Pernicious Oral Habits Introduction
Habit is described as an automatic response to a specific situation that is usually acquired as a result of learning and repetition.
Table of Contents
It is a mode of behaviour or performance that typifies an individual’s natural style.
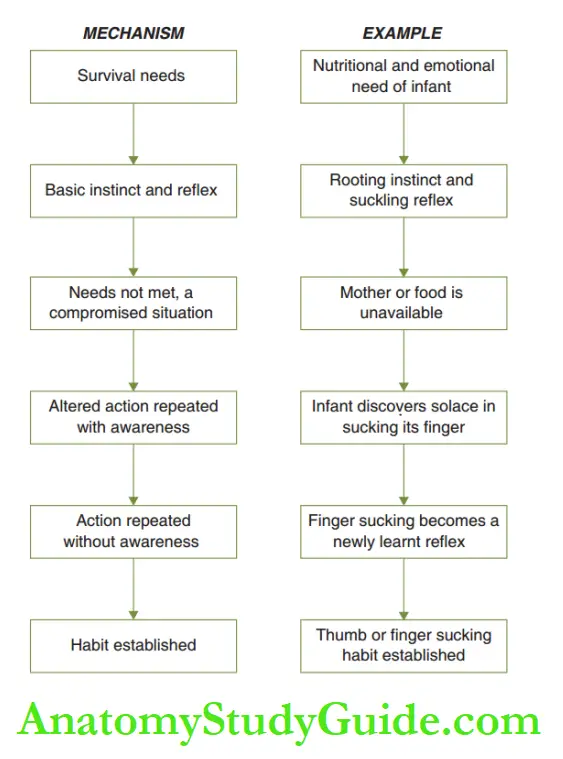
Each time the particular style of action is repeated, the individual becomes less conscious of the performance of the act and if often repeated, it may enter the realm of unconscious behaviour.
Certain compromised situations trigger an altered action in individuals. For instance, rooting and suckling are basic instincts of an infant.
Read And Learn More: Paediatric Dentistry Notes
The infant is used to an immediate supply of food. An altered situation like a delay in food supply results in a change in action.
When the food is unavailable, the infant discovers solace in sucking its own finger. The action is repeated at the next craving and later at the least instance of wanting.
Repetition of such altered situations is imbibed as a newly learnt reflex and gets established as a habit. The mechanism of habit establishment is depicted.
A habit that causes deleterious effects on the oral structures is termed a pernicious oral habit. Pernicious oral habits cause derangement of the maxilla and mandible.
They affect the position of teeth, oral functions and facial aesthetics.
Knowledge buccinator mechanism is essential to understanding how derangement of jaws and teeth occurs due to such oral habits.
Buccinator Mechanism
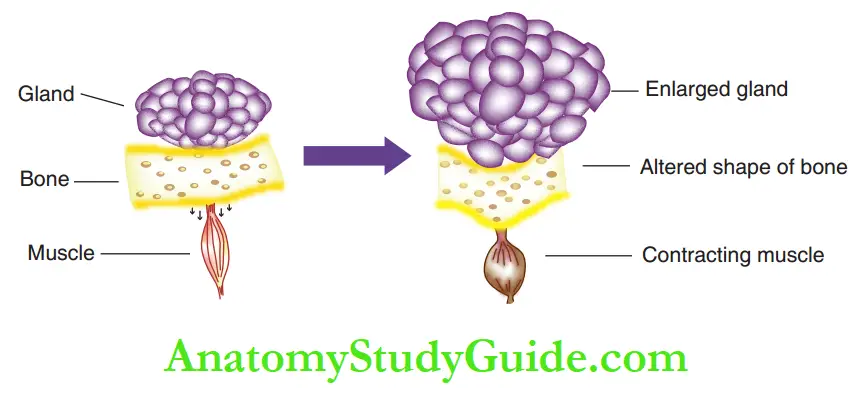
Bone, the hard tissue supports and protects the soft tissues such as muscles and glands. The functional matrix theory proposes that soft tissue matrices such as glands and muscles govern the position, shape and pattern of the hard tissue matrices supporting them.
For instance, an enlarging gland exerts constant pressure on the abutting bone, while a contracting muscle exerts a constant pull/tension. The bone responds by changing its structure and shape.
The final reshaped bone is in a neutral zone where there is no form of pressure or tension subjected by the soft tissue matrix.
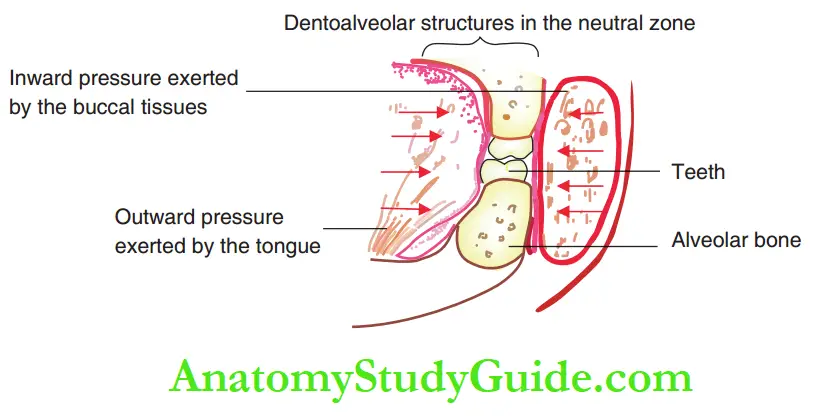
The presence and functional activity of the buccal soft tissues and the buccinator muscle exert constant inward pressure on the dentoalveolar complex. The inward pressure is exerted primarily by the buccinator muscle.
The powerful tongue musculature exerts outward pressure on the dentoalveolar. There exists a neutral zone where both these forces, exerted in opposing directions, are equal and opposite.
The teeth and alveolus are positioned in the neutral zone. This is called the buccinator mechanism.
The pernicious oral habits alter the equation between the opposing forces, thus disrupting the buccinator mechanism. The position of the neutral zone is altered leading to the derangement of dentoalveolar structures.
Three major factors, referred to as trident factors, decide the extent of damage caused to oral structures by a pernicious oral habit:
- Frequency of the habit: Number of times the habit is performed in a day
- The intensity of the habit: How strongly or vigorously is the habit performed
- Duration of the habit: For how many years is the habit being performed
Classification Of Pernicious Oral Habits:
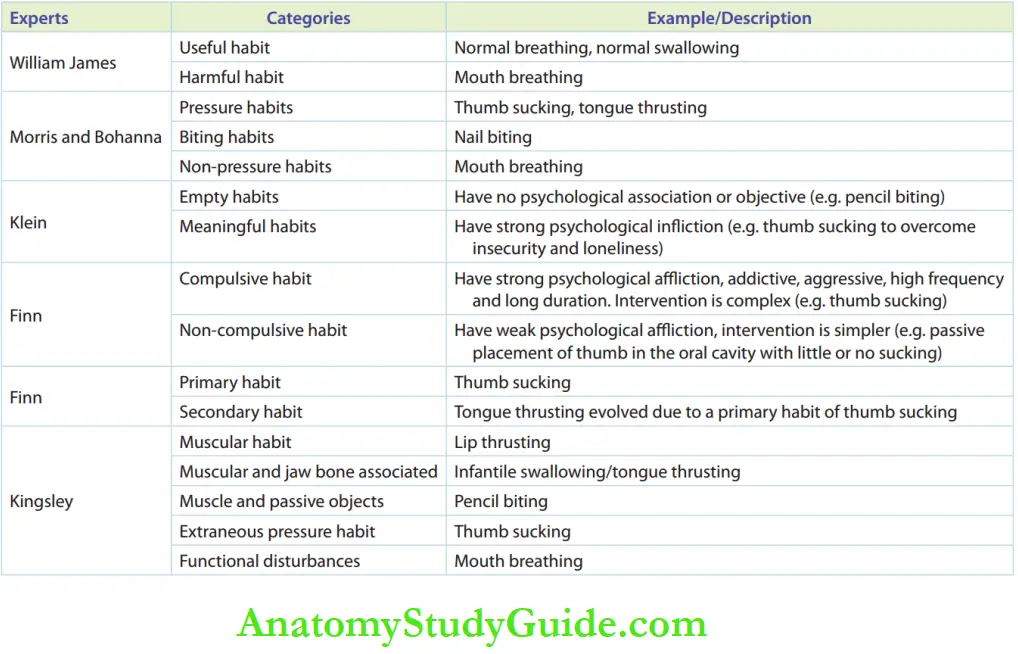
Pernicious oral habits have been classified in different ways according to effects, aetiology, etc. A glimpse of various classifications by different experts is given in the table.
