Exodonti Introduction
Exodontia or extraction of teeth in pediatric dentistry is special due to the morphology of primary teeth and the presence of developing permanent teeth beneath them.
Table of Contents
Extraction of primary teeth can be avoided by all means as they are the ideal space maintainers and can be best preserved till natural exfoliation.
Indications
Extraction of a primary tooth is sought in the following conditions:
1. Primary teeth that are contraindicated for endodontic therapy due to:
- Poor storability of tooth structure with gross caries involvement
- Dental caries beyond the gingiva
- Associated periradicular lesion
- The poor motivation of the parent
Read And Learn More: Paediatric Dentistry Notes
2. Retained deciduous teeth: Primary tooth retained even after the permanent tooth is clinically visible
3. Fractured and extremely: mobile teeth with a poor prognosis on immobilization.
Contraindications
There are no absolute contraindications for the extraction of primary teeth.
A strategically important primary tooth with irreversible pulpal lesion and acceptable storability is a contraindication to extraction.
Extraction is considered in such cases due to poor parent motivation.
Systemic illness such as hemophilia and leukemia restrains choosing extraction as a treatment option on an indicated tooth.
In these cases, extraction can be carried out only with the physician’s assessment and subsequent consent.
Protocol Of Uncomplicated Extraction
The extraction protocol consists of the following:
- Awareness, consent, and pre-operative assessment
- Operative technique
- Post-operative instructions
Each parameter is discussed separately.
Awareness, Consent, And Pre-Operative Assessment
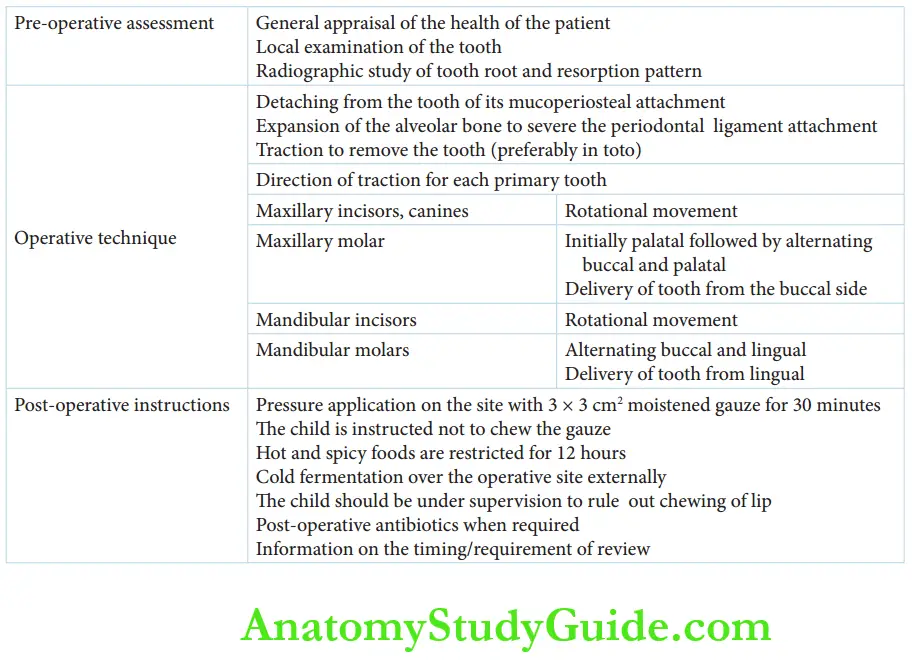
The pre-operative assessment includes the general appraisal of the child, local clinical examination, and radiographic examination.
1. General appraisal of the child: The general health of the child is examined.
Any medical concern requires a referral to the concerned physician to obtain a fitness for the procedure.
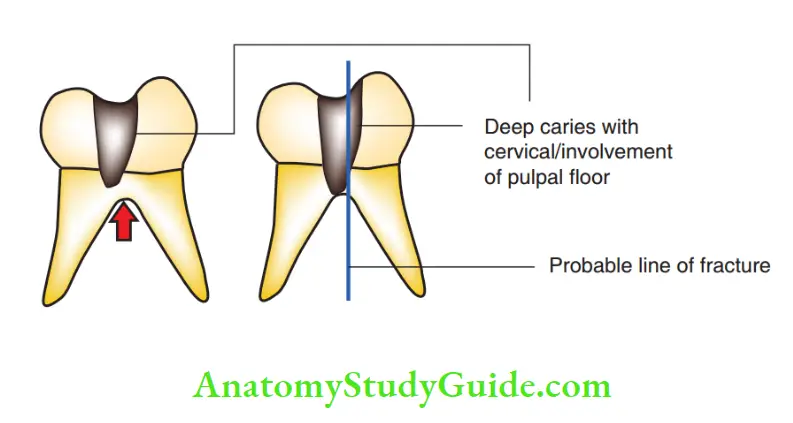
2. Local clinical examination of the tooth: This helps to assess the extent of carious involvement in a decayed tooth, the line of fracture in a fractured tooth, and the extent of the mobility of the retained deciduous tooth.
