Joints Of The Lower Limb
Which muscles are chief flexors of hip joint?
Table of Contents
1. Iliacus,
2. Psoas major, and
3. Pectineus.
Hip Anatomy Muscles
What is the nerve supply of hip joint?
Nerve supply: The three nerves of the pelvic girdle and lower limb supply the hip joint (Hilton’s law).
1. Femoral nerve via the nerve to rectus femoris,
2. Sciatic nerve via the nerve to quadratus femoris, and
3. Obturator nerve directly from its anterior division.
Read And Learn More: Anatomy Notes And Important Question And Answers
Name the articulating surface participating in formation of hip joint
There are two bones taking part in hip joint. They are
1. Head of femur, and
2. Articulating surface of acetabular cavity of hip bone.
Lower Extremity Joints
Dislocation of hip joint
Attachments of capsule of hip joint
1. Attachments of the capsule: The fibrous capsule is attached on the
1. Hip bone to the
- Acetabular labrum including the transverse acetabular ligament, and to
- Bone above and behind the acetabulum;
2. Femur to the
- Intertrochanteric line in front, and
- One cm medial to the intertrochanteric crest behind.
3. Variation of thickness of capsule
- The capsule is thick and firmly attached anterosuperiorly. This part is subjected to maximum tension in the standing posture.
- It is thin and loosely attached posteroinferiorly
Lower Extremity Joints
Hip Anatomy Muscles
Describe Hip Joint under following heads
1. Hip Joint Classification,
2. Hip Joint Ligaments,
3. Hip Joint Relations,
4. Hip Joint Blood supply,
5. Hip Joint Nerve supply,
6. Hip Joint Movements,
7. Hip Joint Muscles bringing movements, and
8. Hip Joint Applied anatomy.
1. Classification of hip joint:
Axis: Multiaxial. There are three axes.
No. of Bones taking part: There are two bones taking part in formation of hip joint.
Hence it is classified as simple joint. The bones are
- Head of femur, and
- Articulating surface of acetabular cavity of hip bone.
Surfaces of articulating bones are spherical and socket like. Hence, it is classified as
ball and socket type of synovial joint.
2. Ligaments
1. Capsule
1. Attachments
- Superiorly: It is attached superiorly 5 to 6 mm above the acetabular margin of hip bone.
- Inferiorly Anteriorly: On the intertrochanteric line. Posteriorly: One cm medial to intertrochanteric crest.
Lower Extremity Joints
2. Variation in thickness
- Anterosuperiorly: It is thick and attached firmly. It is subjected to maximum tension in standing.
- Posteroinferiorly: It is thin and loosely attached to bone.
3. Types of fibres: There are two types of fibres
- The outer fibres are longitudinal and are best developed anterosuperiorly. They are called retinacula. The blood vessel supplying head and neck of femur travel along these retinacula.
- The inner fibres are circular and are called zona orbicularis.
4. Capsule is re-enforced by
- Iliofemoral,
- Pubofemoral,
- Ischiofemoral ligaments,
- Acetabular labrum,
- Transverse acetabular ligament, and
- Ligament of the head of the femur (ligamentum teres)
5. Synovial membrane: It lines
- The inner surface of fibrous capsule,
- Intracapsular portion of neck of femur,
- Both surfaces of acetabular labrum,
- Transverse acetabular ligament, and
- Fat in the acetabular fossa.
6. Acetabular labrum (labrum—edge, brim). It is fibrocartilage.
- Functions:
- Deepens the acetabular cavity.
- Accommodates distal end of the head of femur. Thus, it protects the socket in case of pulling the head of the femur.
- Maintains the bony contacts
- Protects the edges.
Lower Extremity Joints
2. Iliofemoral ligament (ligament of Bigelow)
- It is Y-shaped, strongest ligament in the body.
- It extends from the anterior inferior iliac spine to the intertrochanteric line.
- It prevents backwards falling.
3. Pubofemoral ligament
- It is lar.
- It extends from iliopubic eminence, obturator crest and obturator membrane to inferior part of capsule.
4. Ischiofemoral ligament
1. It should be ideally called ischiocapsular because it is attached to inner layer of capsule.
2. It is weak and almost horizontal across the capsule of hip joint.
1. It extends from
- Posterior inferior surface of acetabular margin to
- Posterior part of neck of femur.
2. It is continuous with zona orbicularis.
Hip Anatomy Muscles
5. Ligament of head of femur (ligamentum teres or round ligament)
1. It is flat and lar.
2. Its apex is attached to the depression present on the head of femur called fovea centralis, and
3. Base is attached to
- Transverse acetabular ligament, and
- Margins of acetabular notch by two bands.
4. It transmits arteries of head of femur (from acetabular branches of the obturator and medial circumflex femoral arteries).
6. Transverse ligament of the acetabulum
- It is a part of acetabulum, and
- It bridges the notch.
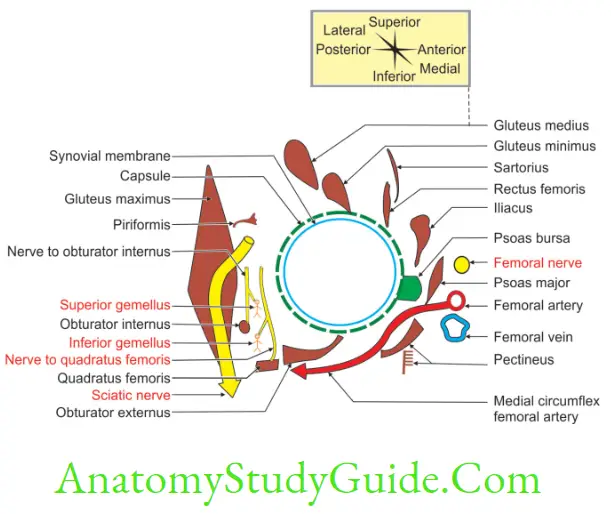
3. Relations
1. Posterior
1. Tendon of
- Obturator externus, and
- Obturator internus.
2. Gemelli, and
3. Piriformis.
2. Superior
- Reflected head of rectus femoris, and
- Gluteus minimus.
3. Inferior
- Pectineus and cover of gluteus maximus, and
- Obturator muscle.
4. Nerve supply: There are three nerves of the pelvic girdle and lower limb that supply the hip joint (Hilton’s law).
- Femoral nerve via the nerve to rectus femoris,
- Sciatic nerve via the nerve to quadratus femoris, and
- Obturator nerve directly from its anterior division.
5. Blood supply
- Obturator artery branch of anterior division of internal iliac artery.
- Ascending branches of medial circumflex femoral artery branch of profunda femoris artery.