This chapter discusses the effects of various oral pernicious habits on dentoalveolar structures and their treatment modalities.
Management Of Pernicious Oral Habits:
Pernicious oral habit causes structural changes to the dentoalveolar complex. These changes can be observed as early as 3–4 years of age.
Early interruption breaks the habit more easily and achieves better results. Prolonged pernicious oral habit causes irreversible damage to the dentofacial system.
Habits die hard, especially when attempts to eliminate the habit have not begun in the early years. The common formula for eliminating pernicious oral habits is as follows:
- Elimination of aetiology
- Education and motivation to parents and child
- Psychological support for the child
- Habit breaking appliances
- My functional exercises
In general, the earliest possible age to introduce a habit-breaking appliance is 5 years.
The optimal age for advocating the habit-breaking appliance is between 5 and 10 years, depending on the child’s confidence and cooperation.
A delayed attempt, apart from being difficult for the patient, worsens the situation.
The skeletal and dental malocclusions are firmly established with delay in treatment time. The correction then requires long and complicated mechanotherapy.
Habit correction is never complete without the oral muscles returning to their appropriate tone.
Knowledge about basic myology is essential to understand how my functional exercise helps in toning muscles. This is discussed in Box.
Children with pernicious oral habits often exhibit deranged tone of lip and tongue muscles.
Appropriate myofunctional toning exercises are suggested to correct the tone of the lip and tongue muscles.
Lip exercises are indicated in the case of mouth breathers and those with hypotonic lips. Tongue exercises are indicated in children displaying an altered tongue position.
Apart from the lip and tongue exercises, speech therapy is important to obtain correct pronunciation by coordination of the tongue, lips, vocal cords and soft palate.
Speech therapy helps in regulating the posture and tone of the muscles of the tongue, lips and soft palate.
Mouth Breathing Habit
Opening the mouth to breathe is an immediate, lifesaving measure when the nasal airway is blocked.
Air breathed in through the oral route reaches the common nasopharynx and then the larynx. This is a survival measure.
However, an unattended nasal airway block leads to repeated mouth breathing. The act gets fixed as a habit and sometimes remains even after the removal of the causative nasal block.
Aetiology:
Mouth breathing can be categorised according to the aetiology of the habit as obstructive, anatomical or habitual.
- Obstructive mouth breathing: Caused by nasal airway obstruction due to enlarged turbinates, tonsils, adenoids or severe deviation nasal septum
- Anatomical mouth breathing: The anatomy of orofacial structures may allow easy passage of air through the mouth (e.g. incompetent, short upper lip)
- Habitual mouth breathing: Habit with no associated obstructive/anatomical feature
Pathogenesis:
Blockednasalairwayinitiatesmouth breathing. A brief period of mouth breathing until the nasal block is cleared does not harm the dentoalveolar structures.
Prolonged mouth breathing precipitates skeletal changes in the maxilla as depicted.
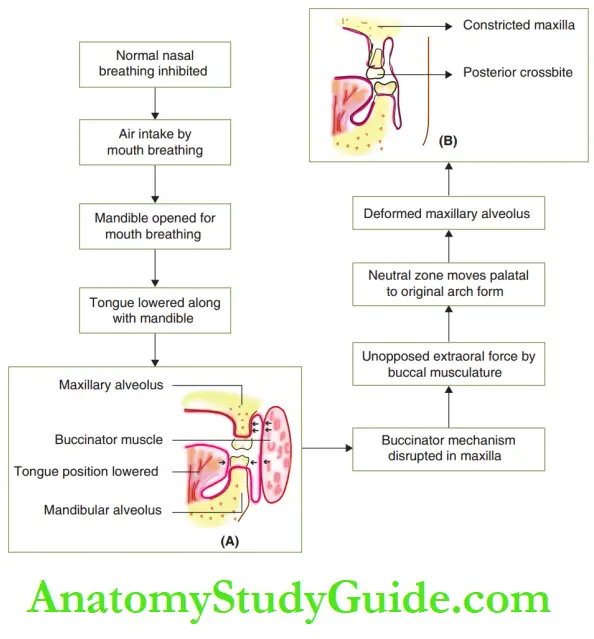
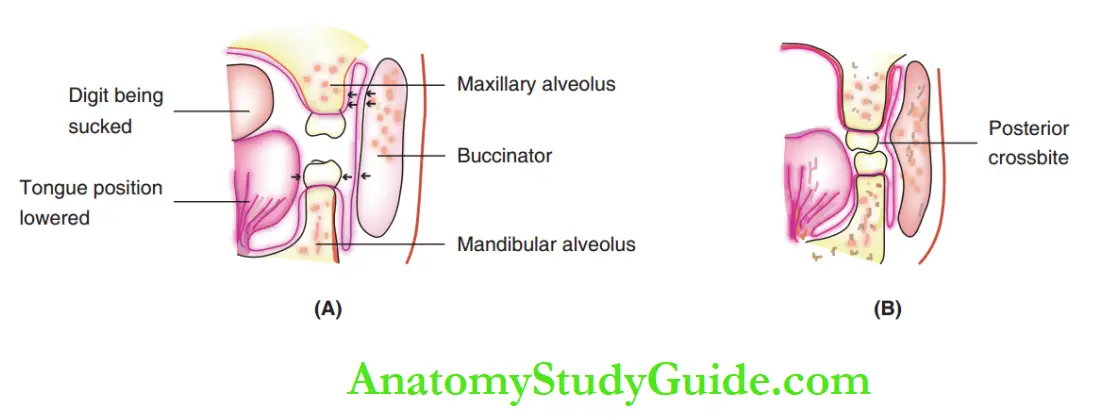
The mandible opens during mouth breathing and the tongue is lowered along with the mandible.
The buccinator mechanism collapses as the tongue is not in its position to counter the forces exerted by the buccal soft tissues.
The small arrow marks. show that the buccal forces exerted against the maxillary are unopposed, while those exerted against the mandible are countered well.
The buccinator muscle pushes the maxilla inside, leading to a constricted and palatally placed maxillary alveolus.
Clinical Features:
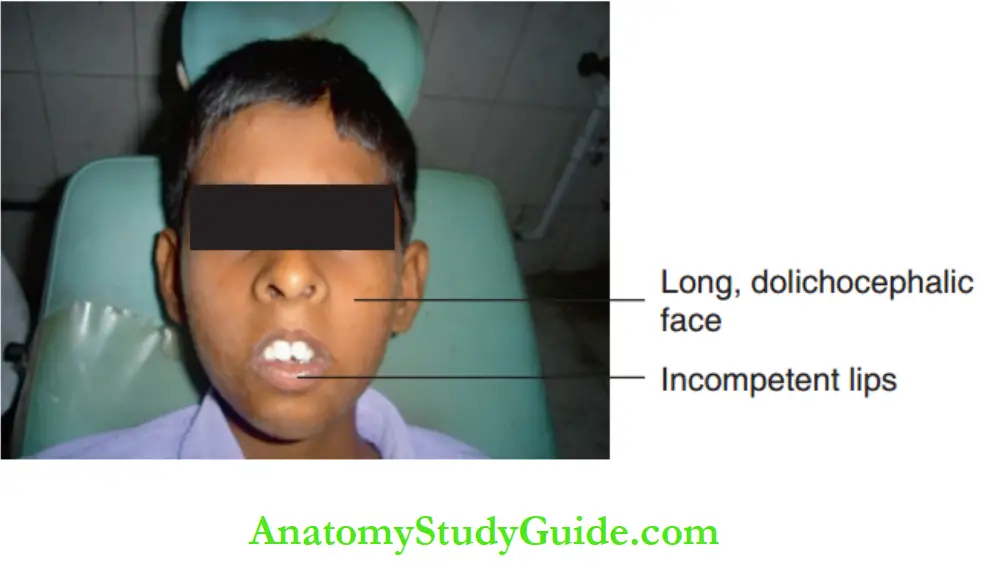
The extraoral features of a mouth-breathing individual include the following:
Long dolichocephalic face, increased anterior lower facial height as the posterior teeth erupt out
The downward and backward rotation of the mandible leads to a hyper-divergent mandible and high clinical FMA
Incompetent lips due to increased lower facial height These structural changes give a lethargic appearance to the face.
