The Skin
Normal Structure
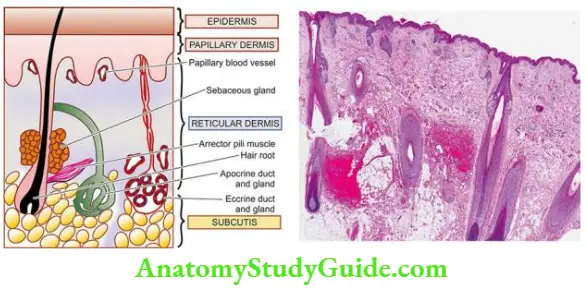
The histology of normal skin shows some variation in different parts of the body. In general, it is composed of 2 layers, the epidermis and the dermis, which are separated by an irregular border. Cone-shaped dermal papillae extend upward into the epidermis forming peg-like rete ridges of the epidermis.
Table of Contents
presents a diagrammatic representation of the main structures identifiable in a section of the normal skin while showing the various layers of the epidermis.
Read And Learn More: Systemic Pathology Notes
Epidermis: The epidermis is composed of the following 5 layers from the base to the surface:
1. Basal cell layer (stratum germinated): The basal cell layer consists of a single layer of keratinocytes that forms the junction between the epidermis and dermis. The nuclei of these cells are perpendicular to the epidermal basement membrane.
- These are hyperchromatic and normally contain a few mitoses indicating that the superficial epidermal layers originate from the basal cell layer.
- These cells are interconnected with each other and with the overlying squamous cells by desmosomes. Interspersed in the keratinocytes are melanocytes, a type of dendritic cells, in the ratio of 1: 4 to 1: 10 depending upon the site of the body.
- However, racial difference in the complexion depends upon the content of melanin per melanocyte rather than on the number of melanocytes. These cells have small nuclei with clear cytoplasm containing melanin pigment granules that determine the appearance of an individual.
- They are always positive about Dopa’s reaction. The other type of dendritic cells in the basal layer are Langerhans cells which are bone marrow-derived cells of the mononuclear-phagocyte system.
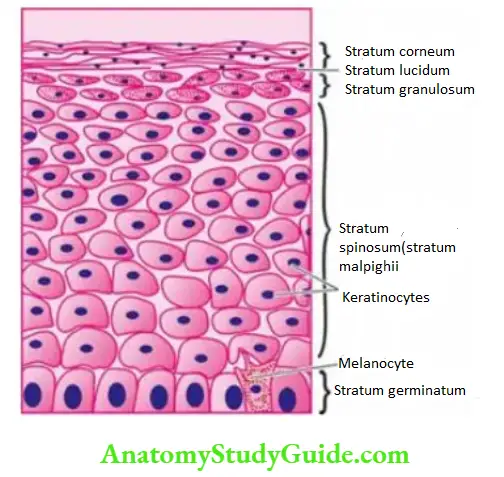
2. Prickle cell layer (Stratum spinosum, Stratum malpighii): This layer is composed of several layers of polygonal prickle cells or squamous cells. The layers become flat as they near the surface so that their long axis appears parallel to the skin’s surface.
These cells possess intercellular bridges or tonofilaments. These intercellular cytoplasmic tonofilaments contain PAS-positive material that is a precursor of keratin.
3. Granular cell layer (Stratum granulosum): This layer consists of 1 to 3 layers of flat cells containing keratohyalin basophilic granules which are PAS-negative. The granular cell layer is much thicker in palms and soles.
4. Stratum lucidum: This layer is present exclusively in palms and soles as a thin homogeneous, eosinophilic, non-nucleate zone.
5. Horny layer (Stratum corneum): The stratum corneum is also normally devoid of nuclei and consists of eosinophilic layers of keratin. Intraepidermal nerve endings are present in the form of Merkel cells which are touch receptors.
Dermis The dermis consists of 2 parts the superficial pars papillaris or papillary dermis, and the deeper pars reticularis or reticular dermis.
The dermis is composed of fibro collagenic tissue containing blood vessels, lymphatics and nerves. In the skin of fingers, arteriovenous shunts or glomeruli are normally present. The specialised nerve endings present at some sites perform specific functions. These are as under:
- Pacinian corpuscles concerned with pressure are present in the deep layer of skin.
- Meissner corpuscles are touch receptors, located in the papillae of the skin of palms, soles, tips of fingers and toes.
- Ruffini corpuscles are cold receptors found in the external genitalia.
- End-bulbs of Krause are cold receptors found in the external genitalia.
Besides these structures, the dermis contains cutaneous appendages or adnexal structures. These are sweat glands, sebaceous glands, hair follicles, arrectores pilorum and nails:
1. Sweat Glands: These are of 2 types eccrine and apocrine.
- Eccrine glands They are present all over the skin but are most numerous on the palms, soles
and axillae. They are coiled tubular glands lying deep in the dermis. Their ducts pass through the
epidermis on the surface of the skin as pores via which they empty their secretion of sweat.- The glands are lined by two main types of secretory cells basal, acidophilic, clear or chief cells, and
superficial, basophilic, dark granular cells. The secretory cells are surrounded by myoepithelial cells.
- The glands are lined by two main types of secretory cells basal, acidophilic, clear or chief cells, and
- Apocrine glands are encountered in some areas only in the axillae, in the anogenital region, in the external ear as modified glands called ceruminous glands, in the eyelids as Moll’s glands, and in the breast as mammary glands.
- Apocrine glands are also tubular glands but have larger lumina. Apocrine glands have a single layer of secretory cells which contain acidophilic, PAS-positive, prominent granular cytoplasm.
- The type of secretion in apocrine glands is decapitation secretion as if the cytoplasm of the secretory cells is pinched off (apo = off).
2. Sebaceous (Holocrine) Glands: Sebaceous glands are found everywhere on the skin except on the palms and soles. They are often found in association with hair but can be seen in a few areas devoid of hair as modified sebaceous glands such as in the external auditory meatus, nipple and areola of the male and female breast, labia minora, prepuce, and meibomian glands of the eyelids. Sebaceous glands are composed of lobules of sebaceous cells containing small round nuclei and abundant fatty, network-like cytoplasm.
3. Hair: The hair grows from the bottom of the follicle. It has, therefore, an intracutaneous portion present in the hair follicle and the shaft. The hair follicle consists of epithelial and connective tissue components. The hair shaft is made up of an outer sheath and pigmented cortex and inner medulla.
4. Arrectores Pili: These are small bundles of smooth muscle attached to each hair follicle. When the muscle contracts, the hair becomes more erect, and the follicle is dragged upwards so as to become prominent on the surface of the skin producing what is known as ‘goose pimple skin’.
5. Nails: The nails are thickenings of the deeper part of the stratum corneum that develop at the specially modified portion of the skin called the nail bed. The nail is composed of clear horny cells, resembling stratum lucidum but these cells are much more keratinised.
Common Histopathologic Terms
Before describing the pathology of common skin diseases, the following pathologic terms in common use need to be defined for the understanding of dermatopathology:
Acanthosis Thickening of the epidermis due to hyperplasia of stratum malihini.
Acantholysis Loss of cohesion between epidermal cells with formation of intraepidermal space containing oedema fluid and detached epithelial cells.
Dyskeratosis Abnormal development of epidermal cells resulting in rounded cells devoid of their
prickles and having pyknotic nuclei. Dyskeratosis is a feature of premalignant and malignant lesions and is rarely seen in benign conditions.
Hyperkeratosis Thickening of the horny layer.
Parakeratosis Abnormal keratinisation of the cells so that the horny layer contains nucleated keratinocytes rather than the normal non-nucleate keratin layer.
Spongiosis is Intercellular oedema of the epidermis which may progress to vesicle formation in the epidermis.
Pigment incontinence Loss of melanin pigment from damaged basal cell layer so that the pigment accumulates in the melanophages in the dermis.
Normal Structure:
- The skin has 2 layers, the epidermis and the dermis. Cone-shaped dermal papillae extend upward into the epidermis forming peg-like rete ridges.
- Various layers of the epidermis from below upwards are stratum germinated, stratum malihini, stratum granulosum, stratum lucidum (in palms and soles) and stratum corneum.
- The dermis has fibro collagenic tissue containing blood vessels, lymphatics and nerves, and adnexal structures (sweat glands, sebaceous glands, hair follicles, arrectores pilorum and nails).
Dermatoses
Dermatosis is a common term used for any non-neoplastic skin disorder. Dermatosis may be of various types such as genetic, inflammatory, infectious, granulomatous, connective tissue, bullous and scaling type. A few common examples of each of these groups are described below.
Genetic Dermatoses
1. Ichthyosis: Two important forms of ichthyosis are ichthyosis vulgaris and X-linked ichthyosis.
Ichthyosis vulgaris: is an autosomal dominant disorder. It is more common and appears a few months after birth as scaly lesions on the extensor surfaces of the extremities.
Histologically, the characteristic feature is an association of hyperkeratosis with a thin or absent granular layer.
X-linked ichthyosis: is a sex-(X) linked recessive disorder. It begins shortly after birth and affects extensor as well as flexor surfaces but palms and hands are spared.
Histologically, there is hyperkeratosis with normal or thickened granular cell layer and acanthosis.
2. Keratosis Palmaris Et Plantaris: The condition occurs in both autosomal dominant and autosomal recessive forms. It mainly affects the palms and soles as localised or diffuse lesions.
Histologically, there is marked hyperkeratosis, hypergranulosis, acanthosis and mild inflammatory infiltrate in the upper dermis.
3. Xeroderma Pigmentosum: This is an autosomal recessive disorder in which unexposed skin is more vulnerable to damage. The condition results from decreased ability to repair the sunlight-induced damage to DNA. Patients of xeroderma pigmentosum are more prone to develop various skin cancers like squamous cell carcinoma, basal cell carcinoma and malignant melanoma.
Histologically, the changes include hyperkeratosis, thinning and atrophy of stratum malihini, chronic inflammatory cell infiltrate in the dermis and irregular accumulation of melanin in the basal cell layer. Changes in skin cancers mentioned above may occur when the disease is in the advanced stage.
4. Darier’S Disease (Keratosis Follicularis) The condition is either transmitted as an autosomal dominant disorder or as a mutation. In typical cases, there is an extensive papular eruption.
Histologically, the characteristic changes are hyperkeratosis, papillomatosis and dyskeratosis.
Dyskeratosis results in the formation of ‘corps roads (present in the granular layer as a central homogeneous basophilic dyskeratotic mass surrounded by a clear halo) and ‘grains’ (having grain-shaped elongated nuclei surrounded by homogeneous dyskeratotic material) and there is the appearance of suprabasal clefts containing acantholytic cells. The dermis often shows chronic inflammatory cell infiltration.
5. Urticaria Pigmentosa: Urticaria pigmentosa may occur as a congenital form or may
appear without any family history in adolescents. Clinically, the condition presents as
extensive pigmented macules.
Histologically, the epidermis is normal except for an increase in melanin pigmentation in the basal cell layer. The characteristic feature is the presence of numerous mast cells in the dermis.
6. Ataxia Telangiectasia: An autosomal recessive disorder caused by mutation of the Atm gene on Chromosome 11, ataxia appears in infancy, while telangiectasia appears in childhood.
