Semi Permanent Restorations Introduction
Dental caries are better prevented than restored. Prompt detection and early restoration are the best ways of dealing with dental caries. Full-coverage restorations are indicated in clinical situations where simple restorations with amalgam or plastic materials may not be sufficient.
Table of Contents
Full-coverage restorations or crowns fabricated to rehabilitate compromised tooth structures are called semi-permanent restorations. They are expected to serve for an average span of 2–5 years. Hence, they are called ‘semi-permanent’.
Read And Learn More: Paediatric Dentistry Notes
Semi-permanent restorations are of three types. They are as follows:
- Stainless steel crowns (SSCs)
- Cellulose acetate strip crowns
- Polycarbonate crowns
Semi-permanent restorations are pre-fabricated. Minor tooth preparation is done and the pre-fabricated crown is customized to the tooth to be rehabilitated in a single appointment.
SSCs facilitate full coverage for primary and permanent fist and second molars. Cellulose acetate strips and polycarbonate crowns are modes of rehabilitating primary incisors and canines. SSCs are also available for primary incisors.
Semi Permanent Restorations Indications Of Semi-Permanent Restorations
The following three clinical situations nieces site the fabrication of full-coverage restorations:
1. Grossly carious primary tooth:
A grossly decayed incisor or a molar with the carious involvement of three or more surfaces requires a full-coverage restoration.
An amalgam or GIC restoration may not be useful in this case. A rigid amalgam restoration requires extensive tooth preparation, which can expose the pulp or leave the prepared tooth with a very poor resistance form.
A glass ionomer restoration involves the removal of the carious tooth structure only, and no specific cavity preparation is needed. But such a restoration has poor fracture resistance and shear strength to qualify as a successful multisurface restoration.
2. Pulpotomised/pulpectomised primary teeth:
Partial or total excision of pulp leads to dehydration of the tooth making it prone to fracture. A full-coverage restoration is required in this case to avoid fracture. The success of a pulpotomy/pulpectomy procedure is also dependent on the coronal seal obtained by post-endodontic restorations.
Full-coverage restorations serve as ideal post-endodontic restorations.
3. Developmental defects:
Rapid wear and tear occurs in teeth with developmental defects such as enamel
hypoplasia and dentinogenesis imperfect.
They demonstrate non-carious pulpal exposures. Dental caries, once initiated, spreads faster in these teeth. Full coverage is a logical mode of treatment to prevent the initiation of dental caries and eliminate the susceptibility of such teeth to wear and tear.
Stainless Steel Crowns
SSCs were introduced by Humphrey in 1950. Initially, SSCs were chrome steel crowns with the following composition:
- Chromium – 18%
- Nickel – 8%
- Iron – rest
Later, the composition of SSCs was replaced due to their superior strength and other physical properties.
Nickel–chromium alloy crowns are dimensionally more stable during a function in the oral cavity. The composition of this alloy is as follows:
- Nickel – 77%
- Chromium – 15%
- Iron – 7%
Nowadays, the term SSC corresponds to the nickel–chromium alloy crowns only.
SSCs are available in a ‘box-form’ where there are six sizes of crowns ranging from 2 to 7 corresponding to each primary/permanent molar.
Size 2 is for the smallest crown and size 7 is for the largest.
Stainless Steel Crowns Indications
The following are the indications of an SSC.
1. Pulpectomised or pulpotomies primary and permanent molars:
Access cavity preparation on a palpably involved molar leaves the tooth structure compromised. A post-endodontic direct amalgam restoration makes the tooth prone to vertical fractures.
SSC rehabilitation is ideal under such circumstances as it gives full coverage and leaves no chances for coronal microleakage to augment the rigidity of the tooth, which is otherwise brittle and fractures on tensile/ compressive stresses depicts a case of palpably involved primary molar rehabilitated with an SSC.
