Pit And Fissure Sealants Introduction
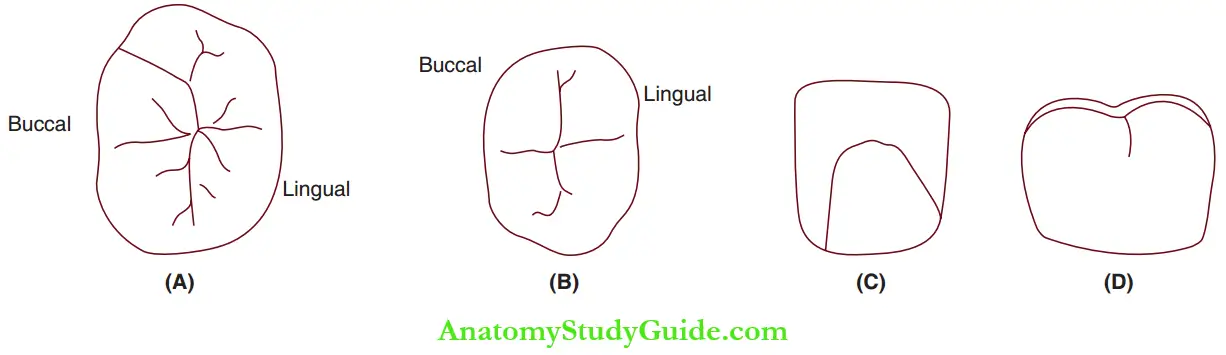
Dental caries can be classified as pit and fissure caries and smooth surface caries. While smooth surface caries are found on the proximal surfaces, pit and fissure caries can occur in the following surfaces of teeth:
Table of Contents
Read And Learn More: Paediatric Dentistry Notes
1. (A) Occlusal surfaces of molars,
2. (B) occlusal surfaces of premolars,
3. (C) palatal surfaces of incisors and
4. (D) buccal surfaces of molars.
- Occlusal surfaces ofmolars and premolars
- Palatal surfaces ofincisors
- Occlusal onethird of buccal/lingual (palatal) surfaces of molars as buccal/lingual (palatal) grooves ending in pits
The pits and fissures on tooth surfaces are usually inaccessible to mechanical cleansing action. They have the capacity to allow stagnation of food debris and bacterial growth due to their morphology. Primary prevention of dental caries is essential for health promotion and specific protection.
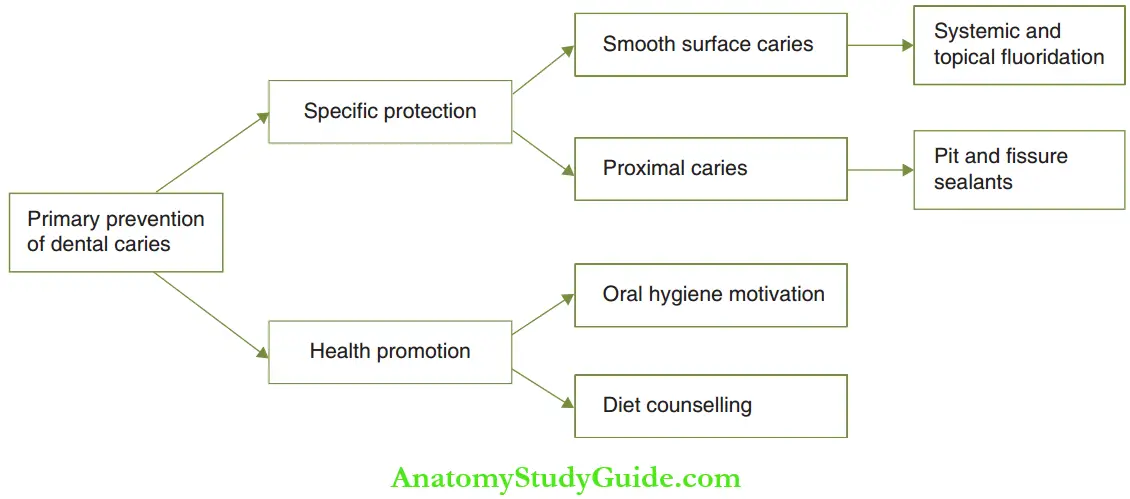
Water fluoridation (systemic fluoridation) and topical fluoridation are modes of specific protection of dental caries. These modes have reduced the prevalence of dental caries by 60%. But much of this reduction pertains to a decrease in smooth surface decay. The modes of specific protection of pit and fissure caries are pit and fissure sealants.