The lesions are located on the conjunctivae, cheeks, ears and neck. These children are more prone to develop infections, especially of sinopulmonary, carcinoma (skin, breast, lung etc) and lymphoma-leukaemia.
Histologically, the papillary dermis shows numerous dilated blood vessels.
Non-Infectious Inflammatory Dermatoses
A very large number of skin diseases have acute or chronic inflammation as a prominent feature. A few selected examples of non-infectious acute and chronic inflammatory dermatoses which have not been covered in other groups of dermatoses are given below.
1. Dermatitis (Eczema): The pathologic term dermatitis is synonymous with the clinical term eczema. Both refer to inflammatory responses to a variety of agents acting on the skin from outside or from within the body such as chemicals and drugs, hypersensitivity to various antigens and haptens etc.
- Accordingly, clinical types such as contact dermatitis, atopic dermatitis, drug-induced dermatitis, photo-eczematous dermatitis and primary irritant dermatitis are described.
- Many idiopathic varieties of skin disorders such as pompholyx, seborrheic dermatitis, exfoliative dermatitis (erythroderma) and neurodermatitis (lichen simplex chronic) are also included under this heading.
- In general, these conditions are clinically characterised by itching, erythema with oedema, oozing and scaling. However, irrespective of the clinical type of dermatitis, the histopathologic picture is similar.
Histologically, dermatitis reaction may be acute, subacute or chronic.
- Acute dermatitis is characterised by considerable spongiosis (intercellular oedema) that may lead to the formation of intraepidermal vesicles or bullae.
- The vesicles and bullae as well as the oedematous epidermis are permeated by acute inflammatory cells. The upper dermis shows congested blood vessels and mononuclear inflammatory cell infiltration, especially around the small blood vessels.
- Subacute dermatitis may follow acute dermatitis. Spongiosis and vesicles are smaller than in acute dermatitis. The epidermis shows moderate acanthosis and varying degree of parakeratosis in the horny layer with the formation of surface crusts containing degenerated leucocytes, bacteria and fibrin. The dermis contains perivascular mononuclear infiltrate. The classical example of subacute dermatitis is nummular dermatitis.
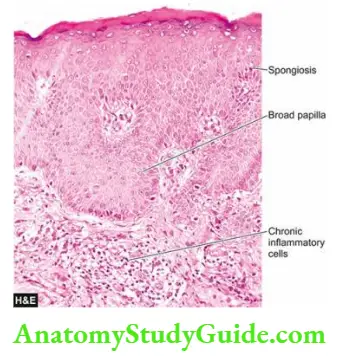
- Chronic dermatitis shows hyperkeratosis, parakeratosis and acanthosis with elongation of the rete ridges and broadened dermal papillae. Vesicles are absent but slight spongiosis may be present.
- The upper dermis shows perivascular chronic inflammatory infiltrate and fibrosis. The most characteristic example of chronic dermatitis is lichen simplex chronicus.
2. Urticaria: Urticaria or hives is the presence of transient, recurrent, pruritic wheals (raised erythematous areas of oedema). Hereditary angioneurotic oedema is an uncommon variant of urticaria in which there is recurrent oedema not only on the skin but also on the oral, laryngeal
and gastrointestinal mucosa.
Histologically, there is dermal oedema and a perivascular mononuclear infiltrate. There is localised mast cell degranulation by sensitisation with specific IgE antibodies but no increase in dermal mast cells (c.f. mastocytosis in which there is an increase in dermal mast cells).
3. Miliaria: Miliaria is a condition in which there is cutaneous retention of sweat due to obstruction of sweat ducts. There are 2 types of miliaria: miliaria crystallina and miliaria rubra.
- Miliaria crystallina occurs when there is obstruction of the sweat duct within the stratum corneum. It occurs in areas of the skin exposed to the sun or may occur during a febrile illness.
- Histologically, there are intracorneal or subcorneal vesicles which are in continuity with underlying sweat ducts.
- Miliaria rubra occurs when there is obstruction of sweat ducts within the deeper layers of the epidermis. It is seen more often in areas of skin covered by clothes following profuse sweating and the lesions are itchy.
- Histologically, there are spongiotic vesicles in the stratum malpighii similar to those seen in dermatitis. These vesicles are in continuity with a sweat duct. The adjacent dermis usually shows chronic inflammatory infiltrate.
4. Panniculitis (Erythema Nodosum And Erythema Induratum):
Panniculitis is an inflammation of the subcutaneous fat. Panniculitis may be acute or chronic. Generally, panniculitis appears as nodular lesions, predominantly on the lower legs. The following types of panniculitis are described:
- Erythema nodosum, acute or chronic, is the most common form. The lesions consist of tender red nodules, 1-5 cm in diameter, seen more often on the anterior surface of the lower legs. Erythema nodosum is often found in association with bacterial or fungal infections, drug intake, inflammatory bowel disease and certain malignancies.
- Erythema induratum is a less common variety. The lesions are chronic, painless, slightly tender, recurrent and found on the calves of the lower legs.
Histologically, the early lesions show necrotising vasculitis involving the blood vessels in the deep dermis and subcutis. In the chronic stage, there is an inflammatory infiltrate consisting of lymphocytes, histiocytes and multinucleate giant cells. The infiltrate is located in the septa separating the lobules of fat.
5. Acne Vulgaris: Acne vulgaris is a very common chronic inflammatory dermatosis found predominantly in adolescents in both sexes.
- The lesions are seen more commonly on the face, upper chest and upper back. The appearance of lesions around puberty is related to physiologic hormonal variations.
- The condition affects the hair follicle, the opening of which is blocked by keratin material resulting in the formation of comedones.
- Comedones may be open having a central black appearance due to oxidation of melanin called blackheads, or they may be in closed follicles referred to as white heads. Closed comedones may get infected and result in pustular acne.
Histologically, a comedone consists of keratinised cells, sebum and bacteria. The hair follicle containing a comedone is surrounded by lymphocytic infiltrate in papular acne, and neutrophilic infiltrate in pustular acne.
Sometimes, the wall of the distended follicle is disrupted so that the contents escape into the dermis where they may incite a granulomatous reaction.
Infectious Dermatoses
Microorganisms such as bacteria, viruses and fungi are responsible for a large number of dermatoses. Some common examples of each category are described below.
- 1. Impetigo: Impetigo is a common superficial bacterial infection caused by staphylococci and streptococci. The condition may occur in children or in adults and more commonly involves hands and face. The lesions appear as vesica-pustules which may rupture and are followed by characteristic yellowish crusts.
- Histologically, the characteristic feature is the subcorneal pustule which is a collection of neutrophils under the stratum corneum.
- Often, a few acantholytic cells and gram-positive bacteria are found within the pustule. The upper dermis contains severe inflammatory reactions composed of neutrophils and lymphoid cells.
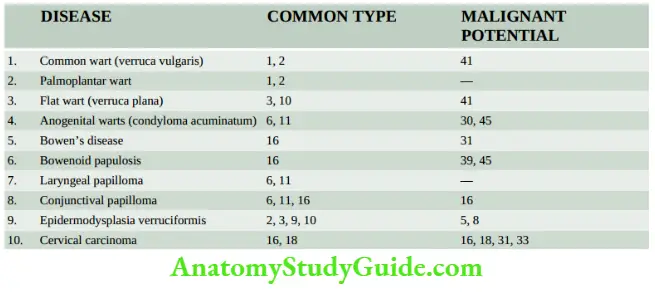
- 2. Verrucae (Warts): Verrucae or warts are common viral lesions of the skin. They are caused by human papillomaviruses (Hpv) that belong to the papovavirus group, a type of DNA oncogenic virus. More than 100 HPV types have been identified.
- But it must be appreciated that various types of HPVs produce not only different morphologic lesions but also have variable oncogenic potential as summed up.
- Infection with HPV is acquired by direct contact or by autoinoculation. Verrucae may undergo spontaneous regression in a few months to 2 years or may spread to other sites. Depending upon the clinical appearance and location, they are classified into different types described below.
- Verruca vulgaris: is the most common human wart, commonly caused by HPV-1 and 2. The lesions are often multiple, less than 1 cm in size, circumscribed, firm, elevated papules occurring more commonly on the dorsal surfaces of hands and fingers.
- Verruca plana, on the other hand, is a flat or slightly elevated wart, common on the face and dorsal surface of hands and is usually associated with HPV-10.
- Verruca planetaries or plantar warts: occur on the sole of the foot and are caused by HPV-1. They are covered with a thick callus. They may, therefore, resemble calluses or verrucous carcinoma.
- Epidermodysplasia verruciformis: resembles verruca plana but differs by having familial occurrence with autosomal recessive inheritance. The genome of HPV types 5 and 8 have been found in some of these tumours.
- Epidermodysplasia verruciformis: is of special clinical significance as it may undergo malignant change, usually into Bowen’s disease, and occasionally into squamous cell carcinoma.
- Condyloma acuminatum or venereal wart: or anogenital wart occurs on the penis, on the vulva and around the anus. They are commonly caused by HPV-6. The lesions appear as soft, papillary, cauliflower-like masses that may grow fairly large in size (giant condyloma acuminate). In rare cases, transformation into verrucous carcinoma may occur.
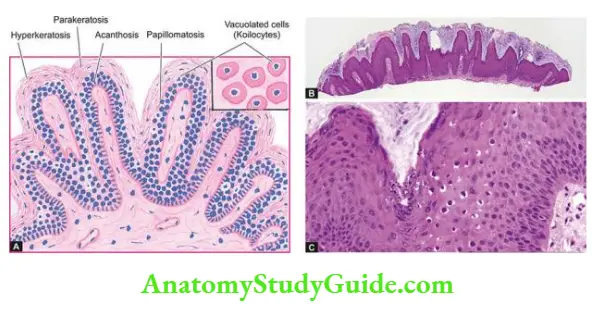
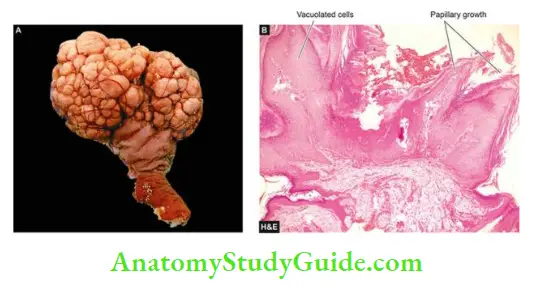
Histologically, a prototype of verruca is a common viral wart having the following features:
- Papillomatosis (papillary folds).
- Acanthosis (hyperplasia of stratum malpighii) containing foci of vacuolated cells in the upper stratum malpighii.
- Hyperkeratosis with parakeratosis.
- Clumped keratohyalin granules in the granular cells in the valleys between adjacent papillae.
- Elongation of rete ridges with their lower tips bent inwards.
- Virus-infected epidermal cells contain prominent vacuolation (koilocytosis) and keratohyalin granules of intracytoplasmic keratin aggregates due to viral cytopathic effects. These cells on electron microscopy reveal numerous intranuclear viral particles.
