Urine Formation Introduction
Urine formation is a blood-cleansing function. Normally, about 26% of cardiac output enters the kidneys to get rid of unwanted substances.
Table of Contents
- Kidneys excrete unwanted substances along with water as urine.
- The unwanted substances include metabolic end products and those substances, which are present in excess quantities in the body.
- Normally, about 1-5 liters of urine is formed every day. The mechanism of urine formation includes several processes.
Read And Learn More: Medical Physiology Notes
- First, when blood passes through the glomerular capillaries, the plasma is filtered into the Bowman’s capsule. This process is called glomerular filtration.
- When the filtrate from Bowman’s capsule passes through the tubular portion of the nephron, it undergoes various changes both in quality and quantity.
- Many wanted substances like glucose, amino acids, water, and electrolytes are reabsorbed from the tubules.
- This process is called tubular reabsorption.
- And, some unwanted substances are secreted into the tubule from peritubular blood vessels.
This process is called tubular secretion or excretion.

Thus, urine formation includes three processes:
- Glomerular filtration
- Tubular reabsorption
- Tubular secretion.
Among these three processes filtration is the function of the glomerulus.
Reabsorption and secretion are the functions of the tubular portion of the nephron.
Glomerular Filtration
Introduction
Glomerular filtration is the process by which the blood that passes through glomerular capillaries is filtered through the filtration membrane.
It is the first process of urine formation.
Filtration Membrane
The filtration membrane is formed by three layers:
- The glomerular capillary membrane
- Basement membrane
- Visceral layer of Bowman’s capsule.
1. Glomerular Capillary Membrane
The glomerular capillary membrane is formed by a single layer of endothelial cells which are attached to the basement membrane.
The capillary membrane has many pores called fenestra or filtration pores with a diameter of 0.1 p.
2. Basement Membrane
The basement membrane of glomerular capillaries fuses with the basement membrane of the visceral layer of Bowman’s capsule.
Thus, the basement membranes, which are fused together, form the separation between the glomerular capillary endothelium and the epithelium of the visceral layer of Bowman’s capsule.
3. Visceral Layer of Bowman’s Capsule
This is composed of a single layer of flattened, epithelial cells resting on a basement membrane. Each cell is connected to the basement membrane by cytoplasmic extensions called pedicles or feet.
The pedicles are arranged in an interdigitating manner leaving small cleft-like spaces in between. The cleft-like space is called a slit pore. The epithelial cells with pedicles are called podocytes.
Process of Glomerular Filtration
When the blood passes through the glomerular capillaries, the plasma is filtered into the Bowman’s capsule.
All the substances of plasma are filtered except the plasma proteins. The filtered fluid is called glomerular filtrate.
Ultrafsltication
The glomes-filtration is called ultrafiltration because even the minute particles are filtered. But, the plasma proteins are not filtered due to their large molecular size.
The protein molecules are larger than the slit pores present in the endothelium of capillaries. Thus, the glomerular filtrate contains all the substances present in plasma except the plasma proteins.
Method Of Collection Of Glomerular Filtrate
The glomerular filtrate is collected in experimental animals by the micropuncture technique.
This technique involves the insertion of a micropipette into the Bowman’s capsule and the aspiration of filtrate.
Glomerular Filtration Rate (GFR)
Glomerular filtration rate (GFR) is defined as the total quantity of filtrate formed in all the nephrons of both kidneys in the given unit of time.
The normal GFR is 125 mL per minute or about 180 liters per day.
Filtration Fraction
Filtration fraction is the fraction (portion) of the renal plasma which becomes the filtrate. It is the ratio between renal plasma flow and glomerular filtration rate. It is expressed in percentage.

The normal filtration fraction varies from 15-20%.
Pressures Determining Filtration
The pressures, which determine the GFR are:
- Glomerular capillary pressure
- Colloidal osmotic pressure in the glomeruli
- Hydrostatic pressure in the Bowman’s capsule. These pressures determine the GFR by either favoring or opposing the filtration.
1. Glomerular Capillary Pressure
It is the pressure exerted by the blood in glomerular capillaries. It is about 60 mm Hg and, varies between 45 and 70 mm Hg.
Glomerular capillary pressure is the highest capillary pressure in the body. This pressure favors glomerular filtration.
2. Colloidal Osmotic Pressure
It is exerted by plasma proteins in the glomerular The plasma proteins are not filtered through the glomerular capillaries and remain in the glomerular capillaries.