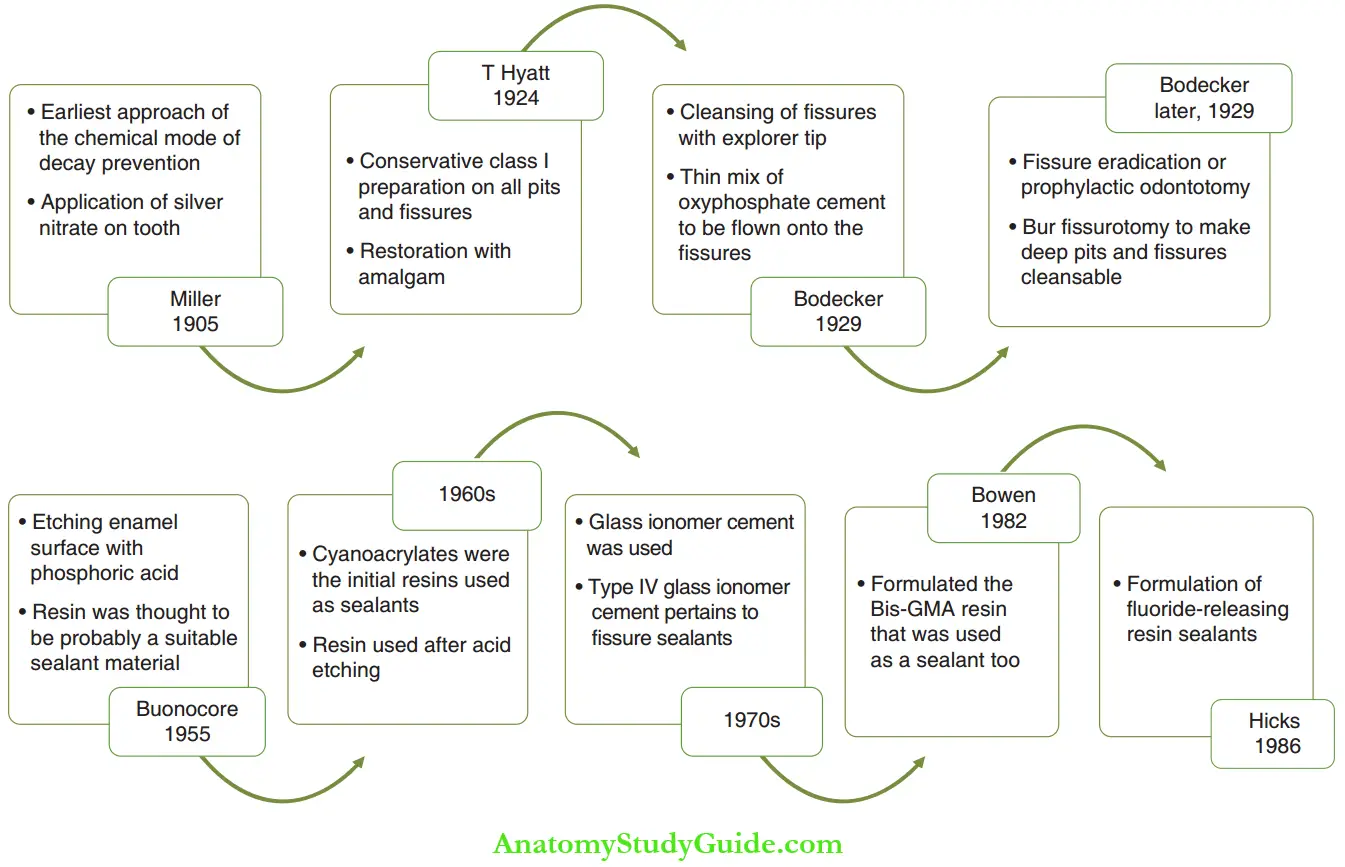
Pit and fissure sealants have been developed to prevent caries in pits and fissures as described by Gordon. These sealants obliterate the occlusal fissures and remove the sheltered environment in which dental caries may thrive. The history of it and fissure sealants is depicted in Figure.
