Science Of Child Behaviour Introduction
The pattern in which a child responds to any social and environmental stimulus is described as the behaviour of the child. Behavioural paediatric dentistry is described as the science that understands the development of fear, anxiety and anger of a child in a dental clinic. Children are influenced in various ways in a dental operatory.
Table of Contents
While the behaviour of children cannot be dictated, the pedodontist can try to understand, analyse and manipulate it with a few strategic techniques. The technical skills of a pedodontist and his ability to acquire and maintain the cooperation of a child decide the success of dental treatment delivered to the child.
Read And Learn More: Paediatric Dentistry Notes
Management of the child’s behaviour at the dental operatory is a strategy with a clearly defined outline. This chapter enumerates the factors that influence the behaviour of a child.
- Classification Of Behaviour
Child behaviour in a dental operatory has been classified by a few authors. The widely accepted classifications are as follows:
- Wilson’s classification: Wilson classified the behaviour of children in 1933. His classification is the earliest established, comprehensive classification of child behaviour. However, it was not proposed for the purpose of paediatric dentistry primarily. It had been later adapted as appropriate for the science. It consists of four classes.
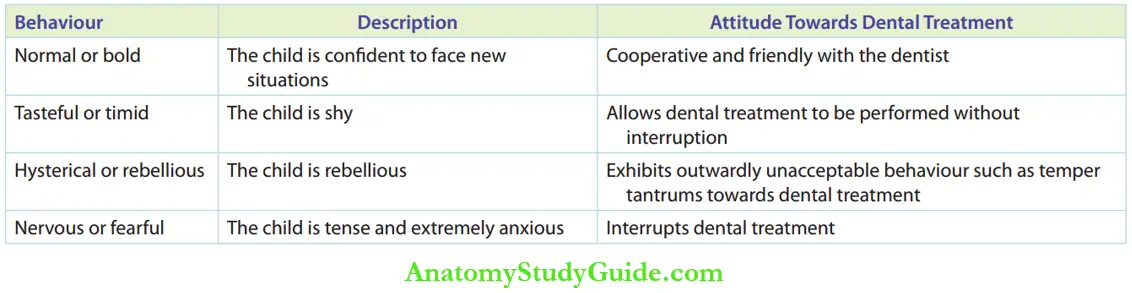
- Lampshire’s classification: Lampshire gave a comprehensive description of child behaviour in 1970.
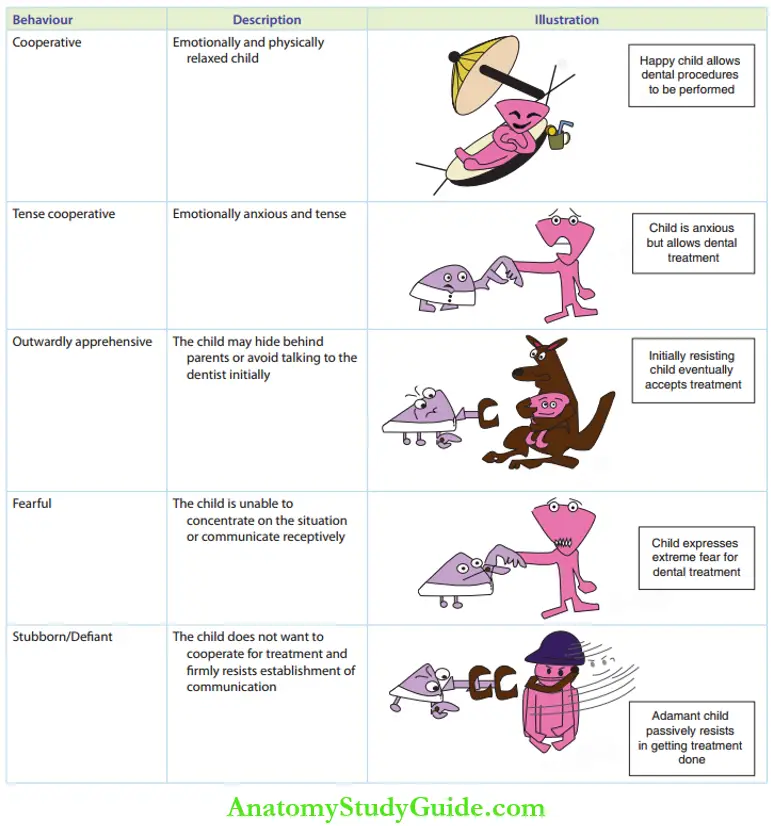
- Wright’s classification: Wright’s classification can be broadly classified into positive or cooperative and negative behaviour. A cooperative child is relaxed and accepts treatment.