- Ascending branches of lateral circumflex femoral branch of profunda femoris artery.
- These supply the neck and head of the femur.
Hip Anatomy Muscles
6. Movements
1. Axis
1. Transverse axis of hip joint
1. Flexion:
- Psoas major, and
- Iliacus are powerful flexors.
2. Extension: Muscles
1. Gluteus maximus, and
2. Hamstring muscles.
- Ischial fibres of adductor magnus,
- Biceps femoris,
- Semimembranosus, and
- Semitendinosus.
2. Sagittal axis of hip joint
1. Adduction
- Adductor magnus,
- Adductor longus, and
- Adductor brevis.
2. Abduction
- Gluteus medius, and
- Gluteus minimus.
3. Longitudinal axis of hip joint
1. Medial rotation
- Tensor fascia lata, and
- Anterior fibres of gluteus medius.
2. Lateral rotation
- Gluteus maximus,
- Obturator internus and externus,
- Superior and inferior gemelli,
- Piriformis, and
- Quadratus femoris.
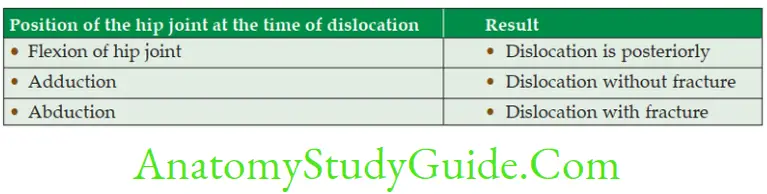
7. Applied anatomy
- Congenital dislocation is more common in hip joint than in any other joint.
- The position of the hip joint is weak in flexion and lateral rotation of femur. Hence posterior dislocation (dashboard injury) is more common.
- Anterior dislocation is less common.
- Central dislocation is very rare.
- Fracture of neck of femur occurs between 40 and 60 years.
- Disease of hip joint may produce shortening of limb.
- Disease of hip may cause referred pain to knee joint.
Classify Knee Joint (Genual)
1. Structurally:
- Axis: Uniaxial
- Modified hinge joint: The movements are in transverse axis. The movements permitted are flexion, extension hence hinge joint. The transverse axis is not fixed, so it is modified hinge joint.
- Number of Bones: There are three bones in the knee joint sharing a common capsule. Hence, it is a compound joint.
- Complex: Joint is divided into two compartments by a fibrocartilage structure— menisci.
- Condylar: Medial and lateral condyles of femur and tibia are taking part.
- Shape: Saddle-shaped: Between femur and patella, the surface of which is concave convex and reciprocating convex concave.
2. Functionally: Diarthrosis (freely movable).
Capsule of Knee Joint
1. Attachments
1. To femur: It is attached to the peripheral margin of articular surface of lower end of femur.
- It excludes articulating area of patella.
- It includes tendon of popliteus.
2. To tibia: It is attached 1 cm distal to articular margin.
- Anteriorly, it is attached along the upper margin of the tibial condyles.
- Posteriorly, it is attached to the intercondylar ridge.
3. Deficient at
- Tibial tuberosity on tibia, and
- Gap for popliteal tendon behind the lateral condyle of tibia for the passage of tendon of popliteus.
4. Strengthened by
- Anteriorly by medial and lateral patellar retinacula,
- Posteriorly by oblique popliteal ligament,
- Laterally by iliotibial tract, and
- Medially by tendon of sartorius and semimembranosus.
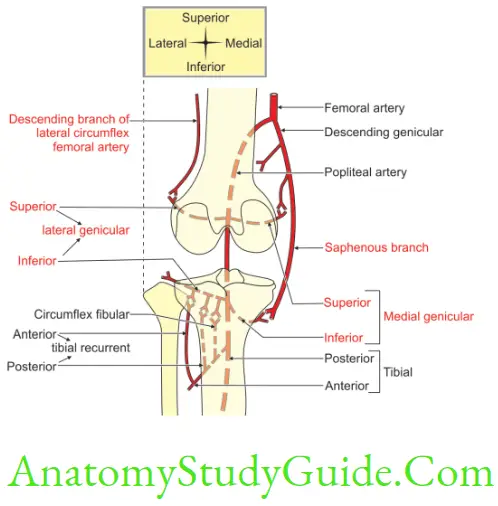
Draw and label the diagram showing anastomosis around knee joint
Five genicular branches of the popliteal artery
1. Descending
- Genicular branch of the femoral artery, and
- Branch of the lateral circumflex femoral artery.
2. Two recurrent branches of the anterior tibial artery, and
3. Circumflex fibular branch of the posterior tibial artery.
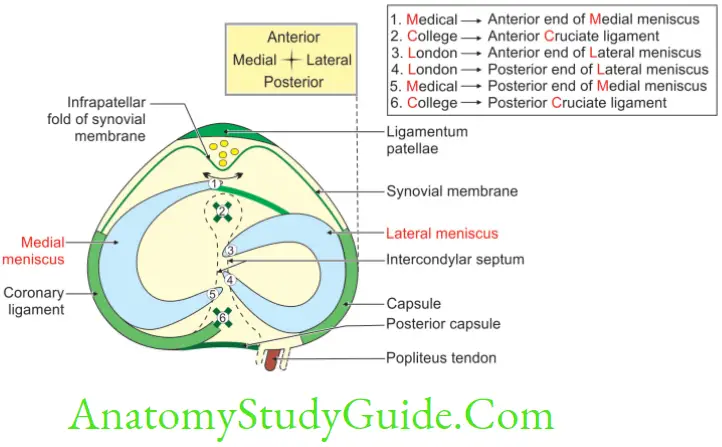
Enumerate intra-articular structures of knee joint
The most important structure is cruciate ligament. The other intra-articular structures include the menisci, and the femoral tendon of popliteus.
The other structures are: The intra-articular structures start with the first letters of days of the week.
Menisci (Mon),
Tendon of popliteus (Tue),
Meniscofemoral ligament (Wed—the first letter of Wednesday is inverted M),
Transverse ligament (Thu),
Haversian pad of fat (Fri),
Synovial membrane (Sat), and
Coronary ligament (Cun) (The pronunciation of c and s is similar)
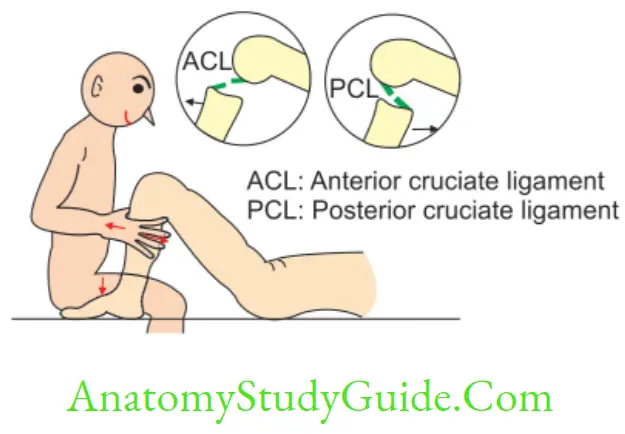
Cruciate Ligament
Cruciate Ligament Introduction: The ligaments connecting the femur and tibia are in the form of cross. Hence, they are called cruciate ligaments. The nomenclature is based on the attachments to the part of upper surface of tibia.