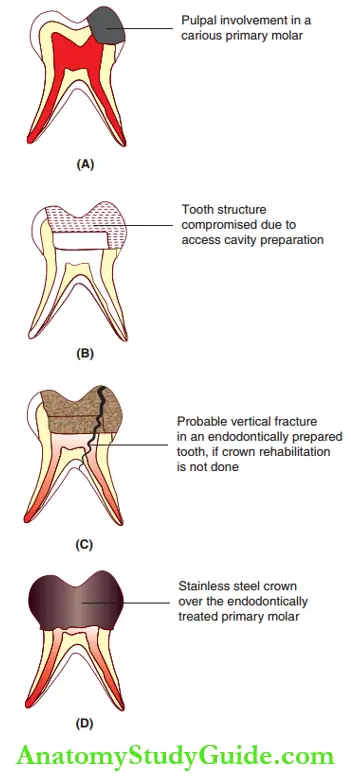
- (A) Pulpally involved primary molar.
- (B) Access cavity preparation on the primary molar.
- (C) Post-endodontic restoration leading to vertical fracture.
- (D) Stainless steel crown on the primary molar tooth.
2. Multisurface carious lesions:
When decay involves more than two surfaces of a tooth, residual, non-carious, intact tooth structure may be less. Carious excavation with or without specific cavity preparation leaves the tooth with unfavorable or poor resistance form.
This may lead to a fracture of the tooth involving undermined marginal ridges. These marginal ridges are better rehabilitated with an SSC than with amalgam restoration.
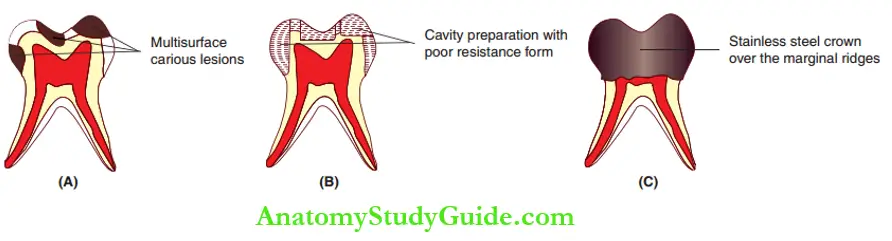
- (A) Multisurface carious lesion.
- (B) Poor resistance form due to caries excavation without specific cavity preparation.
- (C) Stainless steel crown rehabilitation on the marginal ridges.
3. Teeth with developmental defects:
The enumerated developmental disturbances of teeth decrease the abrasion resistance, necessitating the placement of a full-coverage crown.
- Single tooth hypoplasia (Turner’s hypoplasia)
- Molar-incisal hypoplasia
- Enamel hypoplasia
-
- Hereditary type – amelogenesis imperfecta
- Non-hereditary type – dental fluorosis
- Abnormalities in the dentin–dentinogenesis imperfect
Dental caries spreads faster on hypoplastic teeth owing to their poor matrix quantity/quality. Initiation of caries can be prevented on such teeth by full coverage crown rehabilitation.
4. Support for space maintainers or habit-breaking appliances:
A case where the first primary molar has been extracted prematurely for unknown reasons is discussed in depicted. It also shows a palpably involved second primary molar tooth. A pulpectomy is done and the tooth is restored.
The crown fabricated on the restored tooth supports the loop of the space maintainer employed in place of the extracted primary first molar.
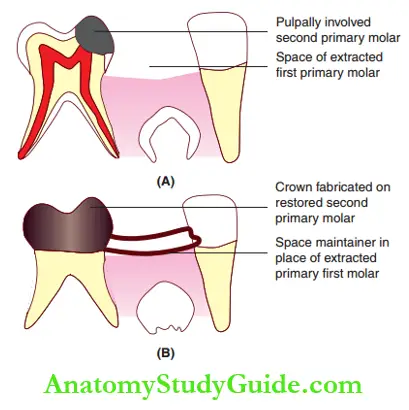
- (A) Pulpally involved second primary molar.
- (B) Crown on the second primary molar supports the loop of the space maintainer for the prematurely extracted first primary molar.
5. En masse cuspal fracture of primary teeth: Traumatic dental injuries lead to en masse cuspal fracture as in Ellis class 9 fractures. Full anterior SSC rehabilitation is the treatment of choice in such cases.
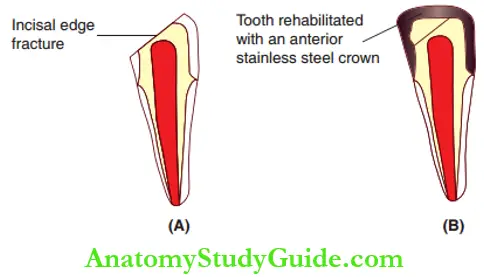
- (A) Primary incisor with incisal edge fracture.