Conventionally, the face of a chronic mouth breather with these features is described as adenoid facies.
The disrupted buccinator mechanism and the constriction of the maxillary arch lead to the derangement of the maxillary arch.
Due to the prolonged opening of the mouth, there is a natural tendency of teeth to erupt out and cause disocclusion of posterior teeth and flying anterior teeth.
Diagnosis:
1. Case history: History of chronic respiratory tract infection. Parent’s observation regarding ‘mouth kept open all time’.
2. Clinical observation: The pattern of breathing and movement of respiratory muscles are noticed when the child is unaware of being observed.
3. Water-holding test: Among many suggested tests, the water-holding test is the most confirmatory test where the child is asked to hold water in the mouth without spitting. A child with a mouth-breathing habit will not be able to hold the water for a few seconds.
4. Mirror test: A double-sided mirror is kept in front of the region between the mouth and nose of the child. Mouth breathing causes fogging of the lower surface and nasal breathing causes fogging of the upper surface of the double-sided mirror.
5. Butterfl test: Butterfl-shaped cotton wisps kept below the nose will not flutter in the case of a mouth breather.
6. Radiographs: Lateral cephalogram can exhibit lower tongue position, prominent respiratory tract obstruction, mandibular rotations, the inadequacy of nasopharyngeal space and the presence of adenoids.
7. Rhinomanometry: This is the confirmatory investigatory parameter that assesses the amount of air flowing through the nose.
Management:
The steps involved in the management of mouth-breathing habits are as follows:
1. Correction of aetiology: Nasal airway blockage is usually associated with
- Deviated nasal septum
- Inflamed nasal turbinates
- Nasal polyp
- Adenoiditis
- Tonsillitis
An assessment by an otolaryngologist is mandatory, who may advise medical or surgical correction for the elimination of nasal obstruction.
Habit intervention can be attempted only after the elimination of the aetiology.
2. Education and counselling — child and parent: Psychological support assurance and cooperation from all family members will assist in habit elimination.
Verbal abuse or strong dictation to breathe through the nose will bear no fruit. Rather, it will instil a negative attitude in the child.
3. Habit-breaking appliances: Pathological mouth breathers become habitual mouth breathers due to delayed supportive remedial measures.
They continue to breathe through their mouth even after clearing the nasal block. In such cases, appliances become necessary for redirecting their breathing pattern.
The oral screen is a functional appliance indicated to eliminate mouth-breathing habits.
The oral screen helps regulate and redirect the airflow from the more pronounced oral way to the nasal way.
It is a ‘U-shaped flat acrylic sheet placed between the dentoalveolar and the buccal musculature.
Buccal flanges of the appliance act as a shield to wall off the constricting effect of the buccal soft tissue matrix on the maxillary alveolus.
This allows the neutral zone to shift to its original position, thus achieving an ideal arch form.
Holes are provided in the anterior part of the appliance initially to allow easy passage of air to a patient who is habituated to mouth breathing.
The change has to be introduced gradually to a child who is unlearning a habit.
So the size of holes is gradually reduced by adding self-cure acrylic while the breathing gets gradually re-routed towards the nasal passage.
Finally, the holes are completely occluded to enable only nasal breathing.
The appliance is held in contact with the incisal third of maxillary anterior teeth to transmit functional pressure.
This corrects the proclamation of anterior teeth and anterior open bite. The appliance is constructed with a forwardly postured mandible.
Hence, it acts as a functional appliance for uninterrupted expression of mandibular growth and corrects diverging mandibular positions.
The appliance therapy spans 6–9 months. The usage can be discontinued when habitual nasal breathing is established after a few months.
4. Muscle exercises: Lip exercises are advocated to alter the position and improve the tone of flaccid and hypotonic lips. This establishes postural lip competence. The following are the myofunctional exercises indicated to improve the tone of lip muscles.
Paper-holding exercise: The child is asked to hold a paper in between their lips with a firm grip. The action is performed for 5–10 minutes and repeated three to four times a day.
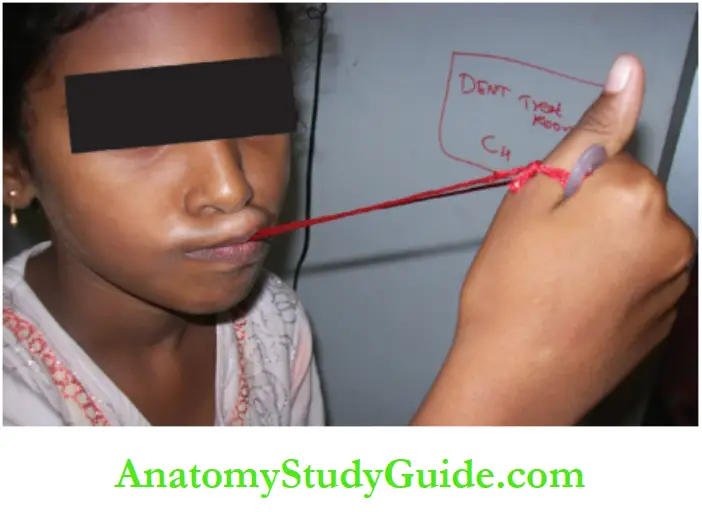
Button-aided exercise: A film thread with a button attached to each of its two ends is used for this exercise.
One button is held in the mouth with the help of the upper and lower lips. The other button is held with the hand.
A pull is exerted to bring out the button from the mouth, while circumoral muscles contract and try to hold it back.
Stretch and curl exercise: This exercise is best indicated for short, flaccid lips with proclined upper anterior.
The child is asked to stretch the upper lip and curl it below and behind the upper incisors while contracting it simultaneously.
Further, the child is asked to hold the upper lip in this position and extend the lower lip to cover the upper lip while contracting the lower lip simultaneously.
The exercise is performed for 20–30 seconds and repeated 20–40 times twice or thrice a day under parental supervision.

Activities such as whistling, blowing a balloon and playing wind instruments help in toning the flaccid/hypotonic upper or lower lips and a buccal group of muscles.
Deep breathing exercises activate all the muscles of respiration and air circulation along air passages. The lip exercises and the breathing exercises help in the total elimination of the habit.
5. Periodic review: Initial review in 3 months and long-term review in 6 months can help in assessing the extent of habit elimination, compliance with the appliance and any habitual recurrence.
Thumb Sucking/Finger Sucking/ Digit Sucking
Thumb and/or digit sucking is the habit of placing thumbs and/or digits to varying depths into the oral cavity.
Sucking is a reflux that is considered normal till the age of 3 after which it is expected to mature out and disappear.
Preference for the digit used for sucking varies. While thumb sucking is more common, some children suck the second and/or third finger too.
Aetiology:
Various theories have been propounded to explain the establishment of this habit. a suckling reflex is triggered when the food supply to the infant is delayed or unavailable.
The infant discovers temporary pleasure and security in sucking the finger or thumb. This action becomes a habit upon repetition.
Other widely advocated causes of finger/thumb sucking habit are listed in Box.