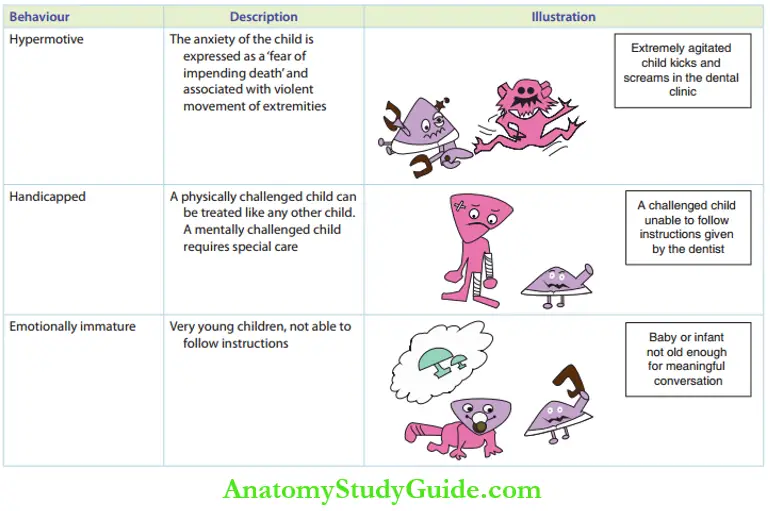
There is a class described as lacking cooperative ability. Establishing communication is not possible with these children. They may be either emotionally immature, very young children or physically or intellectually challenged children.
The negative category children are extremely anxious with inherent fears. But they have the potential to cooperate and can be influenced to become cooperative. Hence, they are also described as a potentially cooperative class.
The various subdivisions under this class are as follows:
- Uncontrolled or hysterical: The child displays temper tantrums including loud cries and violent movement of extremities.
- Defint or obstinate: The child is very stubborn and resists treatment.
- Tense cooperative: The child agrees to the treatment but is tense. This can be described as a borderline between positive and negative.
- Timid or shy: This is usually displayed by overprotected children at their first dental visit.
- Whining: The child receives treatment with continuous complaints throughout the procedure.
- Stoic: The child receives treatment passively without any expression. This is a typical characteristic of physically abused children. They are cooperative but do not communicate.
Of the three classifications discussed in the preceding text, Wright’s classification is clinically more applicable.
Factors Influencing Child Behaviour In A Dental Operatory
The factors that influence the behaviour of children in a dental operatory can be broadly classified into the following three categories:
- Sociocultural And developmental factors
- Familial factors
- Factors associated with the dentist/dental operatory
The first two categories are not in the control of the dentist. The third factor is purely dependent on the dentist. Though the relative strength of each factor has not been described, all the factors cumulatively contribute to the behaviour of the child in the dental clinic.
1. Sociocultural And Developmental Factors
There are four constituents under sociocultural and developmental factors, as shown.
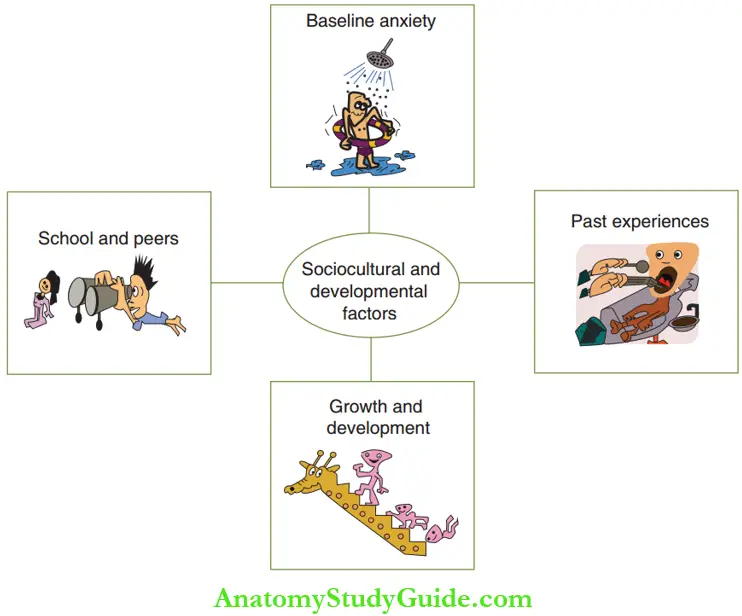
- Baseline anxiety: Th unperturbed initial anxiety of a child before any dental appointment is the baseline anxiety. It depends on the psychological strength of the child to face new situations and challenges. Efficient parenting helps children to have a positive attitude towards new situations. Such children are confident and have less baseline anxiety. The baseline anxiety is high in overprotected or overindulged children. Children born to women with an increased maternal age or nurtured by a single parent can also have high baseline anxiety. These children are under severe tension and do not have a positive attitude towards treatment.