1. Cruciate Ligament Functions
- It is key stabilizer of knee joint.
- It checks anterior and posterior movements of the femur on tibia.
2. Cruciate Ligament Attachments
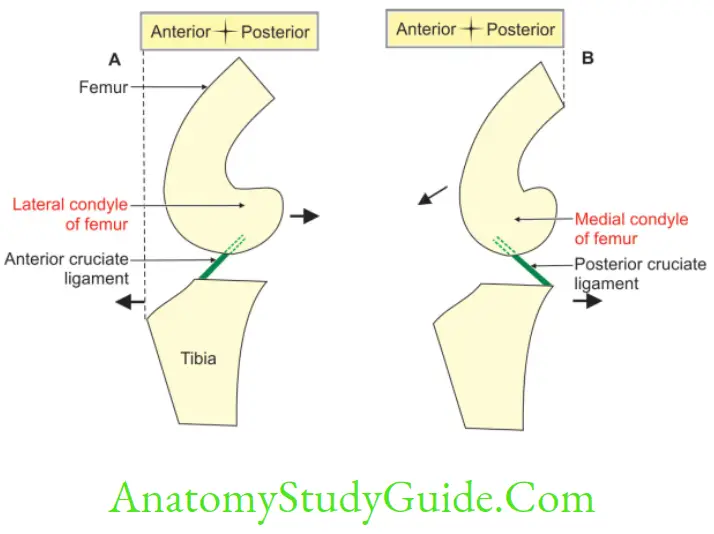
Lateral condyle gives attachment to Anterior cruciate ligament. Medial condyle gives attachment to Posterior cruciate ligament.
Anterior cruciate ligament extends from anterior part of upper surface of tibia to the lateral condyle of femur.
Posterior cruciate ligament extends from posterior part of upper surface of tibia to the medial condyle of femur.
3. Cruciate Ligament Morphology: The posterior cruciate ligament is stronger, shorter and less oblique. In weight-bearing, flexed knee, posterior cruciate ligament is the only stabilizing factor.
4. Cruciate Ligament Functions
1. Anterior cruciate ligament prevents the anterior displacement of tibial condyle on femur. It prevents sliding of the femur backwards on tibia.
2. Posterior cruciate ligament prevents the posterior displacement of tibial condyle on femur. It prevents femur from sliding forward. Both cruciate ligaments prevent side-to-side displacement of tibia and femur.
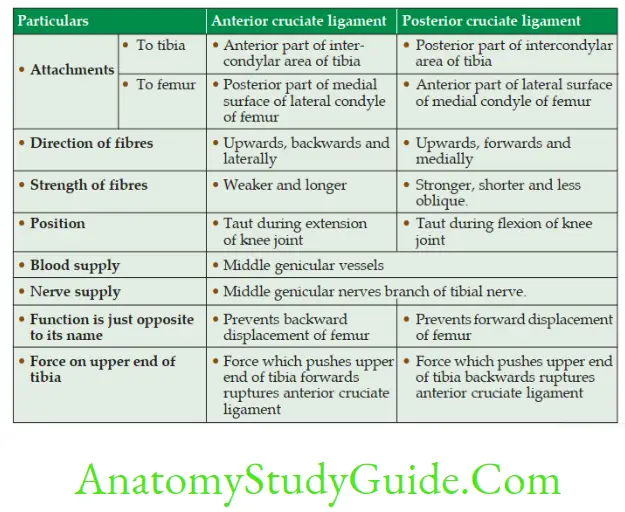
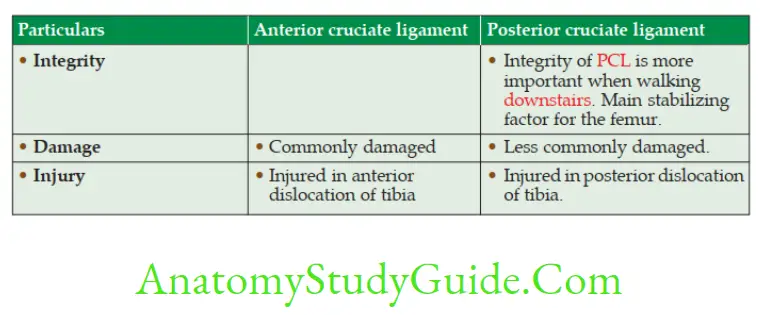
Compare Anterior And Posterior Cruciate Ligaments
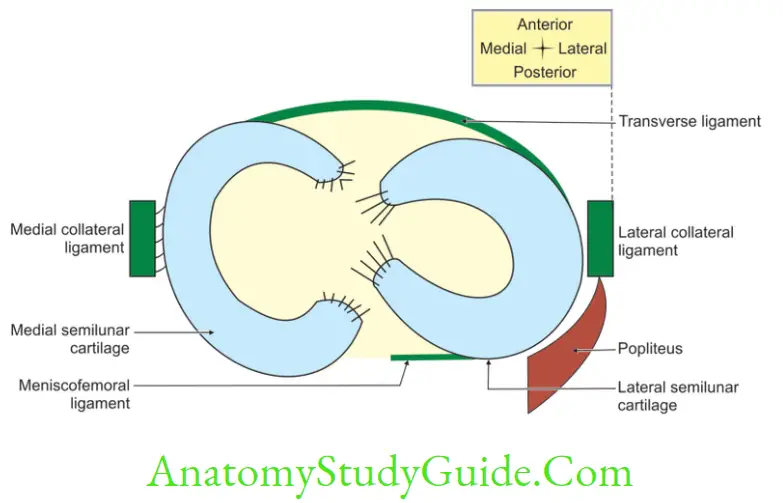
Meniscus
(Menisco—crescent, half moon)
Meniscus Introduction: It is a semilunar, fibrocartilaginous ring, lar in cross-section, covers the articular surfaces of the condyles of tibia.
1. Meniscus Functions: The chief role of meniscus is to
- Rotate the femur, and to
- Spread the synovial fluid uniformly.