- (B) Full anterior stainless steel crown rehabilitation.
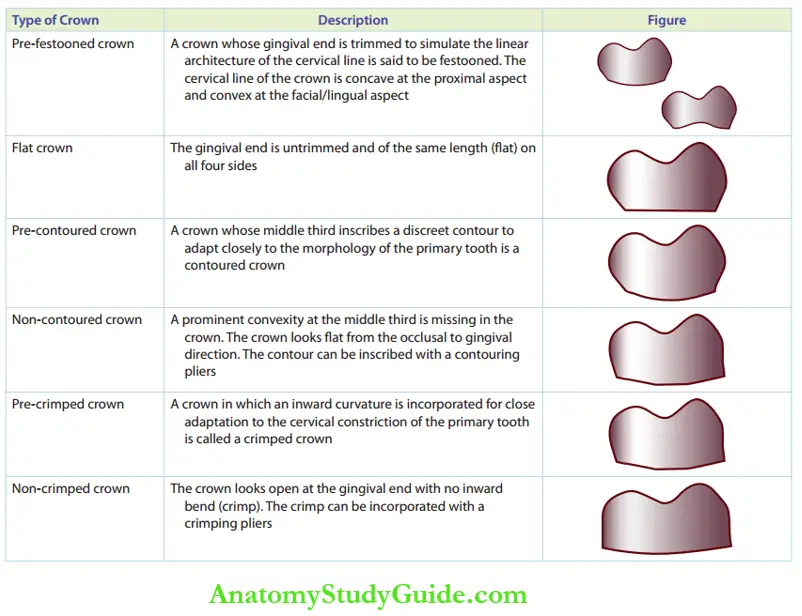
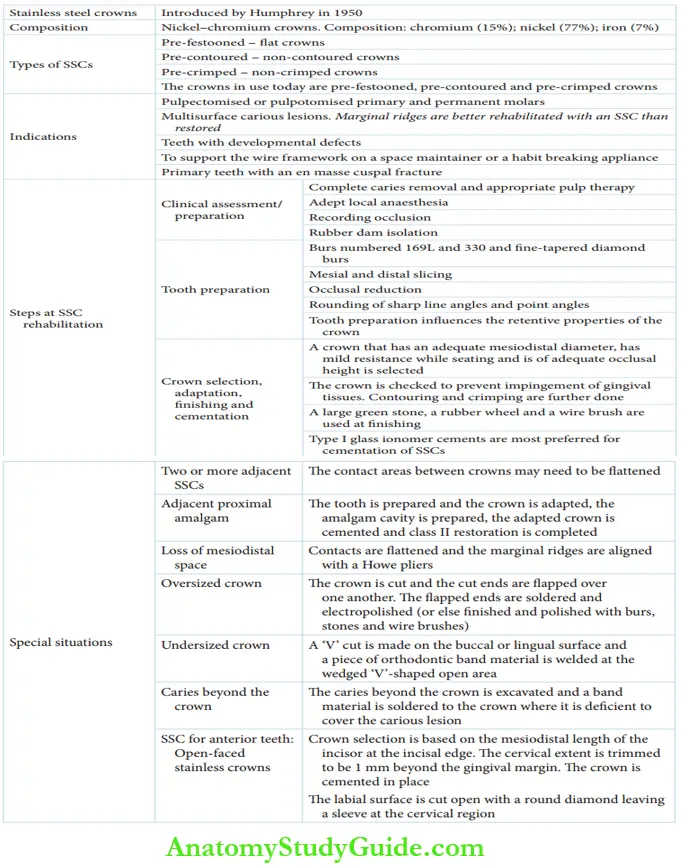
Stainless Steel Crowns Types
The various types of SSCs are described in Table. The crowns mostly used today are festooned, pre-contoured, and pre-crimped. Festooning is inscribing the cervical margin on the crown. Contouring refers to simulating the convexity of the middle third of the tooth.
Crimping is the inward adaptation of the cervical margin to the cervical constriction. These are the three steps to customize a crown to fit a tooth accurately. Only fier adjustments/adaptation is required on such crowns.