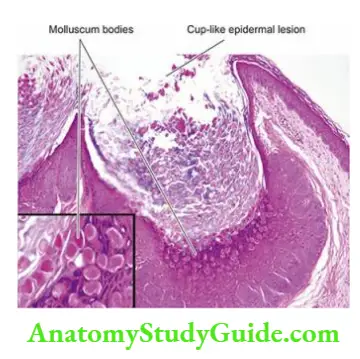
3. Molluscum Contagiosum: Molluscum contagiosum is a common self-limiting contagious lesion caused by a poxvirus which is a DNA virus. It is more common in children and young adults. Infection is acquired by direct contact.
Clinically, the lesions are often multiple, discrete, waxy, papules, about 5 mm in diameter and are seen more frequently on the face and trunk. In a fully-developed lesion, a small amount of paste-like material can be expressed on pressing.
Histologically, a typical lesion consists of a sharply circumscribed cup-like or umbilicated epidermal lesion growing down into the dermis. The proliferating epidermal cells contain the pathognomonic intracytoplasmic eosinophilic inclusion bodies called molluscum bodies. These bodies contain numerous viral particles.
4. Viral Exanthemata: a group of contagious conditions in which the epidermal cells are destroyed by replicating viruses causing eruption or rash. There are predominantly two groups of viruses which may cause exanthem.
- These are the poxvirus group (for example smallpox or variola, cowpox or vaccinia), and the herpesvirus group (for example chickenpox or varicella, herpes zoster or shingles, herpes simplex). Clinically, these conditions have different presentations but the eruptive lesions may look alike and are, therefore, considered together.
- Variola (smallpox) has been globally eradicated since 1978. The route of infection is via the upper respiratory tract or mouth followed by viraemia and characteristic skin lesions.
- Vaccinia (cowpox) is primarily a disease of the teats and udders of cows but humans are infected by milking the infected animals. Varicella (chickenpox) and herpes zoster (shingles) are both caused by a common virus, varicella-zoster virus.
- Chickenpox is transmitted by the respiratory route followed by viraemia and successive crops of lesions. Herpes zoster is a different manifestation of infection with the same viral agent after years of latency. It is a disease of the nerves and the tissues supplied by the nerves.
- The condition is characterised by sharp burning pain, often disproportionate to the rash. Herpes simplex, caused by HSV-1, and another related herpetic infection, herpes genitalis, caused by HSV-2, are characterised by transmission by direct physical contact and prolonged latency.
- The vesicular lesions are often located on the skin, especially the facial skin around lips and external nares; other sites are mucosal surfaces and eyes.
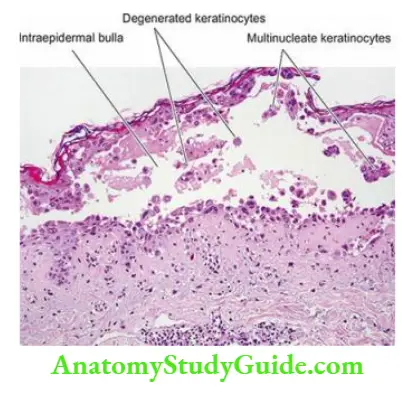
Histologically, the characteristic feature of viral exanthemata is the formation of intraepidermal vesicles or bullae due to the cytopathic effects of viruses. In the early stage, there is a proliferation of epidermal cells and the formation of multinucleate giant cells.
This is followed by intracellular oedema and ballooning degeneration that progresses on to rupture of the cells with the eventual formation of vesicles or bullae.
5. Superficial Mycoses: Superficial fungal infections of the skin are localised to the stratum corneum. These include some of the common dermatophytes such as Trichophyton rubrum and Pityrosporum. Clinically, these fungal infections are labelled according to the region involved. These are as follows:
- Tinea capitis occurs on the scalp, especially in children.
- Tinea barbae affects the region of the beard in adult males.
- Tinea corporis involve the body surface at all ages.
- Tinea cruris occurs most frequently in the region of the groin in obese men, especially in hot weather.
- Tinea pedis or ‘athlete’s foot’ is located in the web spaces between the toes.
- Onychomycosis shows the disintegration of the nail substance.
- Tinea versicolor caused by Malassezia furfur generally affects the upper trunk.
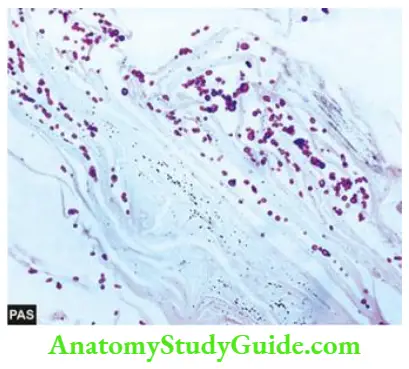
Histologically, fungal hyphae (or mycelia) and arthrospores of dermatophytes are present in the stratum corneum of skin, nails or hair. Hyphae may be septate or nonseptate. Spores are round to oval bodies which grow by budding.
Special stains can be used to demonstrate the fungi. These are the periodic acid-Schiff (PAS) reaction which stains the fungi deep pink to red, and Grocott’s methenamine silver nitrate (GMS) method which stains fungi black.
Granulomatous Diseases
In many skin diseases, the host may respond by granulomatous inflammation to a variety of microbial agents and nonmicrobial material. Tuberculosis of the skin is the classical example in which typical tubercles are formed other conditions are leprosy, syphilis, sarcoidosis, deep fungal infection etc. These conditions have already been discussed.
- Nonmicrobial agents which can incite granulomatous inflammation are keratin, hair, thorns, talc, minerals like beryllium, asbestos and tattoo pigment etc.
- Important representative examples of granulomatous inflammation lupus vulgaris, cutaneous sarcoidosis and granuloma annulare, are described here.
1. Lupus Vulgaris: The lesions of lupus vulgaris, the prototype of skin tuberculosis, are found most commonly on the head and neck, especially the skin of the nose. They are yellowish-brown to reddish-brown tiny nodules (apple-jelly nodules).
Histologically, the nodules consist of well-defined tubercles lying in the upper dermis. They consist of an accumulation of epithelioid cells surrounded by lymphoid cells. Caseation necrosis may be slight or absent. Langhans’ and foreign body types of giant cells are often present.
The condition needs to be distinguished from sarcoidosis of the skin (see below). Tubercle bacilli are present in very small numbers that are hard to demonstrate by acid-fast staining.
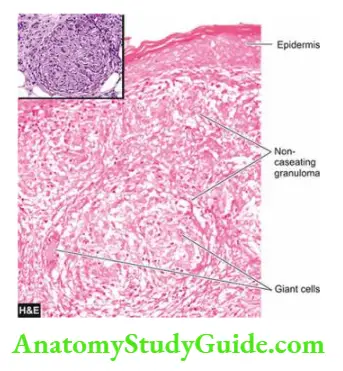
2. Cutaneous Sarcoidosis: Sarcoidosis is a systemic granulomatous disease of unknown aetiology. The lesions appear in the lungs, skin, eyes, nose and lymph nodes.
Cutaneous manifestations appear as presenting features in about a quarter of patients and include erythema nodosum or brown-red jelly-like papules or plaques with central clearing. When these lesions are seen around the nose, eyes and cheeks they are referred to as lupus pernio.

Microscopically, the characteristic feature is the presence of non-caseating epithelioid cell granulomas having Langhans’ giant cells but having a paucity of lymphocytes, also called ‘naked granulomas’. Fibrinoid necrosis and the presence of intracellular inclusions such as asteroid bodies are some other features which may be seen.
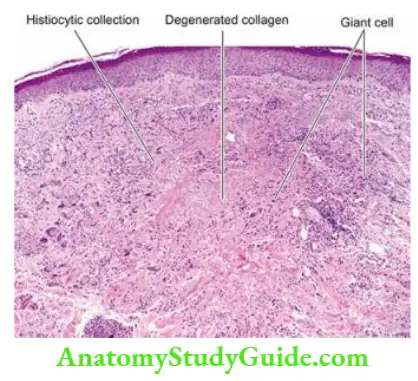
3. Granuloma Annulare: The lesions of granuloma annulare are often numerous. Dermal nodules are arranged in a ring-like fashion, commonly on the hands and feet. The condition appears to have a correlation with diabetes mellitus.
Histologically, the centre of the lesion shows a well-demarcated focus of complete collagen degeneration. These foci are surrounded by an infiltrate composed largely of histiocytes and some mononuclear inflammatory cells forming a palisade arrangement and are therefore also referred to as palisading granulomas.
Connective Tissue Dermatoses
A group of diseases caused by self-antigens or autoimmune diseases are included under connective tissue diseases.
- A list of such diseases along with their etiology and pathogenesis is given. The morphology of skin lesions of two important representative examples lupus erythematosus and systemic sclerosis (scleroderma), is given below.
- Another connective tissue disease of unknown aetiology, lichen sclerosis et atrophicus, is also considered here.
1. Lupus Erythematosus: Two types of lupus erythematosus are recognised—a chronic form, discoid lupus erythematosus (DLE) which is confined to the skin; and a systemic form, systemic lupus erythematosus (Sle) that has widespread visceral vascular lesions.
- The discoid variety is more common and is generally benign, while the systemic form may be fatal, usually from renal involvement. The diagnosis is made on the basis of clinical, serologic and pathologic changes.
- The characteristic cutaneous lesions in Dle consist of well-defined erythematous discoid patches associated with scaling and atrophy and are often limited to the face.
- In contrast, cutaneous lesions in SLE are present only in a small proportion of cases and consist of erythematous, slightly oedematous patches which are without significant scaling and without atrophy.
Histologically, cutaneous lesions in DLE and SLE may not be distinguishable in all cases. The important features are as follows:
- Hyperkeratosis with keratotic plugging.
- Thinning and flattening of rete malihini.
- Hydropic degeneration of basal layer.
- Patchy lymphoid infiltrate around cutaneous adnexal structures.
- Upper dermis showing oedema, vasodilatation and extravasation of red cells.
Direct immunofluorescence reveals granular deposits of immunoglobulins, most commonly IgG and IgM, and components of complement on the basement membrane of the affected skin in both DLE and SLE.
High serum titres of antinuclear antibodies and demonstration of LE cells are other features, especially in Sle.
2. Systemic Sclerosis (Scleroderma): Two types of systemic sclerosis or scleroderma are identified: a localised form called morphea, and a generalised form called progressive systemic sclerosis.
- A variant of progressive systemic sclerosis is CREST syndrome (C = calcinosis, R = Raynaud’s phenomenon, E = oesophagal dysmotility, S = sclerodactyly and T = telangiectasia). The aetiology and pathogenesis of these conditions are already described.
- Morphea consists of lesions limited to the skin and subcutaneous tissue, while progressive systemic sclerosis consists of extensive involvement of the skin and the subcutaneous tissue and has visceral lesions too.
- The lesions generally begin in the fingers and distal extremities and then extend proximally to involve the arms, shoulders, neck and face.
Histologically, there is a thickening of the dermal collagen extending into the subcutaneous tissue. There is a pronounced chronic inflammatory infiltrate in the affected area. The epidermis is often thin, devoid of rete ridges and adnexal structures, and there is a hyalinised thickening of the walls of dermal arterioles and capillaries. Subcutaneous calcification may develop.
