Pharmacological Behaviour Management Introduction
Pharmacological management of child behaviour uses pharmacological agents to help children receive efficient dental care. The commonly used agents are sedatives, hypnotics, general anaesthetics, opioids and antihistamines. Though pharmacological modes of management of child behaviour are very effective, they are indicated in certain cases only.
Table of Contents
It requires adequate infrastructure and qualified personnel to administer anaesthesia. Pharmacological methods should never be emphasised over psychological modes of behaviour management. They should never be regarded as a quick solution for handling children who are difficult to manage.
Read And Learn More: Paediatric Dentistry Notes
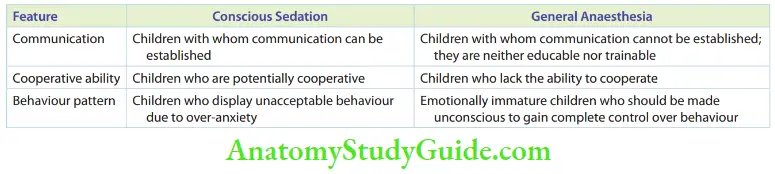
The two modes of pharmacological management are as follows:
- Conscious sedation: To allay the anxiety of children and retain their consciousness while rendering treatment
- General anaesthesia: Bring about a transient loss of consciousness to allow effective treatment
The indications of the two modes of pharmacological management are listed in Table.
Conscious Sedation
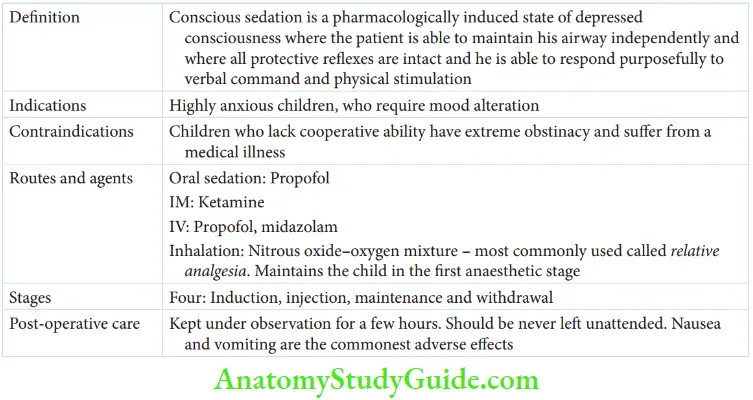
American Academy of Pediatric Dentistry (1993) describes conscious sedation as a pharmacologically induced, state of depressed consciousness where the patient is able to maintain his airway independently, where all protective reflexes are intact, and he is able to respond purposefully to verbal command and physical stimulation.
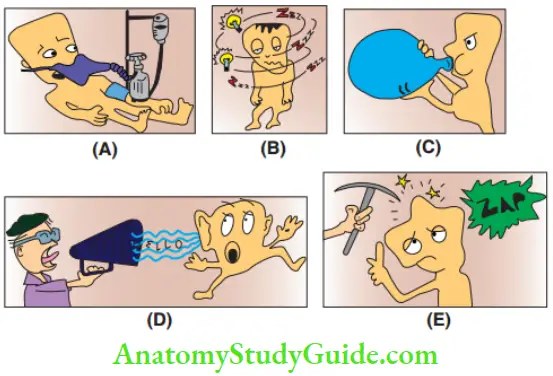
- (A) Pharmacologically induced patient,
- (B) state of depressed consciousness,
- (C) ability to maintain airway,
- (D) the ability to respond to voice and
- (E) ability to respond to physical stimulation.
Conscious sedation alters the mood of an anxious child. It helps in calming the child and elevating the pain threshold.
Indications And Contraindications Conscious sedation is indicated in highly anxious children who can communicate. Such children may have the willingness to cooperate, provided their anxiety is reduced. Conscious sedation is not indicated in the following cases:
-
- Children who lack the ability to listen and follow instructions and respond to a verbal stimulus (cooperative ability), for example intellectually challenged children and very young children.
- Hypermotive, belligerent, obstinate children who do not subdue to behaviour retraining techniques.
