Local Anaesthesia
The composition of local anaesthetic solutions and their mode of action is vividly described in textbooks on local anaesthesia.
Table of Contents
The reader is hence advised to refer to the same before reading the following text, which is pertinent to paediatric dentistry.
Local Anaesthesia Introduction
Covino and Vassallo (1976) described local anaesthesia (LA) as a loss of sensation in a circumscribed area of the body by a depression of excitation in nerve endings or by inhibition of the conduction process in peripheral nerves.
LA induces loss of sensation without loss of consciousness.
Read And Learn More: Paediatric Dentistry Notes
The local anaesthetic agents with proven potential include the following:
1. Esters of benzoic acid: Cocaine, butacaine, piperocaine
2. Esters of para-aminobenzoic acid: Procaine, chloroprocaine,propoxycaine
3. Amides: Lidocaine or lignocaine, prilocaine,etidocaine, mepivacaine, bupivacaine, dibucaine
4. Quinolones: Centbucridine However, lignocaine is the most widely used anaesthetic agent in dentistry.
It is used to such a wide extent in the current practice that it is often considered synonymous with ‘local anaesthetic’.
Modes Of Local Anaesthesia
These modes of LA are applied in paediatric dentistry.
They are as follows:
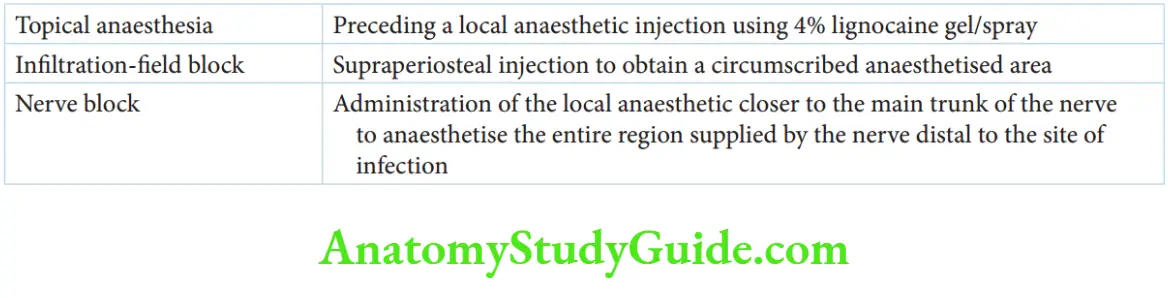
- Topical anaesthesia or surface anaesthesia
- Infiltration-field block
- Nerve block
Other newer, less commonly used modes of LA are discussed at the end of this post.
Topical Anaesthesia (Surface Anaesthesia)
Topical anaesthesia of the mucous membrane the pain/distress associated with the ‘local anaesthetic needle prick’.
Application of the topical anaesthetic on intact mucosa anaesthetises the tissue to a depth of 2–3 mm.
Topical Anaesthesia (Surface Anaesthesia) Procedure:
An appropriate amount of topical anaesthetic has to be applied with a cotton applicator stick over the desired area only.
The application should extend for a sufficiently long time, about 2 minutes, to potentiate topical anaesthesia.
One-minute application is the minimum. It should be applied directly at the injection site only.
Gentle pressure may be applied as dull pressure also potentiates the depth of topical anaesthesia.
Copious application or application over wider, undesired areas can result in an obviously persistent, unpleasant taste.
Itmayalsocauseundesirably wider areas of anaesthesia and rapid absorption into the systemic circulation, leading to a drug overdose.
Agents:
The common agents used to obtain topical anaesthesia are as follows:
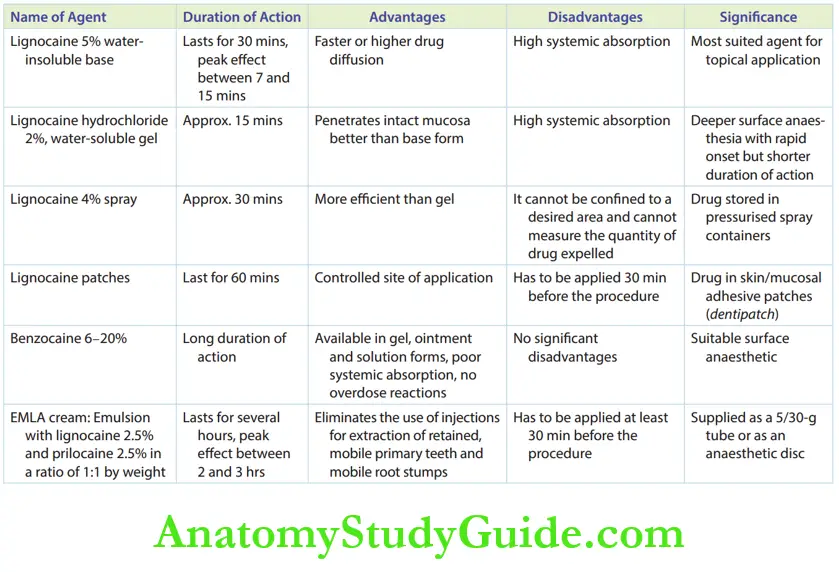
1. Lignocaine
- Lignocaine 5% gel without a vasoconstrictor in a poor water-soluble base form: Increased drug concentration (5% as against 2% being used for systemic administration) facilitates faster or higher drug diffusion. Lignocaine is water-insoluble but is soluble in organic solvents such as alcohol and propylene glycol. It is the most suited agent for topical application. Surface anaesthesia obtained from lignocaine usually lasts for 30 minutes, with a peak effect between 7 and 15 minutes.
