Isolation Matricing And Wedging Introduction
Paediatric operative dentistry focuses on the early detection of a carious lesion and its prompt intervention. Once the carious lesion is detected, it has to be restored promptly.
Table of Contents
The visibility and accessibility of the working field are essential to restore a carious cavity. A few vital procedures are suggested to enhance visibility and accessibility.
They are isolation, matric and wedging. The endodontic considerations of these procedures have been described in this chapter.
Read And Learn More: Paediatric Dentistry Notes
Isolation
Isolation of the operating field is a prerequisite in paediatric restorative dentistry. This is because children have a short attention span and require shorter appointments for restoration.
Long appointments may evoke undesirable behaviour in the child and thus the treatment may be disturbed. Isolation of the operating field keeps the prepared cavity dry.
When the cavity is dry or free of saliva, contamination of the restorative material used or deterioration of its properties is prevented.
Either the tooth being operated or the segment of the quadrant including the tooth being operated can be isolated from the rest of the oral cavity. A whole quadrant can also be isolated if, situations necessitate.
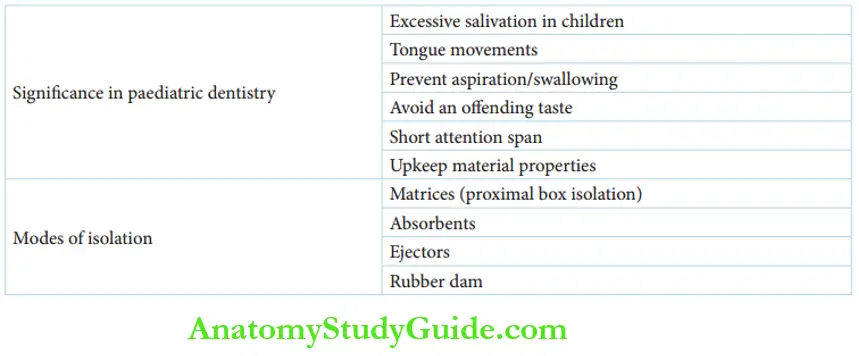
Significance
Isolation is more significant in paediatric dentistry due to the following reasons:
- Children have higher levels of anxiety that promote excessive salivation.
- Inappropriate or undesirable tongue movements are observed in children.
- Chances of aspiration/swallowing of restorative materials or broken instruments or fluids, such as root canal irrigants and aerator coolants, are higher in children.
- The bad taste of the restorative materials or root canal irrigants can be a source of discomfort to the child.
- Excessive salivation can contaminate restorative materials, deteriorating the physical properties and longevity of the materials.
Modes
A rubber dam is the ultimate mode of isolation technique in restorative dentistry. Matrices can be used to keep the proximal box of the prepared cavity free of saliva and gingival crevicular fluid.
Rubber dam application and matric techniques are described in the following text. The other modes of isolation used in paediatric restorative dentistry are as follows:
1. Absorbents: Absorbents commonly used in paediatric dentistry are cotton rolls, gauze pads and absorbent paper blots.
They are placed in the first maxillary molar region at the opening of the parotid gland duct and in the anterior lingual sulcus at the opening of submandibular/sublingual salivary gland ducts to absorb the secretions from the major salivary glands.
Additional pads are placed on the labial, buccal and lingual sulci of the tooth being operated on to dry the secretions from minor salivary glands.
2. Ejectors: Ejectors prevent the pooling of fluids in the floor of the mouth. This helps in the maintenance of a dry operating field.
Fluid ejectors are mounted with plastic or metal suction tips operated on motorised suction apparatus.
Isolation With Rubber Dam
A rubber dam is a comprehensive and efficient mode of isolation in operative dentistry. It was introduced in the nineteenth century by S.C. Barnum. The usage of rubber dams ensures the best restorative care to patients.
The basic apparatus consists of a rubber dam sheet, frame, punch, forceps and clamps. The dam or rubber sheet is spread across the oral cavity. It is held in the oral cavity with the help of Young’s frame.