- Children suffering from other ailments, such as respiratory distress, neuromuscular illness, bleeding disorders and seizures.
Routes And Agents The pharmacological agent or sedative should have the inherent capacity to establish amnesia while the child is awake. By administering these drugs, the child does not remember anything about the procedure. This helps in developing a positive attitude towards dental treatment.
The sedative used is titrated carefully to maintain the dosage in a stage where the child remains cooperative. It is made sure that the child retains normal vital signs and protective reflexes. The pharmacological agents are administered through oral, intramuscular, intravenous and inhalation routes. The oral route is relatively safer but requires the compliance of the child.
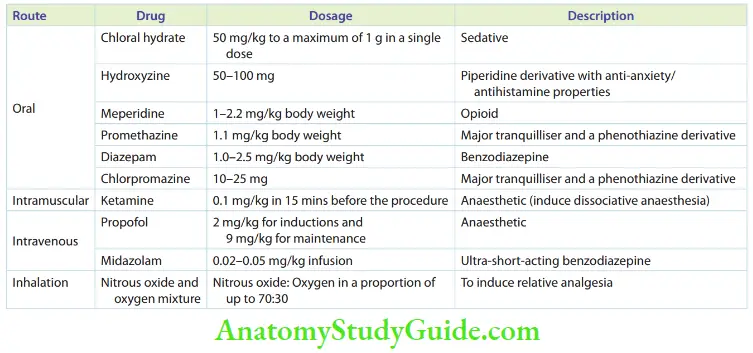
The sedative has to be administered at least an hour before the procedure. Drugs were given intramuscularly in the earlier days to induce dissociative anaesthesia. They are no longer used in paediatric dentistry. Drugs administered through intravenous routes act quickly. They take few seconds to initiate the action and the dosages are best titrated in this route. Inhalation is the route of choice in paediatric dentistry. It is discussed in detail in the following section. The routes of administration of various conscious sedative agents are given in Table.
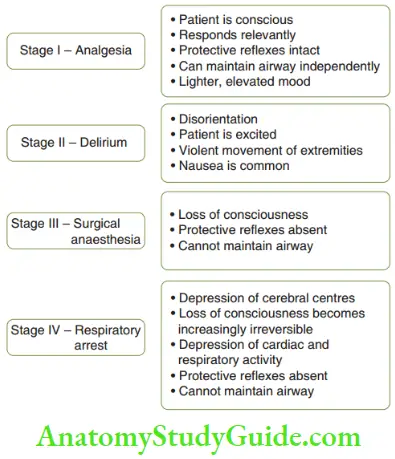
- Relative Analgesia Relative analgesia is produced by inhalation of nitrous oxide–oxygen mixture. It is the most preferred choice of conscious sedation in paediatric dentistry. It is probably the safest method of pharmacologic behaviour management to allay pain and anxiety. Although desflurane and sevoflurane can be used as conscious sedatives through inhalation, a nitrogen dioxide–oxygen mixture is the oldest and the most effective agent. The same mixture acts as an anaesthetic when the percentage of nitrous oxide is increased. the figure shows the stages of anaesthesia. The child is maintained in stage 1 for conscious sedation. The advantages of using a nitrous oxide-oxygen mixture for conscious sedation are as follows:
- Rapid onset of action and rapid withdrawal of the drug to reverse altered consciousness
- Convenient dosage adjustment and titration of the drug to maintain the state of sedation
- High therapeutic index (high relative safety of the drug)
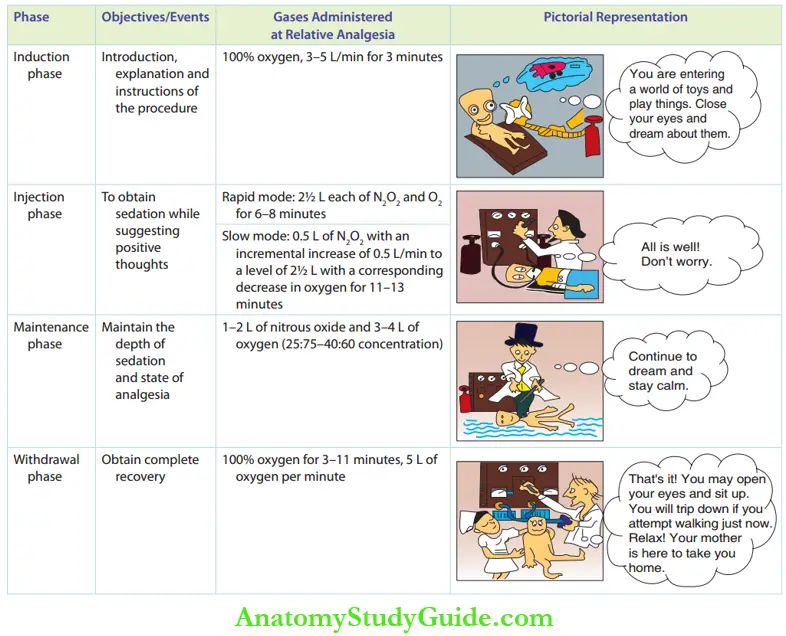
- Phases The administration of nitrous oxide for conscious sedation is divided into four phases, which are given below. A summary of these four phases is given in Table.