- Maintains the bony contact and potential joint space.
- Escorts the articular surfaces.
- Nourishes the articular surface.
- Increases the concavity of tibial condyle.
- Serves as a cushion.
- Deepens the joint cavity.
- Spreads the synovial fluid uniformly.
- Saves from the shock during weight transmission.
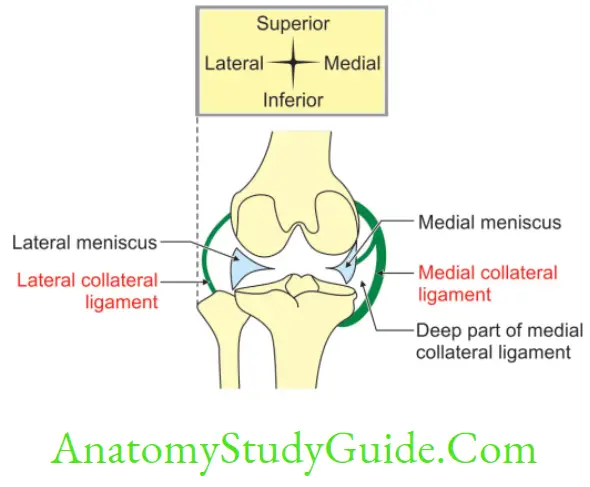
2. Meniscus Number: There are two menisci—medial and lateral.
3. Meniscus Attachment
1. Each meniscus has anterior and posterior horns. Both the horns of both the menisci are attached to the anterior and posterior intercondylar areas, respectively.
2. The medial margin of the medial meniscus and lateral margin of lateral meniscus are attached to the capsule of the knee joint.
3. The medial margin of the medial meniscus is also attached to the tibial collateral ligament.
4. The posterior horn of lateral meniscus provided attachment to
- The meniscofemoral ligament, and
- Fibres of the popliteus.
4. Meniscus Movements
1. The flexion and extension movements occur in the upper compartment.
2. The rotation movement occurs in the lower compartment.
5. Meniscus Applied anatomy: The medial meniscus is more prone for injury as it is more firmly attached to the capsule and tibial collateral ligament.
Meniscofemoral Ligaments
Meniscofemoral Ligaments Introduction: They connect the lateral meniscus to medial condyle of femur.
1. Attachments
1. They arise from posterior horn of lateral meniscus and get attached to medial condyle of the femur.
2. They are named anterior and posterior meniscofemoral ligaments. The anterior meniscofemoral ligament passes anterior to the posterior cruciate ligament and posterior meniscofemoral ligament passes posterior to the posterior cruciate ligament.
2. Meniscofemoral LigamentsFunction: They regulate the forward movement of the lateral meniscus during extension of the knee.
Lower Extremity Joints
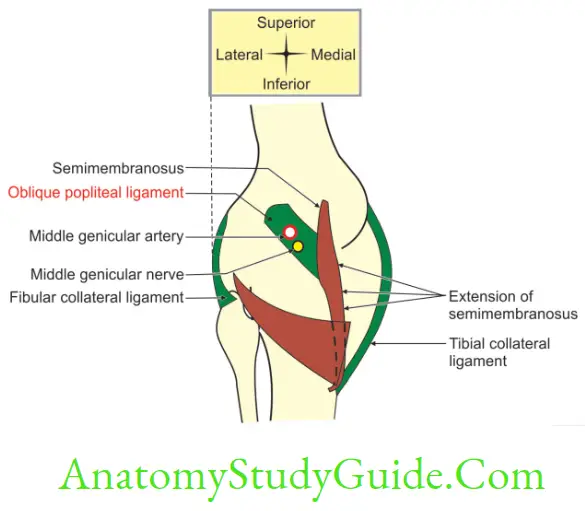
Oblique popliteal ligament
The oblique popliteal ligament is an expansion of tendon of semimembranosus muscle. It extends from posterior surface of medial condyles of tibia to lateral part of intercondylar line of femur. This forms the floor of popliteal fossa. It is pierced by
1. Middle genicular vessels and nerves, and
2. Genicular branch of posterior division of obturator nerve.
Transverse ligament (transverse meniscal ligament)
It connects anterior horn of medial meniscus to anterior margin of lateral meniscus. It is present in 40% of individuals.
Synovial membrane of knee joint
Synovial membrane of knee joint Introduction: It lines the inner surface of capsule and extends on patella. It is a mere capillary film.
1. Synovial membrane of knee joint Amount of synovial fluid—0.5 ml.
2. Synovial membrane of knee joint Features
1. Infrapatellar synovial fold: It is a flattened hollow cone of synovial membrane.
It has a base and an apex.
- Base is opened. It extends from articular cartilage of patella to the anterior intercondylar area of tibia.
- Apex: It is attached to the most anterior point of the intercondylar notch of femur.
2. Synovial cavity: There are three cavities—a patellar and two condylar.
C. Bursae: There are three bursae
- Suprapatellar bursa: It is deep to quadriceps femoris tendon.
- Popliteal bursa: It opens into lateral condylar cavity. It is below the meniscus.
- Gastrocnemius bursa: It is deep to medial head of gastrocnemius.
Coronary ligament
Coronary ligament Introduction: It is a part of fibrous capsule.
Coronary ligament connects
1. Convex margins of medial and lateral menisci to
2. Upper end of tibia.
Arcuate Ligament
Arcuate Ligament Introduction: It is Y-shaped fibrous band.
1. The stem of the arcuate ligament is fixed to styloid process of fibula.
2. The anterior band is attached to lateral condyle of femur.
3. The posterior band is attached to lateral condyle of tibia.
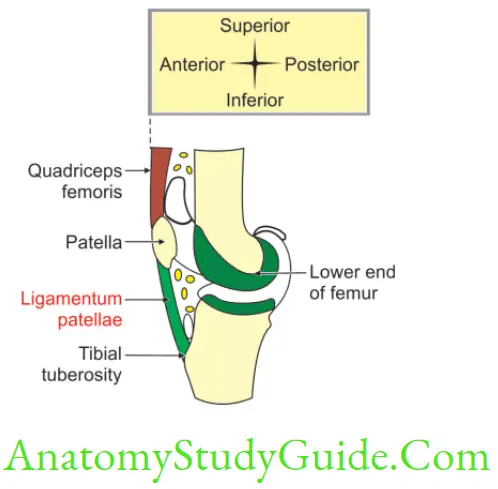
Ligamentum Patellae
Introduction: Ligamentum patellae derived from tendon of quadriceps femoris and extend from the apex of patella to the tibial tuberosity.
