Minor Oral Surgical Procedures Introduction
Minor oral surgical procedures are those that involve the surgical exploration of software tissues intraorally.
Table of Contents
They may be performed to drain a pointing abscess, remove a soft tissue lesion, surgically alter the frenum and aid the eruption of teeth.
These procedures are usually performed under local anaesthesia unless the behaviour management of the child requires general anaesthesia.
The commonly performed minor oral surgical procedures in paediatric dentistry are as follows:
Read And Learn More: Paediatric Dentistry Notes
- Incision and drainage
- Biopsy
- Frenectomy
- Operculectomy
- Extraction of unerupted supernumerary tooth Of these, the incision and drainage procedure. It involves a sharp exploration of an Apus-laden dentoalveolar abscess using the no. 11 blade. The other procedures are explained next.
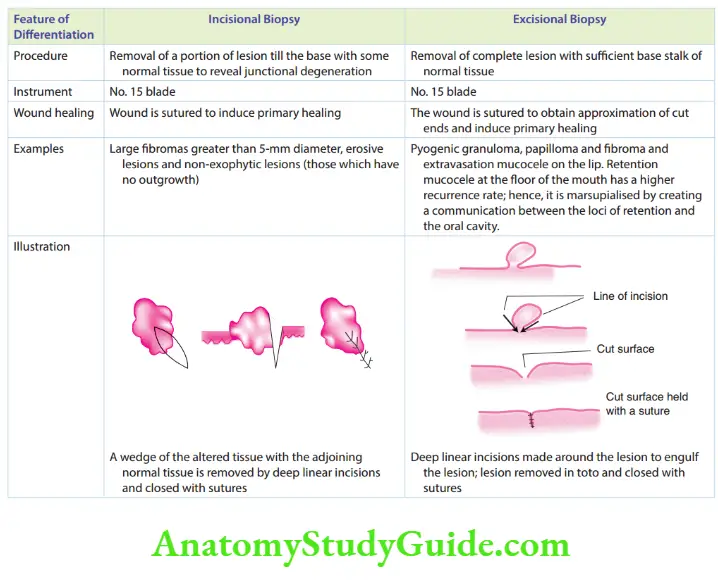
Biopsy
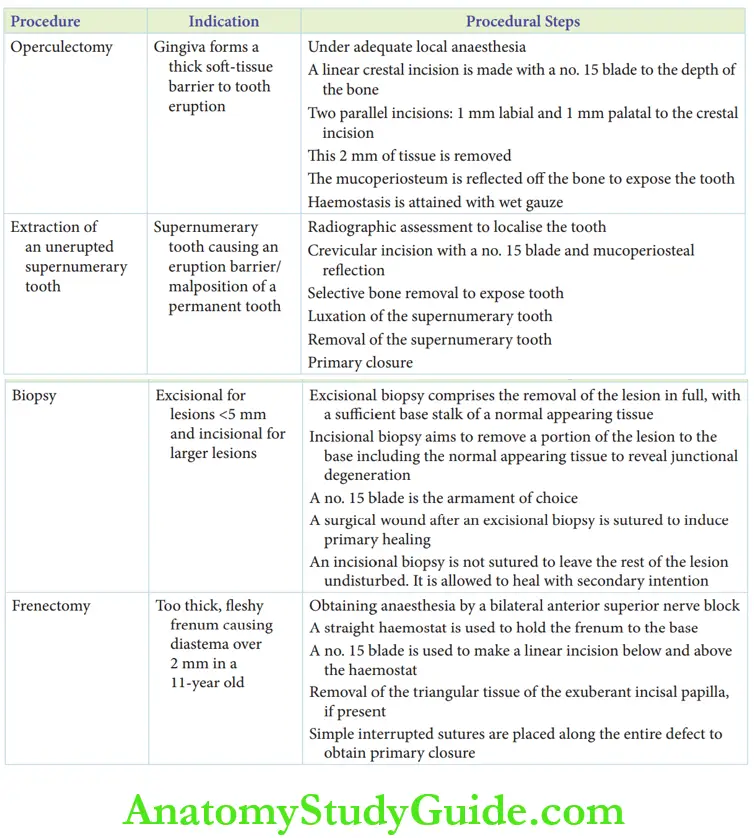
Excisional biopsy is performed for small lesions, maybe for lesions less than 5 mm in diameter.
