Scapular Region
Actions Of Deltoid Muscle And Its Nerve Supply
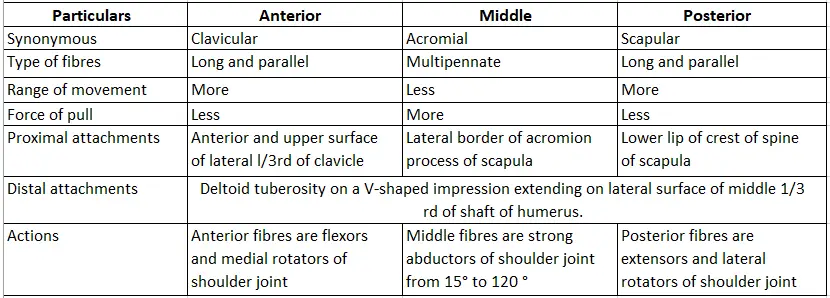
1. Scapular Region Actions Of Deltoid Muscle
Table of Contents
- Anterior fibers are flexors and medial rotators,
- Middle fibers are abductors, and
- Posterior fibers are the extensor and lateral rotator.
2. Scapular Region Nerve supply
- Axillary nerve (circumflex nerve)—ventral rami of C5-C8 and T1
Read And Learn More: Anatomy Notes And Important Question And Answers
Scapular Region Deltoid
Scapular Region Deltoid Introduction:
It is a lar, multipennate muscle present in the shoulder region
Scapula Anatomy
1. Deltoid Morphology, attachments, and actions.

2. Deltoid Nerve supply
Scapula Anatomy
Axillary nerve: C5 and C6 of the posterior cord of the brachial plexus.

3. Deltoid Structures Under Cover Of Deltoid
Structures Under Cover Of Deltoid Bones
1. Upper end of humerus with
- Greater and
- Lesser tubercles,
- Intertubercular sulcus,
- The upper part of the shaft, and
- The surgical neck of the humerus.
2. Structures Under Cover Of Deltoid Coracoid process of scapula.
Muscles attached to
1. Greater tubercle
- Supraspinatus,
- Infraspinatus, and
- Teres minor.
Scapula Anatomy
Glenoid cavity
- Supraglenoid tubercle: Long head of biceps,
- Infraglenoid tubercle: Long head of triceps.
Vessels
- Anterior circumflex humeral, and
- Posterior circumflex humeral.
Nerve: Axillary.
Joints and ligaments
- The shoulder joint, and
- Coracoacromial ligaments.
Bursae:
- Subacromial and
- Subdeltoid bursae, and
- Bursae of the shoulder joint.
4. Applied anatomy
1. Fracture of surgical neck of humerus causes lesion of the axillary nerve. It results in paralysis of the deltoid. This affects the movement of the shoulder joint especially abduction from 15° to 90°.
Paralysis of the deltoid results in loss of the rounded contour of the shoulder region.
2. In complete axillary nerve lesions, there is complete irreversible deltoid palsy.
3. With a functioning rotator cuff but a poor deltoid, the arm is functionally adept (proficient) and useful.
Rotator Cuff
Rotator Cuff Introduction:
It is a musculotendinous cuff of the shoulder joint. This is a fibrous sheath formed by 4 flattened tendons, namely.
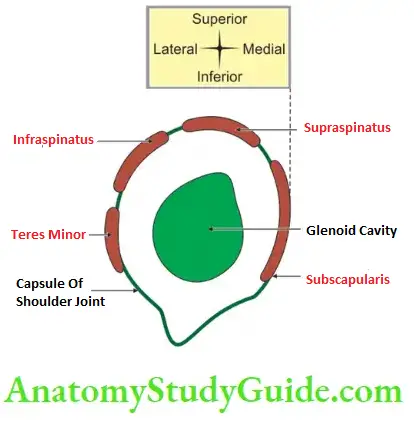
- Supraspinatus,
- Infraspinatus,
- Teres minor, and
- Subscapularis and lateral part of the capsule of the shoulder joint.