These proteins develop the colloidal osmotic pressure which is about 25 mm Hg. It opposes glomerular filtration.
3. Hydrostatic Pressure in Bowman’s Capsule
It is the pressure exerted by the filtrate in Bowman’s capsule. It is also called capsular pressure. It is about 15 mm Hg. It also opposes glomerular filtration.
Net Filtration Pressure
Net filtration pressure is the balance between pressure favoring filtration and pressures opposing filtration.
It is otherwise known as effective filtration pressure or essential filtration pressure. It is very essential for the maintenance of GFR.
The net filtration pressure =

The normal net filtration pressure is about 20 mm Hg, and, it varies between 15 and 20 mm Hg.
Starling’s Hypothesis and Starling Forces
The determination of net filtration pressure is based on Starling’s hypothesis.
Starling’s hypothesis states that the net filtration through the capillary membrane is proportional to the hydrostatic pressure difference across the membrane minus the oncotic pressure difference.
The hydrostatic pressure within the glomerular capillaries is the glomerular capillary pressure.
All the pressures involved in the determination of filtration are called Starling forces.
Filtration Coefficient
The filtration coefficient is the GFR in terms of net filtration pressure, it Is the GFR per mm Hg of net filtration pressure.
For example, when GFR is 125 mL/min and Turnon pressure is 20 mm Hg.
The Filtration coefficient =125ml/20mmhg=6.25mL/mm Hg.
Factors Regulating (Affecting) GFR
1. Renal Blood Flow
It is the most important factor that is necessary for glomerular filtration.
GFR is directly proportional to renal blood flow. Normal blood flow to both kidneys is 1300 mL per minute. The renal blood flow itself is controlled by autoregulation.
Tubuloglomerular Feedback
Tubuloglomerular feedback is the mechanism that regulates GFR through renal tubule and macula densa
Macula densa of the juxtaglomerular apparatus is situated in the terminal portion of the thick ascending limb very close to afferent arteriole.
It is sensitive to the sodium chloride in the tubular fluid.
When the glomerular filtrate passes through the terminal portion of the thick ascending segment, the macula densa acts like a sensor.
It detects the concentration of sodium chloride in the tubular fluid and accordingly alters the glomerular blood flow and GFR.
Macula densa cells detect the sodium chloride concentration via Na+-K+-2CI~ co-transporter (NKCC2) in its luminal membrane.

When the concentration of sodium chloride increases in the filtrate
When GFR increases, the concentration of sodium chloride increases in the filtrate.
By detecting this, the macula densa releases adenosine from ATR Adenosine causes constriction of the afferent arteriole.
So the blood flow through the glomerulus decreases leading to a decrease in GFR.
Adenosine acts on afferent arteriole via adenosine A-, receptors. There are several other factors that increase or decrease the sensitivity of tubuloglomerular feedback.
Factors increasing the sensitivity of tubuloglomerular feedback:
- Adenosine
- Thromboxane
- Prostaglandin E2
- Hydroxyeicosa ethanoic acid
Factors decreasing the sensitivity of tubuloglomerular feedback:
- Atrial natriuretic peptide
- Prostaglandin l2
- Cyclic AMP
- Nitrous oxide
When the concentration of sodium chloride decreases in the filtrate
Conversely, when GFR decreases, the concentration of sodium chloride decreases in the filtrate.
Now macula densa secretes prostaglandin (PGE2), bradykinin, and renin.
PGE2 and bradykinin cause dilatation of afferent arteriole. Renin induces the formation of angiotensin II which causes constriction of efferent arteriole.
The dilatation of afferent arteriole and constriction of efferent arteriole leads to an increase in glomerular blood flow and GFR.
3. Glomerular Capillary Pressure
The GFR is directly proportional to glomerular capillary pressure. Normal glomerular capillary pressure is 60 mm Hg. When glomerular capillary pressure increases, the GFR also increases. The capillary pressure, in turn, depends upon the renal blood flow and arterial blood pressure.
4. Colloidal Osmotic Pressure
The GFR is inversely proportional to colloidal osmotic pressure which is exerted by plasma proteins in the glomerular capillary blood. Normal colloidal osmotic pressure is 25 mm Hg.
During dehydration or increased plasma protein level, the colloidal osmotic pressure is high and GFR decreases.
During hypoproteinemia, colloidal osmotic pressure is low, and GFR increases.