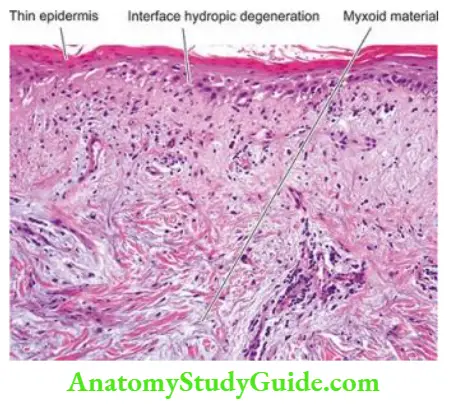
3. Lichen Sclerosus Et Atrophicus: This condition involves genital skin most frequently and is often the only site of involvement. It occurs in both sexes, more commonly in women than in men. It is termed kraurosis vulvae in women while the counterpart in men is referred to as balanitis xerotica obliterans. Occasionally, the condition may coexist with morphea. Clinically, the condition may simulate malignancy.
Histologically, the characteristic features are as under:
- Hyperkeratosis with follicular plugging.
- Thinning and atrophy of the epidermis.
- Hydropic degeneration of the basal layer.
- Upper dermis showing oedema and hyaline appearance of collagen.
- The inflammatory infiltrate in the mid-dermis.
Non-Infectious Bullous Dermatoses
This is a group of skin diseases characterised by bullae and vesicles. A bulla is a cavity formed in the layers of the skin and contains blood, plasma, epidermal cells or inflammatory cells, while a vesicle is a small bulla less than 5 mm in diameter.
- The blister is the common term used for both bulla and vesicle. The blister can be located at different sites such as subcorneal, intra-epidermal (suprabasal or subcorneal) and subepidermal. These blisters can appear in infectious as well as noninfectious dermatoses.
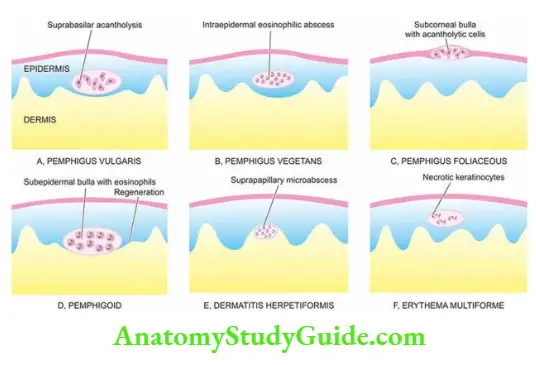
- A few common examples of noninfectious dermatoses are pemphigus, pemphigoid, dermatitis herpetiformis and erythema multiforme which are illustrated.
1. Pemphigus: Pemphigus is an autoimmune bullous disease of the skin and mucosa which has 4 clinical and pathologic variants: pemphigus vulgaris, pemphigus vegetans, pemphigus foliaceous and pemphigus erythematosus.
All forms of pemphigus have acantholysis as a common histologic feature. Sera from these patients contain IgG antibodies to cement the substance of skin and mucosa called desmoglein.
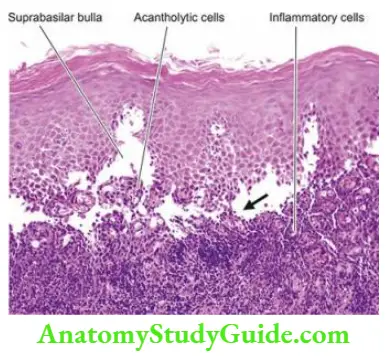
- Pemphigus vulgaris: is the most common type characterised by the development of flaccid bullae on the skin and oral mucosa. These bullae break easily leaving behind the denuded surface.
- Histologically, the bullae are suprabasal in location so that the basal layer remains attached to the dermis like a row of tombstones. The bullous cavity contains serum and acantholytic epidermal cells. On direct immunofluorescence, the fish-net pattern is seen.
- Pemphigus vegetans: is an uncommon variant consisting of early lesions resembling pemphigus vulgaris. But later, verrucous vegetations are found on the skin and oral mucosa instead of bullous lesions.
- Histologically, there is considerable acanthosis (instead of acantholysis as seen in pemphigus vulgaris) and papillomatosis. Intraepidermal abscesses composed almost entirely of eosinophils are diagnostic of pemphigus vegetans.
- Pemphigus foliaceous: is characterised by quite superficial bullae which leave shallow zones of erythema and crust.
- Histologically, superficial subcorneal bullae are found which contain acantholytic epidermal cells.
- Pemphigus erythematosus: is an early form of pemphigus foliaceous. The distribution of clinical lesions is similar to lupus erythematosus involving the face.
- Histologically, the picture is identical to that of Pemphigus foliaceous.
2. Pemphigoid: This is a form of bullous disease affecting the skin or the mucous membranes. Three variants have been described localised form occurring on the lower extremities the vesicular form consisting of small tense blisters, and vegetating form having verrucous vegetations found mainly in the axillae and groins.
Pemphigoid is caused by antibodies which are components of hemidesmosomes that bind proteins essential for adherence of basal keratinocytes to the basement membrane.
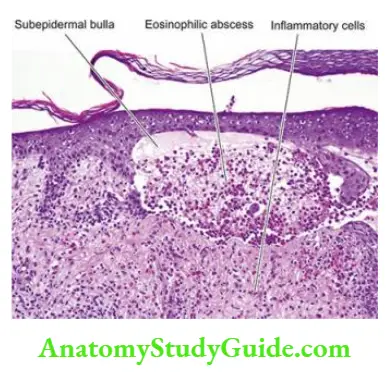
Histologically, the characteristic distinguishing feature from pemphigus is the subepidermal location of the non-acantholytic bullae. With the passage of time, there is some epidermal regeneration from the periphery at the floor of the bulla.
- The bullous cavity contains a fibrin network and many mononuclear inflammatory cells and many eosinophils. Dermal changes seen in inflammatory bullae consist of infiltration of mononuclear cells, a few eosinophils and neutrophils.
- On direct immunofluorescence, linear deposition of components is seen along the dermo-epidermal junction.
3. Dermatitis Herpetiformis Dermatitis: herpetiformis is a form of chronic, pruritic, vesicular dermatosis. The lesions are found more commonly in males in the 3rd to 4th decade of life. The disease has an association with gluten-sensitive enteropathy (coeliac disease).
Both dermatitis herpetiformis and gluten-sensitive enteropathy respond to a gluten-free diet. The pathogenesis of the disease is not quite clear but probably individuals with certain histocompatibility types develop IgA and IgG antibodies to gliadin which is a fraction of gluten present in the flour.
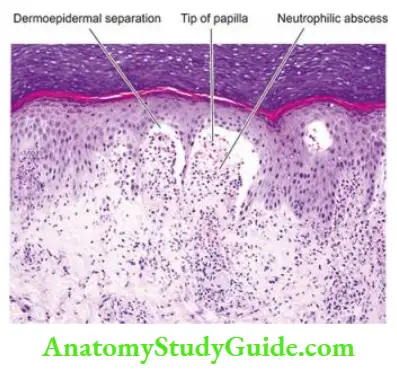
Histologically, the early lesions of dermatitis herpetiformis consist of neutrophilic microabscesses at the tips of papillae, producing separation or blister between the papillary dermis and the epidermis.
The older blisters contain a fair number of eosinophils causing confusion with bullous pemphigoid. Direct immunofluorescence shows granular deposits of IgA at the papillary tips in dermatitis herpetiformis.
4. Erythema Multiforme: This is an acute, self-limiting but recurrent dermatosis. The condition occurs due to hypersensitivity to certain infections and drugs, and in many cases, it is idiopathic.
- As the name suggests, the lesions are multiform such as macular, papular, vesicular and bullous. Quite often, the lesions have symmetric involvement of the extremities. Stevens-Johnson syndrome is a severe, at times fatal, form of involvement of skin and mucous membranes of the mouth, conjunctivae, genital and perianal area.
- Another variant termed toxic epidermal necrolysis consists of diffuse necrosis of the epidermis and mucosa, exposing the dermis and giving the skin a scalded appearance.
Histologically, the changes vary according to the clinical multiform stage.
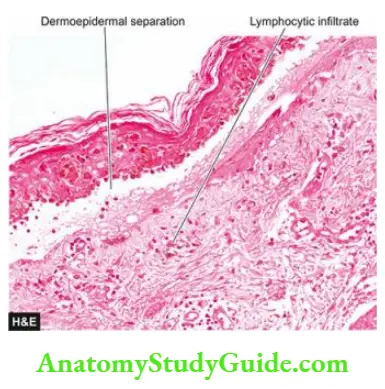
- Early lesions show oedema and lymphocytic infiltrate at the dermo-epidermal junction. The superficial dermis shows perivascular lymphocytic infiltrate.
- The later stage is associated with the migration of lymphocytes upwards into the epidermis resulting in epidermal necrosis and blister formation.
Scaling Dermatoses
The skin surface in some chronic inflammatory dermatoses is roughened due to excessive and abnormal scale formation and desquamation. Common examples of this group are psoriasis and lichen planus. Hereditary ichthyosis having similar scaly lesions has already been described.
1. Psoriasis: Psoriasis is a chronic inflammatory dermatosis that affects about 2% of the population. It usually appears first between the age of 15 and 30 years. The lesions are characterised by brownish-red papules and plaques which are sharply demarcated and are covered with fine, silvery-white scales.
- As the scales are removed by gentle scraping, fine bleeding points appear termed the Auspitz sign. Commonly involved sites are the scalp, upper back, sacral region and extensor surfaces of the extremities, especially the knees and elbows.
- In about 25% of cases, peculiar pitting of nails is seen. Psoriatic arthritis resembling rheumatoid arthritis is produced in about 5% of cases but the rheumatoid factor is absent.
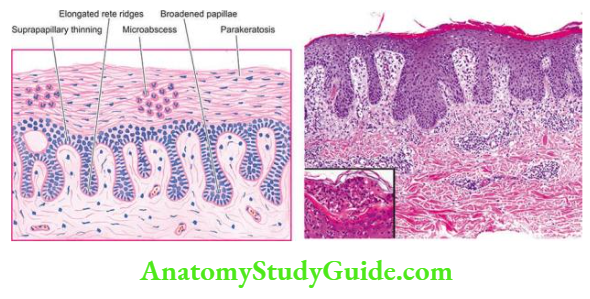
Histologically, the following features are observed in fully-developed lesions
- Acanthosis with regular down growth of rete ridges to almost the same dermal level with thickening of their lower portion.
- Elongation and oedema of the dermal papillae with a broadening of their tips.
- Suprapapillary thinning of stratum malihini.
- Absence of granular cell layer.
- Prominent parakeratosis.
- The presence of Munro microabscesses in the parakeratotic horny layer is diagnostic of psoriasis.
2. Lichen Planus: Lichen planus is a chronic dermatosis characterised clinically by irregular, violaceous, shining, flat-topped, pruritic papules. The lesions are distributed symmetrically with sites of predilection being flexor surfaces of the wrists, forearms, legs and external genitalia. The buccal mucosa is also involved in many cases of lichen planus.