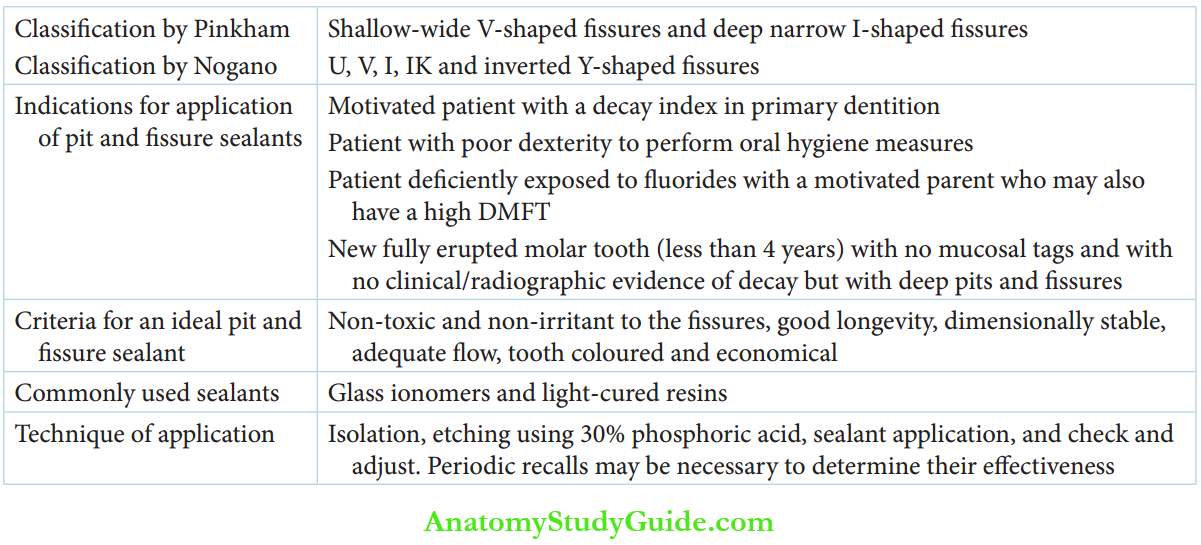
- Classification Pinkham classified fissures into two types:
- Shallow, wide, Vshaped fissures
- Deep, narrow, Ishaped fissures
I-shaped fissures are more prone to decay due to their narrow configuration and low oxygen tension. The pits and fissures get involved quickly due to the decreased thickness of enamel in these areas. They receive minimum protection from fluoride.
Fissures were more comprehensively classified by Nogano in 1961 on the basis of leisure morphology. This classification is as follows:
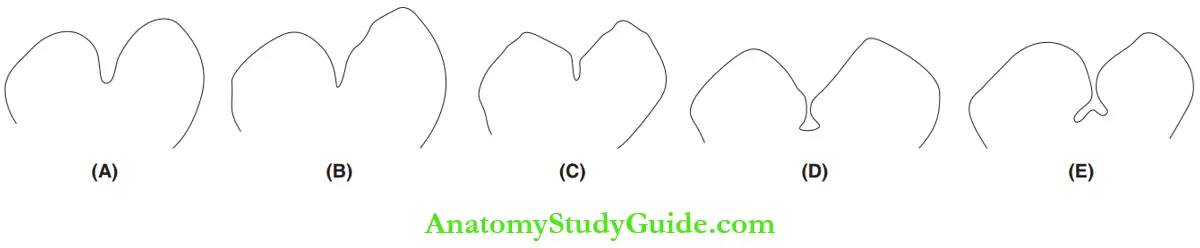
- U Type: The figure has the same width at both the entrance and the base with no narrowing along the length.
- V Type: The fissure is wide at the entry and narrows at the base forming a ‘v’ shape.
- I Type: The figure is extremely narrow at both the entry and the base. It resembles the shape of a long, narrow tube.
- IK Type: The figure has an extremely narrow entry slit and a wide base.