Types of Stainless Steel Crowns
Rehabilitation With Stainless Steel Crowns
SSCs commonly used today require little adaptation as they are pre-contoured, pre-trimmed (pre-festooned), and pre-crimped. The rehabilitation of a tooth with an
SSC involves the following three steps:
- Clinical assessment and preparation for anesthesia and isolation
- Tooth preparation
- Crown selection, adaptation, finishing, and cementation
Clinical Assessment And Preparation For Anaesthesia And Isolation
The extent of the carious lesion of the tooth is assessed and complete caries excavation is done. SSCs are best adapted under local anesthesia. If pulp therapy is indicated in some cases, it is prudent to complete both procedures in one visit under local anesthesia.
The occlusion of a pediatric patient is recorded with alginate or a heavy body elastomeric impression material. It serves as a guide for preventing occlusal alteration during crown cementation.
Rubber dam isolation is preferred before proceeding further due to the following reasons:
- To prevent trauma to the surrounding tissue
- To enhance visibility with better adaptation
- To prevent swallowing or aspiration of crowns during removal or insertion of trial fit
The interseptal rubber dam sheet can be cut or a larger hole punched for the distal tooth to prevent hindrance by the rubber dam during tooth preparation or crown cementation.
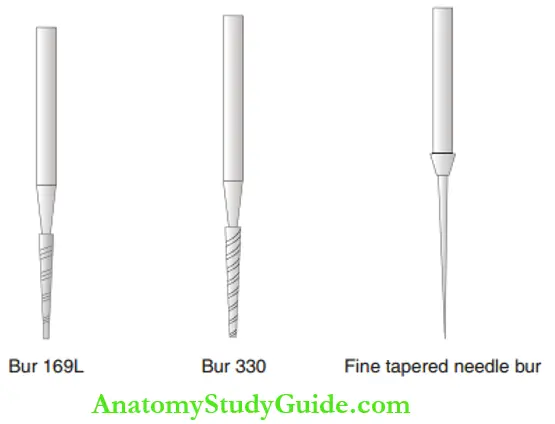
Tooth Preparation
Tooth preparation influences the retentive properties of the crown. Burs numbered 169L and 330 and fie-tapered diamond burs are the rotary instruments required for tooth preparation.
These discrete steps have to be followed during tooth preparation.
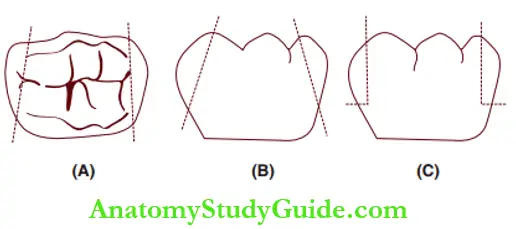
Step 1: Mesial and distal slicing
Step 2: Occlusal reduction
Step 3: Rounding of sharp line angles and point angles
Mesial and Distal Slicing
Mesial and distal contacts of the tooth are sliced with a no. 169L bur sufficiently to open the contacts completely. The depth of slicing extends beyond the contact point or till interproximal caries, whichever is deeper, and to the buccal and lingual line angles.
The slicing should be at an angle to the long axis of the tooth and parallel to the proximal surfaces.
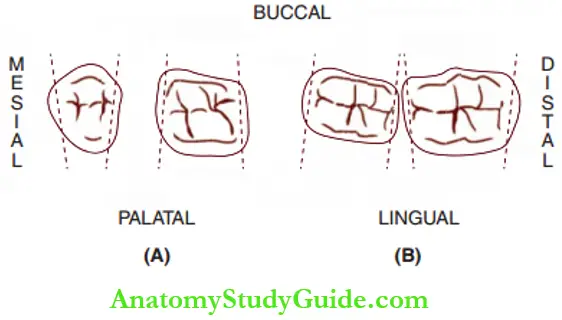
- (A) Maxillary molars.
- (B) Mandibular molars.
Three common errors may occur during proximal slicing. The slicing may not be parallel to the proximal surface, leading to improper angulation. An exaggerated taper may cause over-reduction of the occlusal end. In these two cases, the fitting of the selected crown may be loose and not snap-fi.
Excessive reduction may also lead to a pulpal response in vital teeth. Sometimes, the proximal slicing may not extend beyond the contact point and may be associated with over-reduction in the middle third.