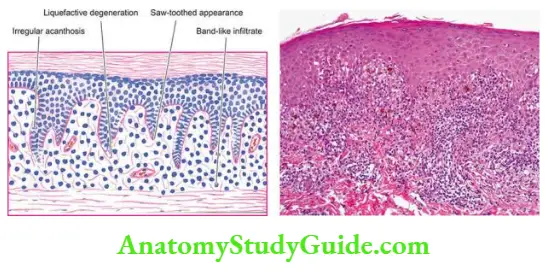
Histologically, the characteristic features are as under:
- Marked hyperkeratosis.
- Focal hypergranulosis.
- Irregular acanthosis with elongated saw-toothed rete ridges.
- Liquefaction degeneration of the basal layer.
- A band-like dermal infiltrate of mononuclear cells sharply demarcated at its lower border and closely hugging the basal layer.
Metabolic Diseases Of Skin
Skin is involved in a variety of systemic metabolic derangements. The examples include the following:
- Amyloidosis (primary as well as secondary,).
- Lipoid proteinosis is rare.
- Porphyria of various types.
- Calcinosis cutis
- Gout due to urate deposits or tophi.
- Ochronosis due to alkaptonuri.
- Mucinosis saw in myxoedema.
- Idiopathic haemochromatosis with skin pigmentation.
Many of these conditions have been discussed elsewhere in the book; calcinosis cutis is briefly considered below.
Calcinosis Cutis: There are four types of calcification in the skin:
- Metastatic calcinosis cutis
- Dystrophic calcinosis cutis
- Idiopathic calcinosis cutis
- Subepidermal calcified nodule
- Metastatic calcinosis cutis: develops due to hypercalcaemia or hyperphosphataemia as discussed.
- Dystrophic calcinosis cutis: results when there is the deposition of calcium salts at damaged tissue.
- Idiopathic calcinosis cutis: resembles a dystrophic type but is not associated with any underlying disease. A special manifestation of idiopathic calcinosis cutis is tumoral calcinosis in which there are large subcutaneous calcified masses, often accompanied by foreign body giant cell reaction.
- Calcium may discharge from the surface of the lesion. Idiopathic calcinosis of the scrotum consists of multiple asymptomatic nodules of the scrotal skin.
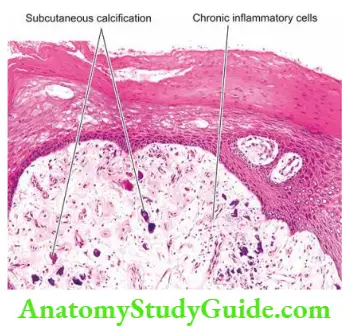
- Subepidermal calcified nodule: or cutaneous calculus is a single raised hard calcified nodule in the upper dermis
Dermatoses:
- Dermatoses are any form of non-neoplastic skin disorder example genetic, inflammatory, infectious, granulomatous, connective tissue, bullous and scaling type.
- Common examples of genetic dermatoses are ichthyosis, xeroderma pigmentosum and urticaria pigmentosa.
- A few non-infectious inflammatory dermatoses are eczema, urticaria, miliaria, panniculitis, and acne.
- Common infectious dermatoses are impetigo, verrucae, viral exanthemata, and superficial mycoses.
- Granulomatous dermatoses may be infectious (for example lupus vulgaris) or non-infectious (for example sarcoidosis, granuloma annulare).
- Examples of connective tissue dermatoses are DLE, SLE, and scleroderma.
- Some common non-infectious bullous dermatoses are pemphigus, pemphigoid, dermatitis herpetiformis, and erythema multiforme.
- Common scaling dermatoses are psoriasis and lichen planus.
Tumours And Tumour-Like Lesions
Tumours and tumour-like lesions may arise from different components of the skin such as the surface epidermis, epidermal appendages and dermal tissues. Each of these tissues may be the site for tumour-like lesions, benign tumours and malignant tumours as well.
- Besides these, there is a group of conditions and lesions which are precancerous. Another group of tumours have their origin from elsewhere in the body but are cellular migrants to the skin. A comprehensive list of tumours and tumour-like lesions of the skin is presented.
- It is beyond the scope of this book to describe all these tumours and lesions, for which the interested reader may consult specialised work on dermatopathology. Some important and common examples of these conditions are briefly described here.
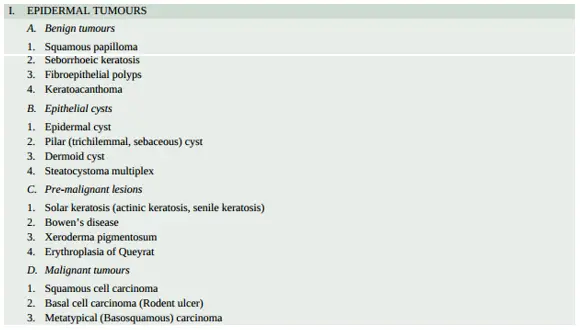
Tumours And Cysts Of The Epidermis
Benign Tumours:
1. Squamous Papilloma: a benign epithelial tumour of the skin and oral mucosa. Though considered by many authors to include common viral warts (verrucae) and condyloma acuminata, true squamous papillomas differ from these viral lesions. If these ‘viral tumours’ are excluded, squamous papilloma is a rare tumour.
Histologically, squamous papillomas are characterised by hyperkeratosis, acanthosis with elongation of rete ridges and papillomatosis. The verrucae or common warts closely resemble squamous papilloma but they can be distinguished by having foci of vacuolated cells in the acanthotic stratum malihini, vertical tiers of parakeratosis between the adjacent papillae and irregular clumps of keratohyaline granules in the virally-infected granular cells lying in the valleys between the papillae.
2. Seborrheic Keratosis: This Is A Very Common Lesion In Middle-Aged Adults. There may be only one lesion, but more often there are many. Its sudden appearance in large numbers may be a part of paraneoplastic syndrome, most commonly in tumours of GIT.
The common locations are the trunk and face. They are sharply demarcated, brownish, smooth surfaced, measuring a few millimetres in diameter.
Histologically, the pathognomonic feature is a sharply-demarcated exophytic tumour overlying a straight line from the normal epidermis at one end of the tumour to the normal epidermis at the other end. The other features are papillomatosis, hyperkeratosis and acanthosis as seen in squamous cell papillomas.
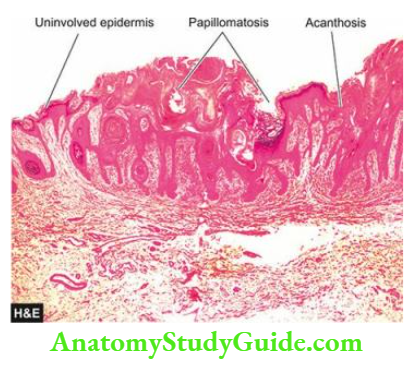
3. Fibroepithelial Polyps: Also known by other names such as skin tags acrochordons’ and ‘soft fibromas’, these are the most common cutaneous lesions. They are often multiple, soft, small (a few mm in size), bag-like tumours commonly seen on the neck, trunk and axillae.
Histologically, the tumours are composed of loosely-arranged fibrovascular cores with an overlying hyperplastic epidermis.
Epithelial Cysts
Various cysts in the skin may arise from the downward growth of the epidermis and the appendages. These cysts often contain paste-like pultaceous material containing keratin, sebaceous secretions and lipid-containing debris. Depending upon the structure of the cyst wall, these cysts are of various types as under:
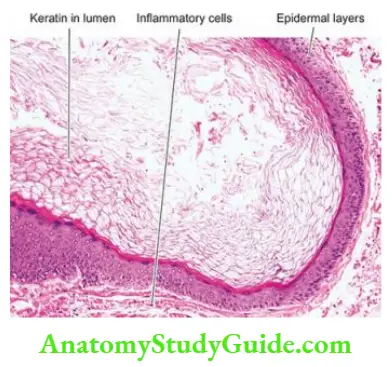
1. Epidermal Cyst: These intradermal or subcutaneous cysts, commonly called sebaceous cysts, are common and may occur spontaneously or due to implantation of the epidermis into the dermis or subcutis (implantation cysts). The most frequent sites are the skin of the face, scalp, neck and trunk.
Histologically, epidermal cysts have a cyst wall composed of a true epidermis with laminated layers of keratin. Rupture of the cyst may incite foreign body giant cell inflammatory reaction in the wall.
2. Pilar (Trichilemmal, Sebaceous) Cyst: These cysts clinically resemble epidermal cysts but occur more frequently on the scalp and are less common than epidermal cysts.
Histologically, the cyst wall is composed of palisading squamous epithelial cells having abruptly keratinised layers without an intervening granular cell layer. These squamous cells undergo degeneration towards the cyst cavity. Rupture of the cyst wall is common and leads to foreign body giant cell inflammatory reaction. Calcification in the cyst wall is often present.
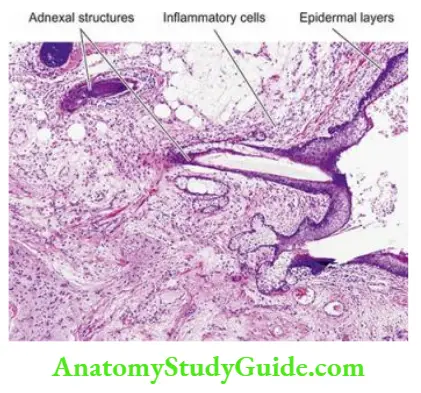
3. Dermoid Cyst: These are subcutaneous cysts often present since birth. Dermoid cysts are more common on the face, along the lines of embryonic closure.
Histologically, the cyst wall contains epidermis as well as appendages such as hair follicles, sebaceous glands and sweat glands.
4. Steatocystoma Multiplex: This is an inherited autosomal dominant disorder having multiple cystic nodules, 1-3 cm in size. They are more common in the axillae, sternum and arms.
Histologically, the cyst walls are composed of several layers of epithelial cells and contain lobules of sebaceous glands in the cyst wall.
Pre-Malignant Lesions:
1. Solar Keratosis (Actinic Keratosis, Senile Keratosis): Solar (sun-induced) or actinic (induced by a variety of rays) keratoses are multiple lesions occurring in unexposed areas of the skin in fair-skinned elderly people.
- Similar lesions may be induced by exposure to ionising radiation, hydrocarbons and arsenicals. The condition is considered to be a forerunner of invasive squamous cell and/or basal cell carcinoma.
- Clinically, the lesions are tan-brown, erythematous, about 1 cm in diameter with a rough, sandpaper-like surface and are seen more commonly on the dorsum of the hands and on the balded portion of the skin.
Histologically, solar keratosis has the following characteristic features:
- Considerable hyperkeratosis
- Marked acanthosis
- Dyskeratosis and dysplasia of the epidermal cells show features such as hyperchromatism, loss of polarity, pleomorphism and an increased number of mitotic figures.
- Non-specific chronic inflammatory cell infiltrates in the upper dermis encroach upon the basement membrane of the epidermis.
2. Bowen’S Disease: Bowen’s disease is also a carcinoma in situ of the entire epidermis but differs from solar keratosis in having solitary lesions often that may occur on sun-exposed as well as sun-unexposed skin.