Sequelae:
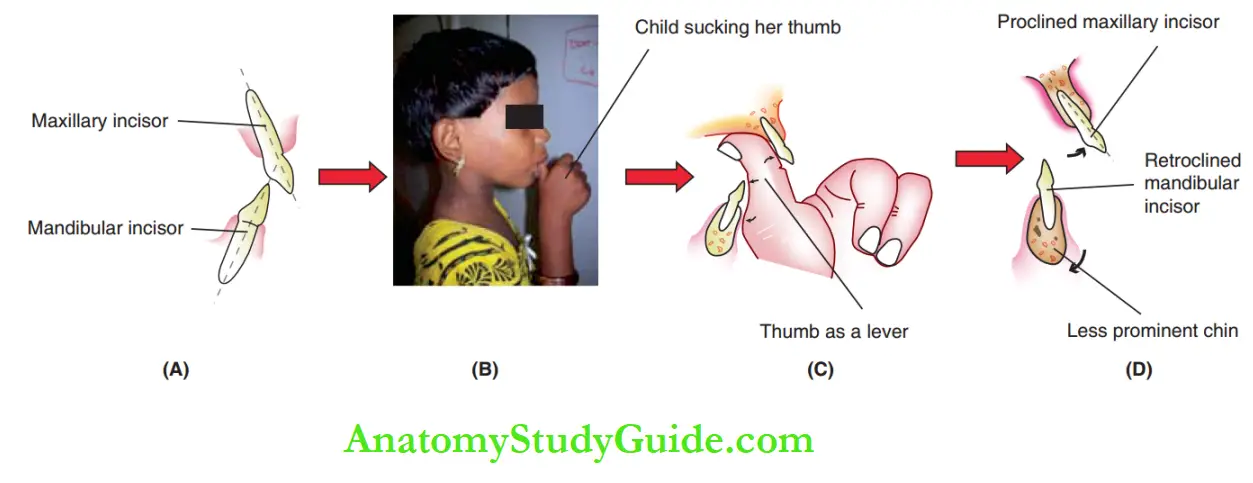
Plastic deformation of the alveolus is established if the digit-sucking habit prolongs beyond 3 years of age. Deformation of the dentoalveolar and face is due to two important factors.
1. Lever effects of hand and digit position: During thumb sucking, constant pressure is exerted by the hand over the chin.
Moreover, as the mouth is kept open, the mandible gets positioned downwards and backwards. Over a period of time, the mandibular growth itself gets redirected clockwise, reducing the prominence of the chin.
Intraorally, the pulp of the thumb exerts an outward force on the upper anterior, while the root of the thumb exerts an inward force over the lower incisors.
This lever-like action proline upper incisors and retro lines lower incisors.
When fingers other than the thumb are sucked, the changes occur according to their position and the force exerted.
2. Collapse of buccinator mechanism: The tongue is lowered when a digit is sucked. The buccinator mechanism is disrupted and the posterior teeth dis occlude.
With unequal pressure in the maxillary region, the neutral zone gets shifted to a more palatal position. This leads to a constricted posterior maxillary segment and posterior crossbite.
Clinical Features:
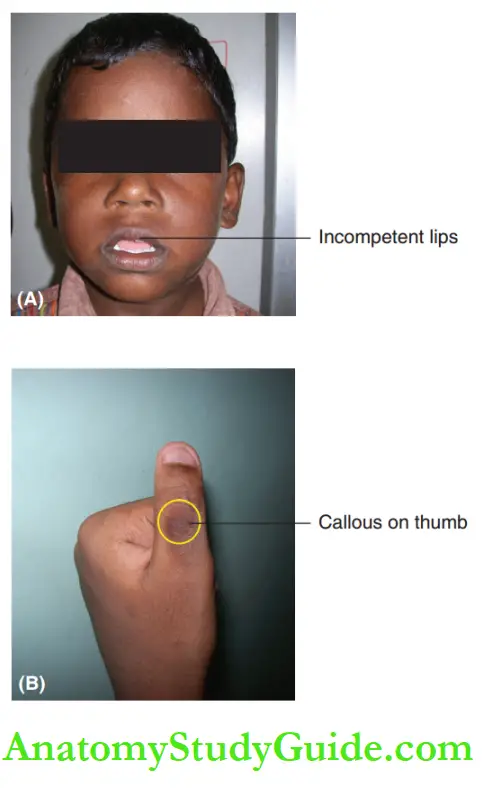
The upper lip of a thumb or digit-sucking child is incompetent, hypoactive and functionless. Open and backwardly rotated mandible causes loss of chin prominence and hyper divergence of the mandible.
Callous is observed on the digit or the thumb being sucked due to constant friction with the incisal edges of the anterior teeth. The nail of the sucked digit is overly clean giving a clean dish pan appearance.
Some children exhibit associated habits such as twisting or pulling their hair while sucking the digit, leading to patchy hair loss.
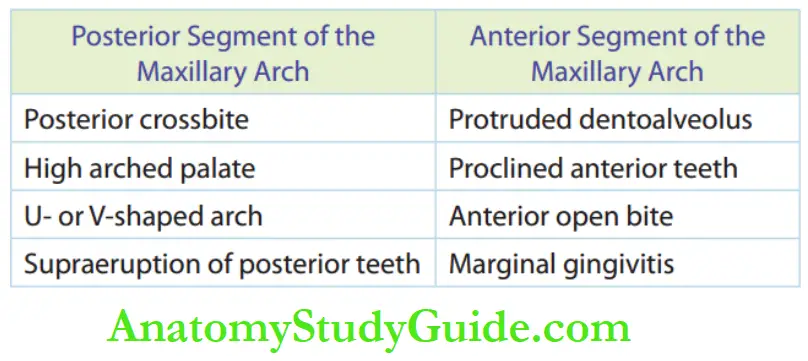
The intraoral features include derangement of anterior and posterior segments of the jaw:
Features of the posterior segment:
- Constricted posterior segment
- Posterior crossbite
- High arched palate
- Extrusion of posterior teeth due to supereruption
Features of the anterior segment:
- Retroclination and crowding of lower anterior teeth
- Proclamation of upper anterior teeth
- Anterior open bite
- Tongue thrusting may develop into the anterior open bite as a secondary habit.
Management:
Digit-sucking habit disappears spontaneously around 2 years of age with good parental care.
No active intervention and only observation are required if the child has grown out of the habit at least by the third year and has a normal occlusion.
When the habit continues beyond 3 years of age, the optimal time for intercepting is between 3½ and 4½ years.
The desire of the child to discontinue the habit and parental awareness and motivation are the primary goals of management.
Appliances or approaches should not work against children but work along with them.
Management of thumb-sucking comprises three approaches:
- Counselling and motivation
- Restrainer therapy
- Reminder therapy
1. Counselling and motivation: A thorough case history can be obtained from parents without the child in the discussion room.
This may reveal whether the habit is a part of abnormal behaviour requiring a psychiatrist’s help. The emotional and psychological needs of the child should also be understood.
A frank and open discussion will help the child to cooperate for treatment and get out of the habit.
Parents’ role:
- Parents have to create a conducive and supportive atmosphere at home.
- They should be encouraging, helping and appreciating the cooperation extended by the child.
- The child should not be teased or threatened with abusive words by anyone in the family and neighbourhood.
- The parents are advised not to mention that the attempt is to break the habit. Rather, they can explain that it is only to improve the teeth position of the child.
The motivation of the child:
- The child should be educated about the consequences of the habit by showing models and pictures of children with unpleasant faces due to the habit.
- Dunlop’s beta hypothesis is a self-observation programme during the performance of the habit. According to this hypothesis, a child is forced to observe his own reflection in the mirror while sucking the thumb or digit.
- Such repeated episodes gradually make the habit an unpleasant action and the child slowly refrains from the sucking habit.
- The child should be made to understand that the aim of treatment using appliances is only to improve the appearance and biting efficiency and not as a means of punishment.
2. Restrainer therapy: This therapy aims at making the thumb or digit-sucking habit difficult to perform.
Passive inhibitors or restrictors are indicated so that the habit is no longer pleasurable or satisfying to the child.