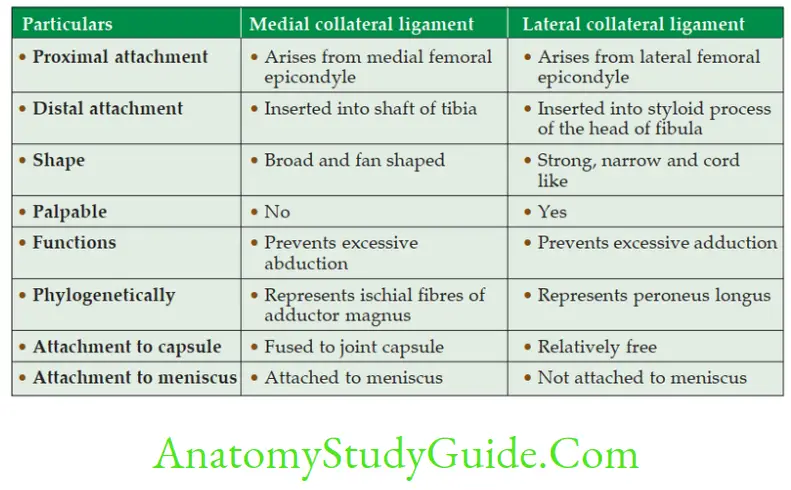
Collateral Ligaments
The collateral ligaments are present on the medial and lateral side of knee joint. These can be described as follows
Relations of Knee Joint
1. Anterior: Quadriceps femoris.
2. Posterior
- Popliteal vessels,
- Tibial nerve, and
- Lateral and medial head of gastrocnemius.
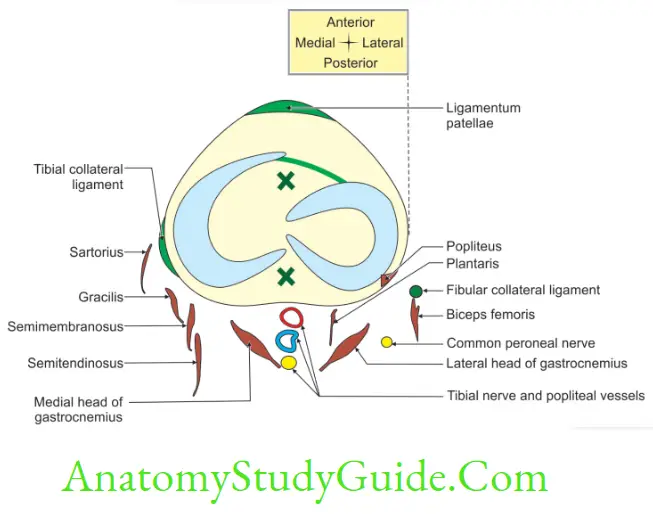
3. Medially
- Medial patellar retinaculum,
- Sartorius,
- Gracilis,
- Semimembranosus, and
- Semitendinosus.
4. Laterally
- Common peroneal nerve,
- Lateral patellar retinaculum, and
- Tendon of biceps femoris.
Movements of knee joint and muscles bringing the movements of knee joint
1. Flexion
1. Main muscles
1. Hamstring muscles,
- Semimembranosus,
- Semitendinosus, and
- Biceps femoris.
2. Sartorius, and
3. Gracilis.
2. Accessory muscles
- Gastrocnemius, and
- Plantaris.
2. Extension
1. Main muscles
- Quadriceps femoris, and
- Tensor fascia lata.
2. Accessory muscle
3. Muscular slips of articularis genu
3. Rotation of the knee joint: May be adjuvant or conjunct.
1. Adjuvant (aiding, assisting, independent of flexion and extension) rotation. Rotation around the vertical axis independent of flexion and extension, e.g. when foot is off the ground and knee in semiflexed position, tibia rotates medially and laterally around the vertical axis.
2. Conjunct (associated and integrated with flexion and extension) rotation
- It takes place along with flexion and extension of knee joint.
- In last 30° of extension, the anterior cruciate ligament is stretched.
- It acts as a vertical axis around which the medial condyle of femur rotates in backwards and medially.
- It (medial condyle of femur) reaches the anterior horn of medial meniscus and completely obliterates the medial meniscofemoral compartment.
- This completes the last 30° of extension.
- It is achieved by conjunct rotation of medial condyle of femur on tibia.
- This mechanism locks the knee joint.
- During unlocking, the popliteus contracts. It causes the lateral rotation of medial condyle of femur on tibia.
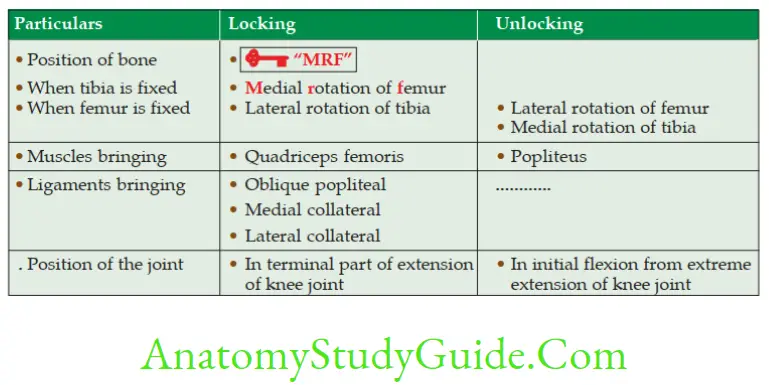
4. Locking: The key word is for locking
1. Definition: It is
- Medial Rotation of the Femur on fixed tibia, or
- Lateral rotation of tibia on fixed femur.
2. Muscle: Quadriceps femoris
3. Medial rotation: Semimembranosus, semitendinosus, gracilis and sartorius.
4. Lateral rotation: Biceps femoris.
5. Unlocking
1. Definition: It is
- Lateral rotation of femur on fixed tibia, or
- Medial rotation of tibia on fixed femur.