Larger lesions require an incisional biopsy. compares excisional and incisional biopsy techniques.
Any biopsy requires adequate local anaesthesia. The possibility of the lesion being a vascular lesion has to be ruled out before doing a biopsy.
On palpation, a vascular lesion demonstrates vibration which is felt by the finger.
This is due to blood filling the lesion. This sign is called a ‘vascular thrill’.
It has to be examined before a biopsy. However, intraoral vascular lesions are rare in children.
Frenectomy
Frenum is a muscular attachment between the lip and the gingiva.
The labial frenum, lingual frenum and buccal free are the different frena in the oral cavity.
The maxillary labial frenum is the most commonly indicated frenum for excision.
The release of the fire bands in the frenum is called fibrotomy. However, the indication for fibrotomy is not specific with respect to paediatric dentistry.
Hence only a frenectomy is performed, almost always.
Frenectomy of the maxillary labial frenum is indicated in the following cases:
1. Frenum associated with a median diastema of >2 mm in a child older than 11 years (after the eruption of the maxillary canine)
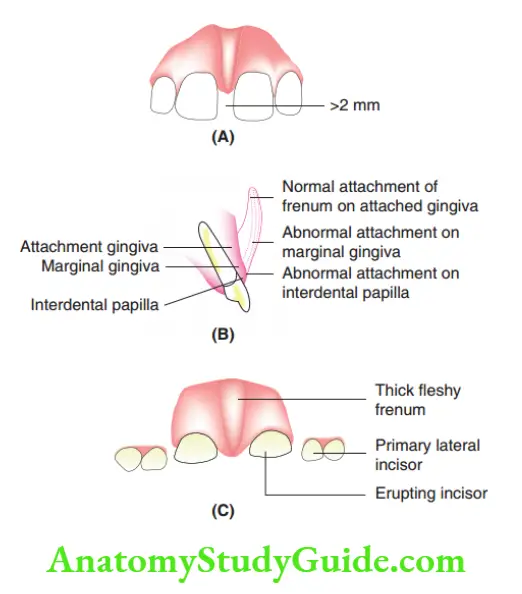
2. Frenum attached lower than the free gingiva. It may get attached to the attached gingiva, labial interdental papilla or the incisal papilla on the palatal side.
All these attachments that are lower than the normal attachment are indicated for excision.
3. Too thick and fleshy frenum may pose a risk of abnormal alignment of incisors.
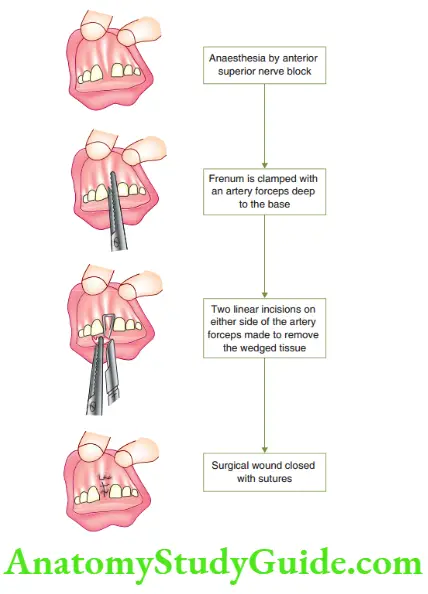
Frenectomy Procedure
Anaesthesia is obtained by a bilateral regional block through an anterior superior nerve block.
The infiltration method of local anaesthesia administration will obscure the boundaries of the frenum; hence, it is not preferred.
A straight haemostat/artery forceps is used to hold or clamp the frenum to the base.
A number 15 blade is used to make a linear incision, above and below the beaks of the straight haemostat.
The incision is made up to the base of the frenum so as to touch the bone.
Removal of the triangular tissue exposes a rhomboidal defect.
The exuberant incisive papilla, if present, is removed with parallel incisions extending from the lower angle of the rhomboidal surgical wound.
Simple interrupted sutures are placed along the entire defect to obtain primary closure. The procedure is depicted.
Post-operative instructions are similar to those after an extraction procedure.
In addition, the child is asked to refrain from moving the lip voraciously during eating/speaking for the first 3 days.
The child may be on a soft solid/semi-solid diet. Post-operative instructions should be given to the patient and parent.
They should include a prescription for post-operative antibiotics and anti-inflammatory drugs.