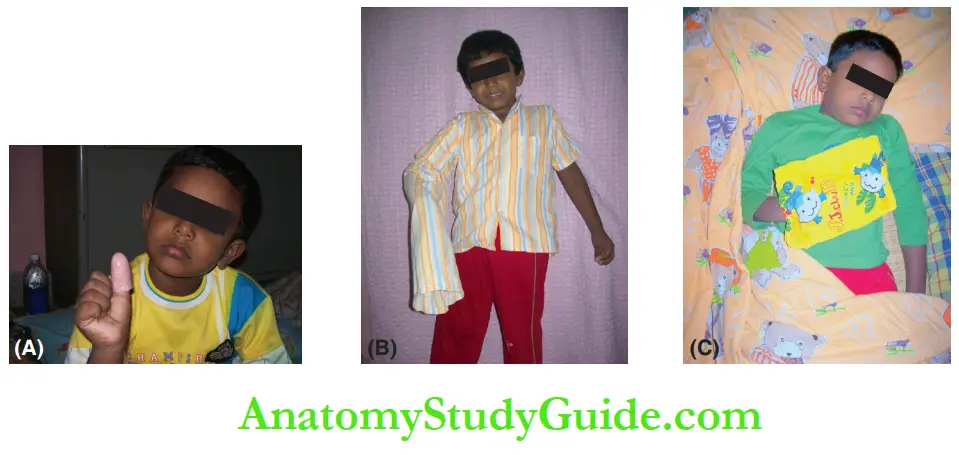
Various modes of restrainer therapy include wearing a thumb cap, modification of nightwear and an ace-bandage approach.
An ace-bandage approach is where the elbow is tightly bandaged and flexing of the arm becomes a difficult task.
The nightwear is modified for children who intensely suck their fingers during sleep. The sleeve of the particular thumb-sucking arm of the nightwear is made longer.
It hangs out and covers beyond the fingers. Children are delighted about having a novel ‘home-for-hand’, a small pouch stitched on a shirt, and willingly prefer to rest their hand inside it.
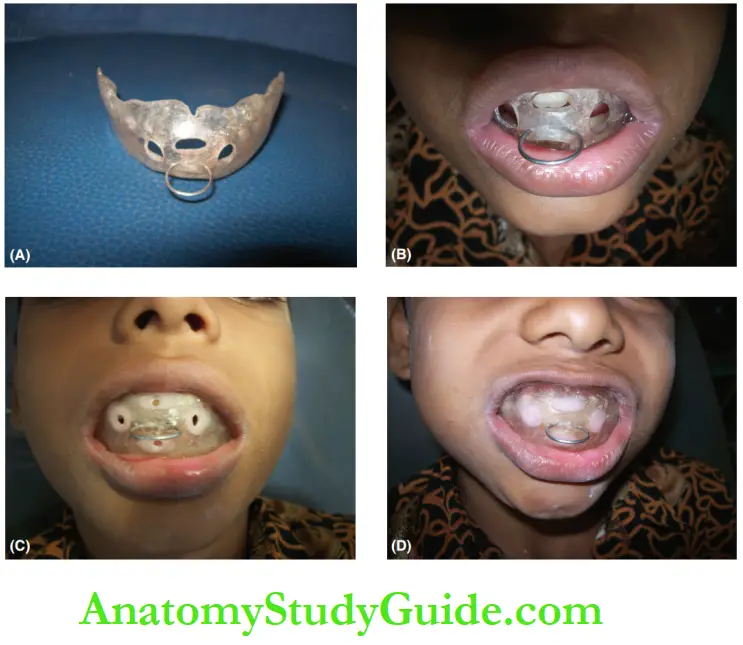
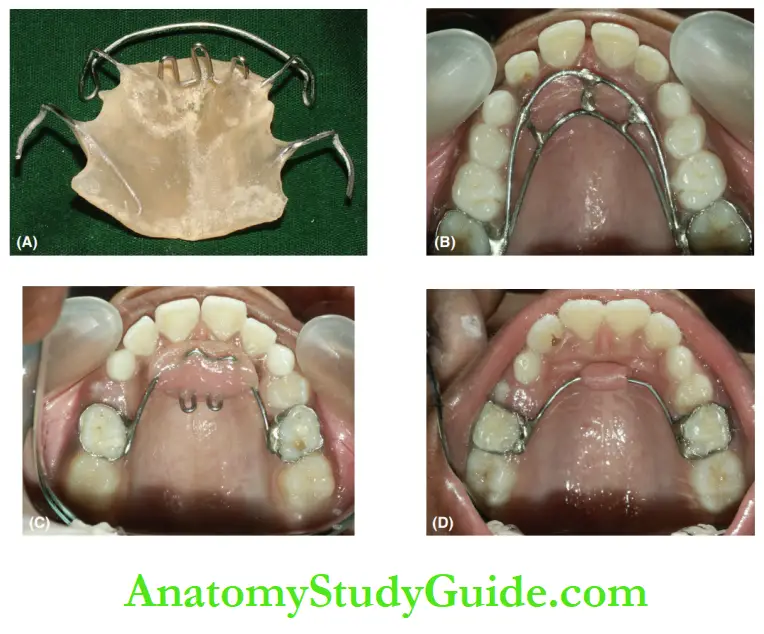
3. Reminder therapy: This therapy involves the insertion of various removable or fixed intraoral appliances. It reminds the child of his desire to discontinue the habit.
Removable appliances may be indicated. But they require the child’s cooperation and commitment to wear the appliance. Fixed appliances are hence a better choice.
Appliances that possess rakes, spikes and cribs break the comfort of sucking and make it difficult to place the digit into the mouth.
Thereby, the gratifying feeling derived from the sucking habit is lost. The appliance should have the following features:
- It is essential that the rakes/cribs/spikes extend 1–2 mm below the incisal edges of lower incisors.
- They should not interfere with the occlusion and not be in contact with the lingual surface of the lower anterior.
- They should not be sharp and create no harm to the child.
4. An oral screen can also be used as it fulfils the requisites for breaking the thumb-sucking habit.
5. A bluegrass appliance is another useful habit-breaking appliance. It has a six-sided roller bead made of Tefln that is incorporated in the anterior part of the palatal archwire.
The child is diverted to roll the bead with a tongue instead of sucking the digit.
Duration Of Appliance Wear:
The length of habit intervention therapy depends on the age of introduction of the appliance, the severity of the deformity and the cooperation of the patient. Usually, it is indicated for 4–9 months.
The advantage of habit elimination is the spontaneous concomitant correction of malocclusion. Once the habit is discontinued, the buccinator mechanism is restored and occlusion tends to become normal.
Tongue Thrusting Habit
A thrust tongue is anteriorly postured between maxillary and mandibular anterior teeth and it is forced more forward during wallowing.
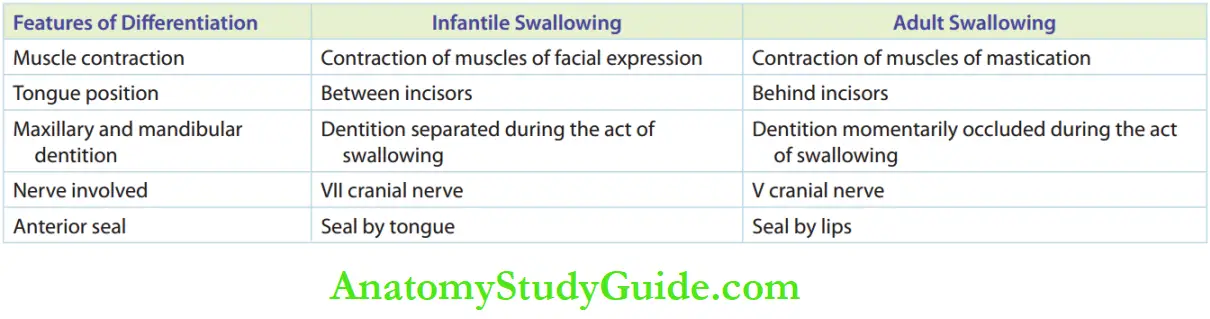
Tongue thrusting is normal in neonates as they have an infantile swallowing pattern.
The tongue is in between the gum pads and is associated with an infantile open bite. With the eruption of teeth, the infantile swallowing pattern is expected to mature into an adult swallowing pattern.
The tongue is thrust against the rugae of the palate (where the vault of the palate descends) while swallowing.
Failure of transformation from an infantile swallowing pattern to an adult (mature) swallowing pattern is termed retained infantile swallow and demonstrates tongue thrusting.

