consists of dentin covering the pulp chamber occlusal or incisal
- The floor of the pulp chamber merges into the root canal at orifices.
Read And Learn More: Endodontics Notes
Pulp Horns:
- Pulp horns are landmarks present occlusal to the pulp chamber. These may vary in height and location. The occlusal extent of pulp horn corresponds to the height of contour in young permanent teeth
- The pulp horn tends to be a single horn associated with each cusp of posterior teeth and mesial and distal in anterior teeth.
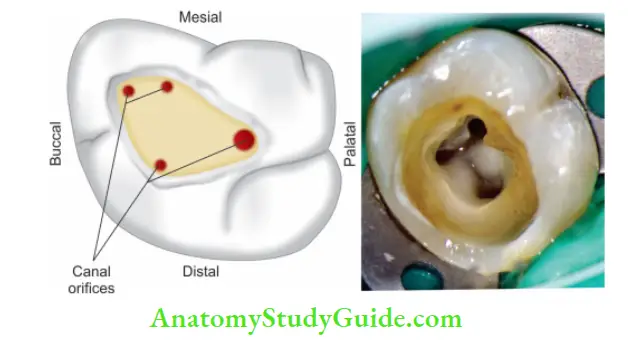
Canal Orifice:
Canal orifices are openings in the floor of pulp chamber leading into root canals.
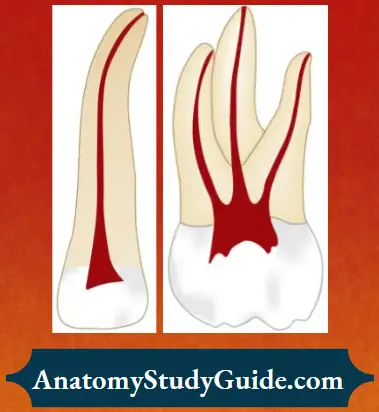
Root Canal:
- Root canal extends from the canal orifice to the apical foramen
- In anterior teeth, the pulp chamber merges into the root canal, but in multirooted posterior teeth, this division becomes quite obvious
- Usually, a root canal has curvature or constriction before terminating at the apex
- Curvature in the root canal can be smooth or sharp, single or double in the form of the letter “S”
Apical Root Anatomy:
Following anatomic and histological landmarks are seen in the apical part of the root canal:
Apical Constriction (Minor Diameter):
- It is an apical part of the root canal with the narrowest diameter short of the apical foramina or radiographic apex
- Apical constriction is mostly located within the dentin or at CDJ and rarely in the cementum. So, it may or may not coincide with CDJ
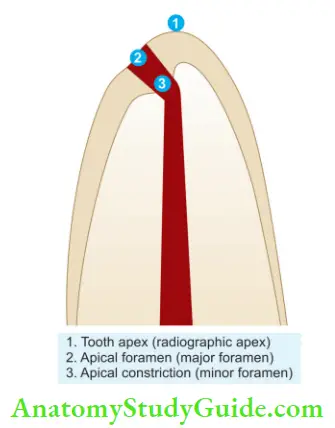
Apical Foramen (Major Diameter):
- It is the main apical opening on the surface of the root canal through which blood vessels enter the canal
- Its diameter is almost double the apical constriction giving it a funnel shape appearance, which has been described as morning glory or hyperbolic
- Apical foramen may not always be located at the center of the apex. It may exit mesial, distal, buccal, or lingual
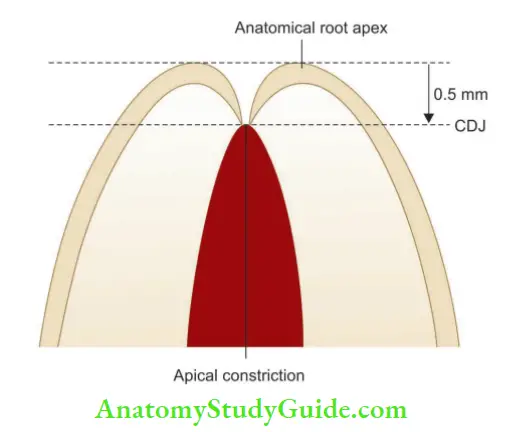
Cementodentinal Junction:
- The cementodentinal junction is the point in the canal, where the cementum meets the dentin
- The position of CDJ varies but usually, it lies 0.5-1 mm from the apical foramen
- According to Kutler’s study, the average distance between minor and major diameters in young persons is 0.5 mm, and in older persons, it is 0.67 mm.
Apical Delta:
It is a triangular area of root surrounded by a main canal, accessory canals, and periarticular tissue.

Significance of Apical Third:
- Apical constriction acts as a natural stop for filling materials. Root canal treatment of the apical part is difficult because of the presence of accessory and lateral canals, pulp stones, varying amounts of irregular secondary dentin, and areas of resorption
- Most of the curvatures occur in the apical third, so one has to be very careful during canal preparation
- The size and shape of the foramen should always be maintained. Apical 3 mm of the root is generally resected during endodontic surgery in order to eliminate canal aberrations
Isthmus:
Isthmus is defined as narrow, ribbon-shaped communication between two root canals encompassing the pulp tissue. It can be seen in any two canals of the same root. It is a part of the root canal system and it is not a separate entity, so it should be cleaned, shaped, and obturated as other root canals.
Identification:
An isthmus can be identifid by using methylene blue dye.
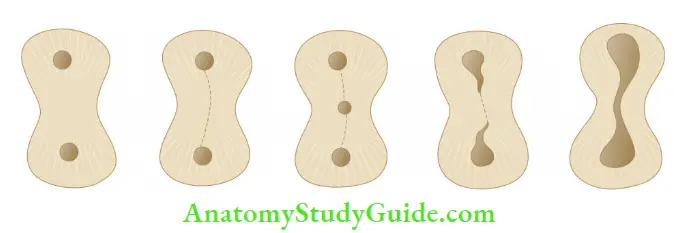
Classification:
Hsu and Kin in 1997 classifid isthmus as
- Type 1:Two or three canals with no visible communication (incomplete isthmus)
- Type 2:Two canals showing the definite connection between them
- Type 3:Thee canals show definite connection between them
- Type 4:It is similar to Type II or Type III with canals extending to the isthmus area.
- Type 5:It is a true connection throughout the section of root.
Clinical signifiance of isthmus:
- Commonly isthmus is found between two canals present in one root like the mesial root of mandibular molars
- Isthmus has been shown to be the main causative agent responsible for root canal failures. So, it is always mandatory to clean, shape, and fill the isthmus area by orthograde or retrograde filing of root canals
Root Canal Classifiation
Various types of research have been conducted to study normal variations in the anatomy of the pulp cavity, but an exhaustive work on canal anatomy was done by Hess. He studied branching, anastomoses, intricate curvatures, shape, size, and a number of root canals in different teeth.
Others who have contributed to the studies of pulp anatomy are Wheeler, Rankine-Wilson, Weine, Perth, etc. Weine classified root canal morphology based on the number of canal orifice, number of canals, and number of foramina in each tooth as the following :
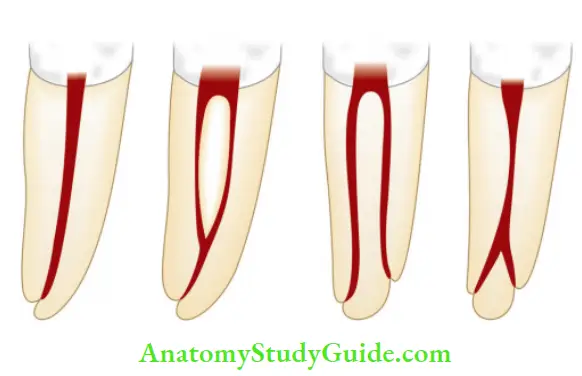
- Type 1:Single canal from the pulp chamber to apex.
- Type 2:Two separate canals leave the chamber but exit as one canal.
- Type 3:Two separate canals leave the chamber and exiting as two separate foramina.
- Type 4:One canal leaving the chamber but dividing into two separate canals and exiting in two separate foramina.