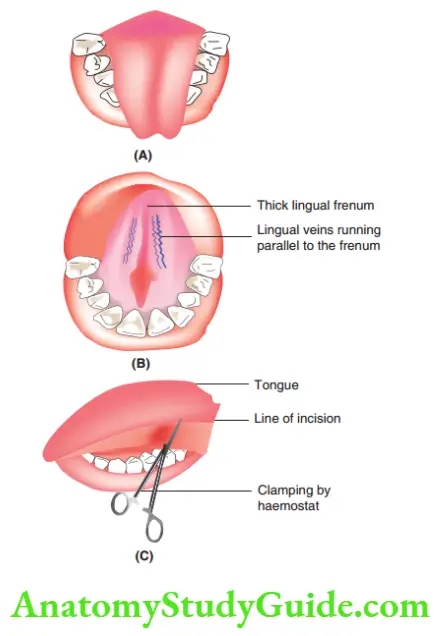
Lingual frenectomy is indicated in children with total, subtotal or partial tongue ties.
Such children have altered phonation of sibilants such as /s/. The clinical test to identify a short lingual frenum is to observe forking at the tip of the tongue on extending the tongue.
The procedure of lingual frenectomy is the same as that of labial frenectomy.
A bilateral lingual block is the preferred mode of anaesthesia. While grasping the lingual frenum with a haemostat, care has to be exercised as the lingual veins that are varicose in nature run almost parallel to the frenum.
Severing the veins leads to pronounced bleeding. After lingual frenectomy, speech therapy is mandatory for a predictable improvement in the pronunciation of sibilants.
Operculectomy
When the attached gingiva of the buccal and palatal sides coalesces, it forms a thick soft tissue barrier to tooth eruption.
The soft tissue barrier has to be relieved to allow eruption. This is called operculectomy.
The procedure is mostly indicated in pertinence to incisors in the early mixed dentition stage.
The procedure is indicated only after an IOPA radiograph assessment.
The following points have to be noticed in the radiograph before indicating operculectomy in the early mixed dentition:
- The presence of supernumerary tooth retarding the eruption of the incisor is ruled out
- The root of the permanent incisor should be 1/3 formed
- There has to be no lack of mesiodistal space dimension
Operculectomy Procedure
Adequate local anaesthesia is obtained by infiltration on the labial side and by a nasopalatine block.
A linear, crystal incision is made with a no. 15 blades to the depth of the bone.
Then, two parallel incisions are made – the first incision 1 mm labial to the crystal incision and the second incision 1 mm palatal to the crystal incision.
The resulting 2 mm of tissue is removed
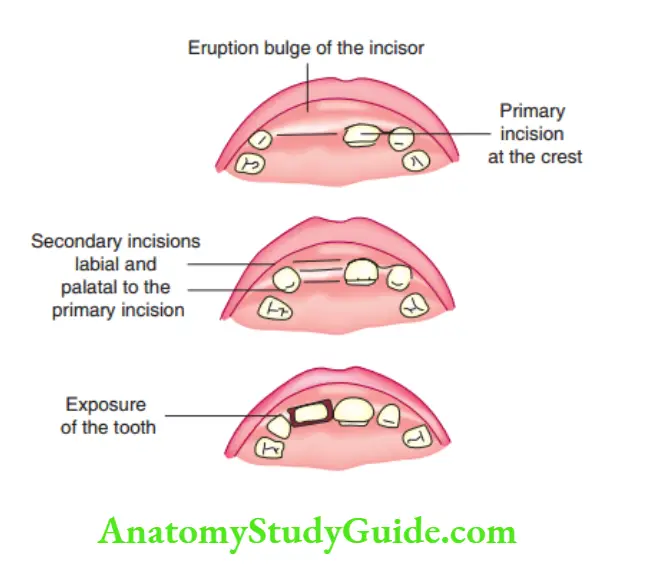
The mucoperiosteum is reflected in the bone to expose the tooth. The expulsion of a greenish fluid at the initial incision confirms an eruption cyst.
Haemostasis is attained with wet gauze. A suture is not indicated as obtaining relief and not primary closure is the objective of the procedure.
Extraction Of Unerupted Supernumerary Tooth
The anterior maxilla is the most common location for a supernumerary tooth in children.
A supernumerary tooth may be clinically evident or unerupted. It is associated with obvious malposition of permanent teeth or with non-eruption of permanent teeth.
