Rickets
Case 1: Incomplete Mineralization
A 4-year-old child is characterized by bone deformities due to incomplete mineralization, resulting in soft and pliable bones. There is also a delay in teeth eruptions. The child is diagnosed to have rickets.
Table of Contents
Question 1. How many types of rickets are there?
Answer:
- Vitamin D deficient rickets in children.
- Osteomalacia in adult.
- Vitamin D-resistant rickets.
- Renal rickets.
- Hypophosphatemic rickets.
Read And Learn More: Biochemistry Clinical Case Studies With Answers
Question 2. State the cause of the disease.
Answer: Vitamin D deficiency.
Question 3. Which biochemical investigations need to be carried out?
Answer:
- Serum Vitamin D level decreases.
- Alkaline phosphatase level increases.
Question 4. How can the disease be treated?
Answer:
- Vitamin D is given orally or injectable.
- Increase sun exposure in the morning and evening by increasing outdoor activities.
- Increase consumption of fish liver oil, fish, and egg yolk.
Rickets Clinical Manifestations
- Insufficient mineralization causes soft and pliable bones.
- Bone deformities and weight-bearing bones get deformed.
- Bow legs, knock-knees, bossing of frontal bones, pigeon chest, and beaded chest appearance due to prominent costochondral junction (rickety rosary).
- Harrison’s sulcus– transverse depression passing outwards from costal cartilage to axilla.
Osteomalacia Clinical Manifestations
- Bones are softened due to insufficient mineralization and increased osteoporosis.
- Patients are more prone to fractures.
- Decreased serum calcium and phosphate.
- Alkaline phosphatase– bone isoenzyme will increase.
RDA– Children 400IU/day
Adult– 200IU/day.
Biochemical Role
- Increases serum calcium level by acting on the kidney, intestine, and bone.
- Causes bone mineralization, remodeling of bone, and increases bone mineral density
Case 2: Low Bone Density
A middle-aged woman reported a history of pain in the back and limbs. She also gave a history of pathological fracture. Her bone scan revealed low bone density.
Question 1. What is the diagnosis and probable cause?
Answer: Osteomalacia due to vitamin D deficiency.
Question 2. Which serum enzyme level will be affected?
Answer: Alkaline phosphatase– bone isoenzyme.
Question 3. Suggest the treatment and preventive measures.
Answer:
- Treatment– Vitamin D is given orally or injectable.
- Prevention– Increase sun exposure in the morning and evening by increasing outdoor activities.
- Increase consumption of fish liver oil, fish, and egg yolk.
Scurvy
Case 1: Bleeding Gums, Delayed Wound Healing
A 10-year-old child was brought to the hospital with complaints of bleeding gums, delayed wound healing, and red hemorrhagic spots all over the body.
- Diagnosis– Scurvy.
- Deficient vitamin– Vitamin C (Ascorbic acid). RDA– 60–75 mg.
- Sources– Indian gooseberry (amla), guava, orange (citrus fruits), etc.
Functions of Vitamin C
- Mnemonic to remember dehydroascorbate.
- Interconvertible into dehydroascorbate.
- Hydroxylation reactions– conversion of proline and lysine into hydroxyproline and hydroxylysine, helps in collagen cross-linking and strengthening.
- Antioxidant.
- Steroid synthesis.
- Cataract prevention.
- Oxidation-Reduction reactions.
- Spare Vitamin A and Vitamin E in antioxidant function.
- Tyrosine and tryptophan metabolism.
Deficiency Manifestations
- Swollen and bleeding gums.
- Scorbutic rosary– the beaded appearance of the chest due to prominent costochondral junctions.
- Ecchymosis or hemorrhagic spots due to capillary fragility (defective collagen synthesis).
- Delayed wound healing.
- Pseudo paralysis due to joint effusion in chronic cases.
Beriberi
Case 1: Numbness In The Legs
A 40-year-old male came to the hospital with complaints of muscle weakness, difficulty to rise from squatting position and numbness in the legs.
- On examination- deep tendon reflexes were diminished.
- Personal history- he is a chronic alcoholic and takes unpolished rice in his diet.
- Lab investigation- decreased RBC transketolase activity.
- Diagnosis– Dry beriberi.
- Deficient vitamin– Thiamine.
- Active form– TPP (Thiamine pyrophosphate).
- RDA– 1-1.5 mg/day.
Sources of thiamine– Cereals, pulses– mainly in the outer layer (bran), polishing of rice removes 80% of thiamine.
Important Functions of TPP
- Energy generation.
- Nerve impulse transmission.
Important Reactions
- Pyruvate dehydrogenase complex.
- Alpha keto glutarate dehydrogenase complex.
- Transketolase.
Deficiency Manifestation
- Dry beriberi– neurological involvement
- Wet beriberi– cardiac involvement and effusions
- Infantile beriberi.
- Acute fulminant CVS involvement– Shoshin beriberi.
- Wernicke’s-Korsakoff’s syndrome.
Wernicke’s-Korsakoff’s Syndrome
- Typically seen in alcoholics.
- Because alcohol decreases the absorption of thiamine from the intestine and also interferes with the conversion of thiamine to TPP.
- GOA MP mnemonic to remember symptoms.
- Global confusion.
- Ophthalmoplegia.
- Ataxia.
- Memory loss.
- Psychosis.
Case 2: Memory Loss And Unstable Gait
An alcoholic individual had symptoms of memory loss and unstable gait. His blood pyruvate level was increased.
Question 1. What is the probable diagnosis?
Answer: Wernicke’s-Korsakoff’s syndrome.
Question 2. What is the biochemical basis of the increase in pyruvate and the presence of neurological signs?
Answer:
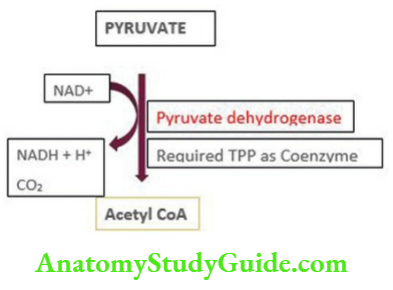
- Because alcohol decreases the absorption of thiamine from the intestine and also interferes with the conversion of thiamine to TPP.
- Decreased activity of TPP leads to the decreased activity of PDH complex and accumulation of pyruvate.
- Pyruvate accumulation in the brain causes neurological symptoms.
- Nerve impulse transmission is also affected by TPP deficiency.
Question 3. Which test can confirm the diagnosis?
Answer: Lab investigation- decreased RBC transketolase activity.
Leave a Reply