3. Radiographic examination: This reveals the resorption pattern and percentage of root resorption.
Parents have to be made aware of the existing dental ailment his/her child is suffering from, the possible modes of treatment, and the reason for choosing extraction as the treatment mode.
The necessity of subsequent space maintenance has to be communicated.
Verbal/written consent has to be obtained before the extraction.
Operative Technique
An extraction procedure can be simplified into three basic steps:
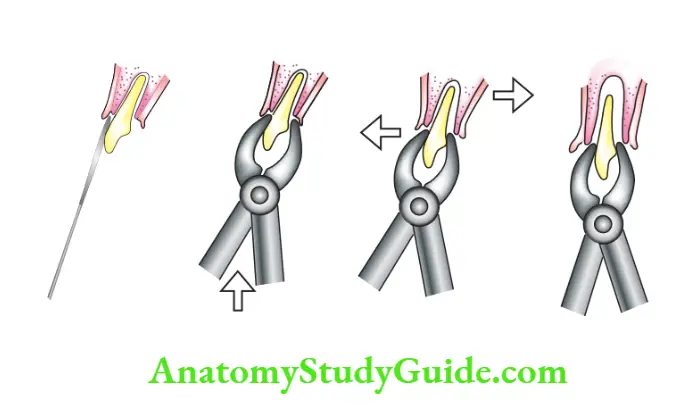
Step 1: Detaching the tooth of its mucoperiosteal attachment Detaching the mucoperiosteal attachment has to be done with the spoon end of a smaller periosteal elevator. Larger-sized instruments can cause undue trauma to the soft tissues.
Step 2: Guided expansion of the alveolar bone with adequate support to sever the periodontal ligament attachment The narrower end of the elevator is used at the mesiobuccal, middle, and distobuccal points of the cervical line of the tooth to luxate the tooth.
It is based on the lever principle using the (interdental) alveolar bone as the fulcrum. This expands the bone to sever the periodontal ligament attachment.
The primary alveolar bone is extremely pliable and expands under minimal pressure.
Step 2 is completed when the tooth is luxated to demonstrate clinical mobility.
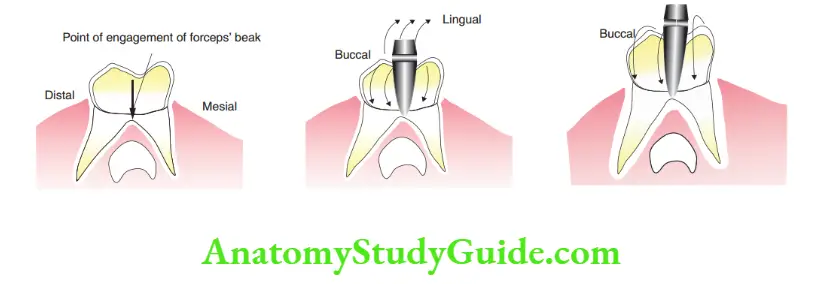
Step 3: Precise traction to remove the tooth with support to the alveolar bone (preferably in toto) A pedodontics extraction forceps can be used to deliver a gentle, yet firm grasp on the tooth.
While grasping, the alveolar bone (maxillary arch) or jaw bone (mandibular arch) should be supported with the thumb and the index finger of the non-working hand.
This support can prevent the delivery of undue pressure and can help feel the distension of the socket wall.
An apical pressure is delivered to expand the socket as per the wedge principle.