- Inverted Y Type: The figure has an extremely narrow slit with a bifurcation at the base resembling the shape of an inverted ‘Y’.
The ‘U’ type is relatively fewer caries conducive owing to its selfcleansable shape. The I type, IK type, and inverted Y type are highly caries-prone as they are inaccessible to a toothbrush bristle and are thus non–selfcleansable.
Case Selection
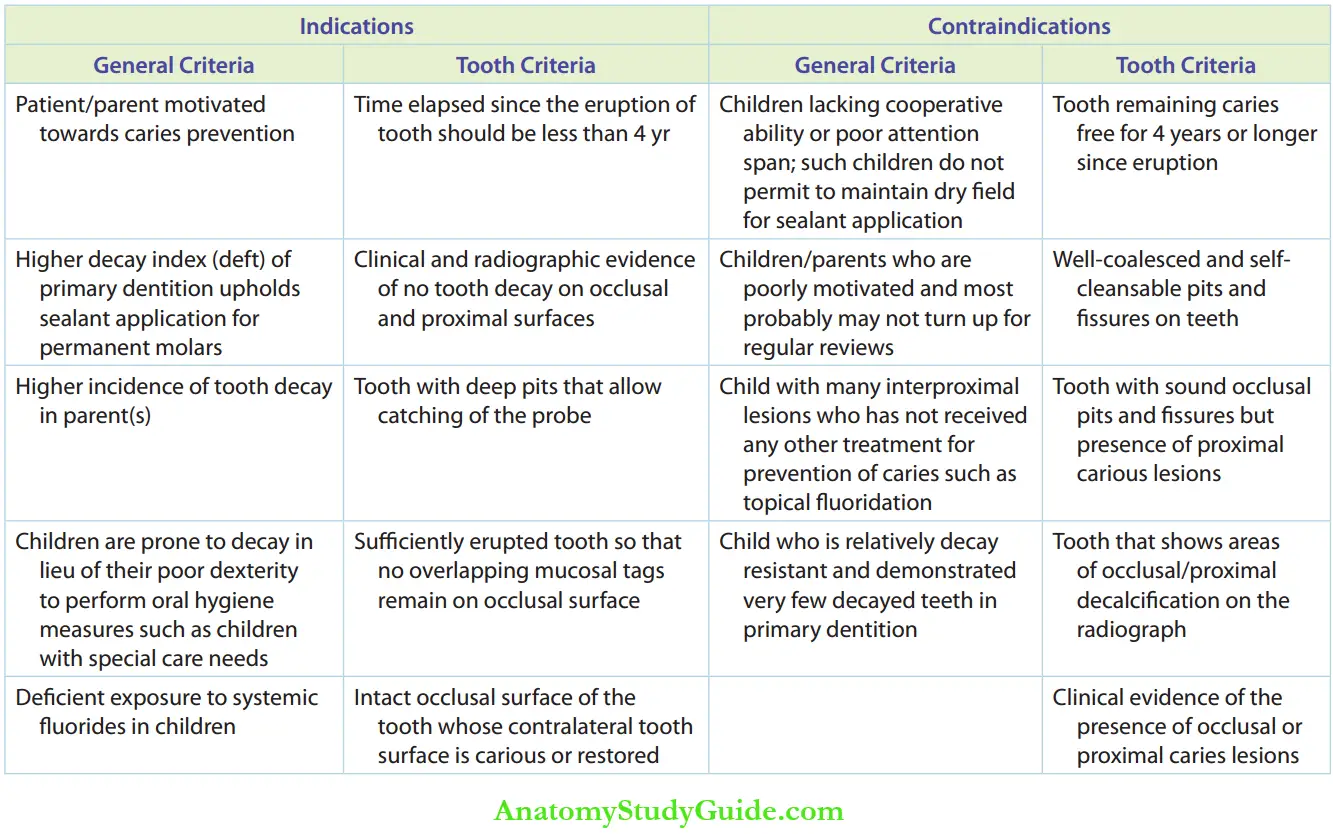
A successful outcome depends on the proper selection of case. Accurate diagnosis is important before sealant application. The application of pit and fissure sealants depends upon general factors and toothrelated factors. Factors such as the general condition of the patient, life expectancy of the tooth, and cooperation of the patient should be evaluated before selecting the case for pit and fissure sealant application.
The table lists the factors that determine the indications and contraindications of sealant application.
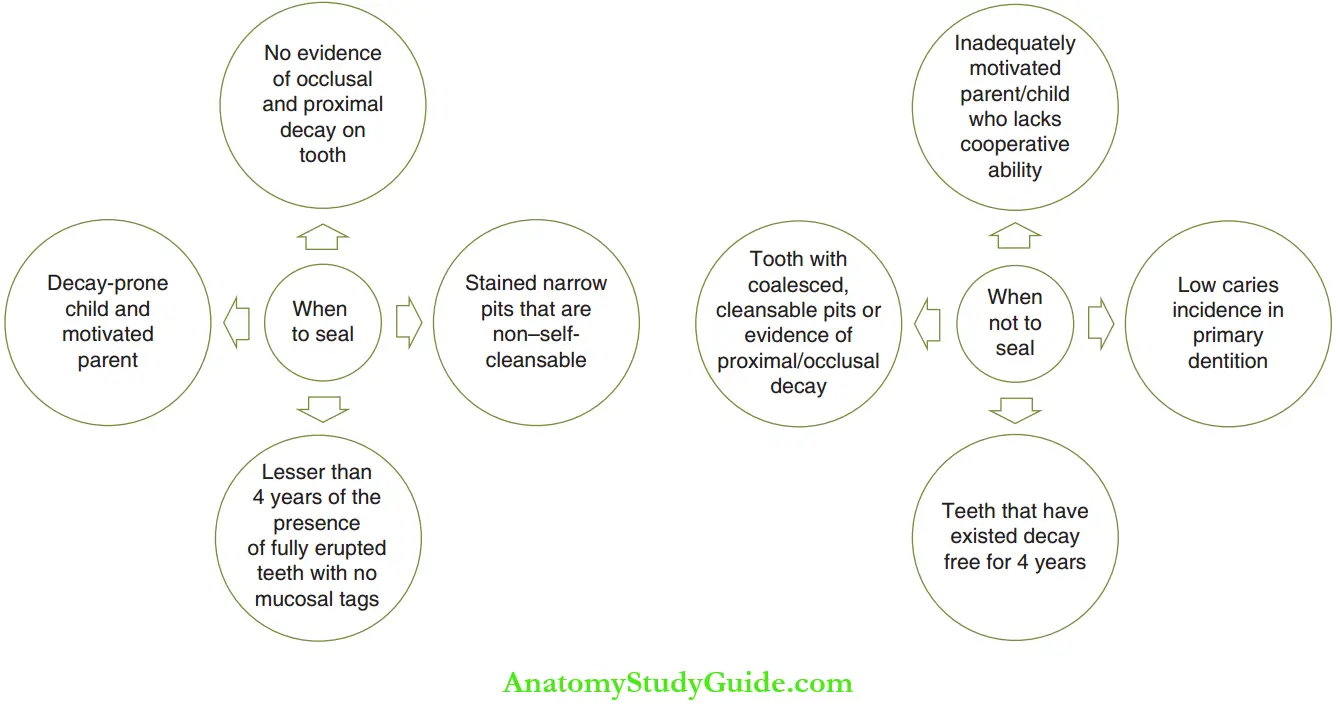
The figure summarises when to apply a sealant and when sealants are not advised in the endodontic practice.