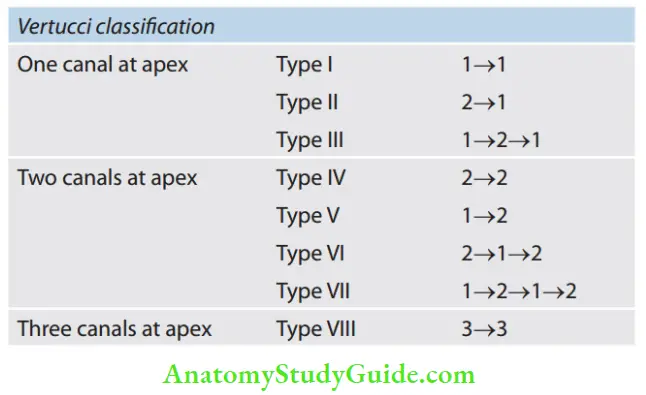
Vertucci gave eight different forms of pulp anatomy rather than four. It does not consider possible positions of auxiliary canals or exit positions of the apical foramen. Vertucci’s classifiation:
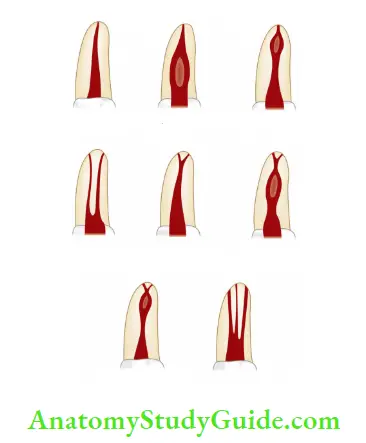
- Type 1:A single canal extends from the pulp chamber to the apex (1).
- Type 2:Two separate canals leave the pulp chamber and join short of the apex to form one canal (2-1).
- Type 3:One canal leaves the pulp chamber and divides into two in the root; the two then merge to exit as one canal (1-2-1).
- Type 4:Two separate, distinct canals extend from the pulp chamber to the apex (2).
- Type 5:One canal leaves the pulp chamber and divides short of the apex into two separate, distinct canals with separate apical foramina (1-2).
- Type 6:Two separate canals leave the pulp chamber, merge in the body of the root and redivide short of the apex to exit as two distinct canals (2-1-2).
- Type 7:One canal leaves the pulp chamber, divides, and then rejoins in the body of the root and finally redivides into two distinct canals short of the apex (1-2-1-2).
- Type 8:Thee separate, distinct canals extend from the pulp chamber to the apex (3).
Methods Of Determining Pulp Anatomy
The following two methods are employed for determining the pulp anatomy of teeth:
- Clinical methods
- Anatomic studies
- Radiographs
- Exploration
- High-resolution computed tomography
- Visualization endrogram
- Fiber-optic endoscope
- MRI
- In vitro methods
- Sectioning of teeth
- Use of dyes
- Clearing of teeth
- Contrasting media
- Scanning electron microscopic analysis
Clinical methods:
Anatomic Studies:
Knowledge of anatomy gained from various studies and textbooks is a commonly used method.
Radiographs:
Good-quality radiographs are useful in assessing root canal anatomy. Since a radiograph is a two-dimensional picture of a three-dimensional object, one has to analyze the radiograph carefully.
High-Resolution Computed Tomography:
It shows a three-dimensional picture of the root canal system using computer image processing.
Fiber-Optic Endoscope:
It is used to visualize canal anatomy.
Visualization Endogram:
In this technique, an irrigant, called Ruddle’s solution, is injected into canals to visualize them on the radiograph. Ruddle’s solution consists of
5% NaOCL + 17% EDTA + Hypaque = Ruddles solution
- Sodium hypochlorite: To dissolve organic tissues
- 17% EDTA: To dissolve inorganic tissue
- Hypaque: It is an iodine-containing radiopaque contrast media
The composition of the Ruddle solution provides solvent action of sodium hypochlorite, visualization as it is radiopaque, and improved penetration because EDTA lowers the surface tension.
MRI:
It produces data on a computer which helps in knowing canal morphology.
Exploration:
On reaching the pulpal floor, one finds the grooves and anatomic dark lines that connect the canal orifices called dentinal map. The map should be examined and explored using an endodontic explorer.
In Vitro methods:
Sectioning:
In this, teeth are sectioned longitudinally for visualization of the root canal system.
Use of Dyes:
Methylene blue or fluorescein sodium dyes help in locating pulp tissue preset in the pulp chamber because dyes stain any vital tissue present in the pulp chamber or root canals.
Clearing of Teeth:
For the clearing process, teeth are initially stored in 5% nitric acid for 5 days. Then these are rinsed, dried, and dehydrated using increasing concentrations of ethanol (70%, 80%, and 95%) successively for 1 day. The teeth are rendered transparent by immersing in methyl salicylate, into which dye is injected to visualize the anatomy.

Hypaque/Contrasting Media:
It is an iodine-containing media which is injected into root canal space and visualized on the radiograph.
Scanning Electron Microscopic Analysis:
Scanning electron microscopic (SEM) uses a focused beam of high-energy electrons to generate a variety of signals at the surface of solid specimens. These signals reveal information about the morphology, chemical composition, and structure of that material. This is how SEM helps in evaluating root canal anatomy.
Variations In The Internal Anatomy Of Teeth
Canal confiuration can vary in some cases because of developmental anomalies, hereditary factors, trauma, etc. Usually the variations in root morphologies tend to be bilateral.
Variations of pulp space:
- Variations in development
- Gemination
- Fusion
- Concrescence
- Taurodontism
- Talon’s cusp
- Dilacerations
- Dentinogenesis imperfect
- Dentin dysplasia
- Lingual groove
- Extra root canal
- Missing root
- Dens evaginates
- Dens invaginatus
- Variations in the shape of the pulp cavity
- Gradual curve
- Apical curve
- C-shaped
- Bayonet-shaped
- Dilaceration
- Sickle-shaped
- Variations in pulp cavity due to pathology
- Pulp stones
- Calcifications
- Internal resorption
- External resorption
- Variations in the apical third
- Different locations of the apex
- Accessory and lateral canals
- Open apex
Variations in the size of a tooth
-
- Macrodontia
- Microdontia
Variations in Development:
Gemination:
Gemination literally means twinning. It arises from an attempt at the division of a single tooth germ by an invagination resulting in the incomplete formation of two teeth. It gives the appearance of completely or incompletely separated crowns having a single root canal.

Fusion:
Fusion results in the union of two normally separated tooth germs. Fused teeth may show separate or fused pulp space.
Concrescence:
In this, fusion occurs after the root formation has been completed. Teeth are only joined by cementum.
Taurodontism:
In this, the body of the tooth is enlarged at the expense of roots (also called bull-like teeth). The pulp chamber of this tooth is extremely large with a greater apical-occlusal height. Bifurcation/trifurcation may be present only a few millimeters above the root apex.
The pulp lacks the normal constriction at the cervical level of the tooth. This condition is commonly seen associated with syndromes like Klinefelter syndrome and Down syndrome.

Talon’s Cusp:
It resembles an eagle’s talon. In this, an anomalous structure projects lingually from the cingulum area of the maxillary or mandibular incisor. This structure blends smoothly with the tooth except that there is a deep developmental groove where that structure blends with the lingual surface of the tooth.
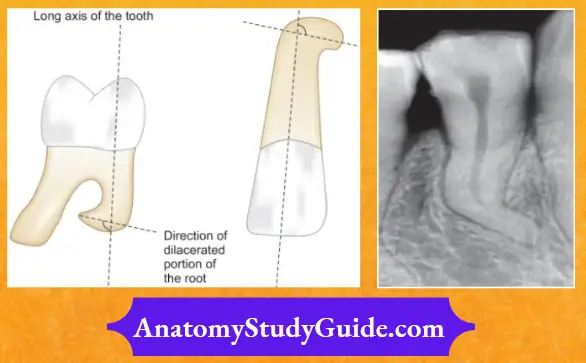
Dilaceration:
Dilaceration is an extraordinary curvature in the roots. It can result from trauma during root development in which movement of the crown and a part of the root may result in sharp angulation after the tooth completes development.
