Radiographic Investigation Introduction
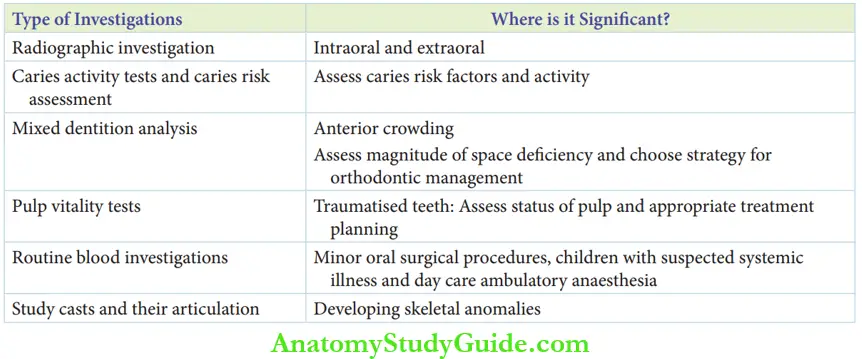
Case history obtained from the patient and a completely general and local examination help in arriving at the diagnosis. Several investigations are necessary to confirm the diagnosis, which are as follows:
Table of Contents
- Radiographic investigations include intraoral and extraoral radiographs. They are discussed in detail in this chapter.
- Caries activity tests and caries risk assessment are used to identify risk factors and assess the activity of caries.
- Mixed dentition analysis is advised in cases of anterior crowding to assess the magnitude of space deficiency and to choose the appropriate treatment mode.
- Pulp vitality tests are performed on a traumatised tooth to assess the status of its pulp and plan for the necessary treatment.
- Routine blood investigations may be required as a protocol to be followed before minor oral surgical procedures and in children with suspected systemic illnesses. Assessment of haemoglobin percentage is mandatory for children indicated for daycare ambulatory anaesthesia to rule out anaemic status. Hb% of 9 g/100 mL is the minimum requirement for treating the child under general anaesthesia and 7 g/100 mL for minor oral surgical procedures under local anaesthesia.
- Studying casts and their articulation may be useful for the assessment of developing skeletal anomalies.
Read And Learn More: Paediatric Dentistry Notes
- Types Of Radiographic Investigations Dental radiographs can be intraoral or extraoral depending upon the indication.
- Intraoral radiographs include the following:
- Intraoral periapical (IOPA) view radiograph
- Bitewing radiographs
- Maxillary and mandibular occlusal radiographs
- Extraoral radiographs include the following:
- Orthopantomograph
- Lateral/anteroposterior cephalogram
- Lateral oblique radiograph
- Paranasal sinus (PNS) view
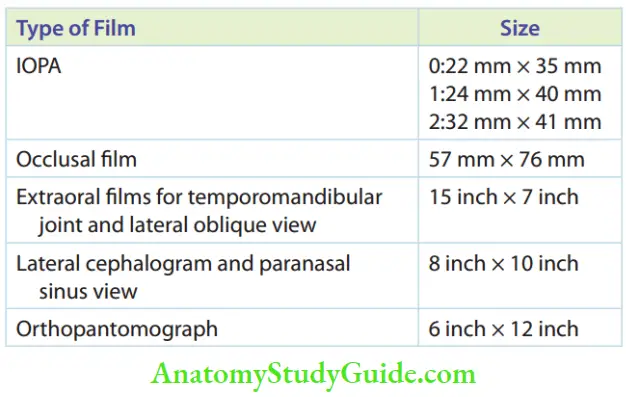
- P.A. skull sizes of the films are listed in Table.