- Requirements An ideal sealant should meet the following requisites:
- The sealant should be nontoxic and nonirritant to the fissures.
- A thin layer of sealant must be able to adhere to the tooth surface.
- The sealant should have a longer shelf life.
- The material should not be sensitive to temperature changes.
- The viscosity of the sealant should be such that it flows easily into the areas of pits and fissures.
- The properties of the sealant after polymerization should be adequate to withstand masticatory stresses.
- Shrinkage should be minimal to avoid marginal leakage.
- Water absorption after polymerization should be as low as possible to assure resistance to displacement and discoloration.
- The sealant should be aesthetically harmonious to the tooth structure.
- The sealant should be economical.
Sealant Materials And Application Techniques
Initially, cyanoacrylates were introduced as sealants. But these materials were not suitable as sealants owing to bacterial degradation of the material in the oral cavity. Currently, the BisGMA system is the material of choice. In this system, auto polymerising sealants, visible light cure, and ultraviolet light cure materials are available. Apart from these, cement such as glass ionomer and polycarboxylate are also used as sealants. Fluoride was also added to resin sealants due to its anticariogenic effect.
Autopolymerising sealants are not used in practice today due to disadvantages such as shorter working time, low wear resistance, and setting time that cannot be controlled. UV lightbased materials are also unavailable and obsolete now. The following three materials are the sealants of choice in the current practice:
- Light-cure resin systems: A visible lightactivated system contains urethane methacrylate as the main component and diketone as the initiator. It provides sufficient working time and the sealant surface can be carved for a longer time and a smoother surface can be achieved with greater compressive strength. Nowadays, colored resins are available such as yellow and white. Titanium dioxide is added to give the resin a brilliant white color.
- Glass ionomer cement (GIC) and polycarboxylate cement: The development of these cement has raised the possibility of direct chemical bonding to dentin and anticariogenicity. They are due to decreased microleakage and slow release of fluorides from the cement, respectively. These are the advantages of GIC over resinbased cement. However, resinbased sealants have better abrasion resistance.
- Resin with fluoride: The addition of fluorides to sealants is another approach. Fluoride from the resin leaches out to be taken up by enamel during its period of contact with the tooth. This provides protection against caries even if the sealant is lost.
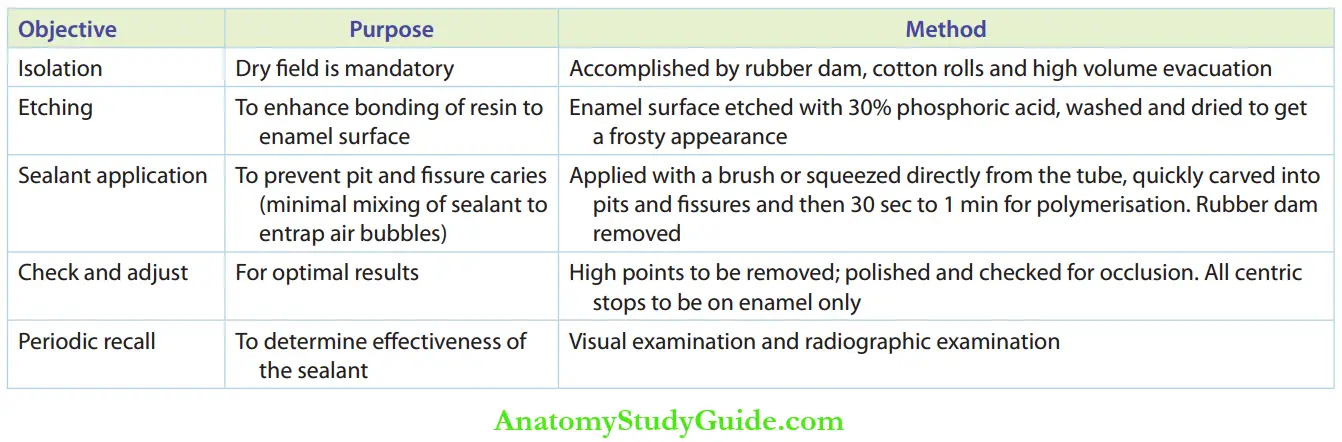
- Technique A clear tooth surface is essential for proper binding of the sealant irrespective of the type of sealant used – resin or GI based. The tooth surface should be polished with pumice and water, washed, and dried before sealant application. The table shows the steps involved in sealant application on the tooth surface.