Dentinogenesis Imperfecta:
It results in the defective formation of dentin. It shows partial or total precocious obliteration of the pulp chamber and root canals because of the continued formation of dentin.
Dentin Dysplasia:
It is characterized by the formation of normal enamel, atypical dentin, and abnormal pulpal morphology. In this, root canals are usually obliterated so need special care while instrumentation.
Lingual Groove:
It is a surface in the folding of dentin directed from the cervical portion toward the apical direction. It is frequently seen in maxillary lateral incisors. A deep lingual groove is usually associated with a deep narrow periodontal pocket which often communicates with the pulp causing endodontic– periodontal relationship. The prognosis of such teeth is poor and treatment is difficult.
Presence of Extracanals:
More than 90% of maxillary first molars show the occurrence of the second mesiobuccal canal (MB2). Location of the orifice can be made by visualizing a point at the intersection between a line running from the mesiobuccal to the palatal canal and a perpendicular line from the distobuccal canal In mandibular molars, extra canals are found in 38% of the cases.
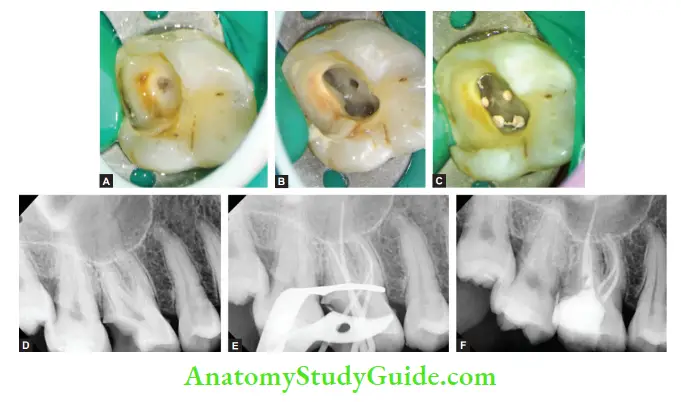
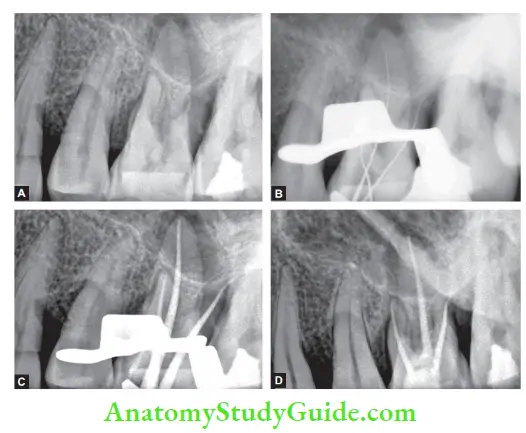
- (A) Preoperative photograph;
- (B) Pulp chamber showing four canals viz; MB1, MB2, distal and palatal;
- (C) Post obturation photograph;
- (D) Preoperative radiograph showing deep caries in maxillary fist molar with pulp involvement;
- (E) master cone radiograph;
- (F) Obturation radiograph
A second distal canal is suspected when it does not lie in the midline of the tooth. Two canals in mandibular incisors are reported in 41% of the cases, and among mandibular premolars, more than 11% of teeth show the presence of two canals.
Extra Root or the Missing Root:
It is a rare condition which affcts less than 2% of permanent teeth. Radix entomolaris was first described by Carabelli. It is commonly seen in mandibular molars and is characterized by the presence of an additional root, typically found distolingually.
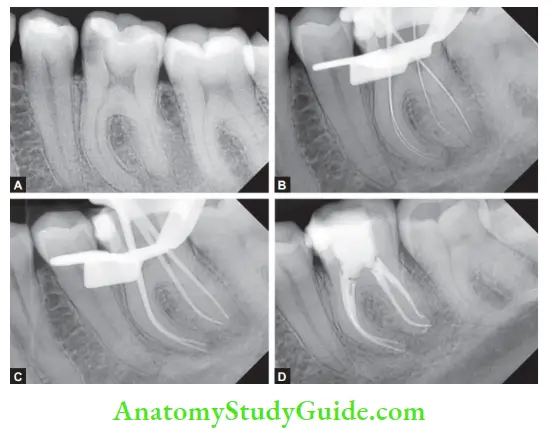
- (A) Mandibular 1st molar with irreversible pulpitis;
- (B) Working length radiograph;
- (C) Master cone radiograph;
- (D) Post obturation radiograph.

- (A) Preoperative radiographs 36 and 46;
- (B) Working length radiograph of 36 and 46;
- (C) Master cone radiograph of 36 and 46;
- (D) Post-obturation radiograph of 36 and 46.
Dens in Dente or Dens Invaginatus:
This condition represents an exaggeration of the lingual pit. Most commonly seen in permanent maxillary lateral incisors, this condition may range from being superficial, that is, involving only the crown part to a pit in which both crown and root are involved. A tooth with dens invaginatus has a tendency of plaque accumulation which predisposes it to early decay and pulpitis.

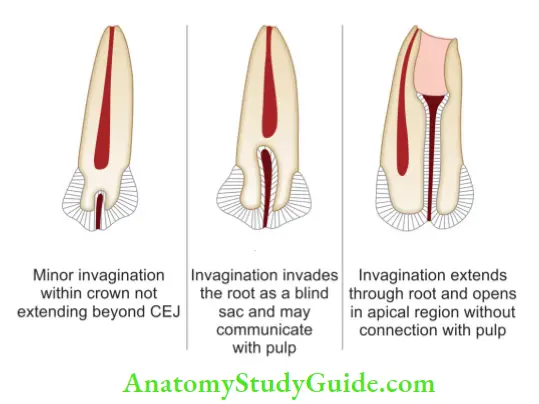
Types of dens invaginatus (according to Oehlers):
- Type 1: Here, minor invagination occurs within the crown and does not extend beyond CEJ.
- Type 2: Here invagination invades the roof as a blind sac and may or may not communicate with pulp.
- Type 3: Here invagination extends through the root and opens in the apical region without connection with the pulp.
Dens Evaginatus:
In this condition, an anomalous tubercle or cusp is located on the occlusal surface. Because of occlusal abrasion, this tubercle wears of fast causing early exposure of accessory pulp horn that extends into the tubercle.
This may further result in periarticular pathology in otherwise caries-free teeth even before the completion of the apical root development. This condition is commonly seen in premolar teeth.
Variation in the shape of Pulp Cavity:
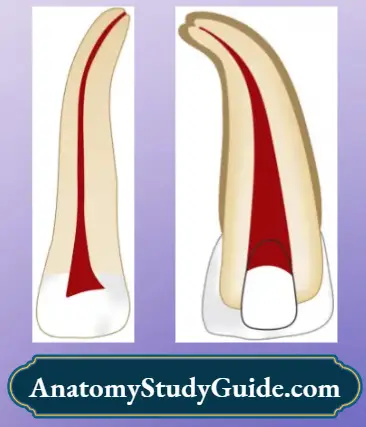
Curved Canals:
Curvature in the canal can be gradual (root canal gradually curves from orifice to the apical foramen)or apical (root canal is generally straight but at apex, it shows a curve, commonly seen in maxillary lateral incisors and mesiobuccal root of maxillary molars)
Classification of Curved Canals:
Determination of Canal Curvature:
Periapical radiographs:
Though radiographs can be used to assess the root curvature, misinterpretation can occur because radiographs produce a two-dimensional image of a three-dimensional object. Curvatures present buccolingually may not be visible on radiographs.
Cone beam computed tomography (CBCT):
CBCT helps in assessing the true size, extent, nature, and position of the lesions as compared to conventional radiography.