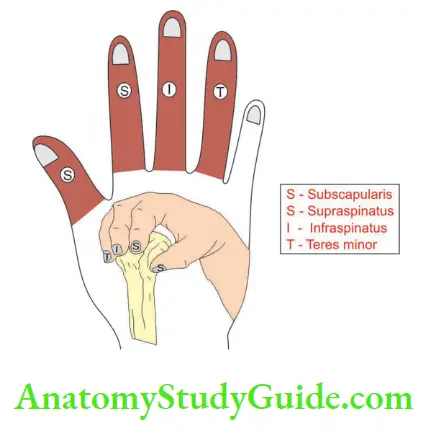
1. Rotator Cuff Features: (S)
- Sits on tuberosities,
- Sticks to the capsule of the shoulder joint,
- Steadie head of the humerus, and
- Strengthens the capsule.
2. Rotator Cuff Applied anatomy
Dislocation of the shoulder joint is more commonly in a downward direction because the capsule is lax inferiorly.
Scapula Anatomy
Quadrangular Space
Quadrangular Space Introduction:
It is an intermuscular space present in the axilla. It provides a passage between the axilla and posterior scapular and deltoid regions.
1. Quadrangular Space Boundaries
Above (from anterior to posterior):
- Subscapularis in front,
- The capsule of the shoulder joint, and
- Teres minor behind.
2 Below: Teres major.
3. Medial: Long head of the triceps.
4. Lateral: Surgical neck of the humerus.

2. Quadrangular Space Structures passing
- Axillary nerve, and
- Posterior circumflex humeral vessels.
3. Quadrangular Space Applied anatomy
Fracture of the surgical neck of the humerus causes lesions of the axillary nerve leading to paralysis of the deltoid muscle.
Upper Triangular Space
Upper Triangular Space Introduction:
It is an upper intermuscular lar space present in the axilla. It is an area of communication between the axilla and posterior scapular region.
1. Upper Triangular Space Boundaries
- Above: Teres minor
- Below: Teres major
- Lateral: Long head of the triceps
- Apex: Lateral border of the scapula where teres major and minor muscles converge.

2. Upper Triangular Space Structures passing
- Circumflex scapular artery, a branch of the subscapular artery.
- It pierces the origin of the teres minor and reaches the infraspinatus fossa to anastomose with the suprascapular artery.
3. Upper Triangular Space Applied anatomy
The circumflex scapular artery anastomoses with the descending branch of the transverse cervical artery and forms important anastomosis around the scapula.
Lower Triangular Space
Lower Triangular Space Introduction:
It is a lower intermuscular lar space present in the axilla.
1. Lower Triangular Space Boundaries
- Medially by the long head of the triceps,
- Laterally by a shaft of the humerus, and
- Above by teres major.
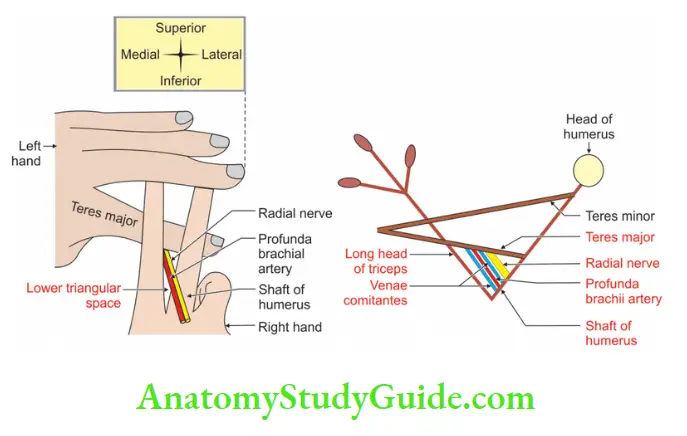
2. Lower Triangular Space Structures passing
- The radial nerve, and
- Profunda brachii vessels.