A butt joint (right angle) is created and this is called shoulder formation. In this case, the crown cannot slip beyond the contact, where it has to be seated.
- (A) Improper angulation.
- (B) Excessive taper.
- (C) Shoulder formation.
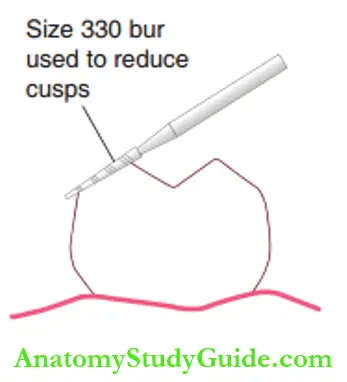
Occlusal Reduction
Occlusal reduction is done with a no. 330 bur and functional cusps are reduced by 1.5–2 mm and non-functional cusps by 1–1.5 mm. The reduction can be confirmed by comparison with the adjacent marginal ridges.
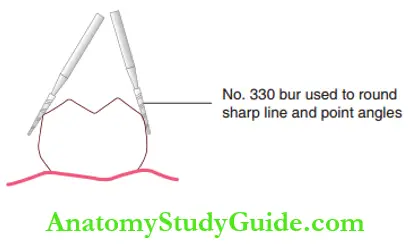
Rounding of Sharp Line Angles and Point Angles
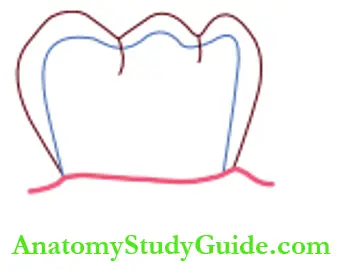
All sharp line angles and point angles are rounded with a no. 330 bur. The tooth preparation is completed with this depicted.
There is very minimal or no specific tooth preparation required on the buccal and lingual sides except for the reduction of an excessively large buccal bulge in the first primary mandibular molar.
Crown Selection, Adaptation, Finishing, And Cementation
Tooth preparation is followed by a selection of an appropriate crown, adapting the same to fit the prepared tooth, finishing the trimmed surfaces, and cementation. When pre-festooned, pre-contoured, and pre-crimped crowns are used, very minimal adjustments/alterations are required.
Crown Selection
Crowns can be selected on a ‘trial mode’. A smaller crown cannot be fitted on a prepared tooth and a larger crown will rotate like a child on a merry-go-round. A crown of appropriate size seats with slight resistance and does not rotate on the tooth.
The ideal size for a crown can be chosen according to the following parameters:
- Has an adequate mesiodistal diameter
- Has mild resistance while seating
- Is of adequate occlusal height
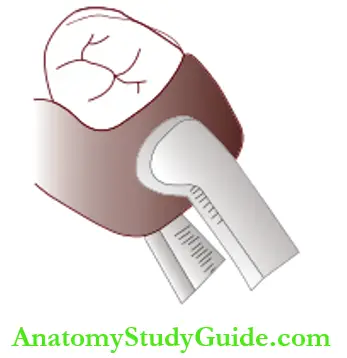
A vernier caliper or a divider can be used to measure the mesiodistal diameter of the tooth.
Crown Adaptation
The following procedures are carried out to adapt the crown to the prepared tooth.
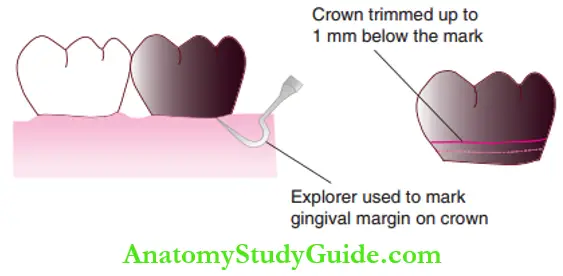
1. Trimming:
The chosen crown is seated on the tooth. The gingival margin is marked on the crown with an explorer. The crown is trimmed up to 1 mm below the mark. The trimmed crown is seated on the tooth and checked for blanching of the gingiva.
Blanching of gingiva implies that the crown is longer and requires more trimming. A well-adapted crown is self-cleansable and promotes good gingival health.