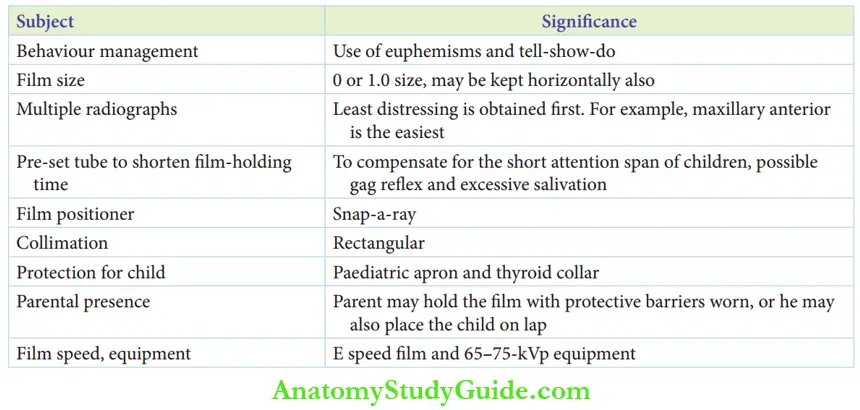
- When a child has to undergo dental radiography, the X-ray machine can be introduced as a camera and the film as a photograph. These are euphemisms. The systematic tell-show-do technique can help in familiarising the child and assessing the cooperative ability of the child. The child should be asked to wear a lead apron and a thyroid collar to provide thyroid and gonadal protection from radiation. The firm may be held by the child or the parent (who also should be wearing a lead apron and thyroid collar) and never by the dental assistant or the dentist. The parent may also seat the young child on his/her lap to hold the film in the child’s mouth.
- Intraoral radiographs include the following:
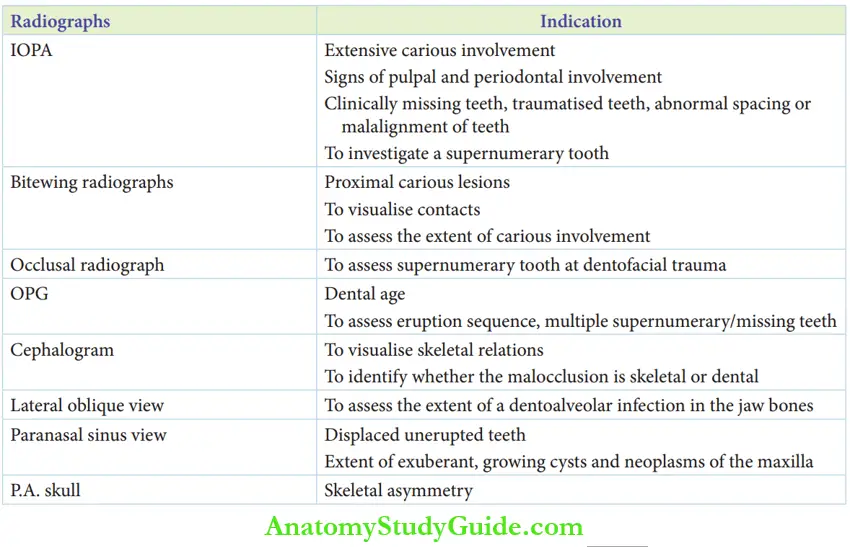
- Indications Of Radiographic Investigation The indications for each type of radiograph are as follows:
- IOPA view radiographs
- Extensive carious involvement with a possible pulp exposure
- Signs of pulpal and periodontal involvement – abscess with or without a draining sinus
- Clinically missing permanent teeth
- Missing primary teeth
- Traumatised primary and permanent teeth
- Abnormal spacing or malalignment of teeth
- Investigating the presence of a supernumerary tooth
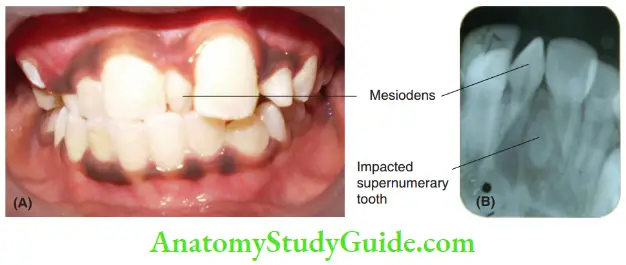
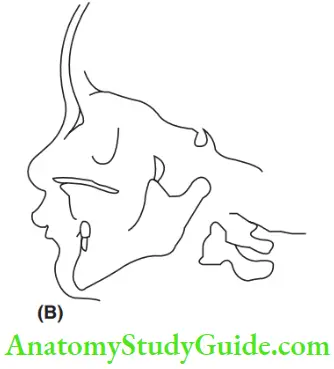
1. (A) Clinical picture of a 9-year-old boy showing a single median supernumerary tooth (mesiodens).