- Past medical or dental experience: Sometimes, a child may have encountered an unpleasant medical or dental treatment in the past. Such a child is negative towards receiving any dental treatment. Similarly, a painless medical/dental experience makes the child positive of receiving treatment.
- School environment and peer influences: Children are active, curious and open to views and suggestions. Association with peers in the school environment gives them bountiful sociocultural learning. The peers may narrate their experiences during medical or dental treatment or express their prejudice towards the situation. This may invoke fear for doctors and make the child frightened at the start of the appointment. A child who benefited by school dental health programmes will have a positive approach towards dental treatment. The importance of teeth and oral hygiene might have been taught to the child.
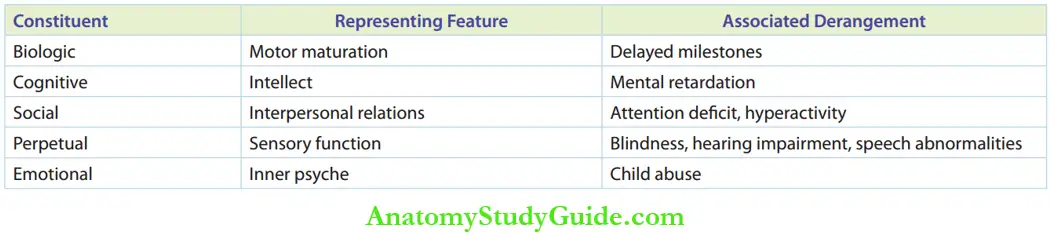
- Growth and development pattern: Physical growth and the pattern of development are associated with each other. The systemic and local (oral) growth should be maturing in a coherent manner for a child to have a positive behaviour pattern. Some derangement in development can leave a negative attitude in the child’s mind. Systemic growth disturbance may lead to retarded physical growth or any illness. Local growth disturbance may cause conditions such as cleft lip and palate. Lists the constituents of growth and associated derangements in the development pattern.
2. Familial Factors
The family plays an important role in influencing the behaviour of a child. Bell put forth a one-tailed theory where he suggested that parents have a unidirectional influence on their child’s attitude. The parent–child relationship has a linear pattern of expression.
In this relationship, parental attitude is an independent variable and child behaviour is a dependent variable. Parental anxiety has been given attention since 1891. Maternal anxiety or the anxiety of the mother has received considerable attention as mothers accompany their children more often. The association between the mother and the child is more pronounced during the first dental visit.
Children of all ages are influenced by their mothers. It is stronger between 3 and 7 years of age and more intense between 3 and 4 years of age. Highly anxious mothers can install a negative influence on their child’s behaviour. Children who are accompanied by their mother with a positive attitude about dental treatment display good behaviour and express minimal anxiety in the dental operatory.
The behaviour of a child is influenced by the siblings also. The children may reproduce the behaviour of their older siblings without awareness. This is described as identification or modelling by various experts. Siblings of the same sex and with an age gap of less than 2 years have maximum behaviour correlation. When the siblings are of the opposite sex and the age gap is more than 4 years, the behaviour correlation may be poor.
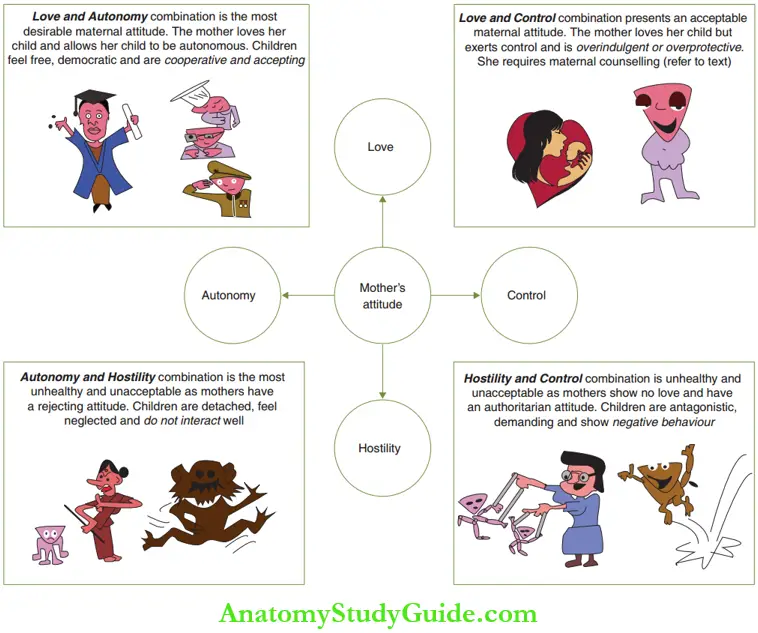
- Expression Of Maternal Behaviour The attitude of a mother can be expressed in two extremes. These extremes influence the child differently. The figure depicts a flowchart with the combination of a mother’s expressions and the corresponding child’s personality. Mothers who express love and exercise control may be overprotective or overindulgent.