3. Lower Triangular Space Applied anatomy
Fracture of middle 1/3rd of humerus causes injury to radial nerve and results in wrist drop.
Name The Muscles Supplied By the Axillary Nerve
- Deltoid, and
- Teres minor.
A Ten-Year-Old Girl Fractures Her Humerus At The Surgical Neck What Damage Would You Check For And How
- Damage to the axillary nerve is checked.
- By testing the sensations over the lower lateral part of the skin of the deltoid.
Question-1: Describe The Axillary Nerve Under The Following Heads
1. Root value,
2. Course and relations,
3. Branches, and
4. Applied anatomy.
Answer:
The Axillary Nerve Introduction:
It is one of the two terminal branches of the posterior cord of the brachial plexus.
The Axillary Nerve Synonymous: Circumflex nerve.
1. The Axillary Nerve Root value
Ventral rami of C5 and C6.
The Axillary Nerve Peculiarities
- The posterior division of the axillary nerve bears pseudoganglion. (It is a thickening of nerves. It simulates ganglion. It does not have cell bodies.)
- The axillary nerve is the ideal example of Hilton’s law, i.e. the nerve supplying the muscles acting on the joint supplies the joint and skin over the joint.
2. The Axillary Nerve Course and Relations
- It arises from the posterior cord of the brachial plexus.
- The posterior cord lies posterior to the 2nd part of the axillary artery. The
- the axillary nerve lies posterior to 3rd part of the axillary artery.
In axilla: Despite its name, it supplies nothing in the axilla.
- Its origin is higher than what is usually imagined.
- First, it lies lateral to the radial nerve and anterior to the subscapularis.
- At the lower border of the subscapularis, it curves posterior, inferior to the capsule of the shoulder joint.
- It enters the quadrangular space.
In quadrangular space
1. The relations of axillary nerves in quadrangular space are
- Subscapularis above and anterior
- Teres minor above and posterior and
- Teres major below,
- The long head of the triceps medially, and
- The surgical neck of the humerus laterally.
In the quadrangular space, the posterior circumflex humeral artery is below it. It is accompanied by venae comitantes. The nerve divides into anterior and posterior divisions.
The anterior division is accompanied by the posterior circumflex humeral artery (branch of the 3rd part of an axillary artery). They curve around the neck of the humerus.
They run deep to the deltoid muscle and supply the deltoid and skin over the anterior part of the deltoid muscle.
The posterior division supplies teres minor which bears pseudoganglion. It also supplies the posterior part of the deltoid muscle. It pierces the deep fascia to become the upper lateral cutaneous nerve of the arm. It emerges at the back of the axilla below the teres minor.
3. The Axillary Nerve Branches And Distribution
Muscular
- Deltoid from both divisions.
- Teres minor from posterior division.
Cutaneous:
The upper lateral cutaneous nerve of the arm arises from the posterior division of the axillary nerve and supplies the skin over
- The posterior border of the deltoid, and
- The upper part of the long head of the triceps.
The articular branch to the shoulder joint arises from the trunk of the axillary nerve.
The vascular branch to the posterior circumflex humeral artery arises from the anterior division.

4. The Axillary Nerve Applied Anatomy
1. Axillary nerve and neurovascular structures are damaged in the fracture of the surgical neck of the humerus.
2. The axillary nerve is damaged in the dislocation of the shoulder. The incidence is about 5%.
The other causes of the lesion of the axillary nerve are
- Fracture of the upper end of the humerus,
- Injection at the rounded contour of the deltoid.
3. Damage of the axillary nerve results into
- Loss of roundness of shoulder,
- The prominence of the greater tubercle of the humerus,
- Loss of abduction of the shoulder joint,
- Overhead abduction of the shoulder joint is prevented by reflex inhibition of the deltoid through the axillary nerve (Hilton’s law), and
- Loss of sensations of the skin over the lower half of the deltoid.