2. (B) The IOPA radiograph of the same patient reveals the presence of one more impacted supernumerary tooth.
- Bitewing radiographs
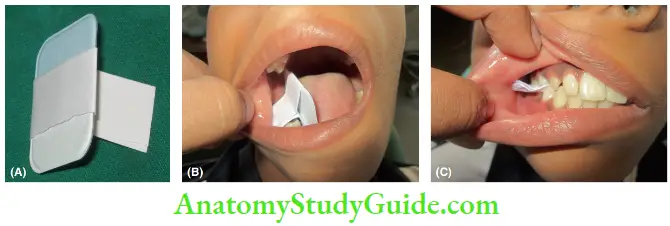 1. (A) An IOPA film wound in a paper bite tab.
1. (A) An IOPA film wound in a paper bite tab.
2. (B) Placement of the film with bite tab.
3. (C) Position at radiographic exposure.- To diagnose incipient proximal lesions
- To visualise contacts between teeth, which cannot be assessed clinically
- To expose the extent of serious involvement
- Occlusal radiographs
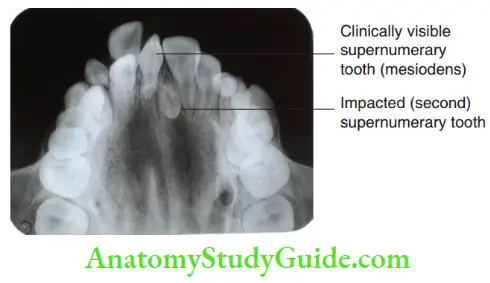
- To rule out multiple supernumerary teeth
- To identify the location of supernumerary teeth
- To diagnose dentofacial trauma
- To assess expansion of cortical bone contour due to infections or neoplasms
- Orthopantomogram (OPG)
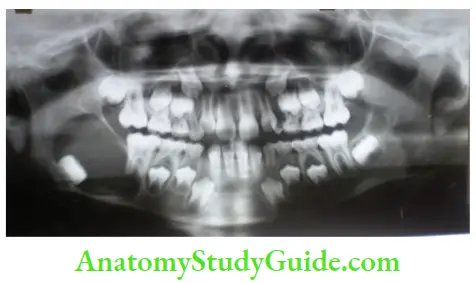
- To assess dental age
- To ensure the normal sequence of eruption
- In case of multiple supernumerary teeth (for example cleidocranial dysplasia)
- In case of multiple missing teeth (for example ectodermal dysplasia)
- Identify bony pathology/neoplasms
- To exhibit the extent of bone resorption/ sclerosis with existent infections, pathology and neoplasms
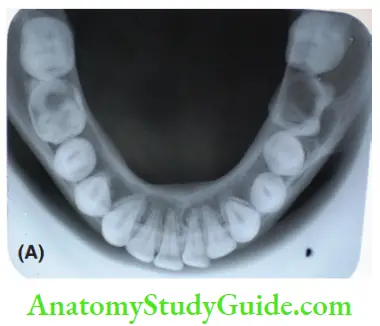
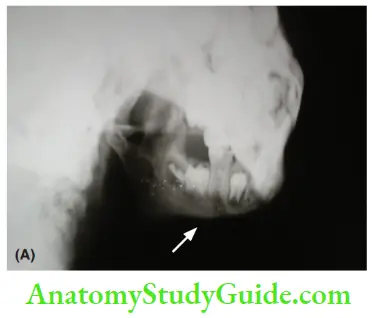
1. (A) Mandibular occlusal radiograph of a 12-year-old boy with chronic osteomyelitis showing the buccal expansion of cortical bone in the mandibular first molar region.