A punch is used to make holes in the dam around the teeth to be operated. The dam is secured in this position with clamps. The clamp can be worn or removed using pliers.
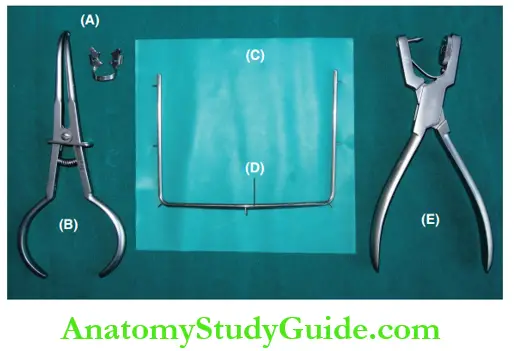
- (A) Ivory no. 3 clamp retainer, commonly used for first and second primary molars.
- (B) Forceps to place the clamp.
- (C) Rubber dam sheet.
- (D) Young’s ‘U’ frame.
- (E) Rubber dam punch.
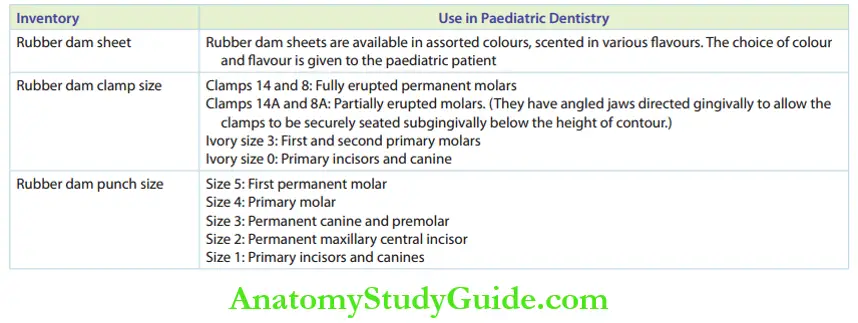
The rubber dam apparatus or inventory can be modified to suit the paediatric patient. The required modifications are enumerated in Table.
Rubber Dam Inventory for Paediatric Dentistry
 The technique of placement and removal of the rubber dam in children is similar to that in adults. A Strategic ‘Tell-Show-Do’ approach can be followed for the placement of rubber dams in children.
The technique of placement and removal of the rubber dam in children is similar to that in adults. A Strategic ‘Tell-Show-Do’ approach can be followed for the placement of rubber dams in children.
Euphemisms are used to allay the anxiety in children while placing the rubber dam. The rubber dam is described as a raincoat and the clamps are described as coat hangers.
Once desensitised, children tend to be more relaxed with the rubber dam in place.
Contraindications
Isolation with a rubber dam is suggested for all children except in the following situations:
- Children wearing a field orthodontic appliance
- A tooth not fully erupted to retain a clamp
- Children with nasal obstructions or constricted nasal passage or upper respiratory tract infections
In children with mouth breathing habits, a 2–3 cm hole is cut in the rubber dam sheet away from the operative quadrant. This allows mouth breathing and does not cause discomfort to the patient.
Matrices
A matrix is a device that functions primarily to confine the restorative material to the axial surfaces of the tooth being restored.
It may be applied to the tooth being restored and fitted around it in part or full.
Marzouk described matric as a procedure where a temporary wall is created opposite to the axial walls surrounding the areas of tooth structure that were lost during cavity preparation.
The matrix provides a stable platform against which the restorative material can be compacted into the proximal cavity.
It creates an appropriate axial contour and establishes an accurate contact around the tooth being restored.
Matrices Advantages
Matrices are used for proximal restorations of primary and permanent teeth. They are not applied for isolated occlusal restorations.