- Lignocaine hydrochloride 2% in a water-soluble gel form: It penetrates the intact mucosa better than the base form. However, the risk of systemic absorption is higher.
- Lignocaine 4% spray: This contains the drug with no vasoconstrictor, stored in pressurised spray containers. It does not demonstrate significant efficacy over gels. It is difficult to confine the spray to the desired area and measure the quantity of anaesthetic expelled. Hence, the use of the spray in children intraorally is not widely accepted.
- Lignocaine patches: The drug is impregnated in skin/mucosal adhesive patches of dimensions 2 cm length, 1 cm width and 1 cm height (despatch). The patches have to be applied at least 30 minutes before the procedure to obtain good surface anaesthesia. The anaesthetic effect lasts for at least 60 minutes.
2. Benzocaine 6–20%: It is a suitable surface anaesthetic, available in gel patches, ointments and solutions.
As it is water-insoluble, it demonstrates poor systemic absorption and no overdose reactions. It also accounts for a longer duration of action.
3. EMLA (eutectic mixture of local anaesthetics): EMLA cream is an emulsion containing lignocaine 2.5% and prilocaine 2.5% in a ratio of 1:1 by weight.
Initially, EMLA was designed as a surface anaesthetic for intact skin and was not recommended for use on mucous membranes.
This was because the systemic absorption of the drug through a topical application (especially on the mucosa) was feared to be high.
Recent studies concluded the efficacy and safety of the drug on the oral mucous membrane.
It is a highly potent drug that delivers a nearly complete topical anaesthetic effect.
It gained popularity in paediatrics and is being exemplarily used in procedures such as vein puncture, skin ulcer debridement, circumcision and gynaecological procedures.
It is supplied as a 5/30-g tube or as an anaesthetic disc.
The anaesthetic disc is a white, round, cellulose disc pre-loaded with the drug mixture, packed in a protective laminated foil and surrounded by adhesive tape.
Studies reveal that EMLA eliminates the use of injections in case of extraction of retained, mobile primary teeth and mobile root stumps.
However, EMLA has to be applied at least 30 minutes before the procedure to obtain a good depth of surface anaesthesia that lasts for several hours.
The peak surface anaesthetic action appears between 2 and 3 hours. EMLA is contraindicated in patients with methemoglobinaemia or in those allergic to any type of amide-local anaesthetic.
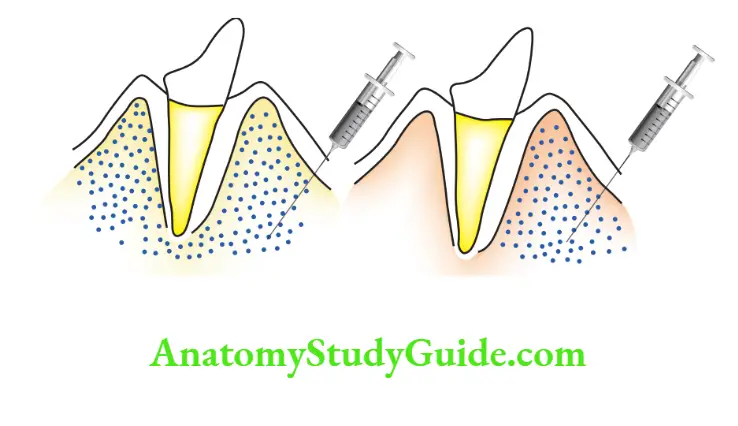
Infiltration – Field Block
A field block is referred to as infiltration or a subperiosteal injection.
The objective is to deposit the solution near the larger terminal nerve to obtain an area of circumscribed anaesthesia.
Afild block around a tooth is obtained by the deposition of the anaesthetic solution above the apices of the tooth for the maxillary arch and below the apices of the tooth for the mandibular arch.
When the alveolar bone is sufficiently cancellous, having large alveoli spaces as in young children, a buccal field block (infiltration) anaesthetises the lingual or palatal tissues also.