2. Muscle: Popliteus.
Stability of knee joint
The stability of knee joint is maintained by following structure
1. The cruciate ligaments are indispensable for anteroposterior stability in flexion.
2. Vastus medialis is indispensable to the stability of patella.
3. Spines of tibia prevent side way gliding.
4. Ilio-tibial tract, gluteus maximus and tensor fascia lata stabilizes slightly flexed knee joint.
5. Bones do not play any role.
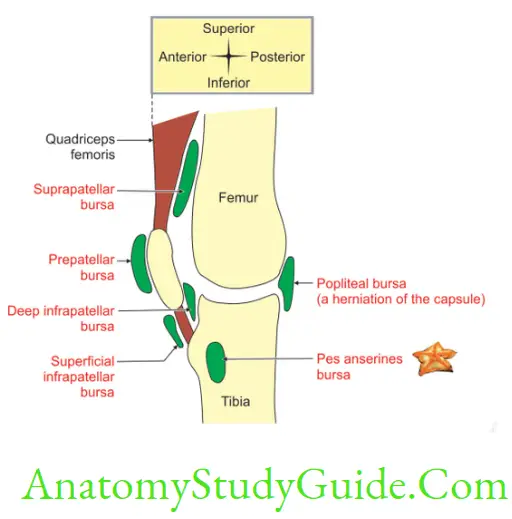
Bursae Around Knee Joint
1. Anterior bursae: They are anterior to knee joint. They are
1. Subcutaneous: It is present beneath the skin. They may be
- Subcutaneous pre-Patellar, e.g. Housemaid’s knee—PPH
- Subcutaneous infrapatellar, e.g. Clergyman’s Knee—SICK.
B. Deep
- Suprapatellar, and
- Infrapatellar.
2. Lateral bursae between
- Lateral condyle of tibia and tendon of popliteus,
- Popliteus and fibular collateral ligament,
- Fibular collateral ligament and biceps femoris, and
- Deep to lateral head of gastrocnemius.
3. Medial
1. Deep to medial head of gastrocnemius,
2. Anserine bursa
- It is a complicated bursa,
- It separates the members of guy ropes from one another. The members of the guy ropes are sartorius, semitendinosus, and gracilis, and
- It also separates from tibia and tibial collateral ligament.
3. Deep to tibial collateral ligament,
4. Deep to semimembranosus, and
5. Between semimembranosus and semitendinosus.
Locking and Unlocking of Knee Joint
Introduction: The function of locking and unlocking of knee joint is to keep the knee in full extension without muscular effort. It is brought by
- Medial rotation of femur on fixed tibia during terminal stage of extension.
- Lateral rotation of femur on fixed tibia during early stage of flexion.
1. Necessity of the movements of locking and unlocking
- The surface area of articular surfaces of tibia and femur are not proportionate.
- The articular surfaces of tibia and femur are incongruent.
- During the terminal part of extension of knee joint, the small articular surface of the tibia is used up by the femur. To accommodate the unused articular surface of femur on tibia, the femur or tibia is required to rotate. This is done to have the stable movement.
Lower Extremity Joints
2. Difference between locking and unlocking
Describe ankle joint (talocrural) under following heads
1. Bones taking part,
2. Classification,
3. Ligaments,
4. Movements and muscles producing movements,
5. Relations,
6. Arterial supply,
7. Nerve supply, and
8. Applied anatomy.
1. Bones taking part
- Lower end of fibula with lateral malleolus,
- Medial malleolus of tibia, and distal part of tibia, and
- Superior surface of talus.
2. Classification
1. Structural:
- Axis: Uniaxial, modified hinge (since the axis of movement is basically transverse with a slight downward inclination on the lateral side) variety of synovial joint. Number of bones: Articulating bones in the formation of ankle joint are three and they are tibia, fibula and talus. Hence it is compound synovial joint.
2. Functional: Diarthrosis (freely mobile).
3. Ligaments
1. Fibrous capsule covers the joint completely
1. Attachments
- It is attached superiorly to the peripheral margins of the articular surfaces of lower end of tibia and fibula.
- It is attached inferiorly to the peripheral margin of Articular surface of the superior surface of talus. Comma-shaped facet present on the medial surface of talus. lar facet present on the lateral surface of talus.
2. Variations in thickness
- Thin in front, thin behind.
- Thick laterally, thick medially.
3. Fate: It blends with collateral ligament.
2. Synovial membrane
- It lines the inner surface of the fibrous capsule.
- It stops at the periphery of the articular cartilage.
- A small synovial recess extends upwards in the inferior tibiofibular joint.
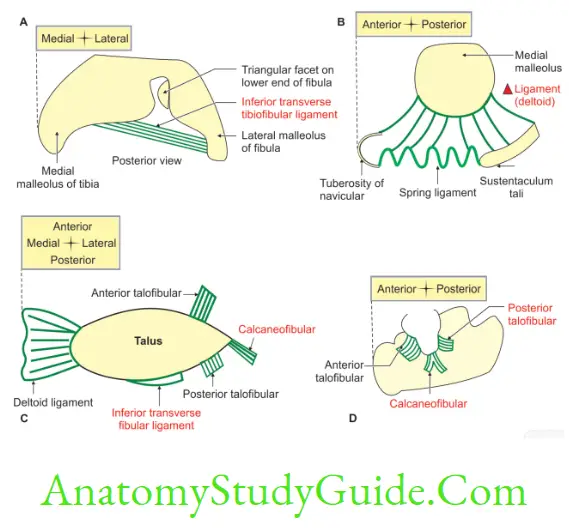
3. Deltoid ligament: It is a strong lar ligament present on the medial side of the ankle joint. It has superficial and deep parts.
4. Lateral ligament: It is a ligament present on the lateral side of ankle joint. It connects talus and calcaneum with fibula.
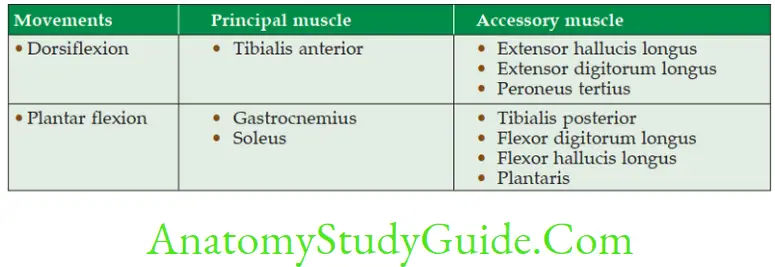
4. Movements and muscles producing movements
1. Dorsiflexion
1. Range of movement—10°–20°
2. All muscles of anterior or extensor compartment of the leg bring dorsiflexion of the ankle joint, i.e.
- Tibialis anterior,
- Extensor hallucis longus, and
- Extensor digitorum longus.
2. Plantar flexion
1. Range of movement is 20°–40°.
2. All the muscles of flexor compartment of the leg are plantar flexors of ankle joint.
3. The gastrocnemius with soleus acts as prime mover.
4. The peroneus longus and brevis come into play in extreme plantar flexion. The muscles bringing plantar flexion are
- Peroneus tertius,
- Tibialis posterior,
- Flexor digitorum longus,
- Flexor hallucis longus,
- Tendo Achilles.