Removal of a supernumerary tooth is almost always indicated to correct the malposition of permanent teeth or to aid the eruption of permanent teeth.
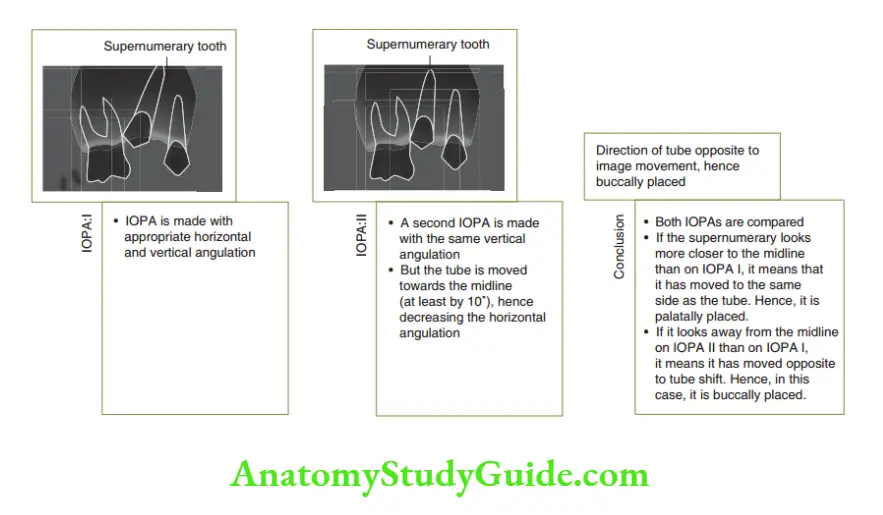
An IOPA radiograph assessment and occlusal radiograph assessment help to:
- Confirm the number of supernumerary teeth as when one supernumerary tooth is discovered, the clinician has to suspect for at least one more
- Localise the supernumerary tooth in relation to the adjacent teeth
The localisation of the supernumerary tooth in a buccopalatal plane (if it is present more towards the buccal plate or the palatal plate) is best done by a tube shif technique or a successive radiographic technique.
The SLOB rule or ‘Same Side– Lingual; Opposite side – Buccal’ is applied for this technique.
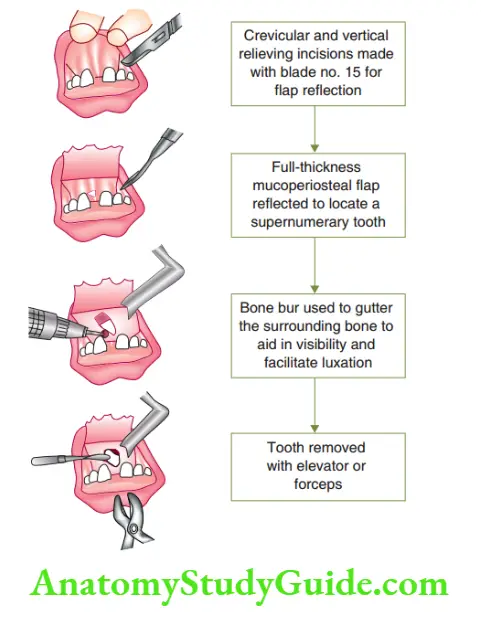
Extraction Of Unerupted Supernumerary Tooth Procedure
Complete regional anaesthesia of the site is obtained.
A no. 15 blade is used to make a crevicular incision around the erupted tooth above which the supernumerary tooth is located.
The incision should be long enough to provide appreciable visibility and access to the site of the location of the supernumerary tooth.
Vertical relieving incisions are also required to aid in access and visibility.
The mucoperiosteal tissues are reflected completely. Selective removal of bone is done with the help of bone-cutting burs.
The burs are used to gutter around the unerupted/supernumerary tooth to expose its height of contour.
Bone removal should be adequate enough to provide an appreciable convenience form for the elevators to luxate the tooth.
The supernumerary tooth is luxated with a small-sized periosteal elevator.
Care should be exercised so that the fulcrum does not fall on the other erupted/ unerupted tooth buds.
The tooth is loosened before grasping with forceps so as to be extracted.
Sutures are placed to obtain primary closure. The procedure of extraction of a supernumerary tooth is depicted.
Post-operative instructions are similar to those of a normal extraction.
Summary
1. Commonly performed minor oral surgical procedures:
Leave a Reply