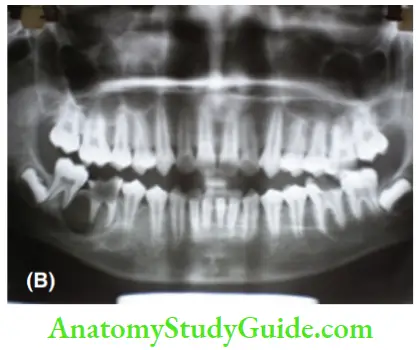
2. (B) Orthopantomogram of the same patient showing the extent of involvement of the chronic osteomyelitis lesion.
- Cephalogram
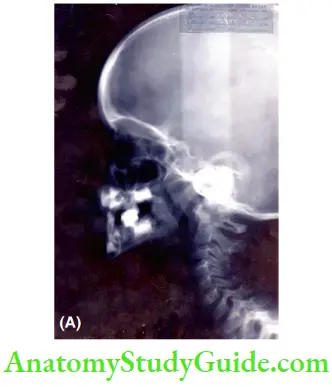
- A lateral cephalogram is a basic diagnostic radiograph for early orthodontic treatment. It can help to visualise skeletal relations and identify whether the malocclusion is skeletal or dental
- To assess if a convex profile is due to excessive maxillary growth or deficient mandibular growth and similarly, if a concave profile is due to excessive mandibular growth or deficient maxillary growth
- Lateral oblique view

- To assess the extent of a dentoalveolar infection in the jaw bones
- It is extremely useful in cases that have an extraoral draining sinus due to a dentoalveolar abscess
- Paranasal sinus view (Less commonly used in paediatric dentistry)
- To assess the location of displaced unerupted permanent or primary teeth
- To find out the extent of exuberant, growing cysts and neoplasms of the maxilla
- P.A. skull view
- Advised in cases with skeletal asymmetry and unilateral growth disturbances of the head and neck region
- IOPA view radiographs
Intraoral Radiographs
For an intraoral radiograph, the size of the film has to be comfortable and compatible with the child. The child is supposed to hold the film immobile in the mouth by clenching the teeth. ‘0’ size fim is the most ideal for children. ‘1’ size film may be used for children older than 10 years.
If a ‘0’ size film is too long to be accommodated in the child’s mouth, the film may be positioned horizontally. Larger-size intraoral periapical films may be used for anterior occlusal radiography of the primary dentition.
Bending the anterior corners of the film may help the child to tolerate the procedure in a better way. However, this may lower the diagnostic quality of the radiograph.
When radiographs of multiple teeth are required, the least difficult tooth image is obtained first. The approach follows the logic of systematic desensitisation.
The child will be able to tolerate more strenuous FIM placements after having completed the easy placement areas. A radiograph of the maxillary anterior region is the easiest to obtain from a child.
All settings are made on the X-ray machine and the tube is positioned before asking the child to hold the film. Thus, the time for which the film is held in the child’s mouth is shortened. This manoeuvre is followed as children have a short attention span.
They may experience gag reflexes, extreme discomfort and excessive salivation if the film is held for too long in their mouths. There are gadgets to hold the film instead of being held by clenching teeth. These are very useful for children who are unable to hold the film on their own. These gadgets are called fim positioners. Snap-a-ray is one such gadget.
Rectangular collimation is preferred over round collimation as some movement during exposure is expected from the paediatric patient. An ‘E’ speed film of size ‘0’, ‘1’ or ‘2’ with a 65–75-kVp machine is the ideal requirement for paediatric dental radiography.
For an extraoral radiograph, X-ray films are available in cassettes of standard sizes. OPG and cephalograms are standardised radiographic techniques as the distance between the source and patient and that between the patient and fim is filed.
Lateral oblique, PNS and P.A. views are non-standardised extraoral radiographs. The distance between the source and the patient may vary. The patient is positioned appropriately against the film cassette. In the extraoral techniques, there is no requirement for the patient to hold/position the film.
- Technique The basic aspects of the intraoral radiography technique include the positioning of the head of the patient and the intraoral film.