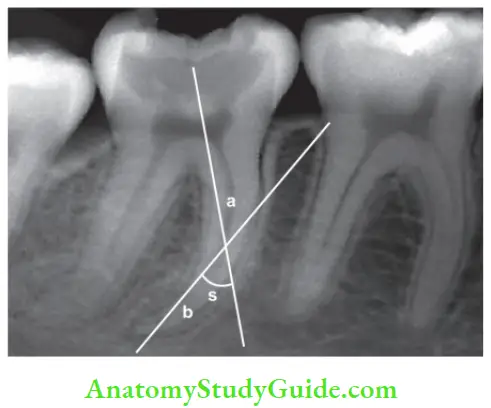
Schneider’s method:
In Schneider’s method of finding root curvature, a straight line is drawn along the coronal third of the canal and marked as A. Second line is drawn from the apical foramen to intersect the point where the first line left the long axis of the canal. The angle formed by the intersection of these lines is measured as Schneider’s angle.
Schneider’s classification on the basis of the degree of curvature:
- Straight: 5° or less
- Moderate: 10–20°
- Severe: 25–70°
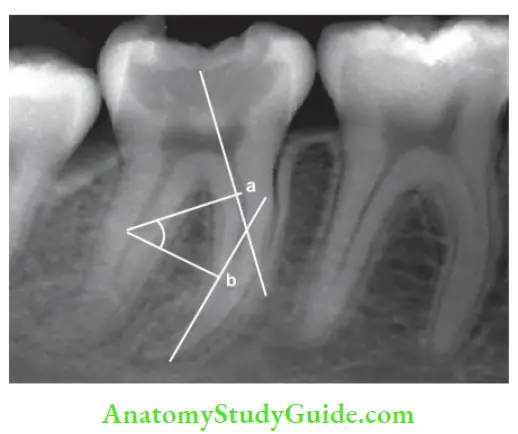
Weine’s method
It is similar to Schneider’s method but shows the differences in the angles according to the curvature of the canal. In this method, a straight line is drawn from the canal orifices to the point of curvature, and a second line is drawn from the apex for the apical curvature, and the angle is measured at the point of intersection between the two lines.
C-shaped Canal
- These are called C-shaped due to their morphology as the pulp chamber appears single ribbon-shaped with an arc of 180° or more. These are commonly seen in mandibular second molars and then in maxillary first molars and mandibular premolars, especially when the roots of these teeth appear very close or fused.
- Pulp chambers of teeth with C-shaped canals have greater apical-occlusal width with low bifurcation. This results in a deep pulp chamber flor
- The root canal system shows broad, fan-shaped communications from the coronal to the apical third of the canal. The canal changes shape from the coronal aspect of the root. For example, a continuous C-shaped canal would change to a semicolon configuration in the midfoot and become a continuous C-shape in the apical third of the root or vice versa
Classification:
Melton’s classification
It is based on a cross-sectional shape.
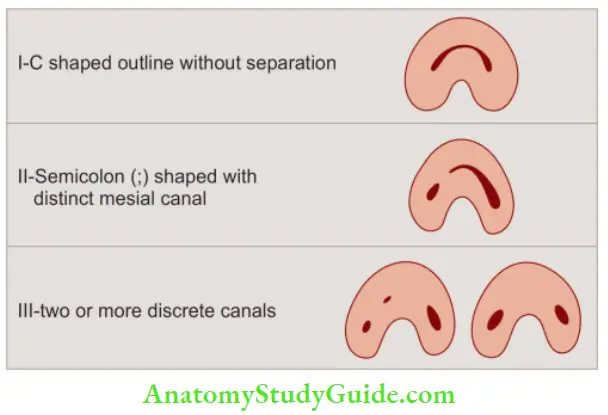
- Category 1: Continuous C-shaped canal running from the pulp chamber to the apex defies a C-shaped outline without any separation
- Category 2: Semicolon shaped (;) in which dentin separates the main C-shaped canal from a mesial distinct canal
- Category 3: Refers to two or more discrete and separate canals
- Subdivision 1: C-shaped orifice in the coronal third that divides into two or more discrete and separate canals that join apically
- Subdivision 2: C-shaped orifice in the coronal third that divides into two or more discrete and separate canals in the midfoot to the apex
- Subdivision 3: C-shaped orifice that divides into two or more discrete and separate canals in the coronal third to the apex
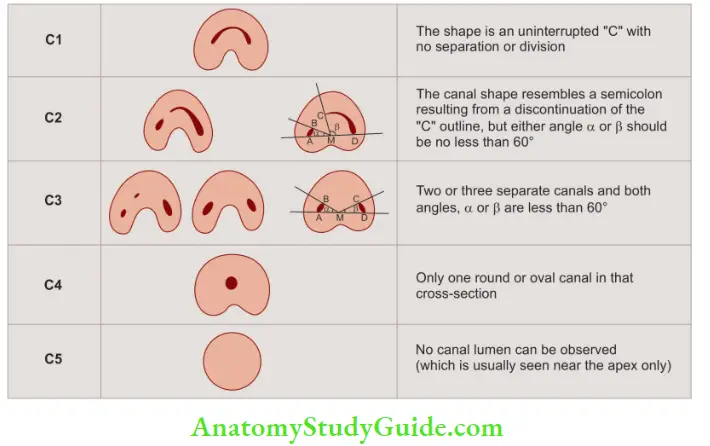
Fan’s classifiation (Anatomic classifiation):
Fan et al. in 2004 modified Melton’s classification into the
following categories:
- Category 1 (C1): Th shape with an interrupted “C” with no separation or division
- Category 2 (C2): Th canal shape resembles a semicolon resulting from a discontinuation of the “C” outline but either angle α or β should not be less than 60°
- Category 3 (C3): Two or three separate canals and both angles, α and β, were less than 60°
- Category 4 (C4): Only one round or oval canal in that cross-section
- Category 5 (C5): No canal lumen can be observed (which is usually near the apex only)
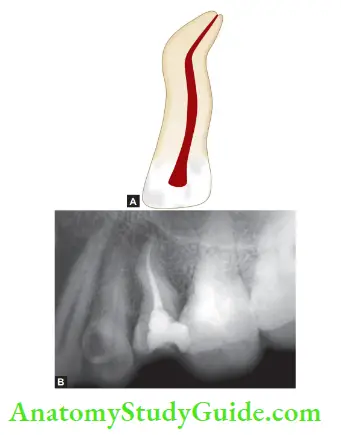
Bayonet/S-shaped Canal:
S-shaped or bayonet-shaped canals pose great problems while endodontic therapy, since they involve at least two curves, with the apical curves having maximum deviations in anatomy. These double-curved canals are usually identifid radiographically if they cross in a mesiodistal direction.
If these traverse in a buccolingual direction, they are recognized using multiangled radiographs, or when the initial apical file is removed from the canal and simulates multiple curves. S-shaped canals are commonly found in maxillary lateral incisors, maxillary canines, maxillary premolars, and mandibular molars.
Sickle-shaped Canals:
In this, the canal is sickle-shaped. It is commonly seen in mandibular molars. The cross-section of this canal is ribbon-shaped.
Variation in Pulp Cavity Due to Pathology:
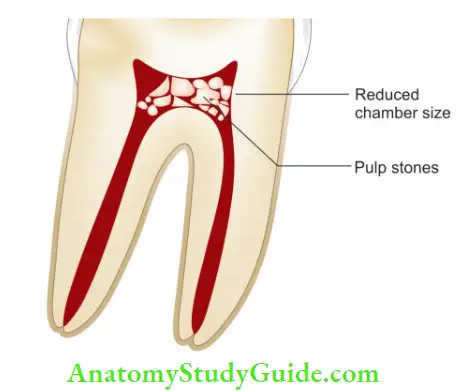
Pulp Stones and Calcifiations:
Pulp canal obliteration is a pulpal response to trauma which is characterized by the deposition of hard tissue within the root canal space
It is characterized by osteoid tissue that is produced by the odontoblasts at the periphery of pulp space or undifferentiated pulpal cells that undergo differentiation. This results in the deposition of dentin-like tissue along the periphery of the pulp space and within the pulp space, causing obliteration of the pulp chamber and canal.
The presence of pulp stones may alter the internal anatomy of the pulp cavity, making the access opening difficult.
Calcifi Metamorphosis:
Calcific metamorphosis is defined as a pulpal response to trauma that is characterized by the deposition of hard tissue within the root canal space. The most common etiology is a traumatic injury resulting in the tooth with a darker hue and yellow color because of a decrease in translucency and greater thickness of dentin under the enamel.