3. In symmetrical standing, the line of gravity passes slightly in front of the ankle joint, therefore, there is a natural tendency for forward dislocation which is prevented by
- Broader anterior part of trochlear surface of talus, and
- Tonic contraction of triceps surae.
5. Relations
1. Anterior (From medial to lateral)
Tibialis anterior
Extensor Hallucis longus
Anterior tibial Artery
Anterior tibial Nerve
Extensor Digitorum longus
Peroneus tertius
2. Posterior: Behind tibial malleolus.
(From anterior to posterior)
Tendon of tibialis posterior,
Flexor digitorum longus,
Posterior tibial artery,
Tibial nerve, and
Tendon of flexor hallucis longus.
3. Behind the fibular malleolus: Tendon of peroneus brevis and peroneus longus. The peroneus brevis is situated deep and peroneus longus is situated superficially.
6. Arterial supply: Malleolar branches of anterior tibial and peroneal arteries.
7. Nerve supply: Branches from deep peroneal and tibial nerves.
8. Applied anatomy
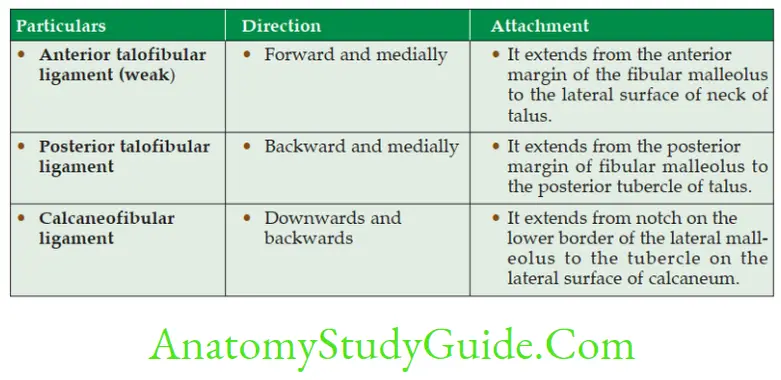
- Ankle sprain: It is due to over inversion of foot, which is one of the common manifestations. The anterior talofibular and calcaneofibular ligaments are sometimes torn and in severe cases the anterior part of the capsule of the ankle joint is ruptured.
- Pott’s fracture: The forceful eversion of the foot causes avulsion of the deltoid ligament, fracture of the tibia and fibula. This is described in 3 degrees.
- In 1st degree there is only an Avulsion (tearing) of deltoid ligament.
- In 2nd degree
- Avulsion (tearing) of deltoid ligament
- Fracture of medial malleolus of tibia.
- In 3rd degree
- Avulsion fracture of the deltoid ligament,
- Fracture of medial malleolus of tibia, and
- Oblique fracture of the lower part of the fibula.
- The ankle sprains usually occur when the foot is plantar flexed.
- The sprains of the ankle joint are almost always abduction sprains of the subtalar joints.
Deltoid Ligament
Introduction: It is a strong lar ligament present on the medial side of the ankle joint and it has superficial and deep parts.
1. Superficial part
1. It is lar.
2. The base of the is attached to tarsal bones, namely navicular, calcaneum and talus.
3. The apex is attached to the tip of medial malleolus. They are subdivided into anterior, middle and posterior fibres.
1. Anterior fibres extend from medial malleolus of tibia to
- Tuberosity of navicular bone, and to the
- Medial margin of spring ligament.
- These fibres are present anteriorly; hence they are called anterior fibres of deltoid ligament or tibionavicular ligament.
2. Middle fibres extend from medial malleolus of tibia to sustantaculum tali of calcaneum. They are called tibiocalcanean ligament.
3. Posterior fibres extend from medial malleolus of tibia to the medial tubercle of talus. They are also called superficial tibiotalar ligament.
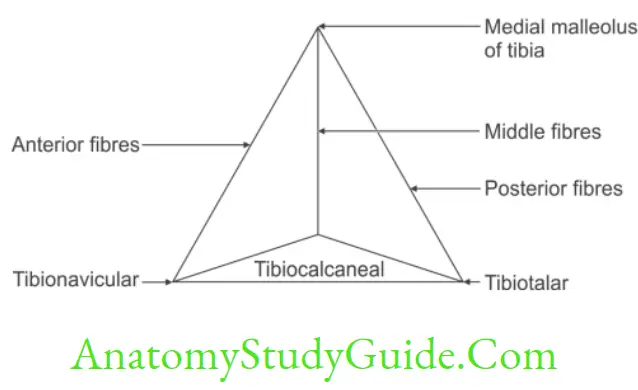
2. Deep part blends with fibrous capsule. It connects tibial malleolus to anterior part of medial surface of talus below comma shaped facet. This is also called deep tibiotalar ligament.
Movements of ankle joint
Lower Extremity Joints
Lateral ligaments of ankle joint
Describe inversion under following heads
1. Bones taking part,
2. Joints and classification of joints,
3. Axis,
4. Combination of action,
5. Range of movements,
6. Functions, and
7. Applied anatomy.
Introduction: It is a movement in which the medial border of foot is elevated so that the sole or plantar surface of the foot faces medially. Inversion and eversion are best demonstrated when the foot is off the ground.
When the foot is on the ground typical inversion and eversion are not observed.
The malleoli lock the talus and suspended foot inverts and everts around it.
1. Bones taking part: Talus, calcaneus and navicular.
2. Joints and classification of joints
- Talocalcaneonavicular: Ball and socket variety of synovial joint.
- Subtalar: Plane synovial joint.
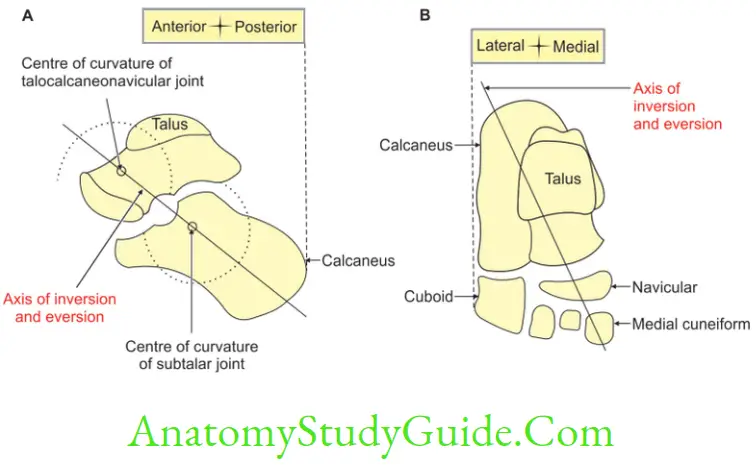
3. Axis: It is an oblique axis. Its direction is forwards, upwards and medially. It passes from the back of lateral tubercle of calcaneus, through sinus tarsi. It emerges at the superomedial aspect of neck of talus. This axis corresponds to abduction, adduction, plantar flexion and dorsiflexion and medial and lateral rotations of calcaneus.