Sequelae:
The tongue position is lowered and the buccinator mechanism is disturbed in mouth breathing and thumb-sucking habits.
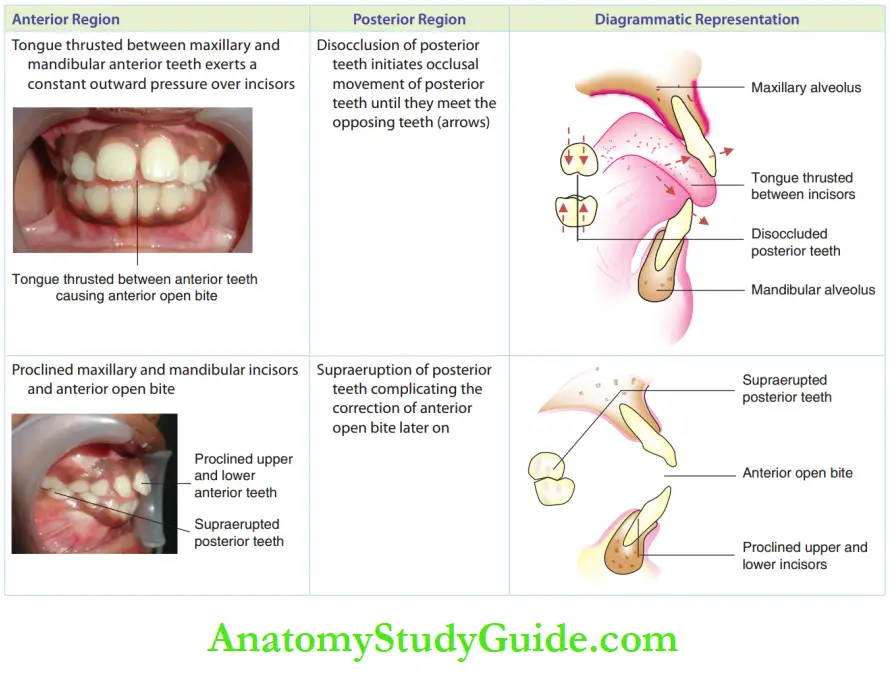
On the contrary, the tongue occupies the whole intraoral space between the upper and lower teeth in the anterior region and exerts outward pressure on the anterior region.
Tongue thrust between anterior teeth exerts an outward pushing force on both maxillary and mandibular teeth, thus dis-occluding posterior teeth.
The differences between the features of the infantile swallow and the adult mature swallow are enumerated in showing an anterior open bite.
Closure of anterior open bite and habit elimination after intervention for 9 months. the posture of the tongue and the posture of the tongue during tongue thrusting.
Aetiology:
The factors that cause the development of tongue thrusting are listed as follows:
Secondary habit:
Tongue thrusting may follow digit sucking habit or a mouth-breathing habit. The space is available due to the anterior open bite in these conditions is occupied by the spreading tongue, thus initiating a new habit.
Delayed weaning out of bottle feed/pacifier.
Forwardly positioned tongue with enlarged tonsils/ adenoids.
Certain general conditions such as hormonal imbalances like cretinism, neuromuscular disorders or mental retardation.
Macroglossia where the tongue is positioned anteriorly.
Clinical Features:
The prolonged deranged posture of the tongue and pressure from the tongue result in various effects as
Tongue thrusting can be simple or complex. Simple tongue thrusting shows proclamation of upper anterior teeth and anterior open bite.
The posterior occlusion remains unaffected.
Treatment is simple and successful. Complex tongue thrusting shows bizarre open bite with no proper intercuspation. The neuromuscular control is poor and treatment is a challenge.

Tongue thrusting can be in the anterior region or in the lateral region, resulting in an anterior open bite or lateral open bite, respectively.
The additional untoward effects of tongue thrusting habit include alteration in speech and affected facial aesthetics.
Linguadental sounds such as /th/, /dh/, /ch/ and /sh/ and sibilants such as /s/ and /z/ are altered.
Pronunciation is severely affected (lisping) due to anterior open bite and deranged tongue tip posture, which causes air escape from the anterior region when not required.
Facial aesthetics is affected due to the increase in lower facial height, incompetent lips and backwardly placed chin. Deranged aesthetics also have a negative psychological impact on the child.
Management:
The management of tongue thrusting habit comprises four steps.
1. Identification of aetiology: As mentioned earlier, enlarged adenoids/tonsils, general health disorders such as hormonal disorders and neural disorders, and mental retardation may cause tongue thrusting habit.
Such causes have to be identified before attempting the elimination of tongue thrusting habit.
Referral to a general physician and concerned specialist is mandatory in such situations before the fabrication of appliances.
2. Education and motivation of parent and child: It is important that both the parents and child understand that tongue thrusting can affect dentition and aesthetics.
It is equally important to explain in simple terms the consequences of leaving the habit untreated and the action appliances in eliminating the habit.
Photos of successfully treated cases and a few untreated adult cases could be shown to the child to make them understand and motivate them to undergo therapy.
3. Tongue thrusting habit-breaking appliances: The objectives of appliance therapy include the following:
- Eliminating the forward thrusting during swallowing
- Restoring the lost lip pressure on anterior teeth
- Re-educating functional posture of the tongue
The appliances indicated are as follows:
Removable or fixed appliances incorporated with spikes, cribs, rakes or roller balls are used to restrict the forward movement of the tongue.
They hold the tongue behind and away from the anterior teeth and allow lip pressure to act on these teeth and enable their correction.
Roller balls help in re-educating the tongue to obtain its functional posture, that is, the dorsum of the tongue approximating with the palate and tip in contact with palatal rugae.
An oral screen with spikes incorporated lingually is useful for the interception of tongue thrusting associated with mouth breathing for rehabilitating the buccinator mechanism.
The oral screen prevents mouth breathing and the lingual spikes prevent anterior positioning tongue.
Fixed tongue spike appliance has a spiked wire soldered to molar bands and cemented to molars. Sometimes spurs are placed instead of spikes.
The spikes and spurs make the tongue uncomfortable in the forward and thrust positions. This discourages the child from pursuing tongue-thrusting habits.
Bluegrass appliance or roller ball appliance is a fixed appliance incorporated with rolling non-toxic beads in the anterior region of the wire that is soldered to molar bands. The tongue is distracted by the rolling beads and remains away from the anterior position, thus avoiding the habit.
4. Muscle exercises: The following myofunctional exercises of the tongue help in restoring the ideal tongue posture and adult swallowing pattern.
1. 4‘s’ exercise: This exercise involves four steps, namely spot, squeeze, salivate and swallow. The child is first taught about the ideal spot for posturing the tongue tip at rest.
The child is then taught to place the tip of the tongue in that spot and squeeze the spot. With the tongue held in the same spot and position, the child is instructed to salivate and swallow the saliva.
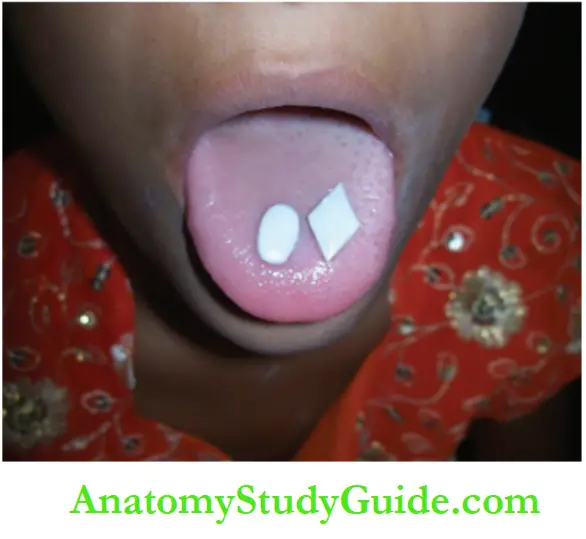
2. Proprioception training: A few small objects shaped like a diamond, oval or small orthodontic elastics are held against the palate with the tongue.
Holding the object in between the palate and tongue, the child is asked to feel and recognise the shape of the object. As the habit gets corrected, the sensation improves.