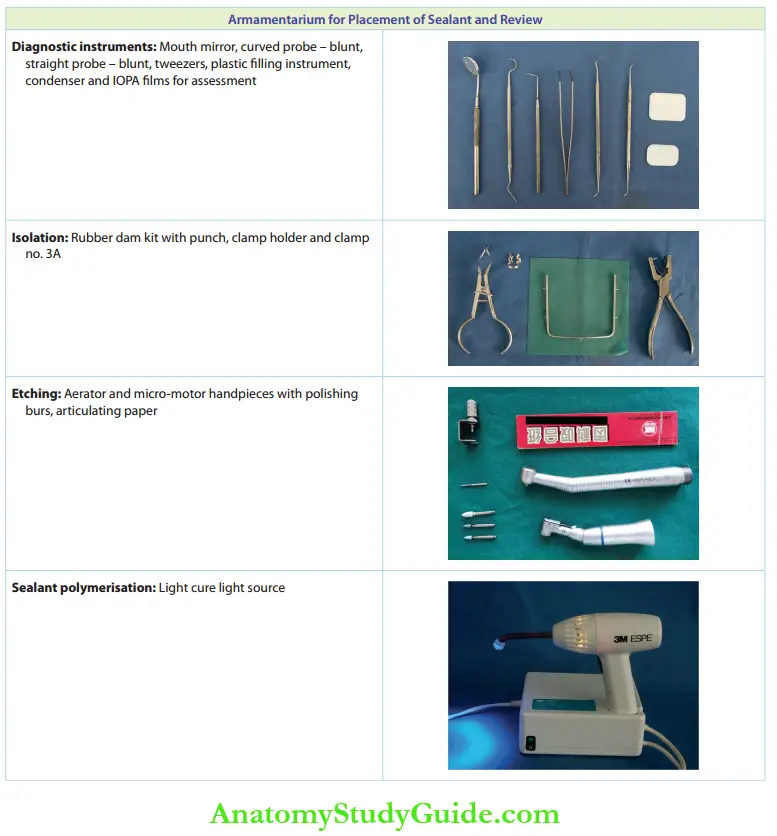
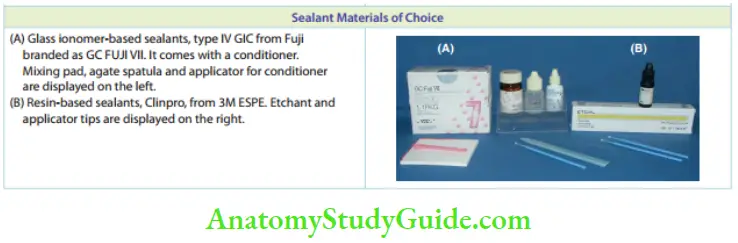
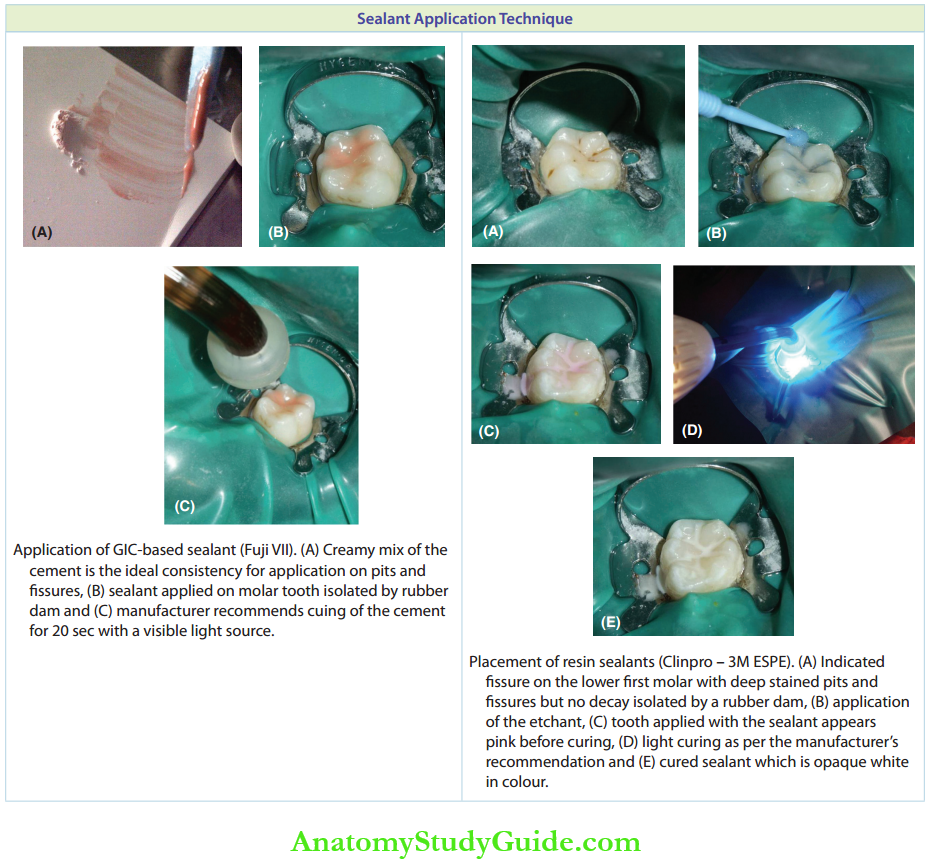
The table depicts the clinical pictures of the armamentarium for placement of sealant and review, choice of sealant material, and appropriate application techniques.