An overprotective mother gives excessive care to the child, disproportionate to his age. She attempts to keep him as a child always. She is very closely associated with the child’s daily activities. The child is not allowed to take even low risks at play. She shows excessive concern over medical/ dental health. This is potentially harmful to the child’s normal development. Maternal overprotection may be due to various reasons such as:- Previous miscarriages
- The long delay in conception
- Death of an earlier sibling
- Childbearing physical, mental retardation or medical illness
- Death or divorce of the partner
An overprotective mother can be either dominating or overindulgent. A dominating mother makes her children extremely shy, submissive and anxious. A mother who is overprotective and overindulgent makes her child aggressive and demanding. The child seeks constant attention and service. He is not anxious in a new situation but has the potential to produce physical assault or temper tantrums when his wishes are denied. The child expects and demands the attention of the dentist.
The overindulgent attitude of the mother may sometimes be associated with an overprotective attitude as explained earlier. But it may show up independently also.
Overindulgence of parents/grandparents leads to the following behaviour of the child:
- The child is given all that he wants due to financial feasibility
- The child is a ‘spoilt child’ and gets on his own way
- The child exhibits impeded emotional development, remains infantile and is dependent
- The child may exhibit temper tantrums or outbursts when he is unable to control the situations happening in the dental office
Common examples of poor maternal attitude corresponding to dental treatment are as follows:
- Threatening the child with dental treatment as a mode of punishment
- Improper preparation of the child for the first appointment
- Imposing her anxiety onto the child
All these lead to a lack of cooperation of the child in the dental operatory. To conclude on maternal attitude and child behaviour in the dental operatory, mothers who love their children and allow them to be autonomous have friendly cooperative, attentive children showing positive behaviour at the dental operatory.
On the contrary, hostile mothers who exercise their control over children have excited and unhappy children who express negative behaviour.
3. Factors associated with the dentist/dental operatory
The constituent factors are shown in Figure and the discussion is given in the following text.
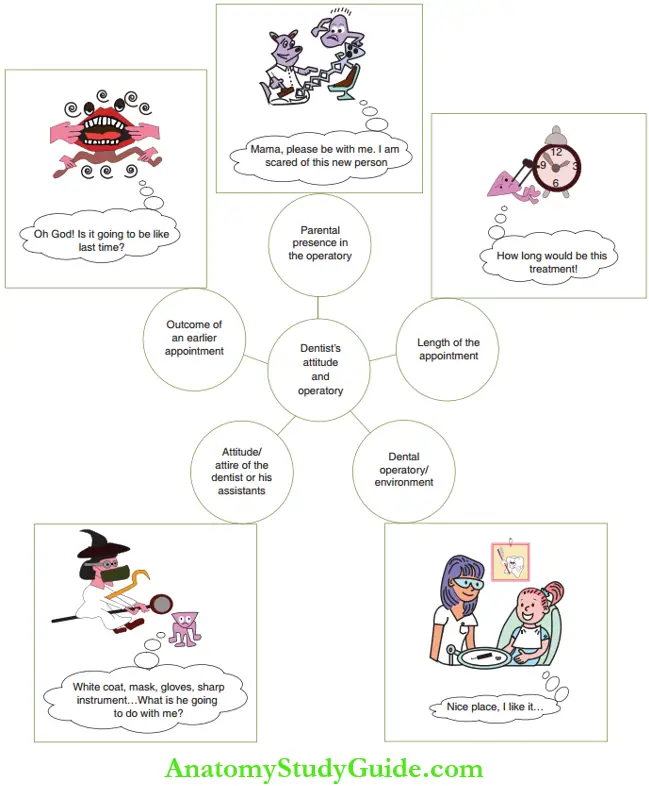
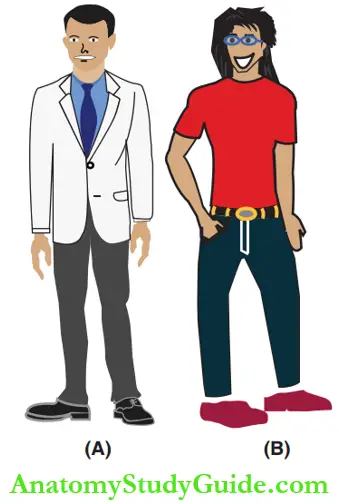
- Dentist attitude/attire: An ideal attitude of the dentist and dental assistant is highly essential to obtain cooperative behaviour of the paediatric patient. The attire of the paediatric dentist implies the hairdo, dress makeover and general outlook. The most appropriate and least appropriate looks of a dentist are depicted in Figure. The dentist’s attire should communicate a ‘security’ symbol as well as an ‘authority’ figure. The attire should be approachable and inviting for children to interact with. Bizarre and flirty clothes to attract children’s attention are absolutely inappropriate.