Hard tissue is an osteoid tissue which is produced by the odontoblasts and undifferentiated mesenchymal cells that undergo differentiation because of traumatic injury. This results in the deposition of dentin-like tissue within and around the periphery of the pulp space.
These tissues eventually fuse with one another, resulting in partial or complete obliteration of the root canal space. Radiographically, it appears as partial or total obliteration of canal space.
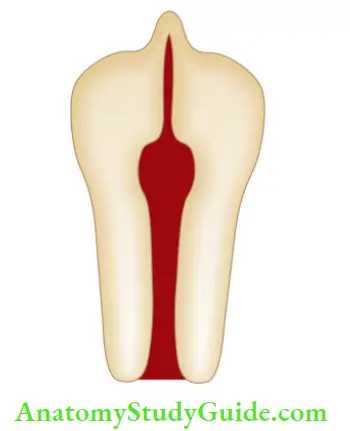
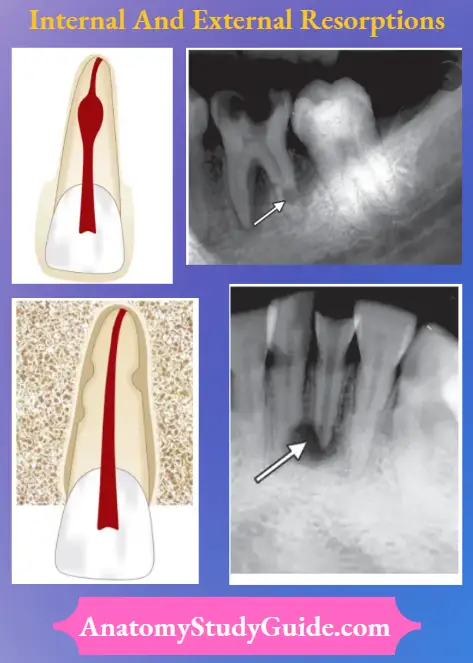
Internal Resorption:
“Internal resorption is an unusual form of tooth resorption that begins centrally within the tooth, initiated in most cases by a peculiar inflammation of the pulp.” It is characterized by an oval-shaped enlargement of root canal space. It is commonly seen in maxillary central incisors but can affect any tooth in the arch.
External Resorption:
External root resorption is initiated in the periodontium and affects the external or lateral surface of the root.
Variation in Apical third:
Diffrent Locations of Apical Foramen:
Apical foramen may exit on the mesial, distal, buccal, or lingual surface of the root. It may also lie 2-3 mm away from the anatomic apex.
Accessory and Lateral Canals:
These are lateral branches of the main canal that form a communication between the pulp and periodontium. They can be seen anywhere from furcation to the apex but tend to be more common in the apical third of posterior teeth.
Open Apex:
It occurs when there is periapical pathology before completion of roof development or as a result of trauma or injury causing pulpal exposure. In this, the canal is wider at the apex than at the cervical area. It is also referred to as a blunderbuss canal. In vital teeth with open apex, treatment is abiogenesis, and in nonvital teeth, it is apexification.

Variation in size of Root:
Macrodontia:
In this condition, pulp space and teeth are enlarged throughout the dentition. This condition is commonly seen in gigantism.
Microdontia:
In this condition, pulp space and teeth appear smaller in size. It is commonly seen in cases of dwarfism.
Factors Affecting Internal Anatomy
The internal anatomy of teeth reflects the tooth form, yet various environmental factors whether physiological or pathological affect its shape and size because of pulpal and dentinal reactions to them. These factors can be enlisted as
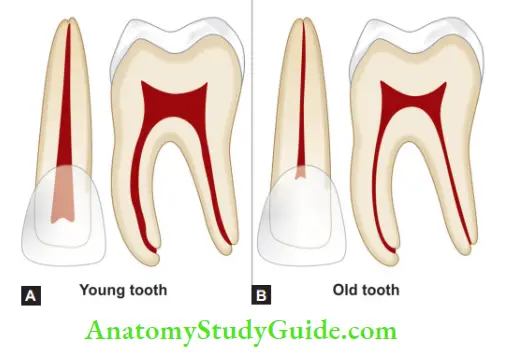
Age:
With advancing age, there is continued dentin formation causing regression in the shape and size of the pulp cavity. Clinically, it may pose problems in locating the pulp chamber and canals.
Irritants:
Various irritants like caries, periodontal disease, attrition, abrasion, erosion, cavity preparation, and other operative procedures may stimulate dentin formation at the base of tubules resulting in a change in the shape of the pulp cavity.
Calcific metamorphosis:
It commonly occurs because of trauma to a recently erupted tooth.

Calcifications:
Pulp stones or diffuse calcifications are usually present in the chamber and the radicular pulp. These alter the internal anatomy of teeth and may make the process of canal location difficult.
Resorption:
Chronic inflammation or internal resorption may result in a change of shape of the pulp cavity making the treatment of such teeth challenging.
Individual Tooth Anatomy
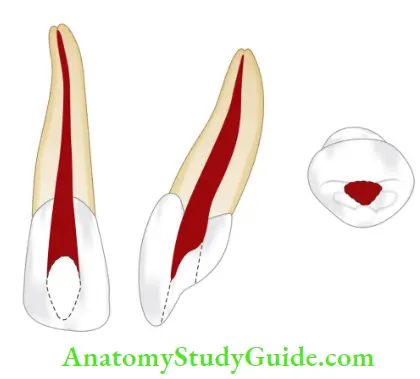
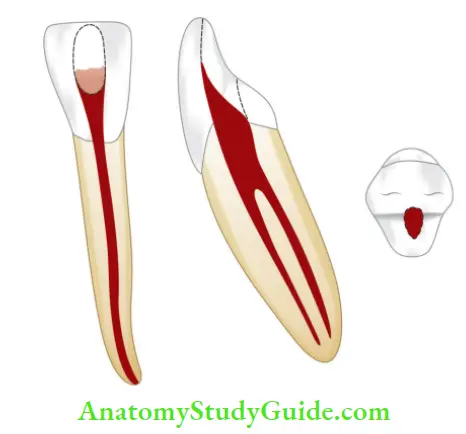
Maxillary Central Incisor:
It has a single root with a single canal system. Canal form is usually Type 1.
- Average length: 22.5 mm
- Average crown length: 10.5 mm
- Average root length: 12 mm
- Average pulp volume: 12.4 mm3
Pulp Chamber:
- Located in the center of the crown and equidistant from the dentinal walls
- Mesiodistally broad with the broadest part facing initially
- In young patients, it shows three pulp horns correspond to enamel mamelons on the incisal edge
Root Canal:
- Usually one root with one straight root canal
- Cross-section of canal
- In the cervical/coronal part: ovoid
- Middle third: ovoid or round
- Apical third: round
Commonly Found Anomalies:
- Palatogingival groove
- Talon’s cusp
- Fusion
- Gemination
Clinical Considerations:
- Pulp horn can be exposed following a relatively small fracture of an incisal corner in the young patient
- Placing the access cavity too far palatally makes straight-line access difficult
- Most canals are straight, but 15% -20% of roots show the labial or palatal curve
- Labial perforation is most commonly seen during access cavity preparation
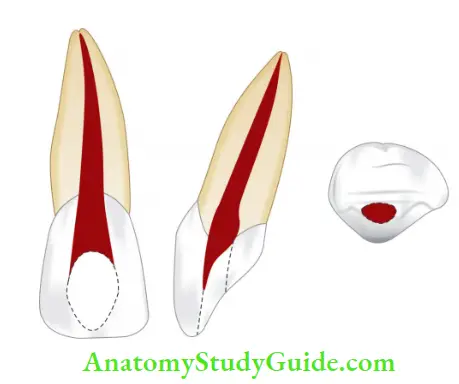
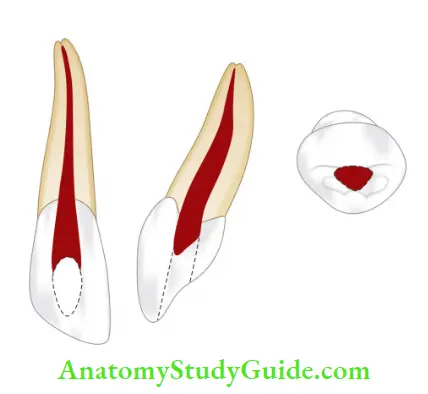
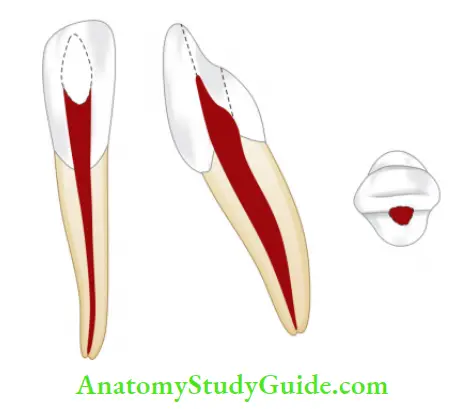
Maxillary Lateral Incisor:
It has a single root with a single canal system. Canal form is usually Type 1.