When the alveolar bone is more compact and dense, a field block anaesthetises the tissues only on the site of administration.
An infiltration anaesthetises the tooth over which it is administered and most probably over the mesial half of the mesial tooth and the distal half of the distal tooth.
Nerve Block
The nerve block involves the administration of the local anaesthetic closer to the main trunk of the nerve.
It is usually at a distance from the site of anaesthesia desired.
On administering a nerve block, the entire region supplied by the nerve distal to the site of injection is anaesthetised.
The various types of maxillary and mandibular nerve blocks used in relevance to paediatric dentistry are as follows:
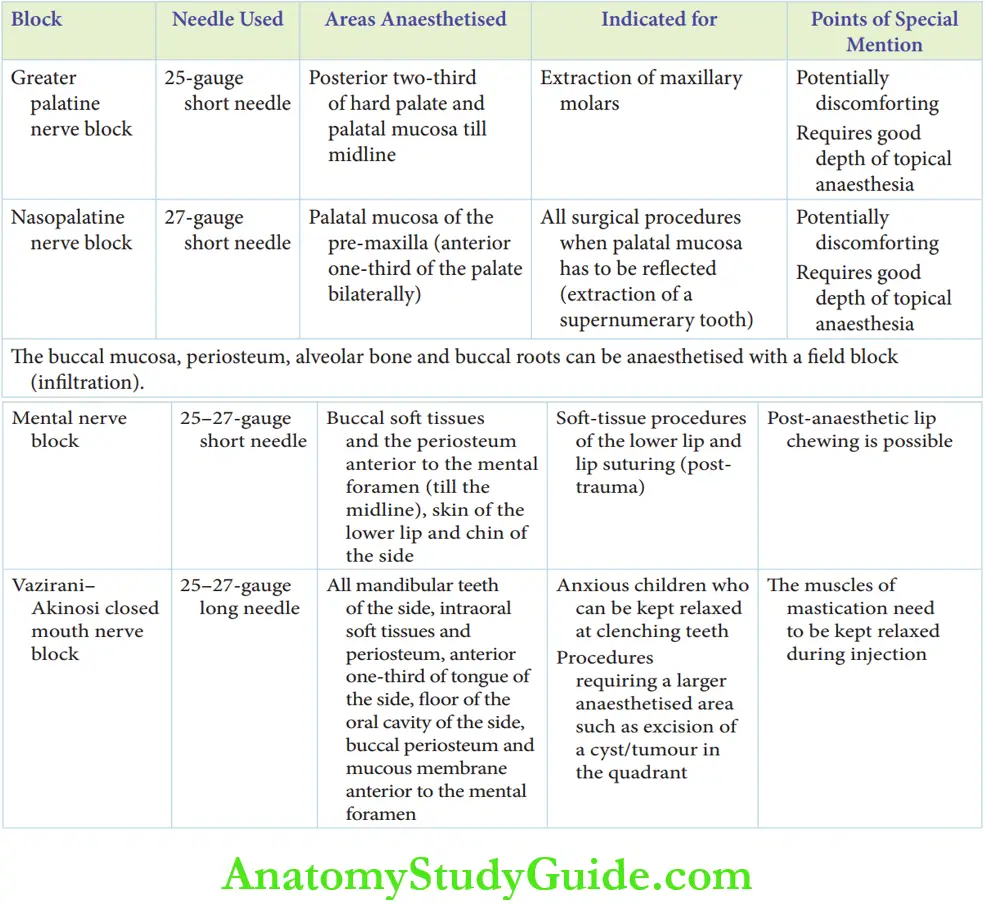
1. Mandibular Nerve Block Techniques
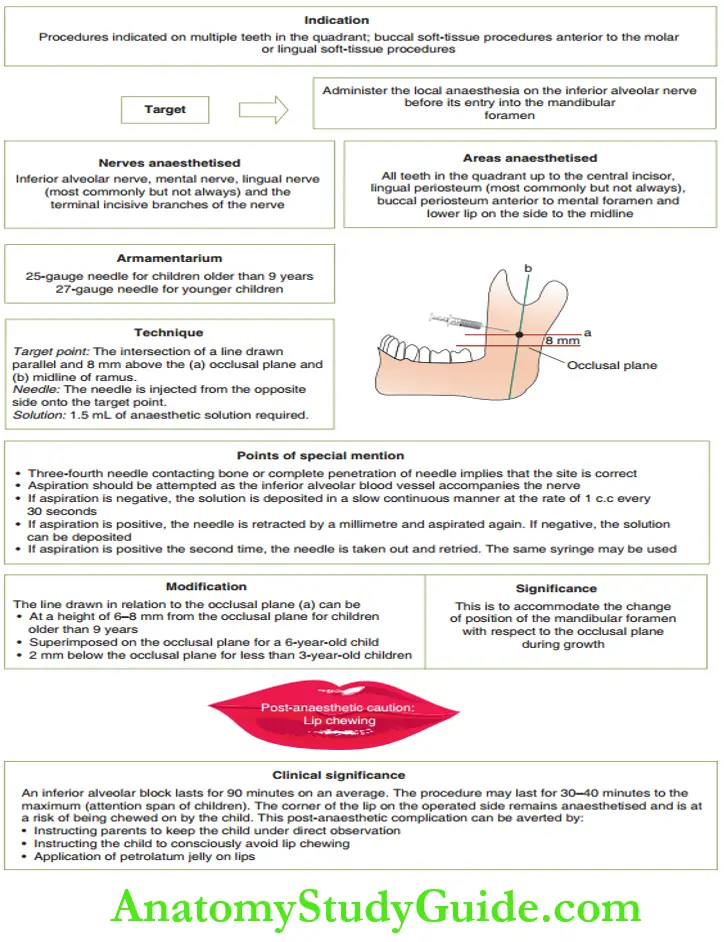
- Inferior alveolar nerve block
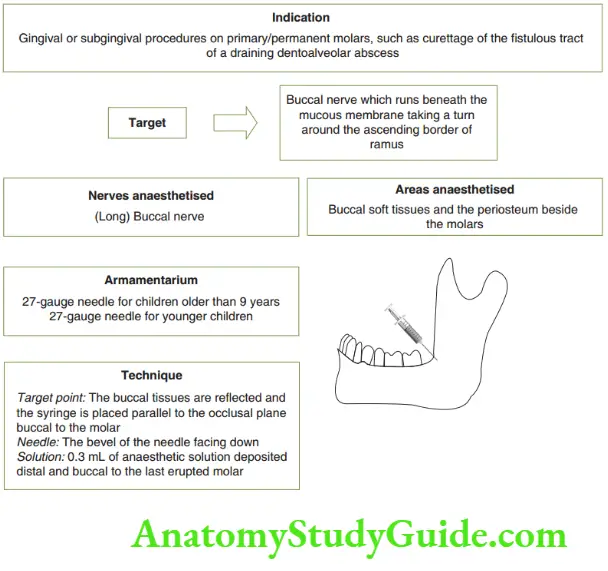
- Buccal nerve block
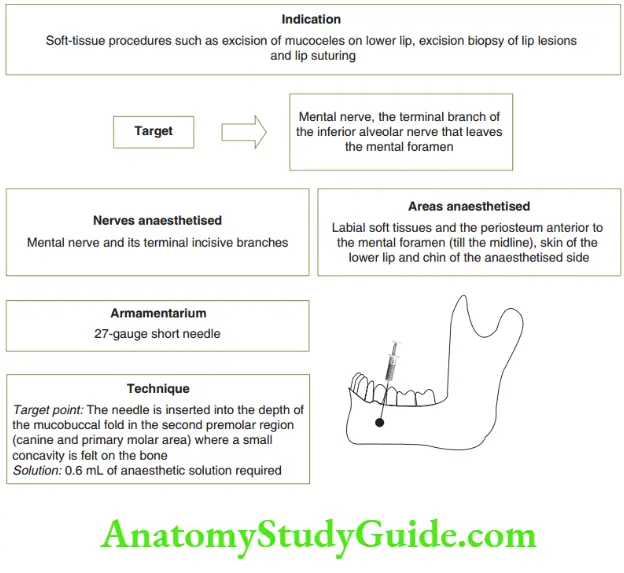
- Mental nerve block