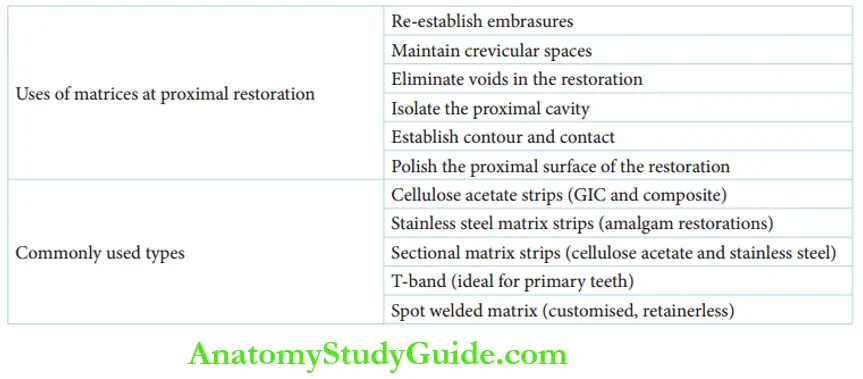
Matricing offers the following advantages:
- Matrices help to re-establish the occlusal or gingival embrasures. Intact embrasures allow the contact areas to be self-cleansable.
- Matrices provide a platform to compact the restorative material, thus eliminating voids in the restoration. This improves the physical properties of the proximal restoration.
- Matrices prevent the impaction of restorative material into the crevicular space.
- They isolate the proximal cavity from saliva and gingival crevicular fluid.
- They prevent overhanging or deficient proximal restoration and establish normal contour and contact.
- The matrix can be used to burnish/polish the proximal surface of the restoration by moving the strip too and forth repetitively in a buccolingual direction.
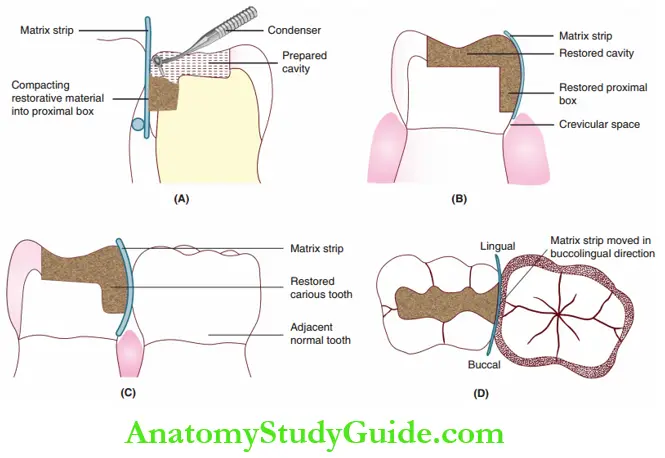
- (A) Restoration material is compacted into the proximal box of the prepared cavity.
- (B) Matrix strip isolates restoration from oral fluids and prevents the impaction of material into the crevicular space.
- (C) Matrix strip establishes the normal contour of restorative material and normal contact with the adjacent tooth.
- (D) Occlusal view of the restored cavity showing the buccolingual movement of the matrix strip for polishing restoration.
Matrix Strips Used In Paediatric Dentistry
The matrix strips that are commonly used in paediatric dentistry are as follows:
- Cellulose acetate preformed matrix strip
- Stainless steel matrix strip
- Sectional matrix strip
- T-band
- Spot welded matrix
Cellulose Acetate Preformed Matrix Strip
Cellulose acetate preformed matrix strips are used for adhesive restorations and resin restorations (glass ionomer cement [GIC] and composites).
They are available in different colours (green, yellow, red and blue) on the basis of width. The preformed strips are customised for use with a pair of sharp curved scissors.
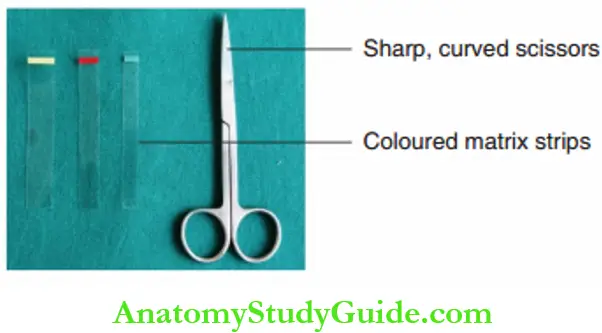
This trip is folded into two along its length. The corner of the folded margin is nipped off with the scissors.