- Head position
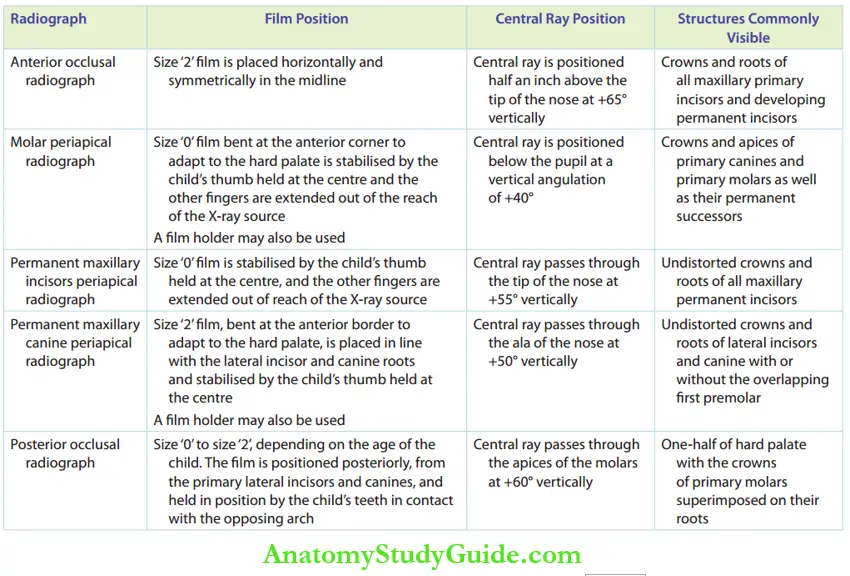
- Maxillary arch: The line connecting the ala of the nose to the tragus of the ear (ala-tragus line) should be parallel to the floor of the mouth for maxillary periapical radiographs and bitewing radiographs.
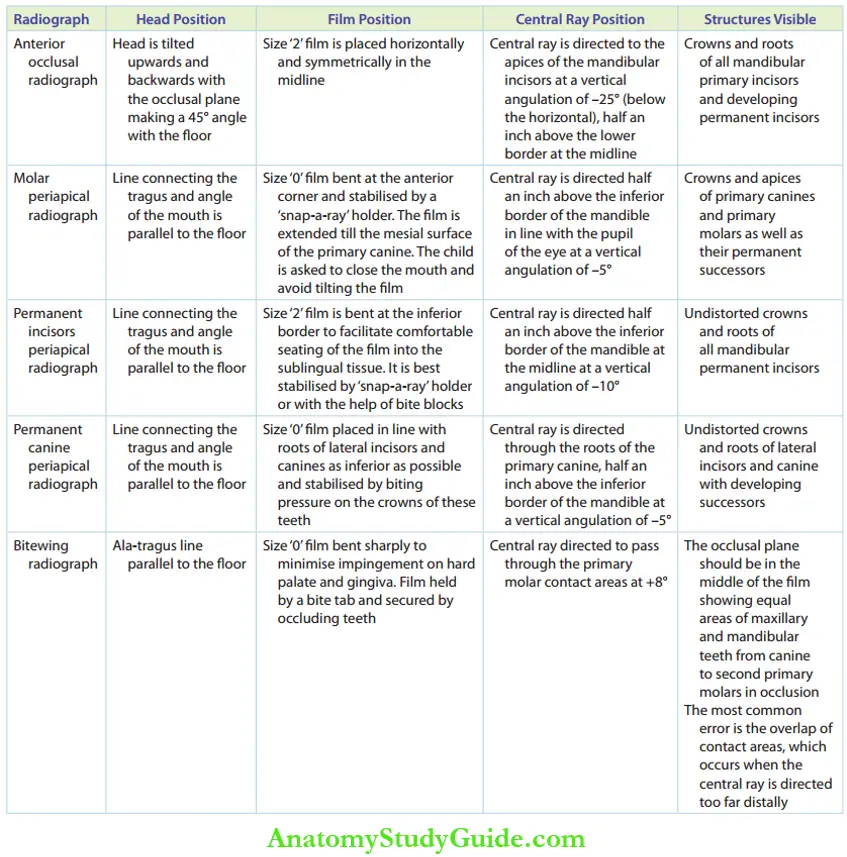
- Mandibular arch: The line connecting the tragus and the angle of the mouth should be parallel to the floor for intraoral radiographs except for the anterior occlusal radiograph. The head is tilted upwards and backwards with the occlusal plane making a 45° angle with the floor for an anterior occlusal radiograph.