- Dental operatory/environment: An ideal paediatric dental operatory should not look like a hospital. A paediatric clinic should allay the anxiety of the child and assist in obtaining cooperative behaviour.
- The outcome of an earlier appointment: A painful previous dental appointment can increase the fear and anxiety in subsequent appointments. A sound understanding of the behaviour management techniques and a structured paediatric operatory can bring down the anxiety of the child by at least 10% with each subsequent appointment. ‘Even with the best quality of a restoration, the appointment is a failure if the child departs in tears’.
- Parental presence in the operatory: The dentist should capture the orientation of the child in a complete and undivided quantum to manipulate child behaviour. Parental presence can be a source of diversion to the child and a barrier to the dentist. Parents tend to repeat commands and this can disturb the child. The child, wanting to seek the attention of the parents, enacts to be distressed and indulged in pain. Hence, parents can be requested to leave their child alone with a dentist for a more effective behaviour management However, the parents can be encouraged to be inside the operatory in the following situations:
- Stranger anxiety is the exuberantly exaggerated level of anxiety manifested in 2-year-old children. It is evoked by absolutely unfamiliar persons, objects or situations. Any familiar entity (parent) can counteract stranger anxiety.
- Separation anxiety is an exaggerated level of anxiety manifested in 2–3-year-old children, more specifically around 30 months of age. The dentist should have
- An academic fatherly look rather than
- A funny Romeo kind of look.
- It is the response to separation and subsequent absence of the primary caretaker. Parental presence and participation during treatment can counteract this.
- The parent can help to restrain the child on either a lap-to-lap mode, patient-on-parent mode or bystander mode.Thus, if the presence of the parents can reduce the anxiety of the child and help in behaviour management techniques, they can be permitted during dental treatment. If the parental presence is a source of diversion of a child’s attention, they can be requested to leave the operatory. If the parent is not confident to leave the child alone with the dentist, when requested, delivery of treatment can be best refused, as ‘mutual trust’ is the basis of the profession.
- Length and schedule of the appointment: ‘Attention span’ refers to the time span during which the orientation of the child required for effective behaviour management can be predictably maintained with no distortion or deviation. Behaviour management techniques do not work as predicted in children with a lapse over this time span.
A short appointment is for around 30 minutes and a longer appointment for around 45 minutes. Literature suggests that early morning appointments are best suited for children as they tend to be more relaxed and cooperative.
Science Of Child Behaviour Summary
- Management of a child’s behaviour is a science more than an art.
- Factors influencing children’s behaviour in the dental operatory are as follows:
- Sociocultural and developmental factors
- Baseline anxiety
- Past experiences at medical and dental treatment
- Normal growth and developmental pattern
- School environment and peer influences
- Familial factors
- Parent attitude/behaviour
- Material anxiety
- Siblings relationship
- Factors associated with dentist/dental operatory
- Sociocultural and developmental factors
- Dental operatory/environment
- Attitude/attire of the dentist/assistants
- The outcome of the earlier treatment
- Length/schedule of appointment
- Presence of the parent in the operatory
- Management of child behaviour can be executed either by psychological behaviour management or by pharmacological means.
- Psychological mode applies techniques to manipulate the child’s mind and pharmacological mode uses sedatives/general anaesthetics.
Leave a Reply