The condition may occur anywhere on the skin but is found more often on the trunk, buttocks and extremities. Clinically, the lesions of Bowen’s disease are sharply circumscribed, rounded, reddish-brown patches which enlarge slowly.
Histologically, the characteristic features are as under:
- Marked hyperkeratosis
- Pronounced parakeratosis
- Marked epidermal hyperplasia with the disappearance of dermal papillae
- Scattered bizarre dyskeratotic cells distributed throughout the epidermis
Bowen’s disease may remain confined to the surface for many years and then develop into invasive cancer.
Malignant Tumours:
1. Squamous Cell Carcinoma: Two important factors in the pathogenesis of squamous cell carcinoma are: prolonged sun exposure and immunosuppression, in a predisposed individual. These etiologic agents induce DNA damage that is followed by p53 mutation and other events leading to dysregulation of a signalling pathway. Various predisposing conditions are as follows:
- Xeroderma pigmentosum
- HPV-5 and 8-induced infection in autosomal recessive disorder epidermodysplasia verruciformis
- Solar keratosis
- Chronic inflammatory conditions such as chronic ulcers and draining osteomyelitis
- Old burn scars (Marjolin’s ulcers)
- Chemical burns
- Psoriasis
- HIV infection
- Ionising radiation
- Industrial carcinogens (coal tars, oils etc)
- In the case of cancer of the oral cavity, chewing betel nuts and tobacco.

- Cancer of scrotal skin in chimney sweeps was the first cancer in which an occupational carcinogen (soot) was implicated. ‘Kangari cancer’ of the skin of the inner side of the thigh and lower abdomen common in natives of Kashmir is another example of skin cancer due to chronic irritation (Kangari is an earthenware pot containing glowing charcoal embers used by Kashmiris close to their abdomen to keep them warm).
- Squamous cell carcinoma may arise on any part of the skin and mucous membranes lined by squamous epithelium. The most common locations are the face, pinna of the ears, back of hands and mucocutaneous junctions such as on the lips, anal canal and glans penis.
- Cutaneous squamous carcinoma arising in a pre-existing inflammatory and degenerative lesion has a higher incidence of developing metastases.
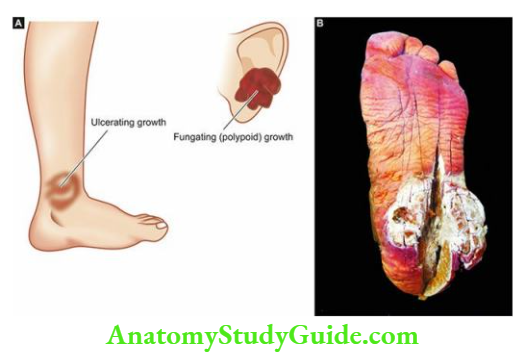
Morphologic Features Grossly, squamous carcinoma of the skin and squamous-lined mucosa can have one of the following two patterns:
- More commonly, an ulcerated growth with elevated and indurated margin is seen.
- Less often, a raised fungating or polypoid verrucous lesion without ulceration is found.
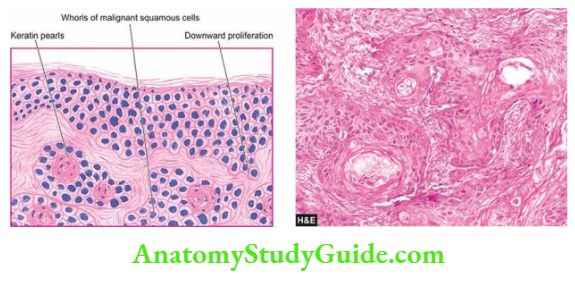
Microscopically, squamous cell carcinoma is an invasive carcinoma of the surface epidermis characterised by the following features:
- There is irregular downward proliferation of epidermal cells into the dermis.
- Depending upon the grade of malignancy, the masses of epidermal cells show atypical features such as variation in cell size and shape, nuclear hyperchromatism, absence of intercellular bridges, individual cell keratinisation and occurrence of atypical mitotic figures.
- Better-differentiated squamous carcinomas have a whorled arrangement of malignant squamous cells forming horn pearls. The centres of these horn pearls may contain laminated, keratin material.
- Higher grades of squamous carcinomas, however, have fewer or no horn pearls and may instead have highly atypical cells.
- An uncommon variant of squamous carcinoma may have spindle-shaped tumour cells (spindle cell carcinoma).
- Adenoid changes may be seen in a portion of squamous cell carcinoma (adenoid squamous cell carcinoma).
- Verrucous carcinoma (Ackerman tumour) is a low-grade variant located most commonly in the oral cavity in which the superficial portion of the tumour resembles verruca (hyperkeratosis, parakeratosis, acanthosis and papillomatosis) but differs from it in having downward proliferation as broad masses of the well-differentiated squamous epithelium into the deeper portion of the tumour. However, there is a lack of significant cellular atypia.
- All variants of squamous cell carcinoma show inflammatory reactions between the collections of tumour cells, while in pseudo carcinomatous hyperplasia, there is the permeation of the epithelial proliferation by inflammatory cells.
- Squamous cell carcinomas are often labelled by pathologists with descriptive terms such as well-differentiated, moderately-differentiated, undifferentiated, keratinising, non-keratinising, spindle cell type etc.
- The overall prognosis of squamous cell carcinoma induced by actinic keratosis is excellent. Superficial invasive tumours may metastasise locally.
- The prognosis of a deeply invading tumour depends upon the TNM staging.
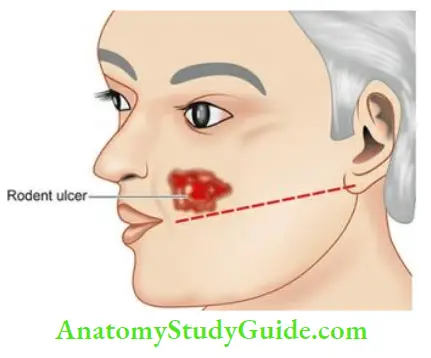
2. Basal Cell Carcinoma (Rodent Ulcer): Typically, basal cell carcinoma is a locally invasive, slow-growing tumour of middle-aged that rarely metastasises. It occurs exclusively on hairy skin, the most common location (90%) being the face, usually above a line from the lobe of the ear to the corner of the mouth.
The following conditions predispose an individual to develop basal cell carcinoma:
- Light-skinned people who have little melanin.
- Prolonged exposure to strong sunlight like in those living in Australia and New Zealand.
- An inherited defect in DNA repair mechanism in xeroderma pigmentosum.
- Nevoid basal cell carcinoma syndrome It is an autosomal dominant condition in which multiple basal cell carcinomas appear at a young age (under 20 years). These individuals inherit one defective allele (PTCH gene on chromosome 9) while another allele undergoes mutation early in life by sun exposure (Knudson’s two-hit hypothesis).
Morphologic Features Grossly, the most common pattern is a nodule-ulcerative basal cell carcinoma in which a slow-growing small nodule undergoes central ulceration with pearly, rolled margins.
- The tumour enlarges in size by burrowing and by destroying the tissues locally like a rodent and hence the name ‘rodent ulcer’.
- However, less frequently nonulcerated nodular patterns, pigmented basal cell carcinoma and fibrosing variants are also encountered.
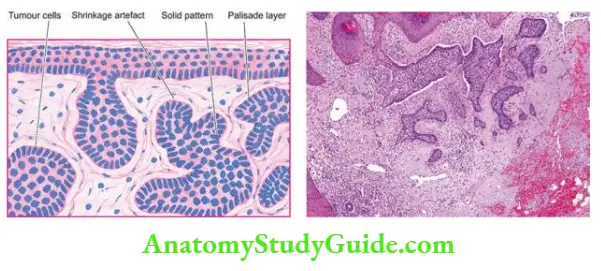
Histologically, the most characteristic feature is the proliferation of basaloid cells (resembling the basal layer of the epidermis).
- A variety of patterns of these cells may be seen solid masses, masses of pigmented cells, strands and nests of tumour cells in morphea pattern, keratotic masses, cystic change with sebaceous differentiation, and adenoid patterns with apocrine or eccrine differentiation.
- The most common pattern is solid basal cell carcinoma in which the dermis contains irregular masses of basaloid cells having the characteristic peripheral palisaded appearance of the nuclei.
- A superficial multicentric variant composed of multiple foci of tumour cells present in the dermis, especially in the trunk, has also been described.
3. Metatypical Carcinoma (Basosquamous Cell Carcinoma):
- Metatypical or basosquamous cell carcinoma is the term used for a tumour in which the cell type and arrangement of cells cause difficulty in deciding between basal cell carcinoma and squamous cell carcinoma.
- The tumour masses are composed of malignant squamous cells with horn pearls and the outer row of dark-staining basal cells. These tumours have a high malignant potential and may occasionally metastasise.
Adnexal (Appendageal) Tumours
Tumours arising from epidermal adnexa or appendages can differentiate towards hair follicles, sebaceous glands and sweat glands (apocrine and eccrine glands). Most of the adnexal tumours are benign but a few malignant variants also exist.
Tumours Of Hair Follicle:
These are uncommon benign tumours. Two important examples are trichoepithelioma and pilomatrixoma.
1. Trichoepithelioma (Brooke’S Tumour): This tumour may occur as a solitary lesion or as multiple inherited lesions, predominantly on the face, scalp and neck.
Histologically, the tumour is often circumscribed. The most characteristic histologic feature is the presence of multiple horn cysts having keratinised centres and surrounded by basophilic cells resembling basal cells. These horn cysts simulate abortive pilar structures which are interconnected by epithelial tracts.
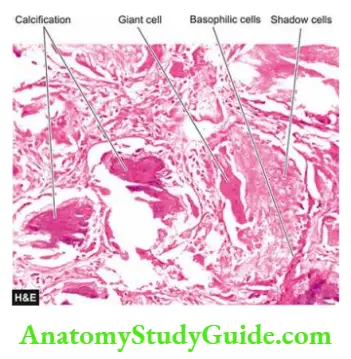
2. Pilomatricoma (Calcifying Epithelioma Of Malherbe): Pilomatricoma usually occurs as a solitary lesion, more often on the face and upper extremities. It may be seen at any age. The lesions vary in size from 0.5-5 cm and appear as well-demarcated dark red nodules.
Histologically, the circumscribed tumour is located in the deeper dermis and subcutis. The masses of tumour cells embedded in cellular stroma characteristically consist of 2 types of cells the peripheral basophilic cells resembling hair matrix cells, and the inner shadow cells having a central unstained shadow in place of the lost nucleus. Areas of calcification are present within lobules of shadow cells in three-fourths of the tumours.
Tumours Of Sebaceous Glands:
Tumours originating from sebaceous glands are commonly benign (for example naevus sebaceous and sebaceous adenoma) but sebaceous carcinoma may occasionally occur.
1. Naevus Sebaceous: Naevus sebaceous of Jadassohn occurs mainly on the scalp or face as a solitary lesion that may be present at birth. Initially, the lesion appears as a hairless plaque, but later it becomes verrucous and nodular.
Histologically, naevus sebaceous is characterised by hyperplasia of immature sebaceous glands and pilar structures. The overlying epidermis shows papillary acanthosis.