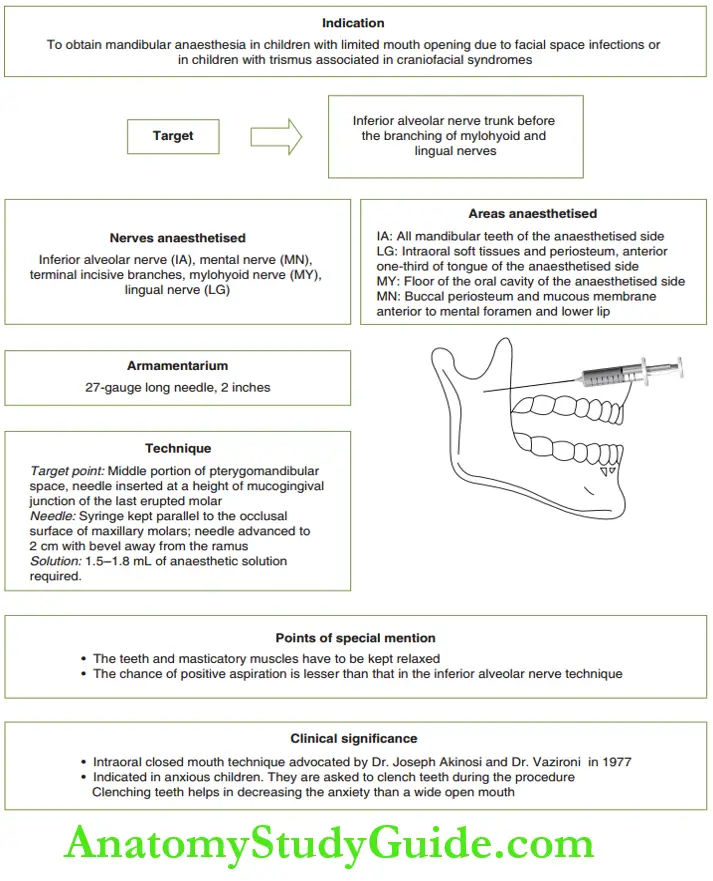
- Vazirani–Akinosi closed mouth nerve block
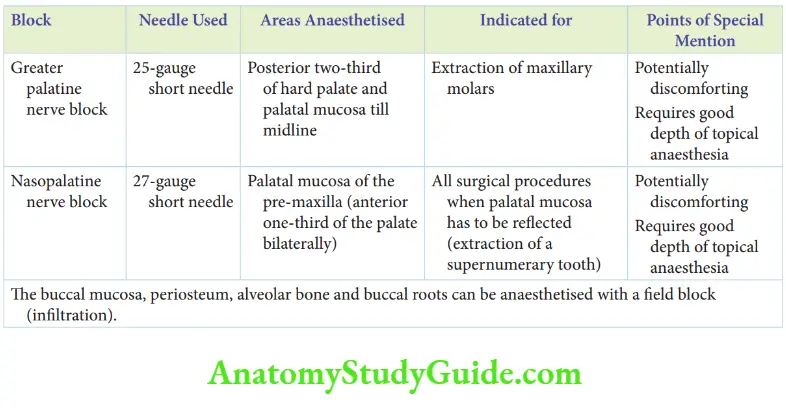
2. Maxillary nerve block techniques
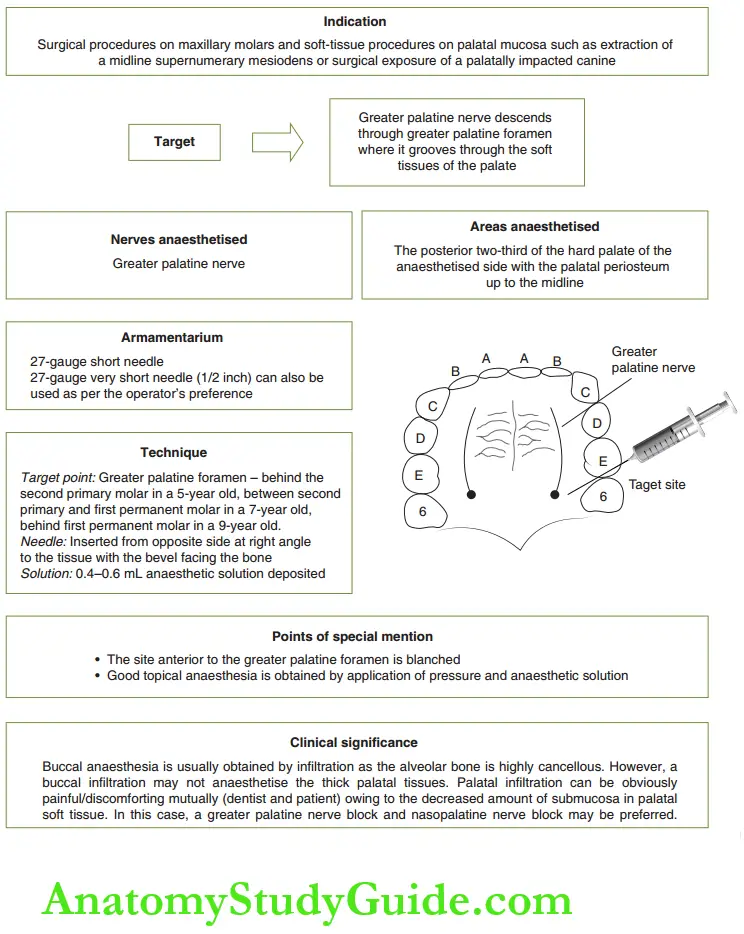
- Greater palatine nerve
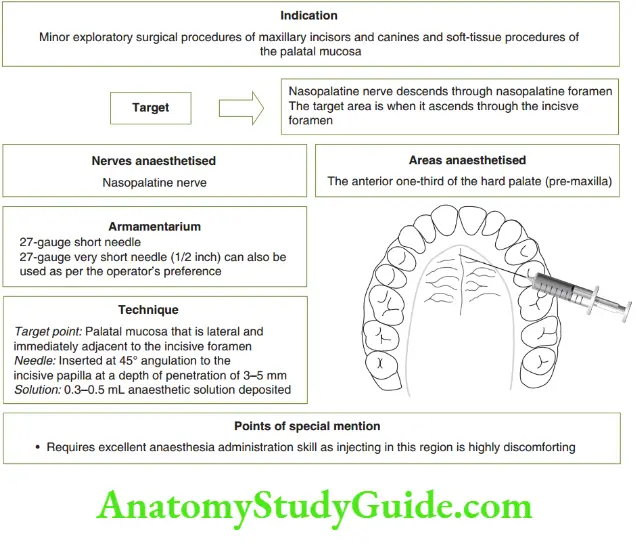
- Nasopalatine nerve block
Clinical Significance Of Local Anaesthetic Administration In Paediatric Operatory
There are three main points to mention under the clinical significance of LA administration in the paediatric dental clinic.