- Phases The administration of nitrous oxide for conscious sedation is divided into four phases, which are given below. A summary of these four phases is given in Table.
-
- Induction phase: In this phase, the child is introduced to the nasal hood/mask. The mask can be scented and presented in several shapes or colours for the child to wear willingly. It serves as a mode of distraction. The child is instructed to consciously dream about a world that he/she loves. Boys may think about driving race cars while girls may dream of decorating their Barbie dolls. The child is made aware of experiencing two symptoms, namely light-headedness and tingling sensation with numbness in extremities. The child is directed to enjoy the experience. During induction, 100% oxygen (3–5 L of oxygen per minute) is administered for 3 minutes. During this period, the dentist continuously communicates with the child over an interesting subject. The same questions may also be asked over and over again.
- Injection phase: This phase can be of two types, rapid and slow. 50% of nitrous oxide is the highest anaesthetic concentration preferred in this stage.
- Rapid induction is indicated for children weighing up to 100 pounds (roughly 35 kg). 2½ L of nitrous oxide and 2½ L of oxygen (50:50 concentration) are administered and the sedation is expected to occur in 6–8 minutes.
- For children weighing more than 100 pounds, a slower mode of induction is followed. Initially, 100% oxygen is administered. Then the concentration of nitrous oxide is increased incrementally with a corresponding decrease in the concentration of oxygen. The nitrous oxide infusion is stepped up gradually from 0.5 L/min to 2.5 L/min. With this mode of infusion, it would probably take 11–13 minutes to sedate the child. In this phase, the child slips into a stage of analgesia, where the pain threshold is elevated. The child looks disassociated but will be able to respond to verbal commands purposefully and react to physical stimulation. Communication is still intact. The child is constantly directed to think or dream about pleasant events verbally at intervals. These positive thoughts help the child in getting over negative associations. Communication is maintained throughout this phase.
-
- Maintenance phase: The child is maintained in the state of analgesia/altered consciousness with 1–2 L of nitrous oxide and 3–4 L of oxygen (25:75–40:60 concentrations).
-
- Withdrawal phase: Five minutes before the completion of the procedure, nitrous oxide administration is tapered and 100% oxygen is given for 3–10 minutes. The level is 5 L of oxygen per minute. This 100% oxygen administration can re-oxygenate the system and drive out residual nitrous oxide. The child should be supervised as listed below for adequate recovery.
-
-
- After sedation, the child may look withdrawn, sleepy and unresponsive which is a natural reaction.
- The child is made to sit erect from the supine position for a few minutes before getting down from the dental chair and standing. This is to prevent postural hypotension.
- Children may not feel dizzy initially. However, when they start walking, the resorted motor functions can take up more oxygen. This may lead to hypoxia due to which they may stagger, fall down and get injured.
- A facial crease may be observed over the bridge of the patient’s nose. This is caused by a firm-fitting nasal mask, particularly after a lengthy sedation procedure. It eventually fades away.