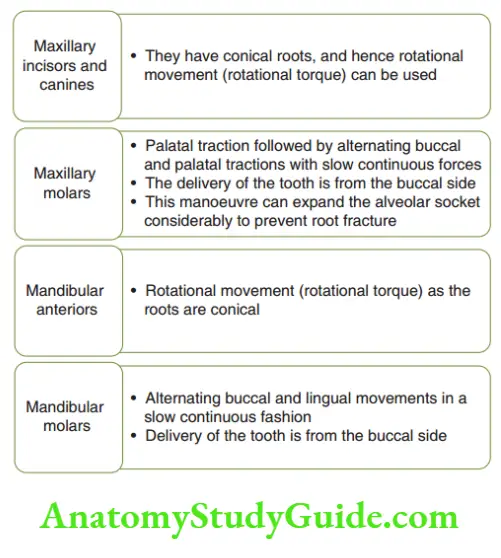
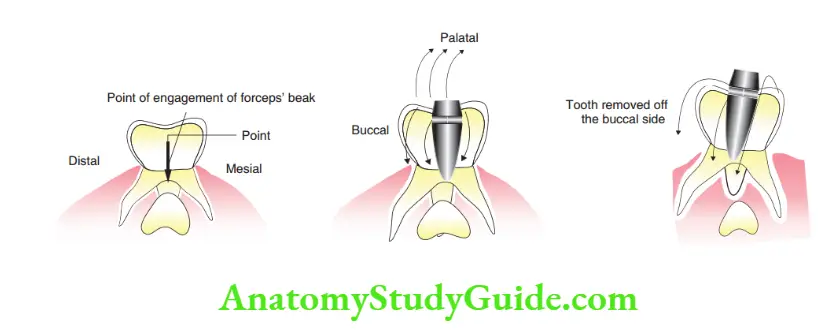
The forceps are then used to deliver traction (which is specific for each tooth) to remove the tooth.
The traction is delivered with the wrist force only. Gives the direction of friction to be applied to a specific tooth.
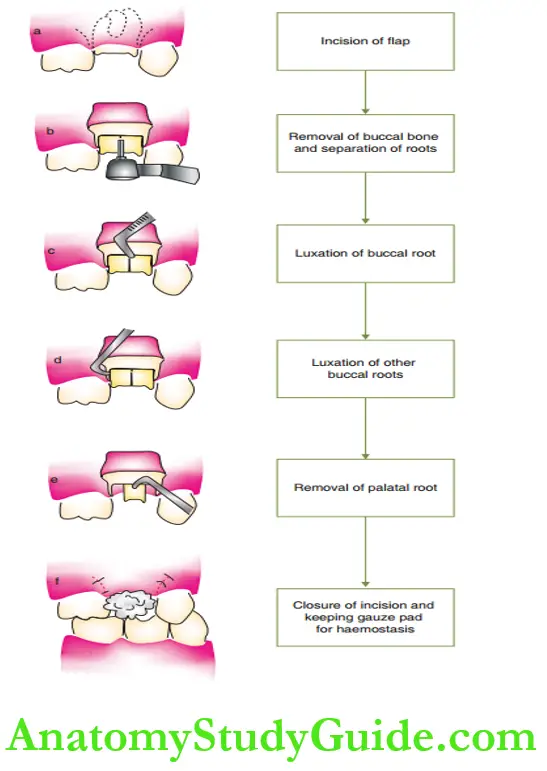
In multirooted teeth (molars), there is a risk of root fracture or dislodgement of the entangled premolar tooth bud (discussed later).
In such a case, the tooth to be extracted is surgically split into two fragments.
The split tooth fragments are extracted using root forceps.
Customizing adult forceps for extracting a primary tooth is absolutely unacceptable.
The beaks of adult forceps do not adapt well to the anatomy of the primary tooth.
They are disproportionate to the small oral cavity.
This may cause undue soft-tissue trauma, excessive traction in an undesired direction, and trauma to adjacent teeth as well.
A cow-horn mandibular forceps is strictly contraindicated as it can, most probably, cause trauma to the erupting premolar both buds.
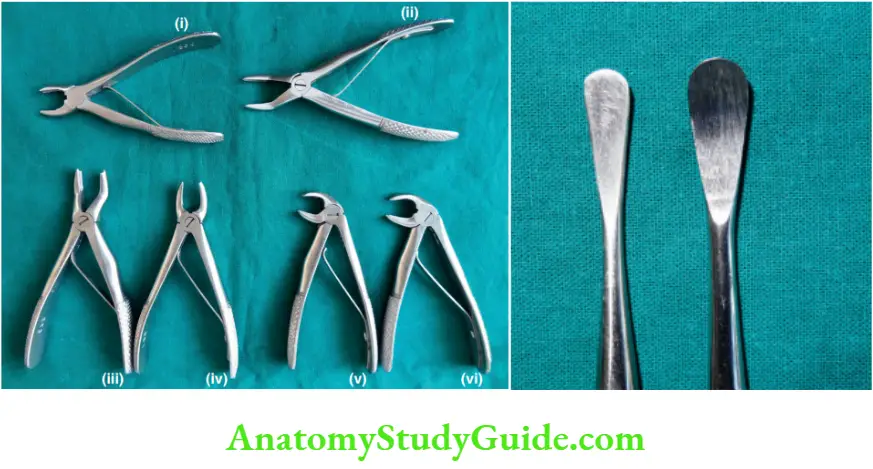
The armamentarium required for the extraction of primary teeth is depicted.