Sometimes, an abrasive air-polishing prophylactic device can be used in the procedure. It produces air, water, NaHCO4, and CaPO4 to remove plaque and stains from teeth. This prevents tissues from getting filled with pumice material. Some clinicians have advocated the vibration etching technique, achieved by an electromagnetic vibrator. This is claimed to completely clear the fissures up to 100 -150 µm allowing the sealants to penetrate easily.
- Atraumatic Restorative Technique/Alternative Restorative Technique
The atraumatic restorative technique (ART) was a minimal intervention technique developed in the mid1980 in Tanzania. It was primarily developed for community fildtreatmentin populations with high decay prevalence but inadequate dental treatment facilities. In 1994, this technique was introduced into clinical practice by Frencken et al.
ART is a mode of minimal invasion and minimal cavity preparation done in carious teeth and noncarious and susceptible pits and fissures. This technique uses no rotary instruments. The armamentarium for the procedure includes hand instruments such as enamel hatchets, spoon excavators, and plastic filing instruments, and condensers. Direct bonding adhesive cement is the restorative/sealant material used.
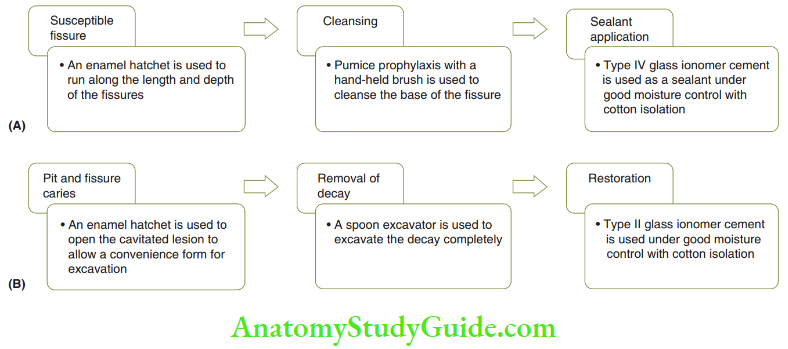
The technique involves the following steps which are depicted in Figure.
Retentivity And Failures (Loss) Of Sealants
Retention of sealants in pits and fissures is influenced by the following factors:
- Maximum surface area: The higher the surface area of contact between the sealant and the tooth surface, the higher the retentivity of the sealant. U-type and V-type fissures have enhanced retentivity when compared to the other types of figures.
- Deep pits and fissures: The flow of the sealant to the base of the figure is decreased when the fissure is deep. This may decrease the retentivity of the sealant.
- Clean and dry surface: A surface free of debris, plaque, and moisture and a smear layer is highly essential for bonding the sealant to the tooth surface.
- Adequate acid etching: Adequate etching enhances the bond strength ofmicromechanical bonding.
- Adequate polymerization: Insufficient curing can lead to loss of sealant. To avoid this, sealants can be added in increments in deep I, IK, and inverted Yshaped fissures.
Sealant failure depends on the morphology of teeth. For example, sealant application on mandibular molars is more prone to failure. This is because an oblique ridge that is present in maxillary molars is absent in mandibular molars.