2. Sebaceous Adenoma: occurs in middle-aged persons, most commonly on the face.
Histologically, it is sharply demarcated from the surrounding tissue. The tumour is composed of irregular lobules of incompletely differentiated sebaceous glands.
3. Sebaceous Carcinoma: is a rare tumour that may occur anywhere in the body except the palms and soles. Variants of sebaceous carcinoma are carcinoma of the Meibomian glands of the eyelids and carcinoma of the ceruminous glands in the external meatus.
Histologically, the tumour is composed of variable-sized lobules of poorly-differentiated cells
containing some sebaceous cells. The tumour cells show marked cytologic atypia such as pleomorphism and hyperchromasia.
Tumours Of Sweat Glands:
A large number of lesions develop from sweat gland structures, either from apocrine or eccrine glands. These are more commonly benign but sweat gland carcinoma may also occur.
1. Eccrine Tumours: Depending upon the portion of the eccrine sweat gland from which the tumour takes origin, the eccrine tumours are of 3 types:
- arising from the intraepidermal portion of the duct example eccrine poroma;
- arising from the intradermal portion of the duct example hidradenoma; and
- arising from secretory coils example eccrine spiradenoma.
- Eccrine poroma This tumour arises from the intraepidermal portion of the sweat gland duct. The tumour is found more commonly on the soles and hands.
- Histologically, it consists of tumour cells arising from the lower portion of the epidermis and extending downward into the dermis as broad anastomosing bands. The tumour cells are, however, different from squamous cells. They are smaller in size, cuboidal in shape and have deeply basophilic nuclei.
- Eccrine hidradenoma Hidradenoma originates from the intradermal portion of the eccrine sweat duct. The tumour may occur anywhere in the body.
- Histologically, hidradenoma consists of solid masses and cords of tumour cells which may have an occasional duct-like structure containing mucin. The tumour cells are round to polygonal and may have clear or eosinophilic cytoplasm.
- Eccrine spiradenoma: This is found as a solitary, painful, circumscribed nodule in the dermis.
- Histologically, the tumour consists of lobules which are surrounded by a thin capsule. The tumour lobules contain 2 types of epithelial cells like in the secretory coils of the eccrine sweat gland.
- Peripheral cells are small with dark nuclei, while the centre of lobules contains large cells with pale nuclei. An occasional area may show glandular structures.
2. Apocrine Tumours: Apocrine sweat glands may give rise to tumours; the two common examples are papillary hidradenoma and cylindroma.
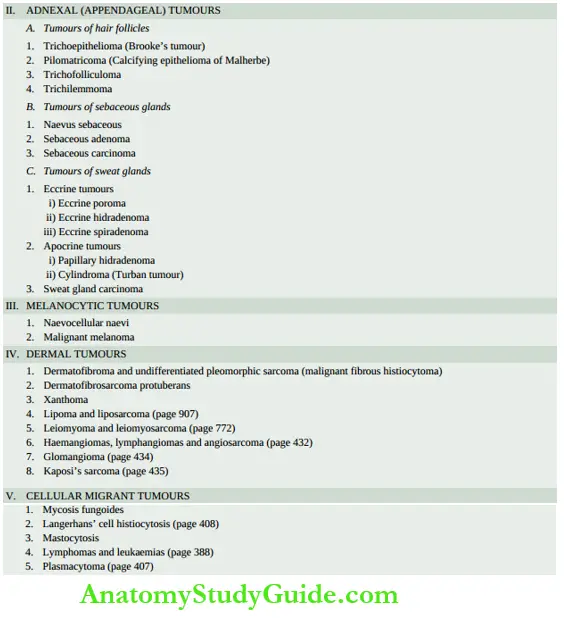
Papillary hidradenoma: or hidradenoma papilliferum is usually located as a small lesion commonly in women in the skin of the anogenital area.
Histologically, it is a circumscribed tumour in the dermis under a normal epidermis. Papillary hidradenoma represents an adenoma with apocrine differentiation and containing papillary, tubular and cystic structures. The tumour cells lining these structures resemble apocrine epithelium with features of decapitation secretions.
Cylindroma: Also called a ‘turban tumour’ due to its common location on the scalp, cylindroma may occur as both solitary and multiple lesions.
Histologically, the tumour is composed of irregular islands of tumour cells creating a pattern resembling a jigsaw puzzle. The islands are surrounded by a hyaline sheath. The tumour cells comprising the islands consist of 2 types of epithelial cells: peripheral small cells with dark nuclei, and inner large cells with light-staining nuclei. Some of the islands may contain tubular lumina containing amorphous material.
3. Sweat Gland Carcinoma: Rarely, the eccrine and apocrine gland tumours described above may turn malignant. All these carcinomas are adenocarcinomas and must be distinguished from metastatic adenocarcinoma in the skin.
Melanocytic Tumours
Melanocytic tumours may arise from one of the three cell types: naevus cells, epidermal melanocytes and dermal melanocytes.
- Benign tumours originating from naevus cells are called parvocellular naevi.
- Examples of benign tumours arising from epidermal melanocytes are lentigo, freckles, pigmentation associated with Albright’s syndrome and café-au-lait spots of neurofibromatosis.
- Benign tumours derived from dermal melanocytes are Mongolian spots, naevi of Ota and of Ito and blue naevus.
- Malignant melanoma is the malignant counterpart of melanocytic tumours. The important examples of these are described below.
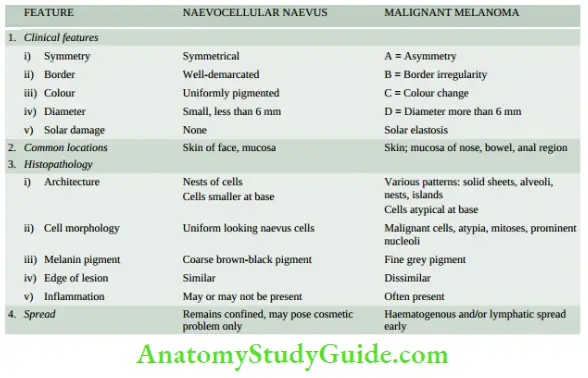
Naevocellular Naevus:
Pigmented naevi or moles are extremely common lesions on the skin of most individuals. They are often flat or slightly elevated lesions; rarely they may be papillomatous or pedunculated. Most naevi appear in adolescence and in early adulthood due to hormonal influence but rarely may be present at birth. They are mostly tan to brown and less than 1 cm in size.
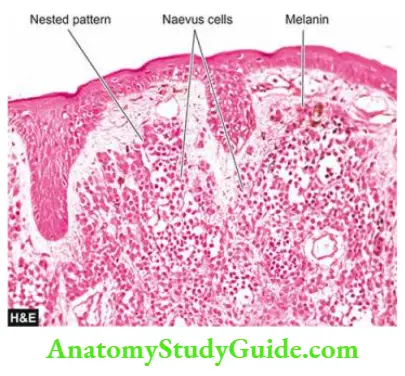
Histologically, irrespective of the histologic types, all parvocellular naevi are composed of ‘naevus cells’ which are actually identical to melanocytes but differ from melanocytes in being arranged in clusters or nests.
- Naevus cells are cuboidal or oval in shape with homogeneous cytoplasm and contain large round or oval nuclei.
- Melanin pigment is abundant in the naevus cells present in the lower epidermis and upper dermis, but the cells in the mid-dermis and lower dermis hardly contain any melanin.
The important histological variants of naevi are as under:
- Lentigo: is the replacement of the basal layer of the epidermis by melanocytes.
- The junctional naevus: is the one in which the naevus cells lie at the epidermal-dermal junction. The naevus cells form well-circumscribed nests.
- The compound naevus: is the commonest type of pigmented naevus. These lesions, in addition to the junctional activity as in junctional naevi, show nests of naevus cells in the dermis to a variable depth.
- Intradermal naevus: shows slight or no junctional activity. The lesion is mainly located in
the upper dermis as nests and cords of naevus cells. Multinucleate naevus cells are common. - Spindle cell (epithelioid) naevus or juvenile melanoma: is a compound naevus with junctional activity. The naevus cells are, however, elongated and epithelioid in appearance which may or may not contain melanin. Juvenile melanoma is important since it is frequently confused with malignant melanoma histologically.
- Blue naevus: is characterised by dendritic spindle naevus cells rather than the usual rounded or cuboidal naevus cells. These cells are often quite rich in melanin pigment.
- Dysplastic naevi: are certain atypical naevi which have an increased risk of progression to malignant melanoma. These lesions are larger than the usually acquired naevi, are often multiple, and appear as flat macules to slightly elevated plaques with irregular borders and variable pigmentation.
- Many of the cases are familial and inherited. Dysplastic naevi have melanocytic proliferation at the epidermal-dermal junction with some cytologic atypia.
Malignant Melanoma:
- Malignant melanoma or melanocarcinoma arising from melanocytes is one of the most rapidly spreading malignant tumours of the skin that can occur at all ages.
- The aetiology is unknown but there is a role of excessive exposure of white skin to sunlight example higher incidence in New Zealand and Australia where sun exposure is high.
- Besides the skin, melanomas may occur at various other sites such as oral and anogenital mucosa, oesophagus, conjunctiva, orbit and leptomeninges.
- The common sites on the skin are the trunk (in men), and legs (in women); other locations are the face, soles, palms and nail beds.
Some high-risk factors associated with increased incidence of malignant melanoma are as under:
- Persistent change in the appearance of a mole.
- Presence of pre-existing naevus (especially dysplastic naevus).
- Family history of melanoma in a patient with an atypical mole.
- Higher age of the patient.
- More than 50 moles 2 mm or more in diameter.
- Molecular studies in familial and hereditary cases have revealed germline mutation in the Cdkn2a gene which encodes for cyclin-dependent kinase inhibitor, activating mutation in Braf, mutational loss of PTEN gene, mutations that turn on telomerase and mutation in several other tumour suppressor genes but not p53.
- Clinically, melanoma often appears as a flat or slightly elevated naevus which has variegated pigmentation, and irregular borders and, of late, has undergone secondary changes of ulceration, bleeding and increase in size. Many of the malignant melanomas, however, arise de novo rather than from a pre-existing naevus.
- Malignant melanoma can be differentiated from benign pigmented lesions by subtle features as summed up by the dermatologists’ terms as ABCD criteria of melanoma (an acronym for Asymmetry, Border irregularity, Colour change and Diameter >6 mm).
Morphologic Features Grossly, depending upon the clinical course and prognosis, cutaneous malignant melanomas are of the following 5 types:
- Lentigo maligna melanoma This often develops from a pre-existing lentigo (a flat naevus characterised by the replacement of the basal layer of the epidermis by naevus cells). It is essentially a malignant melanoma in situ. It is slow-growing and has a good prognosis.
- Superficial spreading melanoma This is a slightly elevated lesion with a variegated colour and ulcerated surface. It often develops from a superficial spreading melanoma in situ (pagetoid melanoma) in 5 to 7 years. The prognosis is worse than for lentigo malignant melanoma.
- Acral lentiginous melanoma occurs more commonly on the soles, palms and mucosal surfaces. The tumour often undergoes ulceration and early metastases. The prognosis is worse than that of superficial spreading melanoma.