The procedure of extraction of primary teeth.
- Extraction of primary anterior tooth
- Extraction of primary maxillary molar
- Extraction of primary mandibular molar
Post-Operative Instructions
The following post-operative instructions are given after the extraction procedure
1. 3 × 3 cm 2 moistened gauze is kept over the extracted socket. The child is asked to bite over the gauze with optimal pressure for 30 minutes. The child is instructed not to chew the gauze.
2. Hot and spicy foods are restricted for 12 hours because they enhance blood supply and can lead to clot dissolution.
3. Cold fermentation is advised over the operative site externally. This enhances homeostasis and brings down the possibility of post-operative edema.
4. The child is under direct supervision to rule out chewing of lip and scratching of cheeks as the anesthesia effect is persistent.
5. Post-operative antibiotics are prescribed when the extracted tooth is septic foci.
The antibiotic of choice is a combination of amoxicillin and cloxacillin in a dose of 20–40 mg/kg body weight in three divided
doses for 3–5 days.
6. If the extracted tooth had a dentoalveolar abscess, metronidazole 5 mg/kg body weight is added thrice a day.
Painkillers or anti-inflammatory drugs are usually unnecessary.
7. An antibiotic/antimicrobial prescription is highly essential following a traumatic extraction as it is tagged with the risk of a dry socket.
8. Information on time and requirements of post-operative review have to be specifically emphasized.
An uncomplicated extraction may be reviewed on the third day. A complicated extraction may be reviewed on the first and third
day.
The first-day review is to check the level of post-operative discomfort and to prevent the possibility of re-infection.
The third-day review should show uneventful and appreciable healing of the socket.
Dry Socket
When a clot formed in the extraction socket is large or poorly supported, it may be lost with inappropriate mechanical stimulation or due to secondary infection.
This leads to a socket devoid of the clot, thus exposing a raw, bony surface.
The surface may also be necrosed. Such a condition is highly tender and is called a ‘dry socket’.
If a dry socket is encountered during the review of the extraction site, it is inspected for necrosed bony fragments.
Necrosed fragments are usually loose and can be picked out with artery forceps.
After the removal of the fragments, the raw bony area is covered with a palliative dressing such as zinc oxide eugenol cement.
The wound is allowed to heal and reviewed every second day till appreciable healing is observed.
Extraction Of Primary Root Stump
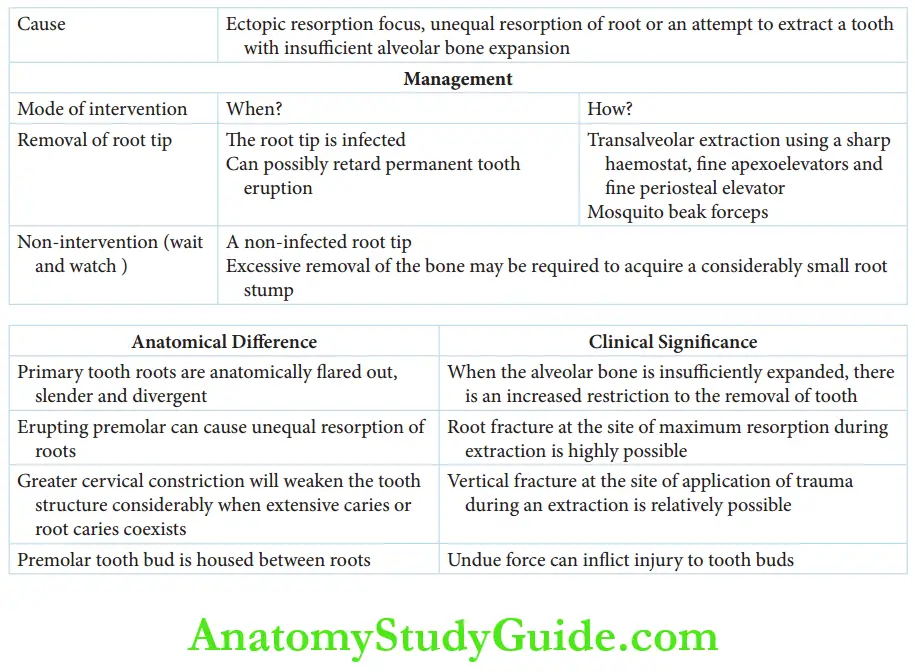
Ectopic resorption focus of the primary tooth root, unequal resorption of the root, or an attempt to extract the tooth with insufficient alveolar bone expansion are the causes of fracture of a primary tooth root.
