Intussusception Definition
Invagination of one segment of the intestine into another (usually the proximal into distal) is called intussusception.
Incidence: 2–4/1000 live births.
Intussusception Types
- Simple ileocolic is the most common type, followed by ileoileal or colocolic.
- Compound—ileo-ileocolic
- Retrograde jejunogastric intussusception, a complication of gastrojejunostomy (GJ) is a rare but interesting type of intussusception
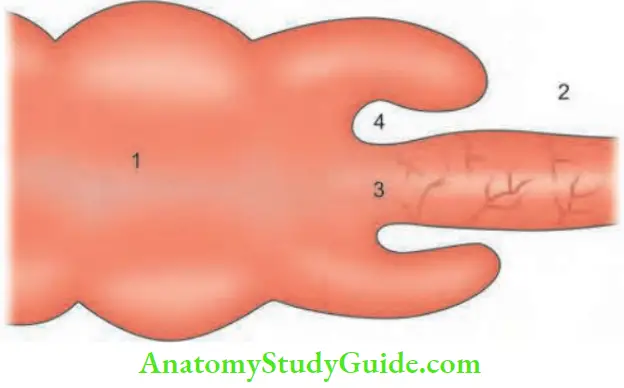
Intussusception Parts
- Intussuscipiens: It is the outer tube (distal bowel which receives the intestine).
- Intussusceptum: Proximal bowel (inner tube) which enters the distal segment.
- Apex: Apex is the part which advances further into the distal bowel.
- Neck: Neck the narrowest portion of intussusception, is the junction of the entering layer with the mass.
The whole mass that develops is called intussusception.
Intussusception Aetiopathogenesis
1. Idiopathic intussusception: Actual cause is not known. It is seen in infants. Possible factors
- Dietary factor: Around the age of 6–9 months, weaning of breast milk is done. Weaning causes alteration in the bacterial flora in the GIT, causing enlargement of the Peyer’s patches. These protrude into the terminal ileum and may precipitate intussusception.
- Infective factor: It usually follows upper respiratory tract infection with virus (adeno rotaviruses) which produce inflammation of Peyer’s patches.
2. Adult intussusception (secondary): In adults, there is always a cause for intussusception.







Predisposing Factors:
- Recent viral infection (upper respiratory)
- Recent operation
- Henoch-Schönlein purpura
- Cystic fibrosis
- Coeliac disease
- Haemophilia
Intussusception Pathophysiology
- As the apex advances, it drags the mesentery containing blood vessels which get obstructed at the neck resulting in mucosal ulcers and haemorrhages.
- Marked lymphadenopathy and hypertrophy of
- Peyer’s patch is found at operation.
- If the neck is too tight, gangrene sets in very early, as in ileocolic intussusception.
- All other features of strangulation, dehydration, distension and septicaemic shock develop later.
Intussusception Clinical Features
- First born male infants between 6 and 9 months are commonly affected. Boys : Girls—3 : 2.
- Child screams with abdominal pain1 (intestinal colic)which is associated with facial pallor.
- One attack of red currant jelly stools is characteristic.
- Bleeding is due to mucosal ulcer (venous infarction).
- Mucus secretion is due to irritation of intestines. This is followed by absolute constipation. Red currant jelly stools are not found in adult intussusception.
- Vomiting 3–4 times, initially due to pylorospasm.
- Later, due to obstruction.
- In between the spasms, the child sleeps but gets up suddenly with pain.


Intussusception Signs
- The mother is asked to feed the baby in sitting position and an examination of the baby’s abdomen is done
- with the left hand, standing in front of the mother.
- A contracting, hardening mass in and around the umbilical region can be felt (sausage-shaped, .60C).
- Emptiness in the right iliac fossa (Dance’s sign— signe de dance).
- There may be a visible step ladder peristalsis.
- Rarely, intussusception can be seen outside the anus due to long mesentery.
- Rectal examination reveals blood-stained mucus on the examining finger.
- Features of peritonitis occur in untreated cases.
Intussusception Investigations
- Ultrasound: Ultrasound is the investigation of choice. It can detect target sign and detect mass (Doughnut sign). With Doppler, it can be used to assess vascularity of the bowel also. Thus, barium enema has become obsolete.
- CT scan: It is the most sensitive imaging modality in the diagnosis of intussusception. Sausage-shaped mass, with blood vessels within bowel lumen are typical findings. Gangrene can be detected.
- Barium enema: ‘Claw (pincer) ending’ is diagnostic of intussusception. This is also called ‘meniscus sign’. If there is any suspicion of gangrene, this test should not be done. In many cases, the diagnosis is established on clinical grounds.


Intussusception Treatment
1. Conservative Treatment:
- Hydrostatic reduction can be attempted when the gangrene is ruled out as in early intussusception. A lubricated catheter is introduced into the rectum and 1–2 litres of saline from a height of 1–2 metres is allowed to run.
- Catheter is removed and the buttocks are pressed together. 50–70% of cases are reduced by this method, 1:3 barium sulphate in warm isotonic saline can also be used.
- Air contrast enema will not reduce gangrenous bowel. Air is pumped into the colon at a pressure of 60–80 mmHg.
Contraindications:
- Peritonitis with shock
- Total intestinal obstruction
Hydrostatic Reduction is Successful when:
- Flatus and faeces are passed with barium
- Child is symptom-free and comfortable
- Small bowel loops are filled with contrast
Advantage: Easy, nonoperative method
Complication: Rarely, colonic perforation
2. Surgical Treatment:
- Laparotomy and reduction of intussusception
- Intussusception is reduced by milking (squeezing) the colon in opposite direction, which is facilitated by breaking the adhesions at the neck using the little finger.
- Appendicectomy is also done, as it avoids any future confusion as to the reason for the abdominal scar. Fixing the caecum is not necessary because idiopathic intussusception rarely recurs. If the loop is gangrenous, resection and ileocolic anastomosis is done.
- Recurrent intussusception is rare: If it occurs, terminal ileum is sutured to the side of the ascending colon.
For some interesting “more common” about intussusception.
Acute Intussusception—Most Common:
- Most common in children between 5 and 10 months of age
- Most common cause of intestinal obstruction in children
- Most common cause is idiopathic (90%)
- Most common variety is ileocolic variety
- Most commonly hypertrophied Peyer’s patches are reported
- Most common type of nonoperative reduction is by using air and barium enema
- Most commonly done surgical procedure is reduction
- Most commonly used noninvasive test for diagnosis is ultrasound—pseudokidney sign, target sign, Duplexassesses vascularity also
- Most incidence of adenovirus infection, common in midsummer and midwinter


Leave a Reply