It is, therefore, called the ULC nerve (upper lateral cutaneous nerve of the arm).
Movements Of The Pectoral Girdle
The Pectoral Girdle Introduction:
Movements of the acromioclavicular and sternoclavicular joints are always associated with the movement of the scapula.
1. The Pectoral Girdle Movements
The movements of the scapula may or may not be associated with the movements of the shoulder joint. The various movements are described as follows :
The Pectoral Girdle Elevation (shrugging the shoulders): It is associated with the raising of the acromioclavicular joint and depression of the sternoclavicular joint.
Muscles bring the movements
- Upper fibres of trapezius, and
- Levator scapulae.
The Pectoral Girdle Depression (drooping of the shoulder): It is associated with depression of the acromioclavicular joint and elevation of the sternoclavicular joint.
Factors bringing the movements
1. Gravity,
2. Muscles
- Lower fibers of the serratus anterior, and
- Pectoralis minor.
The Pectoral Girdle Protraction (as in pushing and punching movement): It is associated with the forward movement of the lateral end and backward movement of the medial end of the clavicle.
Muscles bring the movements
- Serratus anterior, and
- Pectoralis minor.
The Pectoral Girdle Retraction of the scapula (squaring of the shoulder): It is associated with the backward movement of the lateral end and forward movement of the medial end of the clavicle.
Muscles bring the movements
- Rhomboids major and minor, and
- Trapezius.
Forward rotation of the scapula around the chest wall takes place during overhead abduction of the arm. The scapula rotates around the coracoclavicular ligament.
Muscles bring the movements
- Upper fibers of the trapezius, and
- Lower fibers of serratus anterior.
Backward rotation of the scapula occurs under the influence of gravity.
Muscles bring the movements
- Levator scapulae, and
- Rhomboids.

Winging Of Scapula
1. Winging Of Scapula Definition
It is a deformity of the scapula. When the arm is raised, the medial border and inferior angle of the scapula are pulled away from the posterior thoracic wall.
The scapula looks like a wing. Hence, it is called winged scapula or winging of scapula.
2. Winging Of Scapula Nerve damaged
- Nerve to serratus anterior (C5, C6, C7), and
- Scapular instabilities may injure the spinal accessory nerve.
3. Winging Of Scapula Weakness of the serratus anterior may arise from
- Damage to the long thoracic nerve,
- Injury to the brachial plexus,
- Viral infection of the 5th, 6th and 7th cervical nerve roots, and
- Certain types of muscular dystrophy.
4. Winging Of Scapula Causes
Due to trauma
- When the limbs are elevated, as in a knife fight, the nerve is especially vulnerable.
- Weapons, including bullets directed toward the thorax, are a common source of injury.
- Shoulder or neck injuries.
- Carrying a load on the shoulder.
Due to infection: Viral illnesses or toxoid injections, and
Due to surgical intervention: The nerve may be injured during surgical removal of axillary lymph nodes.
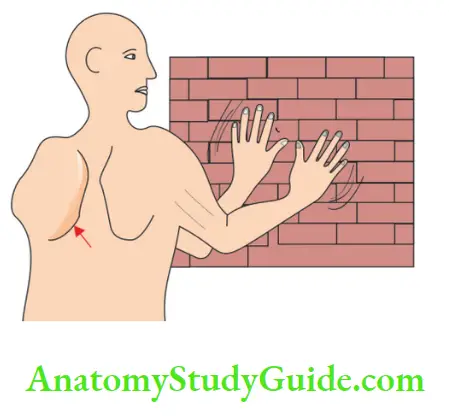
5. Winging Of Scapula Clinical features
- The damage leads to the winging of the scapula (Fig. 27.12). Winging of the scapula causes asymmetry of the shoulders.