A decision either to intervene or to wait and watch is made on a risk-benefit ratio.
A residual tooth root is removed when the root tip is infected.
The root tip is also removed when it can possibly delay or retard the eruption of the permanent tooth.
A non-infected root tip may be left behind to resorb.
thus is because excessive removal of bone may be required to extract a considerably small root stump.
Such an intervention may disturb the developing tooth buds.
Sometimes when non-infected broken root stumps are left behind, the eruptive force of the permanent teeth pushes the stump fragment to the mucosal surface.
The fragment passively lies beside the corresponding erupted permanent teeth and may have to be extracted.

Removal of the root stump can be done either by a closed method using elevators or by an open method by trans-alveolar extraction.
The closed method uses an apexoelevator or a fine periosteal elevator.
The elevator tip is placed at the point of contact between the root stump and the alveolar bone.
A rotational force is delivered to pick out the fragment. Single-root fragments with no root curvatures are usually mobilized with this technique.
When the root fragment is subgingival or has a distinct root curvature or when multiple root stumps are present, the open view or trans alveolar method is Post-operative instructions are the same as those for extraction.
Clinical Significance Of Primary Teeth Extraction
The alveolar bone is expansile. During an extraction, the tooth root socket is expanded due to this property of the alveolar bone.
However, when the alveolar bone is insufficiently expanded there could be an increased restriction to the removal of tooth/root.
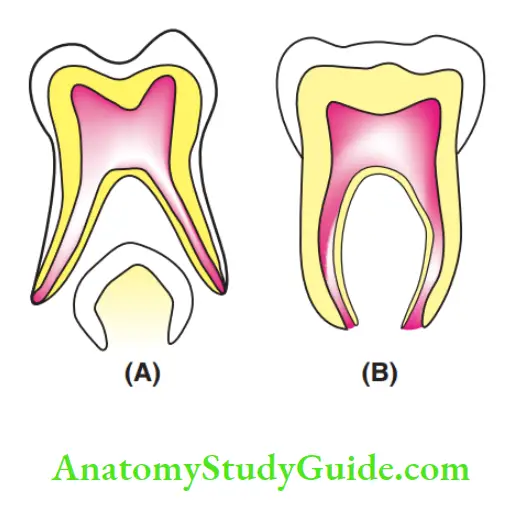
In multirooted primary teeth, the roots are flared out, slender, and divergent so as to house the developing premolars in between.
Exuberant or uncontrolled traction during extraction may harm the developing tooth bud.
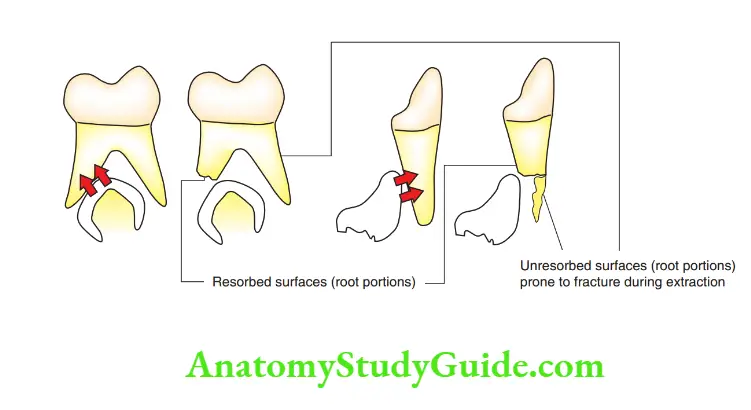
An erupting premolar can cause unequal resorption of roots or resorb the middle one-third of the root leaving the tip intact.
In these situations, root fracture at the site of maximum resorption during extraction is very common.
The greater cervical constriction of the primary tooth will weaken the tooth structure considerably when extensive crown caries and root caries co-exist.
During extraction, a vertical fracture at the site of the application of trauma is possible.
Hence, good pre-operative assessment and application of fundamentals ensure uneventful extraction of primary teeth.
Summary
1. Anatomical differences between primary and permanent teeth have clinical significance in pediatric oral surgery.
2. Primary teeth are at best preserved till exfoliation. However, indications of extraction are as follows:
Primary teeth that are contraindicated for endodontic therapy due to poor storability of tooth structure, presence of a periradicular lesion, or poor motivation
Retained deciduous teeth
Fractured and extremely mobile teeth with a poor prognosis on immobilization
3. Extraction protocol
4. Cause and management of fractured primary tooth root tips
Leave a Reply