5. Hydrostatic Pressure in Bowman’s Capsule
GFR is inversely proportional to this. Normally, it is 15 mm Hg.
When the hydrostatic pressure increases in the Bowman’s capsule, it decreases GFR.
The hydrostatic pressure in Bowman’s capsule increases in conditions like obstruction of the urethra and edema of the kidney beneath the renal capsule.
6. Constriction of Afferent Arteriole
The constriction of afferent arteriole reduces the blood flow to the glomerular capillaries which in turn reduces GFR.
7. Constriction of Efferent Arteriole
If the efferent arteriole is constricted, initially the GFR increases because of the stagnation of blood in the capillaries. Later when all the substances are filtered from this blood, further filtration does not occur.
It is because the efferent arteriolar constriction prevents the outflow of blood from the glomerulus and no fresh blood enters the glomerulus for filtration.
8. Systemic Arterial Pressure
It is responsible for the flow of blood through various organs including kidneys.
However, an increase in mean arterial blood pressure up to 180 mm Hg or a reduction up to 60 mm Hg does not alter the renal blood flow or GFR.
It is due to the autoregulatory mechanism.
Variation in pressure above 180 mm Hg or below 60 mm Hg affects the renal blood flow and GFR accordingly because the autoregulatory mechanism fails beyond this range.
9. Sympathetic Stimulation
Afferent and efferent arterioles are supplied by sympathetic nerves.
The mild or moderate stimulation of sympathetic nerves does not cause any significant change either in renal blood flow or GFR.
Strong sympathetic stimulation causes severe constriction of the blood vessels by releasing the neurotransmitter substance, noradrenaline.
The effect is more severe on the efferent arterioles than on the afferent arterioles.
So, initially, there is an increase in filtration but later it decreases. However, if the stimulation is continued for more than 30 minutes, there is recovery of both renal blood flow and GFR.
It is because of a reduction in sympathetic neurotransmitters.
10. Surface Area of Capillary Membrane
GFR is directly proportional to the surface area of the capillary membrane.
If the glomerular capillary membrane is affected as in the cases of some renal diseases, the surface area for filtration decreases. So there is a reduction in GFR.
11. Permeability of Capillary Membrane
GFR is directly proportional to the permeability of the glomerular capillary membrane.
In many abnormal conditions like hypoxia, lack of blood supply, presence of toxic agents, etc.
the permeability of the capillary membrane increases. In such conditions, even plasma proteins are filtered and excreted in urine.
12. Contraction of Glomerular Mesangial Cells
Glomerular mesangial cells are situated in between the glomerular capillaries.
Contraction of these cells decreases the surface area of capillaries resulting in a reduction in GFR.
13. Hormonal and Other Factors
Many hormones and other secretory factors alter GFR by affecting the blood flow through the glomerulus.
Factors increasing GFR
- Atrial natriuretic peptide
- Brain natriuretic peptide
- cAMP
- Dopamine
- Endothelial-derived nitric oxide
- Prostaglandin (PGE2).
Factors decreasing GFR
- Angiotensin II
- Endothelins
- Noradrenaline
- Platelet-activating factor
- Platelet-derived growth factor
- Prostaglandin (PGF2).
Tubular Reabsorption
Introduction
Tubular reabsorption is the process by which water and other substances are transported from renal tubules back to the blood.
When the glomerular filtrate flows through the tubular portion of the nephron, both quantitative and qualitative changes occur.
Large quantities of water (more than 99%), electrolytes, and other substances are reabsorbed by the tubular epithelial cells.
The reabsorbed substance move into the interstitial fluid of the renal reduce, from here, the substances move into the blood in peritubular capillaries.
Sines the substances are taken back into the blood from the glomerular filtrate, the entire process is called tubular reabsorption.
Method Of Collection Of Tubular Fluid
There are two methods to collect the tubular fluid for analysis.
Micropuncture Technique
A micropipette is inserted into the Bowman’s capsule and different parts of tubular portion in the nephrons of experimental animals, to collect the fluid.
The fluid samples are analyzed and compared with each other to assess the changes in different parts of the nephron.
Stop Flow Method
The ureter is obstructed so that the back pressure rises and stops the glomerular filtration.
The obstruction is continued for 8 minutes. It causes some changes in the fluid present in different parts of the tubular portion.
Later, the obstruction is released, and about 30 samples of 0.5 mL of urine are collected separately at regular intervals of 30 seconds.
The first sample contains the fluid from the collecting duct.