3. Re-education of tongue posture: A flt sugarless fruit drop is placed at the tip of the tongue and the child is asked to hold the tip of the tongue against the palate until the drop melts away.
This enthusiastically followed exercise re-educates the tongue to a correct posture.
4. Training tongue posture at swallowing: While the tip of the tongue is positioned at the vault of the palate, the child is asked to swallow saliva, bringing the teeth into occlusion. This exercise is repeated 20–30 times twice or thrice a day.
In almost all individuals with tongue thrusting habit, lips become incompetent to cover upper anterior teeth due to existing anterior open bite and proclaimed upper incisors.
As the action of lips is similar to that of the buccal group of soft tissues in the buccinator mechanism, the tonicity of a competent lip by itself restricts the firing of upper incisors.
Restoration of tonicity is an important aspect of habit correction.
Lip Thrusting/Lip Biting/Lip Sucking Habit
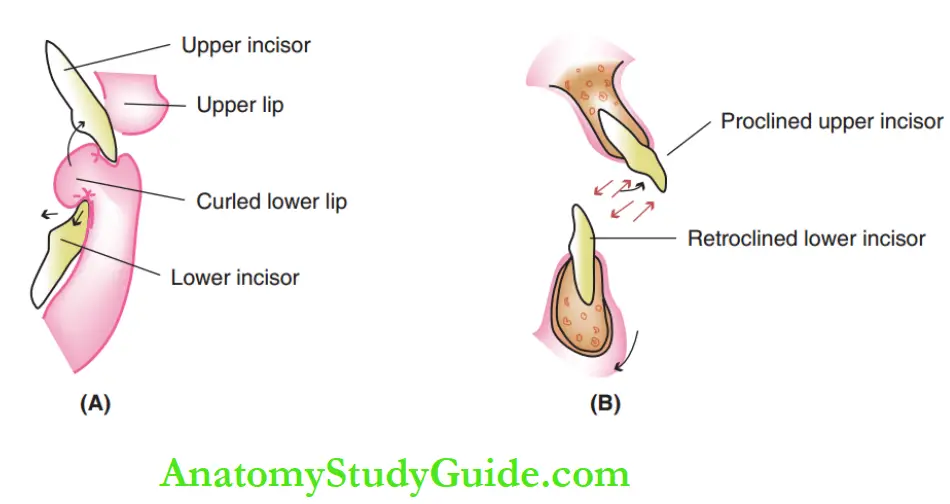
Thusting, biting or sucking of the lower lip has extensive potential to derange the dentoalveolar anatomy and facial pattern. There are two demonstrable patterns of the habit.
The lower lip may curl over lower incisors with upper incisors biting upon them. The impact of biting the lip is experienced by the anterior teeth.
2. The lower lip may be postured cushioning the upper incisors.
The constant presence of the lip below the incisors has the potential to change the positions of the anterior teeth, in spite of no muscle hyperactivity.
Aetiology:
Lip-biting or thrusting habits can be triggered by psychological insecurity or any stressful condition like parental neglect and unacceptability among peer groups.
Severely proclined maxillary incisors as in the case of class II division I malocclusion allow the lower lip to be placed comfortably between the maxillary and mandibular incisors.
The effects of lip biting upon dentoalveolar structures are due to the following factors:
- The kinetic energy derived by biting/sucking the lip
- The potential energy by the passive position of the lip
- Hyperactivity of mentalis muscle during active lip sucking
Clinical Features:
The consequences of lip biting depend on the posture of the lip and the direction and magnitude of the force exerted by lip biting or sucking on the dentoalveolar structures.
Pressure is exerted upon the incisors when the lower lip is curled over the lower incisor and bitten upon by the upper incisor.
The lip exerts an outward thrust on the lingual surface of the upper incisors and an inward and apical thrust on the labial and incisal surfaces of the lower incisors.
It results in an anterior open bite with proclined upper incisors and reclined and intruded lower incisors.
The small arrows indicate the direction of the force exerted upon teeth and the corresponding change in the position of teeth and chin.
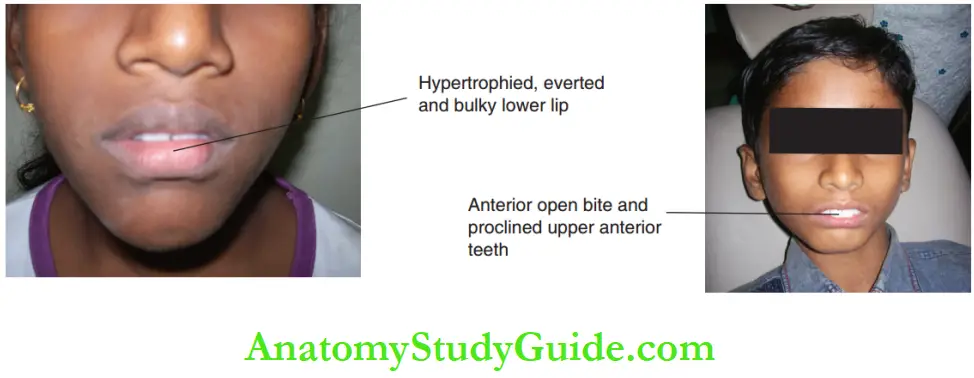
The extraoral features of a child with lip-biting or sucking or thrusting habits are as follows:
- Constant irritation and inflammation of the bitten area of the lip
- Constant wetting oflip
- The lower lip is bulky and ahead of the upper lip
- Proneness to infections like herpes
- Lip morphology changed, looks chapped and wrinkled
- Lower lip everted and hypertrophic
- Deep mentolabial sulcus
- Hyperactive mentalis causing puckering of skin over the chin
- The constant pressure of the lip restricts the expression of the growth of the mandible and the chin is positioned backwards.
Management:
Insults to the stomatognathic system and the abnormal lip size resolve after early cessation of the habit. The management includes the following steps:
1. Elimination of aetiology: When the lip thrust habit is secondary to malocclusion, the correction of malocclusion is the primary goal of management.
Habit interception without the elimination of demonstrable aetiology will not be successful.
2. Psychological support: As the aetiology includes psychological trauma, psychological support is essential for the total correction of lip-biting habits.
Cooperation of family members by way of reassurance is very essential.
3. Habit-breaking appliance: The following appliances are indicated to eliminate lip-biting or thrusting habits.
Lip bumper: The lip bumper has an acrylic pad that holds the lower lip away from the incisors. This makes the habit difficult to perform. Lip bumpers can be removable or fixed.
Oral screen: It prevents the lip from being postured between anterior teeth.
Hawley-type appliance: This appliance with spikes or rakes in the intercanine area makes the lower lip biting habit difficult to perform.
Functional appliances such as Frankel’s functional regulators: Aim at correcting the backwardly placed mandible and eliminating the lip habit. Frankel’s functional regulator appliances have a lip bumper (lip pads) component in them.
Muscle exercises: In lip biting or sucking habit, the tone of lip muscles gets affected. Lips become flaccid and can be corrected with lip exercises while trying to bring altered structures back to their position. The lip exercises are described under the management of mouth breathing habits.
Bruxism/Clenching
Bruxism presents with tectonic-like contraction of muscles of mastication and rhythmic side-to-side grinding and clenching of teeth for purposes other than mastication. It is also called psychogenic tic.
It is a psychogenic or functional aberration seen during any part of the day including sleeping hours or throughout the day.
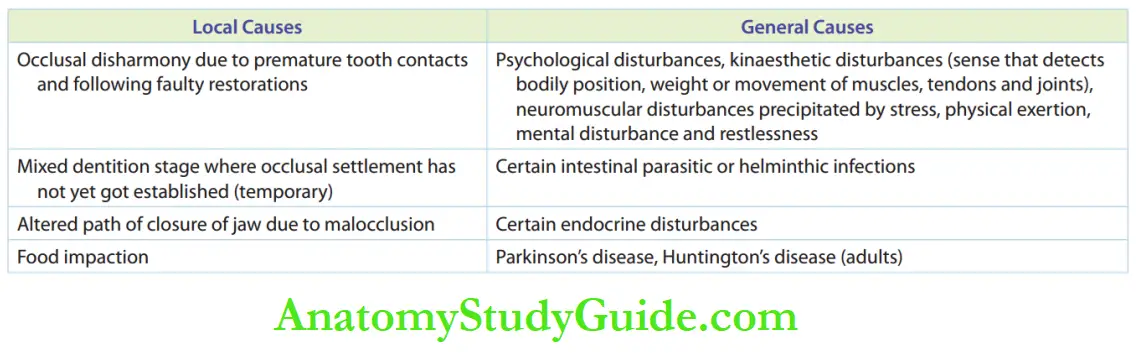
The pathogenesis of bruxism is poorly understood and is still under study. General and local factors associated with bruxism are given.