They are the choice of technique, lingual or palatal anaesthesia, and anxiety of the injection.
1. Choice of technique: There is no ideal or prescribed choice of technique for any particular tissue/ procedure.
The objective is to obtain complete anaesthesia of the desired area with the least number of injections and minimal volume of local anaesthesia possible.
2. Lingual or palatal anaesthesia: A question that often arises in a paediatric dental clinic is ‘Can a buccal infiltration anaesthetise lingual (palatal) tissue?’
The Rule of Ten helps to decide if there is a need for separate anaesthetic administration in the lingual or palatal aspect If the sum of the age of the child and the tooth being treated
(1: incisors, 5: second primary molar) gives a value greater than 10, a separate lingual (palatal) LA administration is required. Else, buccal infitration will suffi.
3. Anxiety associated with injection: The injection is associated with psychological pain rather than physical or organic pain.
Injections have been voted as the most anxiety-provoking procedure in a paediatric dental clinic.
Children express immature emotions such as fear, anxiety and crying at the sight of the need rather than at the prick of the needle.
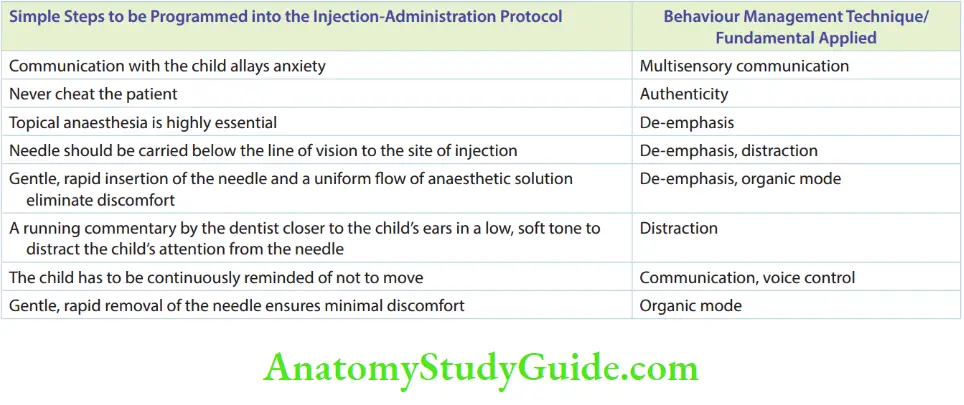
Simple steps can be followed in the injection administration protocol to maintain the cooperation of children.
The steps of handling the child during injecting and the behaviour management associated with the process are listed.
Drug Dosage Of The Local Anaesthetic (Lignocaine)
In the current practice, the commercially used lignocaine has the following constituents:
- 2% solution of lignocaine hydrochloride anaesthetic
- 1:80,000 concentration ofadrenaline – vasoconstrictor
- Sodium metabisulphite– reducing agent
- Methylparaben – preservative
- Thmol– anti-fungal agent
- Benzoic acid – preservative
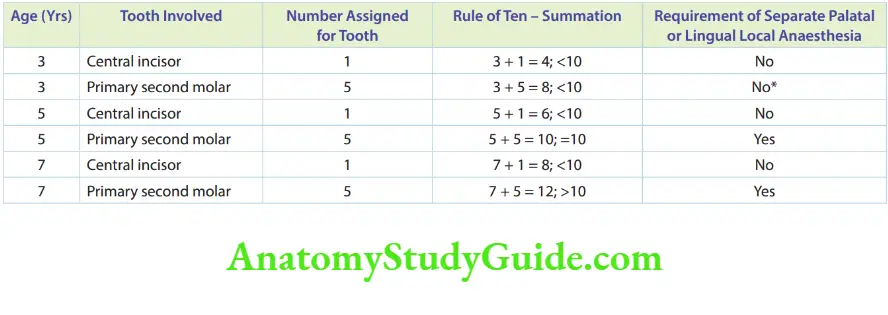
However, check if anaesthesia is profound on the palatal (lingual) root of the tooth before the procedure.