- Average length: 21.5 mm
- Average crown length: 9 mm
- Average root length: 12.5 mm
- Average pulp volume: 11.4 mm3
Pulp Chamber:
It is similar to a central incisor except that
- The incisal outline is more rounded
- Two pulp horns are present
Root Canal:
- A single root with a smaller canal is seen when compared to the central incisor
- Cross-section of canal
- In the cervical/coronal part: ovoid
- Middle third: ovoid to round
- Apical third: round
- The apical region of the canal is usually curved in a palatal direction
Commonly Found Anomalies:
- Palatogingival groove
- Peg laterals
- Fusion
- Gemination
- Dens invaginatus
Clinical Considerations:
- Cervical constriction is removed during coronal preparation to have a straight-line access
- Palatal curvature of the apical part can cause ledge formation, complicate surgical procedures like root end cavity preparation and root resection
- Lateral canals are more common than maxillary central incisors
- Labial perforation is a common error during access cavity preparation
Maxillary Canine:
It has a single root with a single canal system. Canal form is usually Type 1.
- Average length: 27 mm (longest tooth)
- Average crown length: 10 mm
- Average root length: 17 mm
- Average pulp volume: 14.7 mm3
Pulp Chamber:
- Labiopalatally, pulp chamber is almost triangular in shape with apex pointed initially
- Mesiodistallys it is narrow, resembling a flame
- One pulp horn corresponding to one cusp is seen
Root Canal
- A single root canal which is wider labiopalatally than mesiodistally
- Cross-section of canal
- In the cervical/coronal part: ovoid
- Middle third: ovoid
- Apical third: round
- The cross-section at the cervical and middle third show its oval shape, and at the apex it becomes circular
Commonly Found Anomalies:
- Dens invaginatus
- Dilacerations
- Two roots with two canals
Clinical Considerations:
- Cervical constriction needs to be shaped during uniformly tapered preparation
- Surgical access sometimes becomes difficult because of the long length of the tooth
- 32% of canals may show distal apical curvature
- Abscess of maxillary canine perforates the labial cortical plate below the insertion of levator muscles of the upper lip and drains into the buccal vestibule
- If perforation occurs above the insertion of levator muscles of the lip, drainage of abscess occurs into the canine space, resulting in cellulitis
Maxillary First Premolar
It has two roots with two canals. Canal form is usually Type 1.
- Average length: 21.5 mm
- Average crown length: 8.5 mm
- Average root length: 14 mm
- Average pulp volume: 18.2 mm3

Pulp Chamber:
- It is wider buccopalatally with two pulp horns, corresponding to buccal and palatal cusps
- The palatal canal is usually larger than the buccal canal
- The roof of pulp chamber is coronal to the cervical line
- The floor is convex with two canal orifices
Root Canal:
- Two roots with two canals are seen commonly. In the case of fused roots, a groove running in occlusoapical direction divides the roots into buccal and palatal portions each containing a single canal
- The buccal canal is directly under the buccal cusp and the palatal canal is directly under the palatal cusp
- Cross-section of the canal:
- In the cervical/coronal part: ovoid
- Middle third: round
- Apical third: round
Commonly Found Anomalies:
- Dens evaginates
- Dilacerations
Clinical Considerations:
- Good quality radiograph with different angulations is taken to avoid superimposition of canals
- Avoid overflying of the coronal part of the buccal root to avoid the perforation of the mesial groove present on it
- Failure to observe distoaxial inclination of the tooth may lead to perforation
- The palatal canal is usually larger than the buccal canal
Maxillary Second Premolar
It has a single root with a single canal system. Canal form is usually of Type 1 and Type 2.
- Average length: 21.5 mm
- Average crown length: 8.5 mm
- Average root length: 13 mm
- Average pulp volume: 16.5 mm3
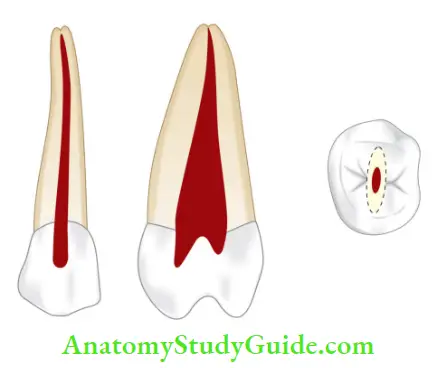
Pulp Chamber:
- One root with a single canal is most commonly seen
- The pulp chamber is wider buccopalatally and narrower mesiodistally
- The cross-section shows a narrow and ovoid shape
Root Canal:
- In more than 60% of cases, a single root with a single canal is found
- If two canals are present, they may be separated along the entire length of the root or merge to form a single canal as they approach apically
- Cross-section of the canal:
- In the cervical/coronal part: ovoid
- Middle third: round
- Apical third: round
Commonly Found Anomalies:
- Dens invaginatus
- Taurodontism
- Two roots with two or three canals
Clinical Considerations:
- The narrow ribbon-like canal is difficult to clean and obturate
- If one canal is present, orifice is indistinct, but if two canals are present, two orifices are seen
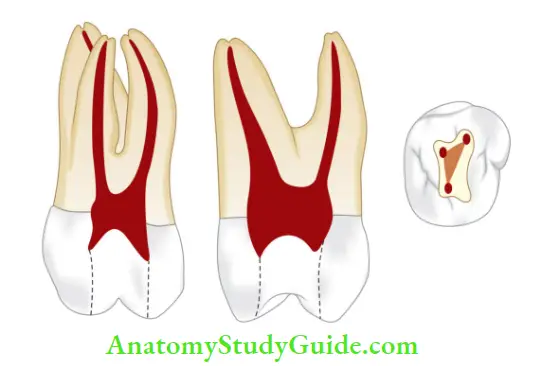
Maxillary First Molar
It has three roots with three to four canals.