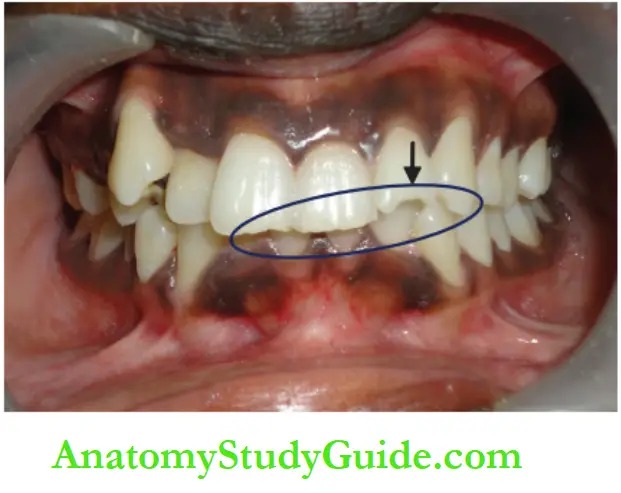
Clinical Features:
Constant grinding of teeth leads to wearing out or attrition of enamel and exposure to dentine. It results in hypersensitivity of teeth.
Localised periodontal trauma is likely to happen around the tooth that experiences maximum stress.
The long-term effects of bruxism include decreased lower facial height and hypertrophied masseter giving an everted appearance to the angles of the mandible.
Nocturnal bruxism or the grinding of teeth during sleep at night is not realised by the individual.
The person wakes from sleep with soreness of muscles of the face, neck and temporomandibular joint. The discomfort is reduced as the day progresses.
Management:
The methods involved in the management of bruxism include the following:
- Elimination of local or general causes
- Occlusal equilibrations/adjustments, traumatic high point elimination
- Psychological counselling – education and motivation
- Medications for symptomatic management:
-
- Analgesics
- Topical counter-irritants and massaging sore areas
- Muscle relaxants
- Topical medicaments, desensitising pastes or restorations to address hypersensitivity of teeth
- Anxiolytic drugs: calming effect on the mind
- Anti-helminthic drugs (as nocturnal bruxism is observed in individuals with helminthic infections, elimination of the habit should include ruling out such infections)
5. Stress-relieving disciplines such as yoga, meditation and autohypnosis, especially in adolescents
6. Appliances:
- Cap splints – help in relieving occlusal interference and prevent attrition of teeth
- Crowns for occlusal worn-out teeth to restore lost occlusal height and prevent further attrition
- Prosthetic replacement of lost teeth
Frenum Sucking Habit
A prominent labial frenum of the maxillary arch may trigger the habit of frenum sucking. The labial frenum is sucked, pulled and held between incisors.
This results in median diastema. The diastema may increase in size and disturb the alignment of teeth and aesthetics.
The frenum is subjected to constant irritation and soreness. Frenectomy solves the problem.
Nail Biting Habit
Abnormal habits that are more often seen among the younger population include nail biting, pencil biting (needle and bobby pin biting – among elders, especially tailors), etc. These habits have fewer untoward consequences.
These habits involve anterior teeth, more often the incisors. Notching, grooving and mild displacement of incisors may be observed.
The habit is initiated by stressful conditions and perceived as a stress reliever and repeated.
Treatment involves identification of any precipitating stress, counselling, motivation and thereby eliminating the habit.
Self-Inflicting Oral Habit
Self-inflicting or self-destructive oral habits are also called masochistic or sadomasochistic habits. These mutilating habits cause serious physical harm to the child’s oral tissues.
Self-inflicting habits are commonly associated with mental retardation syndromes or when a child seems happy to experience discomfort or pain.
Normal children express their anger or revenge by injuring themselves when their ego is hurt due to serious psychological insults.
These habits are commonly seen in
- Attention-seeking children who are neglected
- Mentally challenged children
- Children with organic diseases such as Lesch–Nyhan syndrome and de Lange syndrome
The common self-inflating habits are as follows:
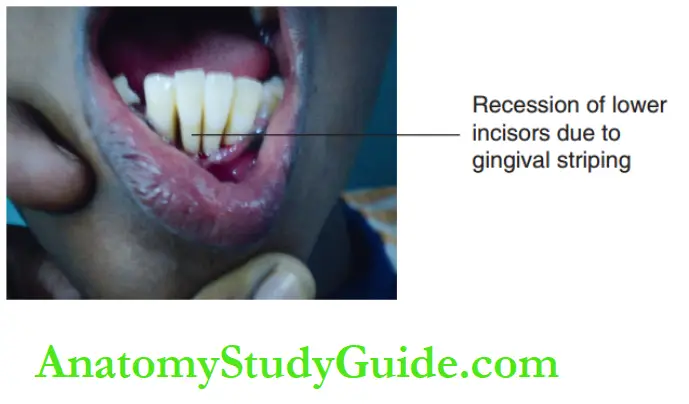
- Stripping gingiva with fingernails
- Cheek sucking and chewing
- Chewing tongue or lip
- Head banging
- Hair pulling
Management:
1. Treatment of the cause
- Psychological management and counselling for parents/siblings and child
- Psychiatrist consultation for a mentally challenged child
- Treatment of organic diseases
2. Appliances
- Capping officers
- Restricting movement of the hand, making it difficult to reach the mouth
- Lip bumper
- Oral screen
Summary
1. Pernicious oral habit is a habit involving orofacial structures that results in highly damaging consequences affecting oral and maxillofacial structures.
2. The trident feature of an oral habit: ‘3’ factors decide the extent of damage caused to oral structures by an oral habit, namely frequency, intensity and duration (FID).
3. The buccinator mechanism explains the balance between soft tissue and hard tissue and muscle and bone in the orofacial region.
4. Various forms of oral pernicious habits:
- Mouth Breathing,
- Thumb/Figer Sucking,
- Tongue Thrusting,
- Lip Biting
- Self-Injurious Habit.
- Other minor forms: pencil biting and bruxism.
5. Common management formula for correction of all oral habits:
- Elimination Of Aetiology,
- Psychological Support,
- Habit Breaking Appliances
- Toning Muscle Exercises.
6. Mouth breathing habit: Mouth breathers are grouped as obstructive mouth breathers, habitual mouth breathers and anatomical mouth breathers.
Water-holding test and rhinomanometry are the confirmatory tests to confirm mouth breathing. Habit-breaking appliance – oral screen.
Thumb/finger/digit sucking habit:
Appliances:
oral screen and Hawley-type removable appliances or fixed appliances with spikes/rakes/cribs.
8. Tongue thrusting habit:
Appliances:
- Hawley-type appliance,
- Fied Appliances With Spikes/Rakes And
- Bluegrass Appliance With Rolling Tefln Beads Placed In The Anterior Region.
9. Lip biting/sucking habit:
- Appliances –
- Lip Bumpers,
- Oral Screens,
- Hawley-Type Appliance With Spikes/ Rakes And
- Functional Appliances Such As Frankel’s Functional Regulators.
10. Bruxism/clenching:
Management-
- Occlusal Equilibrations/Adjustments, Traumatic High Point Elimination And
- Medications For Symptomatic Management.
Appliances:
- Cap Splints,
- Prosthetic Replacement Oflost Teeth
- Crowns.
11. Frenum-sucking habit: Median diastema occurs. Aesthetics is affected.
12. Self-destructive oral habit: The child injures himself and seeks emotional relief from the pain caused.
Leave a Reply