-
Precautions
Nausea and vomiting are the commonest untoward symptoms arising after the administration of nitrous oxide. These are best avoided if the child is kept nil-per-oral (NPO) for at least 3 hours before the procedure.
These can be due to over-dosage, prolonged administration, pre-existent gastrointestinal infection, history of motion sickness or an obsolete drug delivery system. Nausea/vomiting requires no specific medication. The child has to be kept in the recovery area for a longer time.
The precautions to be kept in mind are as follows:
- Nitrous oxide sedation must be administered by trained personnel only.
- Informed written consent has to be obtained from the parent.
- An anaesthetist must evaluate the fitness of the patient to undergo the procedure.
- Fail-safe, foolproof equipment that possesses the following features has to be utilised:
- Can never administer 100% nitrous oxide
- Can deliver 100% oxygen with one switch of a lever
- Adequate communication, smooth induction, maintenance with the lowest possible drug concentration and ensuring a complete recovery can make the procedure efficient and safer.
General Anaesthesia
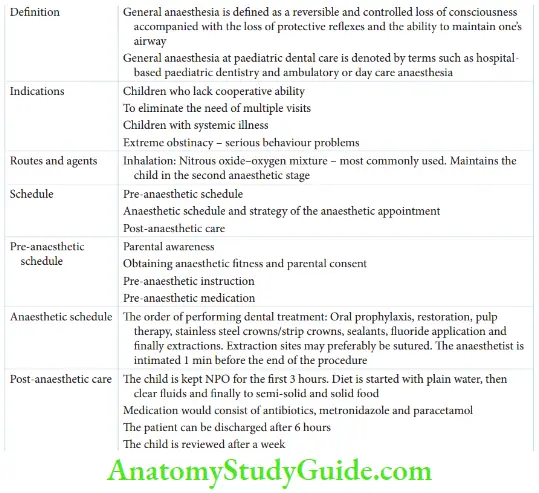
General anaesthesia (GA) is described as a reversible and controlled loss of consciousness accompanied with the loss of protective reflexes and the ability to maintain the airway.
Administration of GA in paediatric dental care can be termed hospital-based paediatric dentistry or ambulatory or daycare anaesthesia. This is because the child requires half-a-day admission and inpatient care with early mobilisation.
Indications Daycare or ambulatory anaesthesia is indicated in the following cases. The figure depicts the indications of ambulatory anaesthesia.
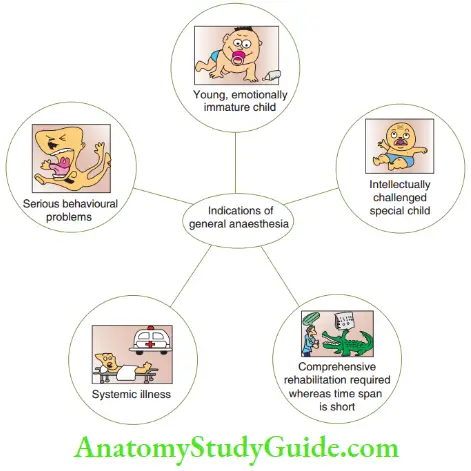
- Very young or emotionally immature children with whom communication cannot be established
- Intellectually challenged children who are neither educable nor trainable
- Children in whom comprehensive dental rehabilitative care is required but parents are unable to comply with multiple visits
- Children with a systemic illness where all the vital signs have to be monitored
- Children with serious behavioural problems are absolutely unwilling to cooperate and do not subdue to psychological behaviour management strategies.
Schedule Daycare ambulatory anaesthesia has three constituent parts, which are as follows:
- Pre-anaesthetic schedule
- Schedule and strategy of the anaesthetic appointment
- Post-anaesthetic care
- Pre-Anaesthetic Schedule
The pre-anaesthetic schedule consists of four steps. These have to be followed very strictly to avoid any medical or legal complications.
- Parental awareness: Parents should be aware of the necessity of GA for their child. The benefits and risks of administering GA, the approximate cost and the need to obtain a fitness assessment have to be explained.