The strip, when unfolded, has a concave outline. This can be appropriately adapted to the convex architecture of the proximal gingiva. It also incorporates a gingival festoon to the matrix strip.
Stainless Steel Matrix Strip
Stainless steel matrix strips are indicated for class 2 restorations. The band strips of varying thicknesses are cut into lengths of 2–3 inches. A Tofflire retainer or an Ivory No. 8 retainer is required to hold the strip around the tooth.
The retainer is kept on the buccal side. A gingival festoon is preferred to simulate the cervical line. It is incorporated into the matrix band with band-cutting scissors.
The final height of the matrix strip used should be 1 mm taller than the cervical-occlusal height of the crown at that proximal surface.
An Ivory no. 1 retainer is a pronged retainer that holds the matrix strip through pre-punched holes on the strip. The matrix strip for this retainer has an elliptical cervical extension and needs no trimming at the gingival end.
The four pairs of pre-punched holes are used to secure the band tightly to the tooth. The Ivory no.1 retainer and band is the most ideal matrix strip for class 2 restoration with a long proximal box.
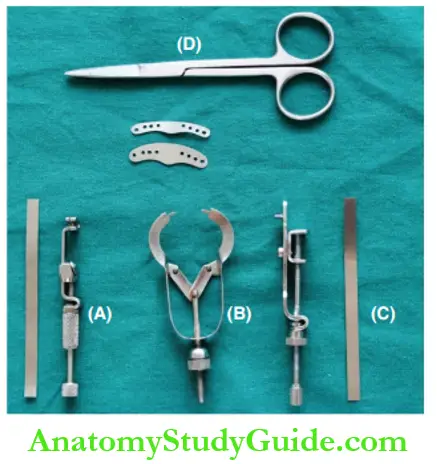
- (A) Ivory no. 8 matrix strip and sectional retainer.
- (B) Ivory no. 1 matrix strip and pronged retainer.
- (C) Universal (Tofflire) matrix retainer and strip.
- (D) Band-cutting scissors.
Sectional Matrix Strip
Sectional matrix strips are used in paediatric operative dentistry as they do not require structured retainers or gingival festooning. These are smaller pieces of matrices of a distorted, semi-lunar shape. They are pliable and can be adapted well to the tooth. They are usually held in place with a wedge or a G-ring.
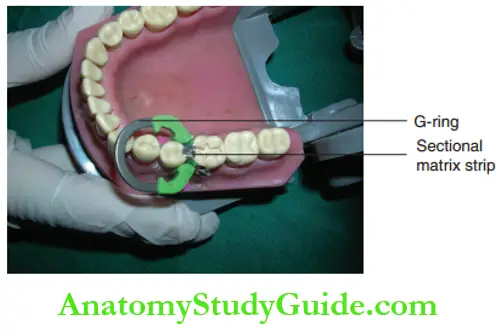
The strips are made of cellulose acetate for anterior proximal restorations with GIC and composite restorations. They are made of stainless steel for posterior amalgam restorations.
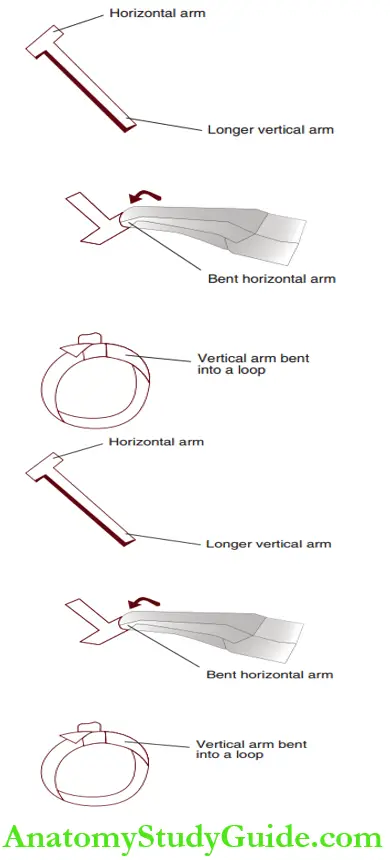
T-band
T-band is a retainer-less matrix system preferred in paediatric operative dentistry. Two sectional unequal pieces of a stainless steel band material are welded in the shape of the letter ‘T’.