2. Contouring:
It incorporates a distinct convexity at the middle third of the crown facilitating the crown to adapt around the buccal convexity of the molar tooth. Crowns are usually pre-contoured. If the crown is non-contoured, Johnson Contouring Pliers No. 114 is used for contouring and adapting the crown to the tooth structure.
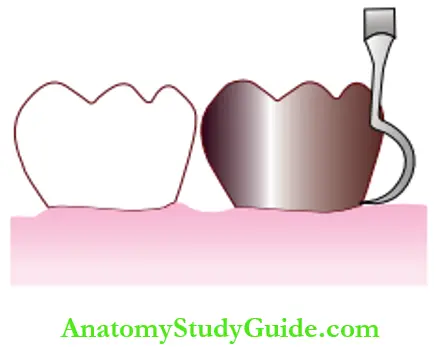
3. Crimping:
This fits the crown into the undercut of the cervical constriction of the tooth. No. 800-417 crimping pliers are used to give a gentle crimp along the gingival margin. The crimping must be smooth around the tooth, the margins of which can be checked with the help of an explorer.
It gives good gingival adaptation and maintains gingival health. Crimping also prevents the flow of luting cement into the crevicular space.
Crown Finishing
A large green stone is used to give a knife edge margin to the crown. A rubber wheel is used to smoothen and polish the margins and a wire brush is used to polish the entire crown. The rubber dam is then removed to check occlusion.
Cementation
Zinc phosphate, reinforced and conventional zinc oxide eugenol, and polycarboxylate cement have been used for crown cementation. However, type 1 glass ionomer cement is the most preferred choice for the cementation of SSCs.
This is due to its optimal physical and manipulative properties, biocompatibility, thermal and viscoelastic properties, and anti-cariogenic and remineralizing properties.
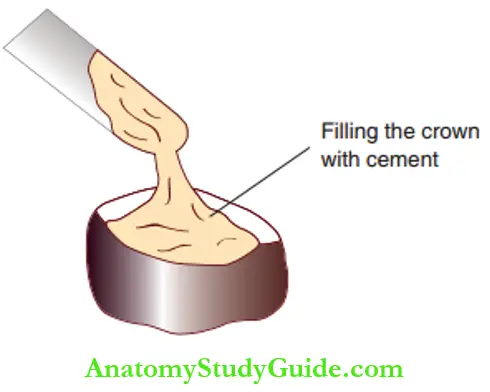
Under adequate isolation (by replacing the rubber dam), the finished crown is filled with mixed cement and seated on the prepared tooth from the lingual to the buccal side under firm finger pressure.
After the initial set, the excess cement on the buccal and lingual sides is removed with a probe/explorer. Knotted floss is passed from the buccal to the lingual sides to remove excess cement from the mesial and distal sides.
The excess cement, if left undisturbed, can cause gingival inflammation and persistent discomfort.
2. Modifications/Special Situation With Stainless Steel Crowns
Diffrent clinical situations warrant modifiations inm the SSC. The following modifications are possible in an SSC.
Adjacent Stainless Steel Crowns
When two or more crowns have to be placed adjacent to each other, the following points are taken into consideration:
- Pulp therapy (if required), tooth preparation, crown adaptation, and cementation are done at the same time for the adjacent crowns.
- The contact areas between crowns may have to be flattened with Howe pliers before cementation.
- The marginal ridges are also aligned with aHowe pliers.
Stainless Steel Crown And Adjacent Proximal Amalgam Restoration
When an SSC and a proximal amalgam restoration have to be fabricated adjacent to each other in a single appointment, the following schedule is followed:
- The tooth for SSC is prepared and the crown is adapted to the tooth.
- The class 2 cavity amalgam is prepared.
- The adapted crown is cemented.
- Class 2 restoration is completed.
Loss Of Mesiodistal Space
Mesiodistal space may be lost due to proximal caries. With conventional tooth preparation and appropriate crown selection, the crowns will fit one tooth. When more than one tooth is involved proximally, crowns cannot be placed together due to the loss of arch length.
Hence, greater tooth reduction is required. One of the teeth may require a smaller crown and the other may require a normal-sized crown. Contacts are flattened as depicted and the marginal ridges are aligned with Howe pliers.