4. Combination of movements: Adduction, plantar flexion, rotation and gliding movements.
5. Range of movements: It is freer as compared to the eversion.
6. Functions
- The inversion movement helps to walk on slippery and uneven surfaces.
- It helps to maintain an efficient shift of weight distribution among the head of metatarsal bones during locomotion.
7. Applied anatomy
Inversion sprain is the most common ankle injury. It involves the tearing of lateral collateral ligaments. Usually, the anterior talofibular ligament is torn first, then the calcaneofibular ligament and in severe cases, the posterior talofibular ligament.
Describe Eversion under following heads
1. Eversion Bones taking part,
2. Eversion Axis,
3. Eversion Combination of action,
4. Eversion Range of movements,
5. Eversion Muscles bringing movement,
6. Eversion Functions, and
7. Eversion Applied anatomy.
Eversion Introduction: It is a movement in which the lateral border of the foot is elevated so that sole or plantar surface of the foot faces laterally when the foot is off the ground. Eversion is a combination of pronation and abduction.
1. Eversion Bones taking part: Calcaneum, talus and cuboid.
2. Eversion Axis: An oblique axis runs forwards, upwards and medially. It passes from the back of lateral tubercle of calcaneus. It passes through sinus tarsi to emerge at the superomedial aspect of neck of talus. This axis corresponds to abduction, adduction, plantar flexion and dorsiflexion and medial and lateral rotations of calcaneus.
3. Eversion Combination of action: Abduction, dorsiflexion, rotation and gliding.
4. Eversion Range of movements: It is less free as compared to inversion.
5. Eversion Muscles bringing movements
1. Peroneus longus,
2. Peroneus brevis, and
3. Peroneus tertius.
Peroneus longus and brevis whose tendons pass behind lateral malleolus are plantar flexors. The peroneus tertius is dorsiflexors of ankle joint. These opposite effects cancel each other and produce simple eversion movement. Eversion is a movement of pronation and is accompanied by abduction of the fore part of the foot.
6. Eversion Functions
- To walk on slippery and uneven surfaces.
- To maintain an efficient shift of weight distribution among the head of metatarsal bones during locomotion.
7. Eversion Applied anatomy
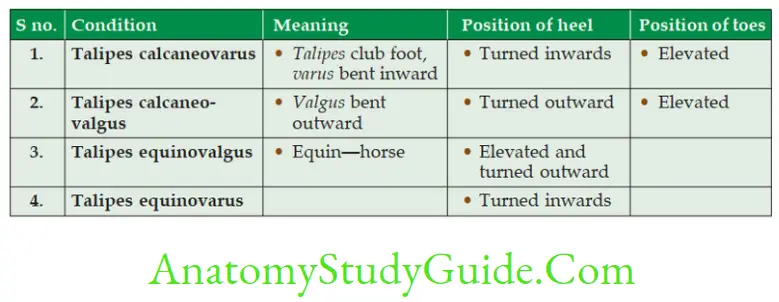
- Talipes calcaneovarus: A deformity of the foot in which the heel is turned toward the midline of the body and the anterior part is elevated.
- Talipes calcaneovalgus: A deformity of the foot in which the heel is turned outward from the midline of the body and the anterior part of the foot is elevated.
- Talipes equinovalgus: A deformity of the foot in which the heel is elevated and turned outward from the midline of the body.
- Talipes equinovarus: A deformity of the foot in which the heel is turned inward from the midline of the leg and the foot is plantar flexed. This is typical club foot.
- Eversion sprains, which are less common, usually involve tearing of the deltoid ligament.
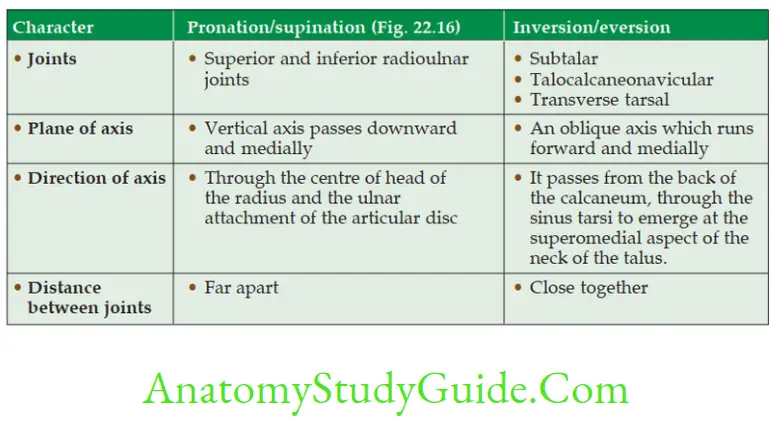
Compare Pronation, Supination with Inversion and Eversion
Spring ligament (plantar calcaneonavicular ligament)
Spring ligament Introduction: It is an anterior segmental tie (staples) and is one of the important ligaments in the maintenance of medial longitudinal arch.
1. Spring ligament Extent: It extends from sustantaculum tali of calcaneus to tuberosity of navicular bone.
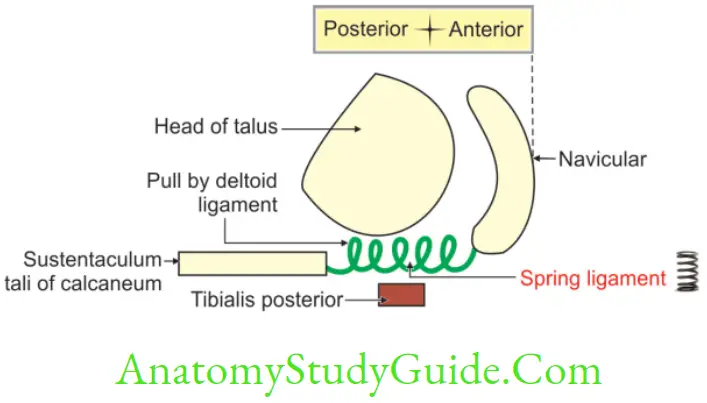
2. Spring ligament Functions
- It supports the head of talus, and
- It provides attachment to deltoid ligament.
3. Spring ligament Applied anatomy: If this ligament is stretched, the navicular and calcaneum move away from each other and the head of the talus sinks and arch is flattened. It is supported by tibialis posterior, tendons of flexor digitorum brevis, and abductor hallucis
Leave a Reply