It has a longer vertical arm. One-half of the horizontal arm is bent. The bent horizontal portion is kept cervico-occlusally on the buccal side of the tooth. The vertical long arm is run around the tooth and passed into the bent loop.
The other half of the horizontal portion is tucked to secure the long arm snugly onto the tooth. The excess of the long arm is cut leaving a few millimetres. This is tucked over the bent horizontal arm.
To remove the T-band, the tucked residual excess of the long arm is opened up. The bent short arms are straightened and the long arm is unwound.
The T-band is an ideal matrix system for primary teeth due to the following reasons:
- It is a retainer-less matrix system.
- It is a customised matrix system.
- It is easy and simple to fabricate, adapt and remove.
Spot Welded Matrix
Spot welded matrix is a customised, retainers matrix system. Stainless steel matrix band material is adapted around the tooth being restored. It is welded using a spot welder to form a snug-fitting band.
Retainers are not required for the snug-fitting band. Hence, the spot welded matrix is a preferred or ideal matrix system for primary teeth. On the initial set of the restoration, the band is removed using band-removing pliers.
Wedges
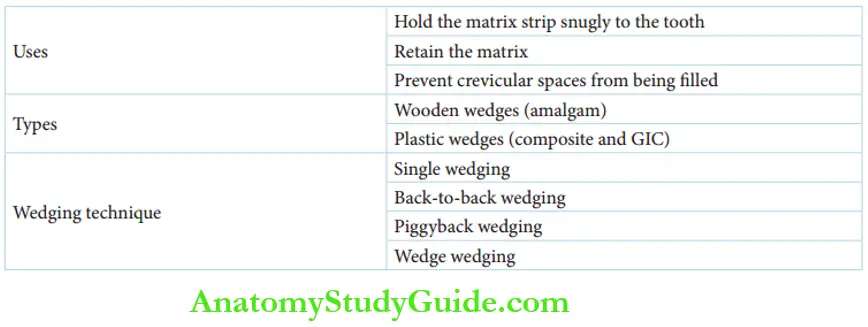
A wedge is a triangular wooden or plastic device inserted into the interproximal region of the tooth being restored. It helps to adapt the gingival extent of the matrix strip snugly to the crevicular space of the tooth structure.
It retains the matrix in place firmly when the restorative material is compacted. Employing a matrix strip and a wedge ensures good contour and contact of the proximal restoration.
Wedges are 1–1½ cm long and can be of two types. Wooden triangular wedges are used for amalgam restorations, while transparent plastic wedges are preferred for composite and GIC restorations.
The plastic wedge reflects light while curing in composite restoration. This helps the restorative material in the proximal box to attain a higher degree of set or cure.
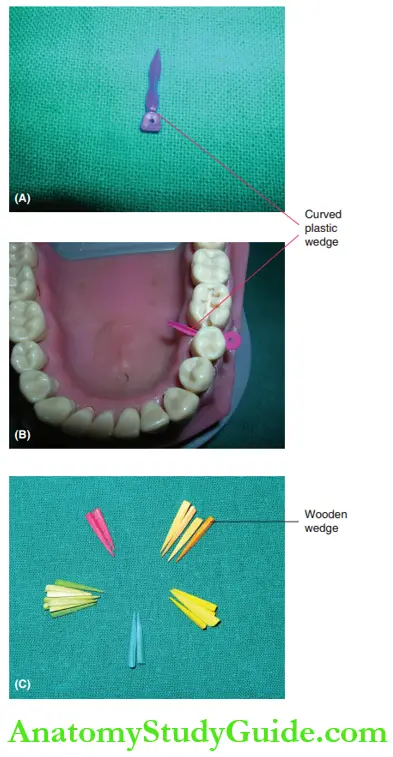
- (A) and
- (B) Curved plastic wedges in use.