- Obtaining anaesthetist fitness and parental consent: The child is referred to an anaesthetist to obtain anaesthesia fitness consent. When the anaesthetist declares the child fi to undergo the procedure under GA, written parental consent has to be obtained.
- Pre-anaesthetic instructions: The child is instructed to be kept strictly NPO for at least 6 hours before the procedure. The child should not be overfed during the last meal. The parents are asked to comply with pre-anaesthetic medication.
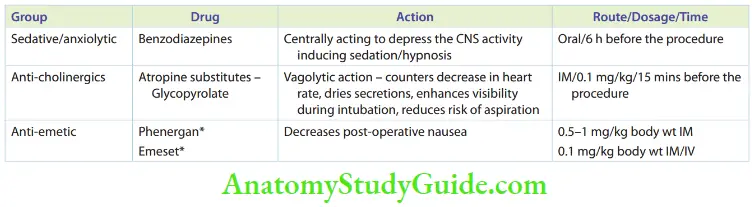
- Pre-anaesthetic medication: The prescription is given by the anaesthetist. It consists of the drugs given in Table.
- Schedule And Strategy Of The Anaesthetic Appointment The anaesthetic appointment consists of a series of steps which when systematically adopted ensure the efficacy and efficiency of the treatment modality. Adequate depth of local anaesthesia is highly essential during treatment. It also ensures no waste of time. The steps to be followed are given below:
- The child is brought into the theatre by the parent. The parent may be allowed to stay in till the induction phase. This is to allay stranger anxiety.
- The anaesthetist establishes the venous route and induces the anaesthesia with an ultra-short-acting barbiturate – thiopentone sodium. The ultrashort-acting drug anaesthetises the patient within 5–12 seconds. Rapidly induced anaesthesia is obtained. Within the next few minutes, the anaesthetic intubates the child (nasal intubation) and starts with nitrous oxide-oxygen anaesthetic mixture inhalation. This maintains the rapidly induced anaesthesia.
- The pulse oximeter is connected to monitor vital signs. Muscle relaxants are also administrated.
- The patient is routed over to the paediatric dental team.
- An ideal order for performing the treatment is oral prophylaxis, restoration, pulp therapy, stainless steel crowns/strip crowns, sealants, fluoride application and finally extractions.
- Extraction sites may preferably be sutured.
- The anaesthetist is intimated 10 minutes before the end of the procedure.
- Loose fragments of restorative materials and cotton pledgets, which could inadvertently be swallowed or aspirated during withdrawal, are wiped of the oral cavity.
- The patient is taken over by the anaesthetist. He reverses the anaesthesia/sedation administration of 100% oxygen for a few minutes and extubates the patient.
- The patient is then shifted to the recovery room and observed for complete recovery.
- Post-Anaesthetic Care Post-anaesthetic care ensures the safe and quick recovery of the child from the anaesthetic appointment. It also facilitates a quicker discharge of the child. The following steps have to be followed:
- The child is kept NPO for the first 3 hours after recovery.
- Diet is started with plain water followed by clear flids, semi-solid and solid food.
- Diffuse oedema of perioral musculature can be expected, especially with longer procedures. This needs no medication. It is expected to dissipate spontaneously with time. Parental reassurance is required.
- Post-operative medication is essential for dental focal sepsis. Medication consists of antibiotics (amoxicillin 20–45 mg) in three divided doses – metronidazole 5 mg/kg thrice a day and paracetamol 15 mg/kg four times a day.
- The patient can be discharged after 6 hours. However, as per the anaesthetist’s opinion, some children would require an overnight hospital stay.
The child is reviewed after a week.
Summary
- Pharmacological means of behaviour management pertain to the use of pharmacological agents (sedatives, hypnotics and general anaesthetics). Conscious sedation and general anaesthesia are two types:
- Conscious sedation
- General anaesthesia (daycare or ambulatory anaesthesia)
- Conscious sedation
- Pharmacological modes are effective methods but need to be advised for indicated cases and are not to be used as a quick-fix solution for ‘difficult children’.
Leave a Reply