The successive samples contain the fluid from the distal convoluted tubule, loops of Henle, and proximal convoluted tubule respectively. All the samples are analyzed.
Selective Reabsorption
Tubular reabsorption is known as selective reabsorption because the tubular cells of the kidney selectively reabsorb the substances present in the glomerular filtrate, according to the
needs of the body. The essential substances which are necessary for the body such as glucose, amino acids and vitamins are completely reabsorbed from the renal tubule.
Whereas unwanted substances like metabolic waste products are not reabsorbed.
Mechanism Of Reabsorption
The basic transport mechanisms involved in tubular reabsorption are of two types:
- Active reabsorption
- Passive reabsorption.
1. Active Reabsorption
Active reabsorption is the movement of molecules against the electrochemical (uphill) gradient.
It needs liberation of energy which is derived from ATP.
Substances reabsorbed actively
The substances reabsorbed actively from the renal tubule are sodium, calcium, potassium, phosphates, sulfates, bicarbonates, glucose, amino acids, ascorbic- acid, uric acid, and ketone bodies.
2. Passive Reabsorption
Passive reabsorption is the movement of molecules along the electrochemical (downhill) gradient.
This process does not need energy. Substances reabsorbed passively The substances reabsorbed by passive transport are chloride, urea, and water.
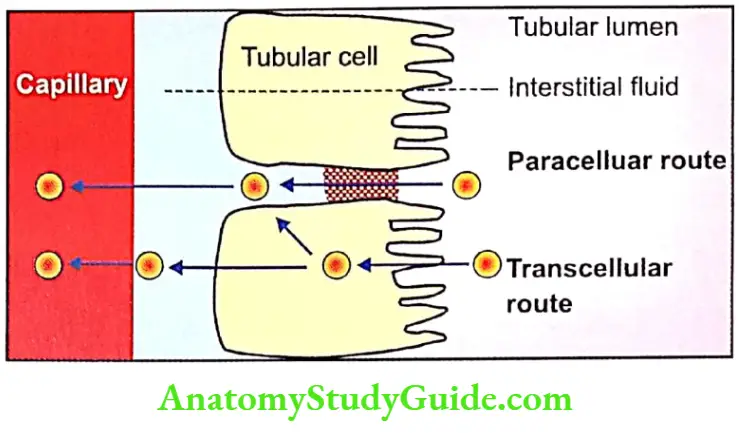
Routes Of Reabsorption
There are two routes for the substances to be reabsorbed from the tubular lumen into the peritubular capillary called transcellular and paracellular routes.
Transcellular Route
In this route, the substances move through the cell. It includes:
- Transport from the tubular lumen into the tubular cell through the apical (luminal) surface of the cell membrane
- Transport from the tubular cell into the interstitial fluid
- Transport from the interstitial fluid into the capillary.
Paracellular Route
In this route, the substances move through the intracellular space. It includes:
- Transport from the tubular lumen into an interstitial fluid present in lateral intercellular space through the tight junction between the cells.
- Transport from the interstitial fluid into the capillary
The reabsorption of the substances occurs in almost all the segments of the tubular portion of the nephron.
1. Substances Reabsorbed from Proximal Convoluted Tubule
About 7/8 of the filtrate (about 88%) is reabsorbed in the proximal convoluted tubule.
The proximal convoluted tubule is formed by brush-bordered epithelial cells. The brush border increases the surface area for reabsorption.
Substances reabsorbed from the proximal convoluted tubule are glucose, amino acids, sodium, potassium, calcium, bicarbonates, chlorides, phosphates, uric acid, and water.
2. Substances Reabsorbed from Loop of Henle
The substances reabsorbed from the loop of Henle are sodium and chloride.
3. Substances Reabsorbed from Distal Convoluted Tubule
Sodium, calcium, bicarbonate, and water are reabsorbed from the distal convoluted tubule.
Regulation Of Tubular Reabsorption
Tubular reabsorption is regulated by three factors:
- Glomerulotubular balance
- Hormonal factors
- Nervous factors.
1. Glomerulotubular Balance
Glomerulotubular balance is the balance between the filtration and reabsorption of solutes and water in the kidney.
When GFR increases, the tubular load of solutes and water in the proximal convoluted tubule is increased.
It is followed by an increase in the reabsorption of solutes and water. This process helps in the constant reabsorption of solutes particularly sodium and water from the renal tubule.
Mechanism of glomerulotubular balance
Glomerulotubular balance occurs because of osmotic pressure in the peritubular capillaries.