- (C) Wooden wedges. (Courtesy: Harpreet Singh, Essentials of Preclinical Conservative Dentistry)
Wedging Techniques
Simple wedging techniques involve a single wedge for one proximal embrasure. Some situations may warrant the use of more than one wedge. The following techniques are used in such cases:
- Back-to-back wedging: When contacts are almost open or the embrasure is mesiodistally wider.
- one wedge is placed from the buccal to the lingual direction and the second is inserted from the lingual to the buccal direction.
- This is called back-to-back wedging.
- Piggyback wedging: When the cervical-occlusal dimension of the embrasure is more, one wedge is placed over the other.
- This is called piggyback wedging.
- Wedge wedging: When the buccolingual diameter is longer, one wedge is kept at an angle over another wedge.
- This wedge wedging technique adapts the matrix band snugly to the entire length of the tooth.
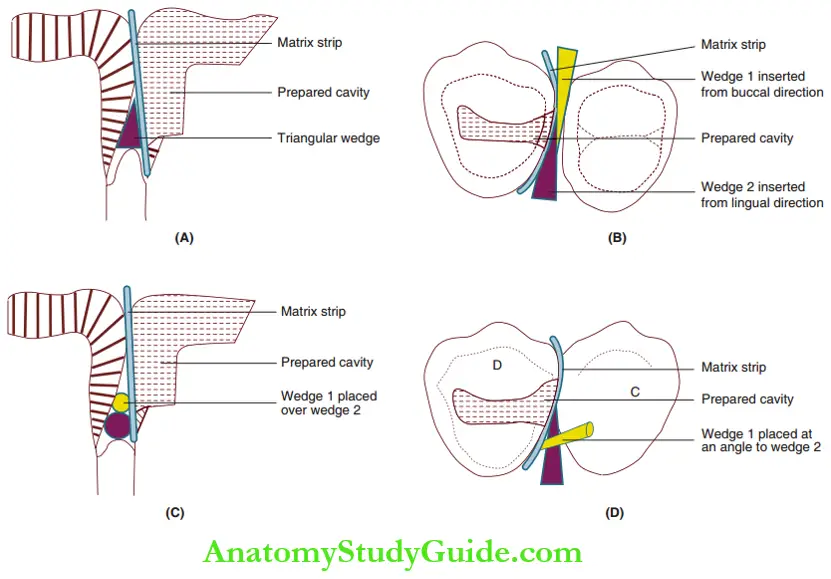
- (A) Simple wedging.
- (B) Back-to-back wedging.
- (C) Piggyback wedging.
- (D) Wedge wedging.
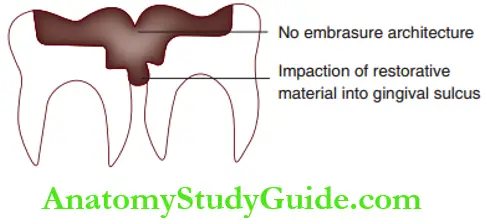

Clinical Application
The use of a matrix strip and wedge is mandatory for a proximal restoration. A small proximal box also requires a matrix and wedge for good contact and contour. depicts the effect of not resorting to the use of matrix and wedge.
The proximal restoration may appear as a no-embrasure architecture. Restoration material may get impacted into the gingival sulcus.
a proximal restoration that uses a matrix with no wedge. A gingival embrasure will not be imparted in this case.
Summary
1. Isolation
2. Matrices
3. Wedges
4. Employing an appropriate matrix system and wedge ensures good contour and contact of the proximal restoration.
Leave a Reply