- Nodular melanoma This often appears as an elevated and deeply pigmented nodule that grows rapidly and undergoes ulceration. This variant carries the worst prognosis.
- Desmoplastic melanoma In this variant, the tumour has a fibrotic stroma, neural invasion and frequent local recurrences.
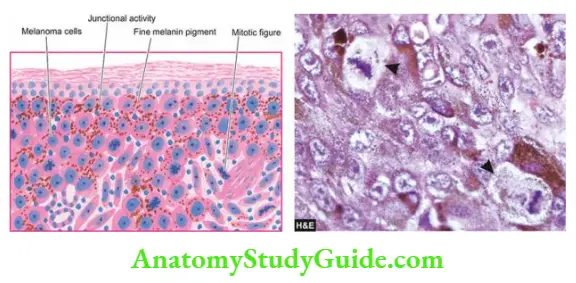
Histologically, irrespective of the type of malignant melanoma, the following characteristics are observed
- Origin: The malignant melanoma, whether arising from a pre-existing naevus or starting de novo, has marked junctional activity at the epidermal-dermal junction and grows downward into the dermis.
- Tumour cells: The malignant melanoma cells are usually larger than the naevus cells. They may be epithelioid or spindle-shaped, the former being more common. The tumour cells have amphophilic cytoplasm and large, pleomorphic nuclei with conspicuous nucleoli.
- Mitotic figures are often present and multinucleate giant cells may occur. These tumour cells may be arranged in various patterns such as solid masses, sheets, islands, alveoli etc.
- Melanin: pigment may be present (melanotic) or absent (amelanotic melanoma) without any prognostic influence. The pigment, if present, tends to be in the form of uniform fine granules (unlike the benign naevi in which coarse irregular clumps of melanin are present).
- At times, there may be no evidence of melanin in H&E stained sections but Fontana Masson stain or dopa reaction reveals melanin granules in the cytoplasm of tumour cells. Immunohistochemically, melanoma cells are positive for HMB-45 (most specific), S-100 and Melan A.
- Inflammatory infiltrate: Some amount of inflammatory infiltrate is present in the invasive melanomas. Infrequently, partial spontaneous regression of the tumour occurs due to the destructive effect of dense inflammatory infiltrate.

Prognosis: In order to determine the prognosis of malignant melanoma, tumour thickness is measured by its depth of invasion into the skin. This is assessed by two types of staging scales: Clark staging and Breslow staging.
Clark staging This was the initial staging system proposed in the 1960s by AJCC staging for malignant melanoma. Clark staging described 5 levels of depth:
Level 1: Malignant melanoma cells confined to the epidermis (melanoma in situ)
Level 2: Invasion into the papillary dermis
Level 3: Invasion to the junction of papillary and reticular dermis
Level 4: Invasion into the reticular dermis
Level 5: Invasion into subcutaneous fat
However, it was subsequently found that Clark staging has lower predictive value and is useful only in superficial melanoma.
Breslow staging: This staging system described in 1970 has better prognostic value than Clark staging. Breslow levels are measured by micrometre on the microscope to know the depth of the tumour; these levels in the original criteria ranged from ≤0.75 mm (stage I) to ≥4 mm (stage 4). In the 2009 AJCC staging system, these levels of thickness of the tumour are further modified as under:
T1:<1.00 mm thickness
T2: 1.01 to 2.00 mm thickness
T3: 2.01 to 4.00 mm thickness
T4: >4.00 mm thickness
In addition to the microscopic depth of invasion of the primary tumour, the AJCC staging system takes into account the number of mitoses, ulceration, nodal metastasis and presence of metastatic disease in internal sites.
Metastatic spread of malignant melanoma is very common and often spreads via lymphatics to the regional lymph nodes and through the blood to distant sites like the lungs, liver, brain, spinal cord, and adrenals. As in breast cancer, sentinel lymph node biopsy is quite helpful in the evaluation of regional nodal status.
Tumours Of The Dermis
All the tissue elements of the dermis such as fibrous tissue, adipose tissue, neural tissue, endothelium and smooth muscle are capable of transforming into benign and malignant tumours.
Many of the examples of these tumours are discussed as soft tissue tumours but a few representative dermal neoplasms are described below.
1. Dermatofibroma And Undifferentiated Pleomorphic Sarcoma:
These soft tissue tumours are composed of cells having mixed features of fibroblasts, myofibroblasts, histiocytes and primitive mesenchymal cells. The histogenesis of these tumours is not quite clear but probably they arise from multidirectional differentiation of the primitive mesenchymal cells.
- The tumours appear at any age but are more common in advanced age. The commonest sites are the lower and upper extremities, followed in decreasing frequency, by abdominal cavity and retroperitoneum.
- The benign variant is also known by various synonyms like dermatofibroma, histiocytoma, sclerosing haemangioma, fibroxanthoma and xanthogranuloma. Benign histiocytomas are often small but undifferentiated pleomorphic sarcoma (earlier called malignant fibrous histiocytoma) may be of enormous size. They are circumscribed but unencapsulated.
Histologically, the tumours are composed of spindle-shaped fibrohistiocytoid cells which are characteristically arranged in a cartwheel or storiform pattern. The benign variety contains uniform spindle-shaped cells with an admixture of numerous foamy histiocytes.
The malignant fibrous histiocytoma shows pleomorphic tumour cells and some multinucleate giant cells in a stroma that may show myxoid change and inflammatory infiltrate.
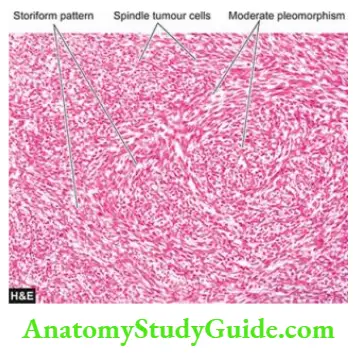
2. Dermatofibrosarcoma Protuberans: This is a low-grade fibrosarcoma that rarely metastasises but is locally recurrent. The tumour usually forms a solid nodule, within the dermis and subcutaneous fat, protruding the epidermis outwards. Sometimes multiple nodules may form.
Histologically, the tumour is very cellular and is composed of uniform fibroblasts arranged in a cartwheel or storiform pattern. A few mitoses are often present. The overlying epidermis is generally thin and stretched and may be ulcerated. The subcutaneous fat is frequently invaded by the tumour cells.
3. Xanthomas: These are solitary or multiple tumour-like lesions, often associated with high levels of serum cholesterol and phospholipids. Many of the cases result from familial hyperlipidaemia. They may occur at different sites such as buttocks, knees, elbows, tendon Achilles, palmar creases and on the eyelids (referred to as xanthelasma).
Histologically, xanthomas are composed of dermal collections of benign-appearing foamy histiocytes. Multinucleate tumour giant cells surrounded by lipid-laden cytoplasm are often present.
Cellular Migrant Tumours
All the tumours described above arise from progenitor cells in the skin only. However, there are some tumours which have their precursor cells elsewhere in the body but are cellular immigrants to the skin. Examples are Langerhans’ cell histiocytosis, mycosis fungoides, mastocytosis, lymphomas and leukaemias. Mycosis fungoides are considered here.
Mycosis fungoides (Cutaneous T-Cell Lymphoma) And Sézary: Syndrome Mycosis Fungoides Or Cutaneous T-Cell Lymphoma (Ctcl) Is The Commonest form of lymphoma in the skin having an indolent course but in an advanced stage, mycosis fungoides may disseminate to the lymph nodes and other organs. Clinically, mycosis fungoides may manifest in 3 stages:
- Premycotic stage: in which the lesions are erythematous, red-brown, scaly and pruritic,
resembling eczema or psoriasis. - The infiltrative stage: has slightly elevated, bluish-red, firm plaques.
- The Fungoid (Tumour) stage: is characterised by red-brown nodules of tumour which often undergo ulceration.
- The aetiology of mycosis fungoides or CTCL has been found to be the same as for adult T cell lymphoma-leukaemia syndrome which is human T cell-leukaemia virus-I (HTLV-1) as discussed.
- Sézary syndrome is a variant of CTCL, often due to the dissemination of underlying CTCL to the blood and infiltration into the skin causing generalised erythroderma, lymphadenopathy and hepatosplenomegaly.
- The condition is found more frequently beyond 4th decade of life. Lesions may affect different body surfaces but often involve the trunk, extremities, face and scalp.
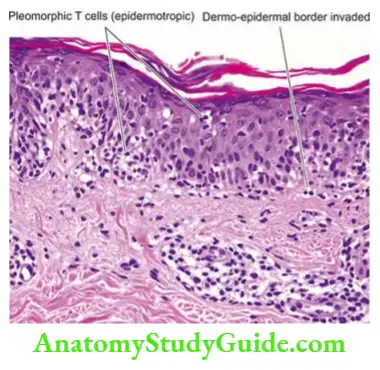
Histologically, the condition has the following characteristics:
- Initially, the lower portion of the epidermis contains hyperchromatic enlarged lymphocytes. In about half the cases, there is the formation of intraepidermal clusters of atypical lymphoid cells forming Darier-Pautrier’s microabscesses which is a misnomer as it does not contain pus cells.
- Later, there are band-like sharply demarcated aggregates of polymorphous cellular infiltrate in the dermis including atypical lymphoid cells (Sézary-Lutzner cells) and multinucleated cells.
- The individual mycosis cells are malignant T lymphocytes which have hyperchromatic and cerebriform nuclei and express CD4 and HLA-DR antigens.
Besides CTCL, other forms of cutaneous lymphomas are adult T cell leukaemia-lymphoma (Atll), anaplastic large cell lymphoma (ALCL), lymphomatoid papulosis and cutaneous B cell lymphoma.
Tumours and Tumour-like Lesions:
- Common examples of benign tumours and cysts of the epidermis are squamous papilloma, seborrheic keratosis, stromal polyps and epithelial cysts (epidermoid, pilar, dermoid).
- A few important premalignant conditions of the epidermis are solar keratosis, Bowen’s disease and xeroderma pigmentosum.
- Squamous cell carcinoma may arise on the skin or squamous mucosa. It may be well differentiated, moderately differentiated or undifferentiated; keratinising or non-keratinising; verrucous or spindle cell type.
- Basal cell carcinoma is a locally invasive, slow-growing tumour of middle-aged that rarely metastasises. It occurs exclusively on hairy skin, most commonly on the face.
- Melanocytic naevus is a benign tumour of melanocytes while malignant melanoma is one of the most rapidly spreading malignant tumours of the skin that can occur at all ages.
- Tumours arising from epidermal adnexa or appendages can differentiate towards hair follicles, sebaceous glands and sweat glands (apocrine and eccrine glands). Adnexal tumours are mostly benign but a few malignant variants also exist.
- Dermis may be the site for certain mesenchymal tumours; common examples are dermatofibroma, undifferentiated pleomorphic sarcoma (malignant fibrous histiocytoma) and dermatofibrosarcoma protuberans.
- Mycosis fungoides or cutaneous T-cell lymphoma (Ctcl) is the T-cell migrant lymphoma in the skin which has an indolent course.
Leave a Reply