- Average length: 21.3 mm
- Average crown length: 7.5 mm
- Average root length: 14 mm
- Average pulp volume: 68.2 mm3
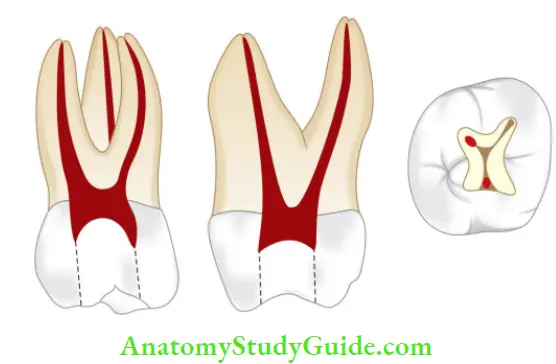
Pulp Chamber:
- Largest pulp chamber
- Four pulp horns, namely, mesiobuccal, mesiopalatal, distobuccal and distopalatal
- The bulk of the pulp chamber lies mesial to the oblique ridge
- Pulp horns are arranged to give a rhomboidal shape in the cross-section
- The roof converges and the lingual wall disappears, forming a triangular form
- Orifices of root canals are located in the three angles of the floor; the palatal orifice is the largest and easiest to locate and appears funnel-like in the flor of the pulp chamber
- The distobuccal canal orifice is located more palatally than the mesiobuccal canal orifice
- More than 80% of teeth show the presence of two canals in the mesiobuccal root. MB 2 is located 3 mm palatally and 2 mm mesially to the MB1 orifice
Root Canal:
- The roots with three or four canals
- Two canals in the mesiobuccal root are closely interconnected and sometimes merge into one canal
- The mesiobuccal canal is the narrowest of the three canals, flattened in the mesiodistal direction at the cervix but becomes round as it reaches apically. Distal curvature is seen in more than 78% of the canals
- The distobuccal canal is a narrow, tapering canal, sometimes flattened in mesiodistal direction but generally, it is round in cross-section
- The palatal root canal has the largest diameter which has a rounded triangular cross-section coronally and becomes round apically
- The palatal canal can curve buccally in the apical one third
- Lateral canals are found in 40% of the molars at the apical third and at the trifurcation area
Anomalies present:
- Two palatal canals
- Two palatal roots
- Two distal canals
- Taurodontism
Clinical Considerations :
- Buccal curvature of the palatal canal (56% of cases) may not be visible on radiographs, leading to procedural errors
- MB 2 should be approached from distopalatal angle since the initial canal curvature is mesial
- Sometimes isthmus is present between mesiobuccal canals and should be cleaned properly for successful treatment
- The Fundus of the alveolar socket of the maxillary first molar may protrude into the maxillary sinus, producing a small, bony prominence in the floor of sinus
- Because of close proximity to the sinus, pulpal inflammation can result in sinusitis.
- Since the pulp chamber lies mesial to the oblique ridge, the pulp cavity is made mesial to the oblique ridge
- Perforation of the palatal root is commonly caused by assuming the canal to be straight
- (A) Preoperative radiograph;
- (B). Working length radiograph;
- (C) Master cone radiograph;
- (D) Post- obturation radiograph.
Maxillary Second Molar:
It has three roots with three to four canals almost similar to first molar.
- Average length: 17.5 mm
- Average crown length: 7 mm
- Average root length: 12.5 mm
- Average pulp volume: 44.3 mm3
Pulp Chamber:
- Similar to the first molar except that it is narrower mesiodistally
- The roof is more rhomboidal in cross-section and floor is an obtuse triangle
- Mesiobuccal and distobuccal canal orifices lie very close to each other, sometimes all the three canal orifices lie in a straight line
Root Canal
Similar to the first molar except that roots tend to be less divergent and may be fused.
Anomalies present:
- Two palatal canals and two palatal roots
- Fusion of roots
- Taurodontism
Clinical Considerations:
- Similar to maxillary first molar
- The maxillary second molar lies closer to the maxillary sinus than first molar
Maxillary Third Molar:
- Average length: 16.5 mm
- Average crown length: 6.5 mm
- Average root length: 12 mm
- Average pulp volume: 40.3 mm3
Pulp Chamber and Root Canal:
It is similar to the second molar but displays great variations in shape, size, and form of pulp chamber with the presence of one, two, three or more canals at times.
Clinical Considerations:
The maxillary third molar is closely related to the maxillary sinus and maxillary tuberosity.
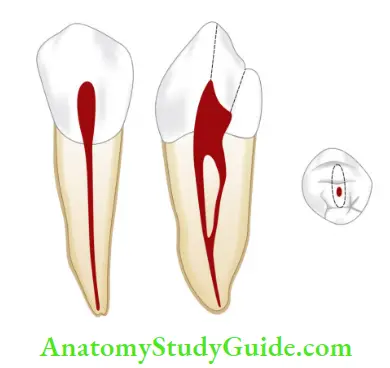
Mandibular Central Incisor:
It is the smallest tooth in the arch. It has a single root with Type 1 canal configuration most prevalent, Type 2 and 3 less common.
- Average length: 21 mm
- Average crown length: 9 mm
- Average root length: 12 mm
- Average pulp volume: 6.1 mm3
Pulp Chamber:
- It is wider labiolingually than mesiodistally
- The cross-section shows an ovoid shape
Root Canal:
There can be
- Single canal with one foramen in 65% of cases
- Two canals with one foramen in 28% of cases and two canals with separate foramen in 7% of cases
Cross-Section of Canal:
- In the cervical/coronal part: ovoid
- Middle third: ovoid
- Apical third: round
Since the canal is flat and narrow mesiodistally and wide buccopalatally, the ribbon-shaped configuration is formed.
Commonly Found Anomalies:
- Dens invaginatus
- Germination
- Fusion
Clinical Considerations:
- Because of grooves along the length of the root and narrow canals, weakening of the tooth structure or chances of strip perforations are increased
- It is common to miss the presence of two canals on a preoperative radiograph if they are superimposed
- The second canal is usually found lingual to the main canal
- Since apex of the mandibular central incisor is inclined lingually, surgical access may become difficult to achieve
Mandibular Lateral Incisor
- Average length: 22.5 mm
- Average crown length: 9.5 mm
- Average root length: 13.0 mm
- Average pulp volume: 7.1 mm3
Pulp Chamber:
It is similar to a central incisor except that it has larger dimensions.
Root Canal:
- Similar to central incisor
- The root is straight or distally curved
Cross-Section of Canal:
- In the cervical/coronal part: ovoid
- Middle third: ovoid
- Apical third: round
Clinical Considerations:
Thse are similar to central incisor.
Mandibular Canine:
It has a single root with a single canal system. Canal form is usually Type 1 and rarely has two roots but may display Type 4 configuration.
- Average length: 25.5 mm
- Average crown length: 11 mm
- Average root length: 16 mm
- Average pulp volume: 14.2 mm3
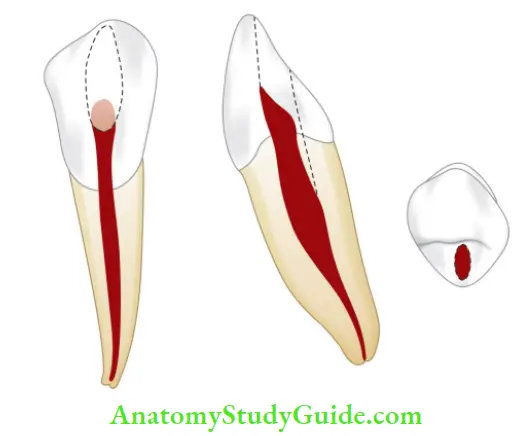
Pulp Chamber:
- Ovoid in cross-section broader labiolingually and narrower mesiodistally
- One pulp horn present
Root Canal:
It has one root and one canal in 94% of cases but two roots with separate foramen are present in 6% of cases
Cross-Section of Canal:
- In the cervical/coronal part: ovoid
- Middle third: ovoid
- Apical third: round
Commonly Found Anomalies
- Dilaceration
- Dens invaginatus
- Two roots with two canals
- Two canals in a single root
Mandibular First Premolar:
It has a single root with a single canal but occasionally division of root is present in the apical third.
- Average length: 21.5 mm
- Average crown length: 8.5 mm
- Average root length: 13.5 mm
- Average pulp volume: 14.9 mm3
Pulp Chamber:
- Buccolingually, wider and ovoid in cross-section
- Mesiodistally narrow
- Two pulp horns are present, the buccal horn being the more prominent
Root Canal:
- One root and one canal is commonly seen (70%), and one canal and two foramina are seen in 24% of cases
- Lateral canals are present in 44% of cases
Cross-Section of Canal:
- In the cervical/coronal part: ovoid
- Middle third: round
- Apical third: round
Commonly Found Anomalies:
- Dens evaginates
- Dens invaginatus
- Two roots with two canals
- Single root splits into two, of which buccal is straight and lingual splits at a right angle, giving the letter “h” appearance

Clinical Considerations:
- Surgical access to the apex of the mandibular first premolar is often complicated due to the proximity of the mental nerve
- Due to close proximity of the root apex to the mental foramen, one may mimic its radiographic appearance to periapical pathology
- The lingual canal when present, is difficult to the instrument. Access can usually be gained by running a fine instrument down the lingual wall of the main buccal canal until the orifice is located
- Perforation at distogingival margin is caused by failure to recognize the distal tilt of the premolar
Mandibular Second Premolar
- Average length: 22.5 mm
- Average crown length: 8 mm
- Average root length: 14.5 mm
- Average pulp volume: 14.9 mm3

Pulp Chamber:
- It is similar to the fist premolar except that the lingual pulp horn is more prominent
- The cross-section shows an oval shape with greater dimensions buccolingually
Root Canal:
Usually, only one root and one canal is seen, but in 11% of the cases, a second canal can be seen.