When GFR increases, more amount of plasma proteins accumulate in the glomerulus.
Consequently, the osmotic pressure increases in the blood by the time it reaches efferent arteriole and peritubular capillaries.
The elevated osmotic pressure in the peritubular capillaries increases the reabsorption of sodium and water from the tubule into the capillary blood.
2. Hormonal Factors
The hormones which regulate GFR

3. Nervous Factor
Activation of the sympathetic nervous system increases the tubular reabsorption (particularly of sodium) from renal tubules.
It also increases tubular reabsorption indirectly by stimulation of renin from juxtaglomerular cells.
Renin causes the formation of angiotensin II which increases sodium reabsorption (Chapter 50).
Threshold Substances
Depending upon the degree of reabsorption, the various substances are classified into three categories:
- High threshold substances
- Low threshold substances
- Nonthreshold substances.
1. High Threshold Substances
High-threshold substances are those substances that do not appear in urine under normal conditions.
The food substances like glucose, amino acids, acetoacetate ions, and vitamins are completely reabsorbed from renal tubules and do not appear in urine under normal conditions.
These substances can appear in urine, only if their concentration in plasma is abnormally high or in renal diseases when reabsorption is affected.
So, these substances are called high-threshold substances.
2. Low Threshold Substances
Low-threshold substances are substances that appear in urine even under normal conditions.
The substances such as urea, uric acid, and phosphate are reabsorbed to a little extent.
These substances appear in urine even under normal conditions.
3. Nonthreshold Substances
Nonthreshold substances are those substances that are not at all reabsorbed and are excreted in urine irrespective of their plasma level.
The metabolic end products such as creatinine are the non-threshold substances.
Transport Maximum – Tm Value
Tubular transport maximum or Tm is the rate at which a substance is reabsorbed from the renal tubule.
The substances reabsorbed actively from the renal tubules require some specific transport system.
The rate of reabsorption of any substance depends upon the rate at which this specific transport system operates.
The transport system, in turn, depends upon the carrier substances or enzymes.
So. for every actively reabsorbed substance, there is a maximum rate at which it could be reabsorbed.
For example, the transport maximum for glucose. (TmG) is 375 mg/minute in adult males and about 300 mg/minute in adult females.
Threshold Level in Plasma for Substances having Tm Value
The renal threshold is the plasma concentration at which a substance appears first in urine.
Every substance having a Tm value has also a threshold level in plasma or blood.
Below that threshold level, the substance is completely reabsorbed and does not appear in the urine.
When the concentration of that substance reaches the threshold. the excess amount is not reabsorbed and so it appears in urine.
This level is called the renal threshold of a substance.
For example, the renal threshold for glucose is 180 mg/dL. That is, glucose is completely reabsorbed from tubular fluid if its concentration in the blood is below 180 mg/dL.
So. the glucose does not appear in the urine. When the blood level of glucose reaches 180 mg/dL it is not reabsorbed completely; hence it appears in urine.
Reabsorption Of Important Substances
Reabsorption of Sodium
From the glomerular filtrate, 99% of sodium is reabsorbed. Two-thirds of sodium is reabsorbed in the proximal convoluted tubule and the remaining one-third in other segments (except descending limb) and collecting duct.
Sodium reabsorption occurs in three steps:
Transport from the lumen of renal tubules into the tubular epithelial cells Transport from tubular cells into the interstitial fluid
3. Transport from Interstitial Fluid to the Blood
From the interstitial fluid, sodium ions enter the peritubular capillaries by a concentration gradient.
In the distal convoluted tubule, sodium reabsorption is stimulated by the hormone aldosterone secreted by the adrenal cortex.
Reabsorption of Water
Reabsorption of water occurs from proximal and distal convoluted tubules and in the collecting ducts.
Reabsorption of water from proximal convoluted tubule – obligatory water reabsorption
Obligatory reabsorption is the type of reabsorption of water in the proximal convoluted tubule, which is secondary to sodium reabsorption.
The proximal convoluted tubule is highly permeable to water.
However, water reabsorption is secondary (obligatory) to sodium reabsorption.
When sodium is reabsorbed from the tubule, the osmotic pressure decreases.
It causes osmosis of water from the renal tubule.
Reabsorption of water from distal convoluted tubule and coll-acting duct – facultative water reabsorption.
Facultative reabsorption is the type of water reabsorption in distal convoluted tubule and collecting duct that occurs by the activity of antidiuretic hormone (ADH).