If inadequate, this rule may be breached and a separate palatal (lingual) technique may be resorted to.
Adrenaline is the most commonly used vasoconstrictor that increases the potential of lignocaine by retaining the drug at the site.
It increases the relative safety of lignocaine by decreasing systemic absorption.
At a concentration of 1:80000, it amounts to 0.0125 mg per mL of LA solution.
Adrenaline is an endogenous substance. The combination of LA with adrenaline is preferred in most of conditions except in patients with hyperthyroidism.
LA with adrenaline is strictly contraindicated in hyperthyroidism.
LA is relatively safe in children with cyanotic/cyanotic congenital cardiac ailments. In fact, it is safer than plain lignocaine.
As adrenaline is an endogenous substance, 0.04 mg of adrenaline can safely be administered in a child.
Roughly, 4 mL of LA with adrenaline can be safely administered in a child with a congenital cardiac lesion also.
Sodium metabisulphate, the reducing agent, absorbs the oxygen entrapped in the vial.
In the absence of this reducing agent, the entrapped air oxidises lignocaine hydrochloride, turning the clear solution brown.
This marks the expiry of the drug and mandates disposal.
Methylparaben, the preservative, is most commonly associated with allergies arising from LA administration.
Allergic reactions are more common due to the preservative than due to the drug (lignocaine).
In patients suspected of possible allergic reactions, cardiac lignocaine, that is, lignocaine without a preservative, is administered.
1 mL of 2% lignocaine contains 20 mg of the drug (lignocaine).
Hence, a 1.8 mL cartridge of 2% lignocaine contains 36 mg of lignocaine.
A safe dose of LA with adrenaline is 7.5 mg/kg while the same without adrenaline/vasoconstrictor is 4.4 mg/kg.
Newer Techniques Of Local Anaesthesia Administration
Newer techniques of LA administration have been recently established.
The scientific research on these techniques is being motivated by the objective of making the procedure ‘needle-less’.
This is to counter the ‘injection phobia’ in children. Wand, EDA and jet injector are the common, newer modes of LA administration.
Wand
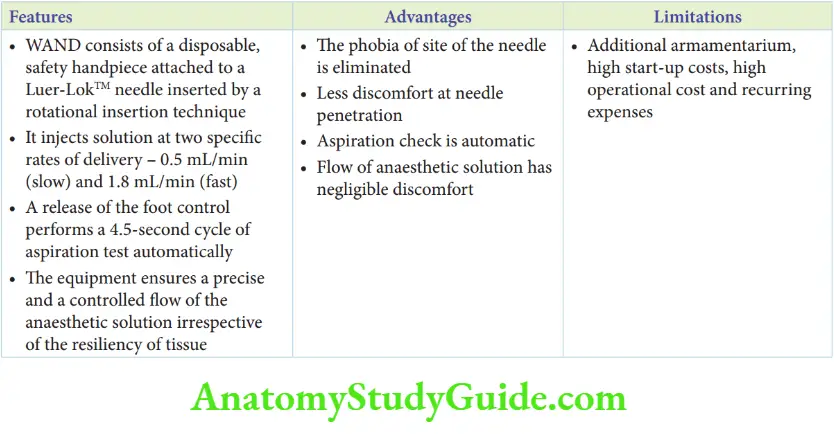
The wand is a computer-controlled, LA drug delivery system.
The equipment ensures a precise and controlled flow of the anaesthetic solution irrespective of the resiliency of the tissue, which may be the periodontal ligament or buccal soft tissues.
Wand Consists Of A Disposable, Safety Handpiece attached to a Luer-LokTM needle.
This handpiece is connected by a 60-inch microchip to a cartridge holder that accepts any standard-sized foot control to deliver pressure for the injection.
The needle is inserted by a rotational insertion technique. It injects solution at two specific rates of delivery, 0.5 mL/min (slow) and 1.8 mL/min (fast).
Delivery of the solution is done by pressing a foot control device.
The release of the foot control device performs a 4.5-second cycle of aspiration test automatically.
Wand Advantages
The advantages of this newer mode of LA delivery are as follows:
The phobia of the site of the needle is eliminated and the hand pieces do not simulate a conventional injection.
There it is performed with a rotational-imitation technique.
Aspiration checks can be quick and automatic.
A controlled flow of anaesthesia is ensured causing negligible levels of discomfort.