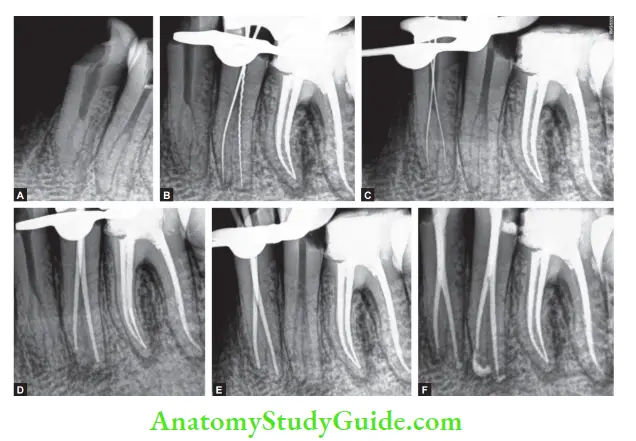
- (A) Preoperative radiograph;
- (B) working length radiograph of fist premolar;
- (C) working length radiograph of the second premolar;
- (D) Master cone radiograph of fist premolar;
- (E) Master cone radiograph of second premolar;
- (F) Post obturation radiograph.
Cross-Section of Canal:
- In the cervical/coronal part: ovoid
- Middle third: less ovoid
- Apical third: round
Clinical Consideration:
They are similar to mandibular first premolar.
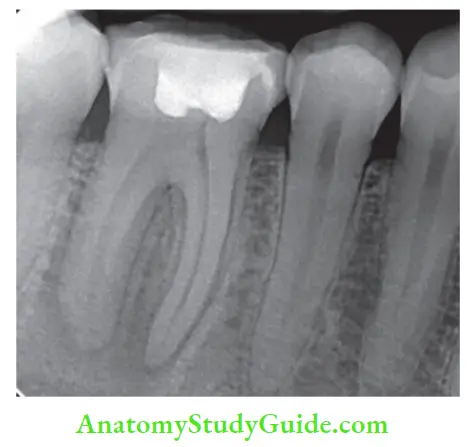
Mandibular First molar
It has two roots with three to four canals.
- Average length: 21.5 mm
- Average crown length: 7.5 mm
- Average root length: 14 mm
- Average pulp volume: 52.4 mm3
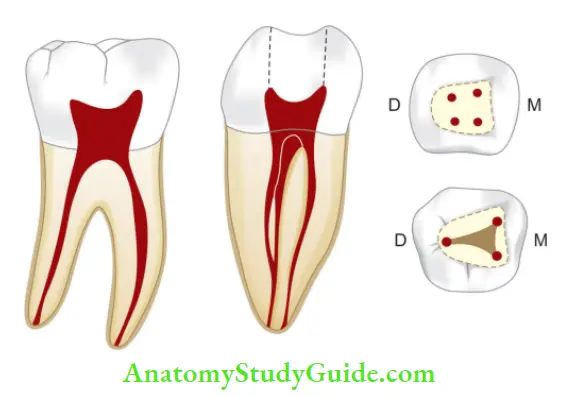
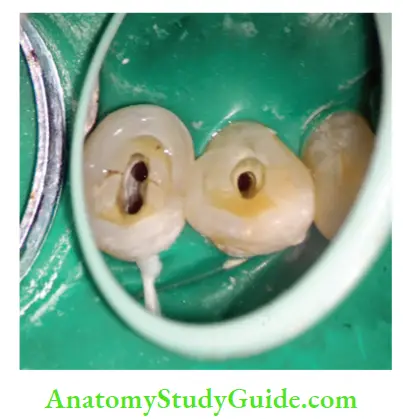
Pulp Chamber:
- It is quadrilateral in cross-section at the level of the pulp floor being wider mesially than distally
- The roof is rectangular in shape with straight mesial and rounded distal walls. Walls converge to form rhomboidal flor
- Four or five pulp horns are present
- Mesiobuccal orifice is present under the mesiobuccal cusp
- The mesiolingual orifice is located in a depression formed by the mesial and lingual walls
- The distal orifice is the widest of all three canals. It is oval in shape with a greater diameter in a buccolingual direction
Root Canal:
- Two roots with three canals are present, but three roots and four or fie canals are also seen
- Mesial root has two canals, namely, mesiobuccal and mesiolingual which may exit in two foramina (>41% cases), single foramen (30%), and in different pattern
- The mesiobuccal canal is usually curved and often exits in the pulp chamber in a mesial direction
- Distal root has one canal in >70% of cases, but two canals are also seen in some cases
- The single distal canal is ribbon-shaped and has a larger diameter buccolingually. But when two canals are present in the distal root, they tend to be round in the cross-section
Anomalies present:
- Taurodontism
- Radix entomolaris—supernumerary roots
- C shaped canals
Clinical Considerations;
- Over-enlargement of mesial canals should be avoided to prevent procedural errors
- To avoid superimposition of the mesial canals, a radiograph should be taken at an angle
Mandibular Second Molar
It has two roots with three canals.
- Average length: 21.5 mm
- Average crown length: 7 mm
- Average root length: 13.5 mm
- Average pulp volume: 32.9 mm3
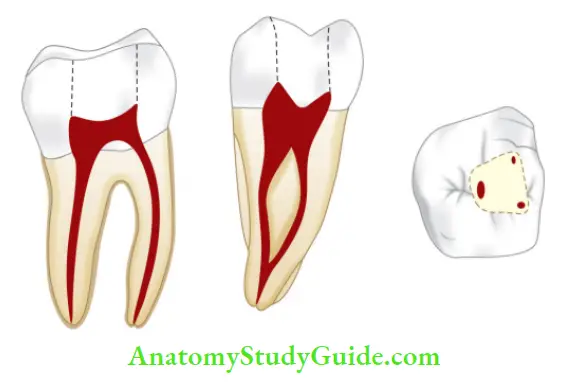
Pulp Chamber:
- It is similar to the first molar but smaller in size
- Root canal orifices are smaller and lie closer
Root Canal:
- Two roots with two or three canals are seen. If two canals are seen, both orifices are in mesiodistal midline
- If two orifices are not in the mesiodistal midline, one should search for another canal on the opposite side
Anomalies present:
- C-shaped canals, that is, mesial and distal canals become fused into a fi
- Taurodontism
- Fused roots
- Single canal
- Radix entomolaris
Clinical Considerations:
- C-shaped canals should be treated with proper care
- Perforation can occur at mesiocervical region if one fails to recognize the mesially tipped molar
Mandibular Third Molar:
Average Tooth Length:
- Average length: 17.5 mm
- Average crown length: 6 mm
- Average root length: 11.5 mm
- Average pulp volume: 44.4 mm3
Pulp Chamber and Root Canals:
Pulp cavity resembles the fist and second molar but with enormous variations, that is, the presence of one, two, or three canals and a “C-shaped” root canal orifices
Clinical Considerations:
- The root apex is closely related to the mandibular canal
- The alveolar socket may project onto the lingual plate of the mandible
Internal Anatomy Conclusion
For successful and predictable endodontics, apart from correct diagnosis and treatment planning, the clinician must have knowledge of the internal anatomy of the tooth. The populations around the world have some peculiarities which must be taken care of. Anatomical variations can occur in any tooth.
This necessitates the use of more precise technology to complete evaluation and treatment planning. The frequencies of the root, root canals, and apical foramina should be taken care of for individual teeth because outcomes of non-surgical and surgical endodontic procedures are influenced by highly variable anatomic structures.
Therefore clinicians should be aware of complex root canal structures, dimensions, and alterations of canal anatomy
Leave a Reply