Normally, the distal convoluted tubule
and the collecting duct are not permeable to water. But in the presence of antidiuretic hormone (ADH), these segments become permeable to water.
So, water is reabsorbed from the distal convoluted tubule and collecting duct.
Mechanism of action of antidiuretic hormone
ADH combines with V2 receptors in the tubular epithelial membrane and activates adenyl cyclase, to form cyclic AMP.
This cyclic-AMP increases the permeability of the tubules for water.
Earlier it was thought that ADH facilitates water reabsorption by acting on the simple water channels.
Now it is found that the water channels are formed by snecTc proteins called aquaporins.
Aquaporins
Aquaporins (AQP) are membrane proteins that function as water channels.
Though about 10 aquaporins are identified in mammals only 5 are found in humans.
Aquaporin-1, 2, and 3 are present in renal tubules. Aquaporin-4 is present in the brain and aquaporin-5 is found in salivary glands.
Aquaporin 2 forms the water channels in renal tubules. It is found that ADH increases water reabsorption in distal convoluted tubules and collecting ducts by regulating the aquaporin.
Reabsorption of Glucose
Glucose is completely reabsorbed in the proximal convoluted tubule. It is transported by secondary active transport (sodium co-transport) mechanism.
Glucose and sodium bind to a common carrier protein in the luminal membrane of the tubular epithelium and enter the cell.
The carrier protein is called sodium-dependant glucose transporter 2 (SGLT 2).
From tubular cells, glucose is transported into the medullary interstitium by another carrier protein called glucose transporter 2 (GLUT 2).
Tubular maximum for glucose (TmG)
In adult males TmG is 375 mg/minute and in adult females it is about 300 mg/minute.
The renal threshold for glucose
The renal threshold for glucose is 180 mg/dL in venous blood. When the blood level reaches 180 mg/dL glucose is not reabsorbed completely and appears in the urine.
Splay
Splay means deviation. With a normal GFR of 125 mL/ minute and TmG of 375 mg/minute in an adult male, the predicted (expected) renal threshold for glucose should be 300 mg/dL. But actually, it is only 180 mg/dL.
When the renal threshold curves are drawn by using these values, the actual curve deviates from the ‘should be’ or predicted or ideal curve.

This type of deviation is called splay. The splay is because of the fact that all the nephrons do not have the same filtering and reabsorbing capacities.
Reabsorption of Amino Acids
Amino acids are also reabsorbed completely in the proximal convoluted tubule. Amino acids are reabsorbed actively by the secondary active transport mechanism along with sodium.
Reabsorption of Bicarbonates
Tvrboneie is absorbed actively, mostly in proximal It is reabsorbed in the form of carbon dioxide
Bicarbonate is mostly present as sodium bicarbonate in the filtrate. Sodium bicarbonate dissociates into sodium and bicarbonate ions in the tubular lumen.
Sodium diffuses into tubular cells in exchange for hydrogen. Bicarbonate combines with hydrogen to form carbonic acid.
Carbonic acid dissociates into carbon dioxide and water in the presence of carbonic anhydrase. Carbon dioxide and water enter the tubular cell.
In tubular cells, carbon dioxide combines with water to form carbonic acid.
It immediately dissociates into hydrogen and bicarbonate. Bicarbonate from the tubular cell enters the interstitium.
There it combines with sodium to form sodium bicarbonate.
Tubular Secretion
Introduction
Tubular secretion is the process by which substances are transported from blood into renal tubules.
It is also called tubular excretion. In addition to reabsorption from renal tubules, some substances are also secreted into the lumen from the peritubular capillaries through the tubular epithelial cells.
In experimental conditions, the dye phenol red was the first substance found to be secreted in renal tubules.
Later many other substances were found to be secreted such as:
- Para-aminohippuric acid (PAH)
- Diodrast
- Hydroxyindole acetic acid
- Amino derivatives
- Penicillin.
Substances Secreted In Different Segments Of Renal Tubules
- Potassium is secreted actively by sodium-potassium pump in proximal and distal convoluted tubules and collecting ducts.
- Ammonia is secreted in the proximal convoluted tubule.
- Hydrogen ions are secreted in the proximal and distal convoluted tubules. Maximum hydrogen ion secretion occurs in the proximal tubule. Thus, urine is formed in the nephron by the processes of glomerular filtration, selective reabsorption, and tubular secretion.
Leave a Reply