However, the requirement of an additional armament atrium, high start-up costs and recurring expenses are the disadvantages.
Electronic Dental Anaesthesia (Eda) – Transcutaneous Electric Nerve Stimulation (Tens)
The use of electrotherapy to control pain has been attempted since the late 18th century.
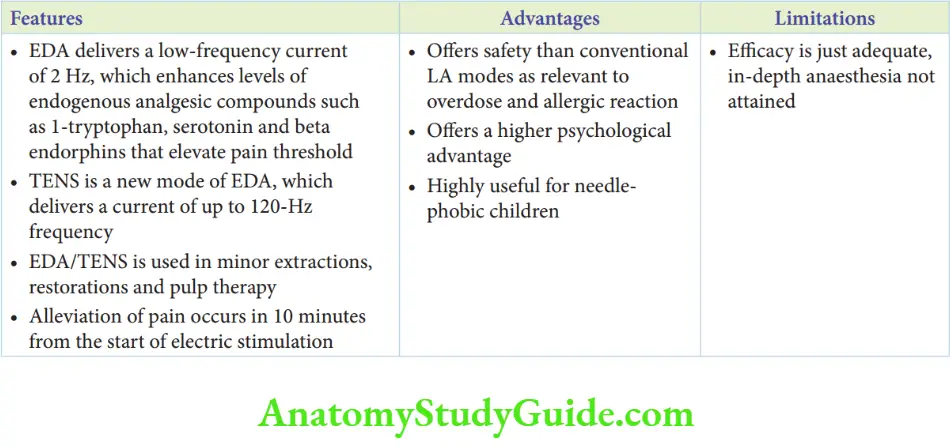
However, interest in this field has been renewed since the 1960s. Electronic dental anaesthesia uses electrodes to deliver a low-frequency current of 2 Hz.
The mechanism of action is believed to be that the current enhances levels of 1-tryptophan, serotonin and beta-endorphins.
These endogenous compounds are analgesics that elevate the pain threshold.
TENS is a new mode of delivering EDA. It delivers a current of up to 120-Hz frequency.
A relatively higher band of current is used for the management of acute orofacial pain in adults.
Alleviation of pain occurs within 10 minutes from the start of electric stimulation.
Dental procedures that have documented success with LA from EDA/TENS are non-surgical periodontal procedures such as scaling, root planning and curettage.
In paediatric dentistry, literature on the use of EDA/TENS in minor extractions, restorations and pulp therapy puts forth the following conclusions:
Offers safety than conventional LA modes as relevant to overdose and allergic reaction
Offers a higher psychological advantage, as ‘the needle’ is non-existent. Highly useful for needle-phobic children
Efficy is just adequate, leaving room for further research to enhance the same.
Jet Injector
The jet injection is a mode of parenteral drug administration where the liquid drug is forced through a small opening (called a jet) under high pressure.
Such a high-pressure-minimal aperture flow can surpass intact skin without puncturing the skin.
This technique was introduced by Figge and Scherer in 1947 and was applied in dentistry by Margetis in 1958.
The jet injection is not a useful alternative to conventional field blocks and nerve blocks.
This technique is used to obtain surface anaesthesia of the mucosa by a jet administration of 0.1–0.2 mL.
The surface anaesthesia obtained is immediate and profound.
Post-administration tissue soreness, its potential to damage periodontal structures and the cost of equipment are the disadvantages.
Local anaesthesia Summary
1. Local anaesthesia has been defined as a loss of sensation in a circumcised area of the body by a depression of exaltation in near-endings or by inhibition of the conduction process in peripheral nerves.
2. Three modes of local anaesthesia applied at paediatric dentistry are as follows:
3. Mandibular block techniques
4. Maxillary nerve blocks
5. The choice of the local anaesthetic technique is not ‘hard and fast’. Obtaining profound anaesthesia, with minimum pricks and minimal drug, is the objective.
6. The site where an infiltration will suffice is decided with the Rule of Ten.
7. Injection administration protocol
- Communication with the child allays anxiety by large.
- Never cheat the patient. Once a dentist cheats, the child’s mind shall retain the thought that all dentists are liars.
- Topical anaesthesia is highly essential.
- The needle should be carried from below the line of vision to the site of injection.
- Gentle, rapid insertion of the needle and uniform flow of anaesthetic solution eliminate discomfort.
- A running commentary by the dentist closer to the child’s ears in a low, soft tone would distract the child’s attention from the needle.
- The child has to be continuously reminded not to move.
- A gentle, rapid removal of the needle ensures very minimal discomfort.
8. Wand is a computer-controlled, local anaesthetic drug delivery system.
9. Electronic dental anaesthesia (EDA)
10. Jet injector
Leave a Reply