- Film positioning and intraoral stabilisation All intraoral films are placed vertically with one edge placed 2 mm beyond the incisal or occlusal surface of the tooth to be studied. The embossed dot is at the incisal/occlusal and mesial end. For bitewing radiographs, the IOPA film is held by bite tabs or by an adhesive bite sponge (similar to those for adults). The embossed dot is kept at the anterior–superior corner. Intraoral stabilisation of IOPA radiographs is obtained by gentle and precise pressure exerted with the thumb by the child himself. All occlusal films are stabilised passively by the child by gently closing the mouth. For infants, the ‘patient on parent’ method is used with the mother stabilising the film.
- Central ray position: The X-ray source is at the centre of the tube. A line drawn from the centre of the X-ray source is called the central ray. The central ray position is very important to obtain a proper X-ray.
- Head position
The techniques of intraoral radiography for the maxillary and mandibular arches are given In the table.
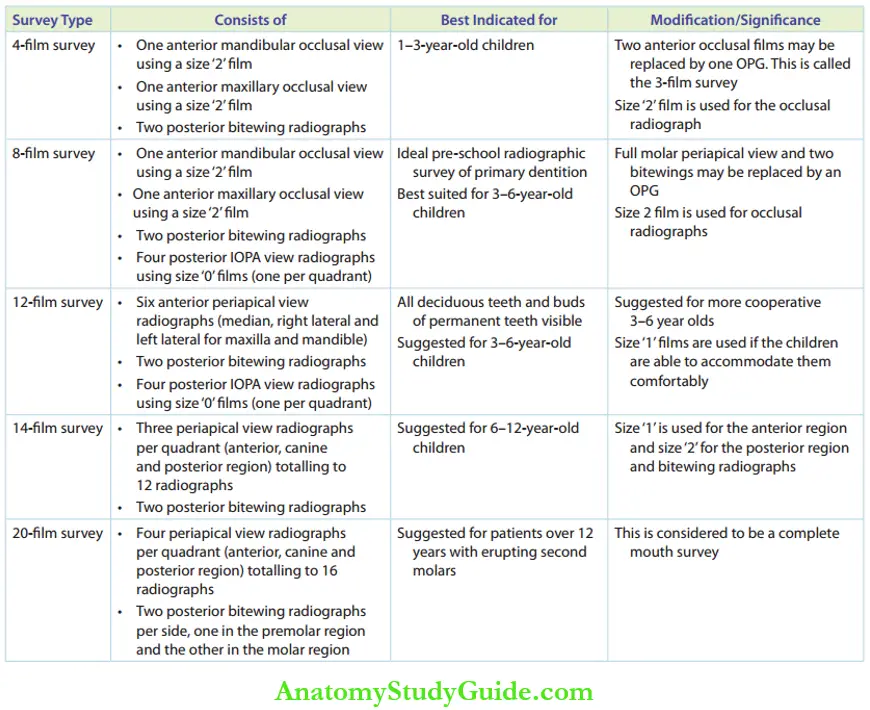
Radiographic Survey
Radiographs are made in accordance with the chief complaint or the clinical signs/symptoms of the patient. Radiographic assessment with a combination of IOPA, bitewing and occlusal radiographs during the preliminary (first) appointment or follow-up dental examination gives a complete picture of the status of the teeth.
Such a thorough radiographic screening is described as a radiographic survey. The advantages of a strategic radiographic survey over isolated intraoral firms are as follows:
- The exact number/extent of decay is studied
- All incipient/proximal cavities are identified
- The decay activity/susceptibility of the individual is concluded
- The status of the erupting/exfoliating teeth is vivid
The five types of radiographic survey modes are 4-fim, 8-fim, 12-fim, 14-fim and 20-fim surveys, respectively. They are recommended as per the age of the child. The table gives the details of each type of survey and its indications.
Summary
- Several investigations are necessary for the accurate framing of a diagnosis. The various diagnostic parameters in paediatric dentistry are as follows:
- General points of Emphasis During Radiography in paediatric dentistry
- Indications of radiography
Leave a Reply