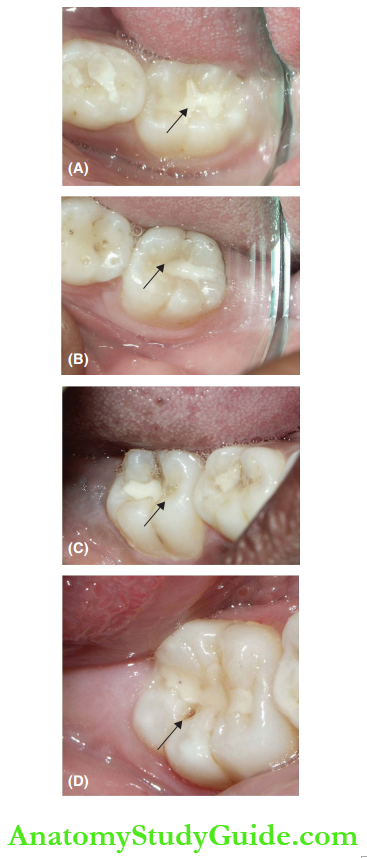
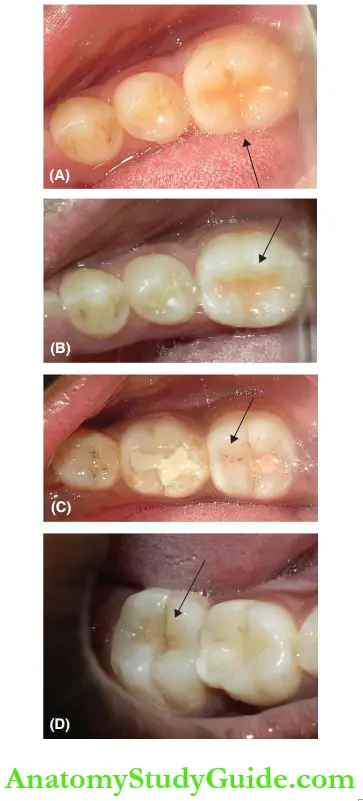
1. (A) sealant totally retentive,
2. (B) sealant minimally lost (indicated by the arrow),
3. (C) sealant partially (almost half) lost and
4. (D) total loss of sealant and ensuing dental caries lesion
The pit and fissure sealants were applied to 100 children as part of a schoolbased preventive health care program. The figure shows clinical pictures indicating various stages of resin pit and fissure sealant retention after 30 months of application. The figure shows various stages of glass ionomer pit and fissure sealant retention after 30 months of application
- (A) sealant totally retentive,
- (B) sealant minimally lost,
- (C) sealant partially (almost half) lost and
- (D) sealant totally lost.
- Retentivity And Failures (Loss) Of Sealants Advantages and disadvantages Pit and fissure sealants have been proven to be effective if used properly by the operator. The advantages and disadvantages of applying pit and fissure sealants are listed.
- Effectiveness Of The Pit And Fissure Sealant Effectiveness and durability depend upon the retention and marginal integrity of the pit and fissure sealants. They are being continuously improved and developed, and superior results are expected from the use of newer pit and fissure sealants than the older ones. At present, at least 85 sealants are completely retentive out of 100 sealants applied at the end of 1 year and 50 sealants are retentive out of 100 at the end of 5 years. Effectiveness can be enhanced by reapplication of the pit and fissure sealant if the review indicates a defect or partial loss of sealant. Hence, regular reviewing is essential.
Deficiency (partial loss) or total loss can be detected by visual inspection upon drying the tooth and by tactile inspection using a blunt end probe. Colored pit and fissure sealants are advantageous as they can be visually detected easily for their complete/partial loss. The applied pit and fissure sealants should be evaluated every 6 months. They should be reapplied, lost
- Advantages and Disadvantages of Pit and Fissure Sealant Application
- Pit and Fissure Sealant Application Advantages
-
-
- Most effective in preventing occlusal caries
- Less discomfort to the patient
- Less fear and anxiety anticipated from the patient
- The tooth is not cut and weakened as it happens in conventional
- cavity preparation
- Sealant can be easily added and replaced if necessary
- No adverse effects on the patient
- Reduces caries up to 85% along with fluoride therapy
- Has better esthetics
- Cost-effective when the cost of treatment of a decayed tooth is considered
- Saves time for both the patient and the operator
- Gives self-esteem of having a caries-free mouth
-
- Pit and Fissure Sealant Application Disadvantages
- Highly technique sensitive
- Long-term retention and benefits over conventional restorations are yet to be determined
- Patient motivation towards the review of sealant is sometimes unrewarding
According to Gordon, the dentist should be encouraged to adopt the maxim ‘when in doubt, seal’ rather than ‘when in doubt fil’. There is abundant evidence about the benefits of applying pit and fissure sealants. Hence, it is an acceptable preventive procedure. Application of pit and fissure sealants has shown reduced bacterial count in pits and fissures, thus preventing the progress of caries. Sealants are effective in communities, both with and without fluoridated water.
The avoidance of restoration and subsequent weakening of the tooth that occurs with it point to the usefulness of the sealant. No systemic toxicity has been reported, and the vitality of pulp and dentin is also not endangered. Educational materials should be developed to expand the use of pit and fissure sealants in endodontic practice. This would substantially reduce the incidence of dental caries beyond what is already achieved by fluorides and other preventive measures.
This would reduce the expenditure required for the treatment of caries and also improve the health of the public.
Pit and Fissure Sealant Application Summary
- Occlusal caries remain a significant problem, and fluoride benefits in these pits and fissures are not great as compared to interproximal surfaces. Pit and fissure sealants offer a solution to the prevention of fissure caries.
- Selection of the case: A successful outcome depends on the proper selection of the case.
- There is abundant evidence of their clear benefits; hence, it is an acceptable preventive procedure. Sealants have shown a reduced bacterial count in pits and fissures to prevent the progress of caries.
- Sealants are effective in communities, both with and without fluoridated water.
Leave a Reply