- It may not be obvious until the patient tries to contract the serratus anterior against resistance.
- It is displayed by asking the patient to push forward against a wall.
- The patient, therefore, experiences difficulty in raising the arm above the head.
- Damage to the nerve to the serratus anterior unable the swimmer from carrying their arm forward in breaststroke swimming, it is called ‘swimmer’s palsy’.
6. Winging Of Scapula Prognosis
There is spontaneous recovery. It may take a year or longer time.
There is little or no recovery in the direct injury of the nerve or division of the nerve.
7. Winging Of Scapula Treatment
- Disability is usually slight and is best accepted.
- If the function is markedly impaired, the scapula can be stabilized by tendon transfer.
Ape Thumb Deformity
Ape thumb deformity
1. Ape-monkey without tail, for Example. gorilla, chimpanzee, orangutan, and gibbons.
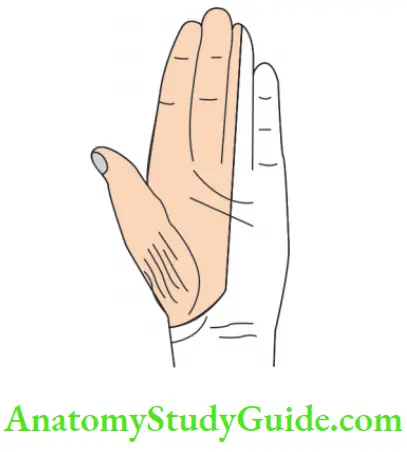
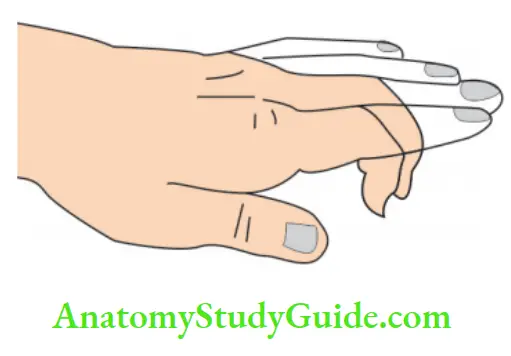
2. Ape hand-hand with the thumb permanently extended.
3. Injuries to the median nerve at the wrist result in ape hand.
Following muscles of thenar eminence are affected
- Abductor pollicis,
- Flexor pollicis brevis-superficial head, and
- Opponents policies.
Clinical features
- Paralysis of the muscles of the thenar eminence,
- Wasting of thenar eminence resulting in a flattening of the thenar eminence,
- The thumb is laterally rotated and adducted,
- The hand is “ape-like”
- Opposition movement of the thumb is impossible, and
- The first two lumbrical are paralyzed. It can be recognized clinically when the patient is asked to make a fist slowly. The index and middle fingers tend to lag behind the ring and little fingers.
Sensory loss: There is loss of sensation over the central part and lateral 1/2 of the palm and lateral 31/2 digits.
Scapular Anastomosis
Anastomoses around the body of the scapula. The anastomoses occur in the three fossae and are a process.
1. Subscapular Fossa
- Posterior circumflex humeral artery, and
- Circumflex scapular artery.

2. Supraspinous fossa
Anastomoses between
- Deep branch of the transverse cervical artery (branch of the subclavian artery) and
- Suprascapular artery, a branch of the thyrocervical trunk (branch of the subclavian artery)
3. Infraspinatus fossa
Anastomoses between
- Suprascapular,
- Deep branch of transverse cervical, and
- Circumflex scapular branches.
4. Anastomoses over the acromion process.
It is by acromial branches of
- Thoracoacromial artery (2nd part of axillary)
- Suprascapular artery (1st part of subclavian).
- Posterior circumflex humeral artery (3rd part of axillary)
Note that this is an anastomosis between the 1st part of the subclavian artery and the branches of the 2nd and 3rd parts of the axillary artery
Leave a Reply