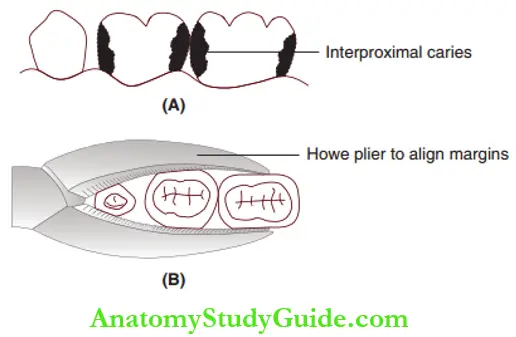
- (A) Loss of arch length due to interproximal caries.
- (B) Aligning of marginal ridges with Howe pliers.
Oversized Crown
The following steps are undertaken to fit a larger crown on a smaller tooth:
- The selected crown is cut on the buccal or lingual surface from the cervical to the occlusal surface.
- The cut ends are flapped over one another, thus making the crown smaller.
- The flapped ends are soldered and electropolished (or else finished and polished with burs, stones, and wire brushes).
- The crown is tried on the tooth.
- It is festooned, contoured, and crimped.
- It is cemented after rechecking marginal adaptation.
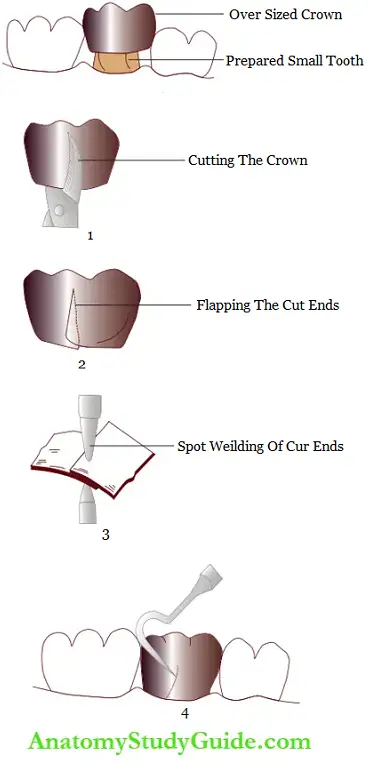
- (A) The larger crown and the smaller prepared tooth.
- (B) The cut is made on either the buccal or the lingual surface.
- (C) The crown is placed on the tooth and cut ends are flapped to adapt to the tooth.
- (D) The flapped ends are spot welded.
- (E) The crown is tried on the tooth.
Undersized Crown
The following steps are undertaken to fit a smaller crown on a larger tooth:
- A ‘V’ cut is made on the buccal or lingual surface of the selected crown.
- The crown is then tried on the tooth.
- A piece of orthodontic band material is welded at the ‘V’ cut area.
- The crown is then tried on the tooth, finished, and polished.
- The crown is festooned, contoured, and crimped.
- The crown is cemented after checking the marginal integrity.
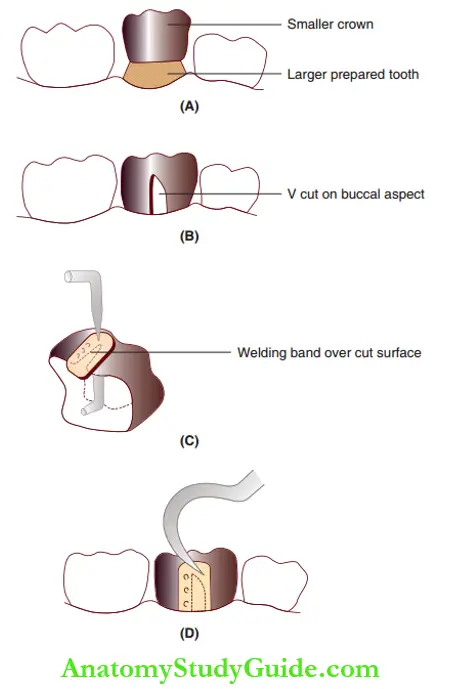
- (A) A small crown and a large prepared tooth.
- (B) A ‘V’ cut is made on the buccal surface and the crown is adapted to the tooth.
- (C) A piece of band material is welded to cover the opened area of the crown.
- (D) The altered crown is tried on the tooth.
Caries Beyond The Crown
The caries beyond the crown are excavated and a band material is soldered to the crown where it is deficient to cover the carious lesion. Alternatively, a non-trimmed crown with long shoulders can also be indicated in this situation.
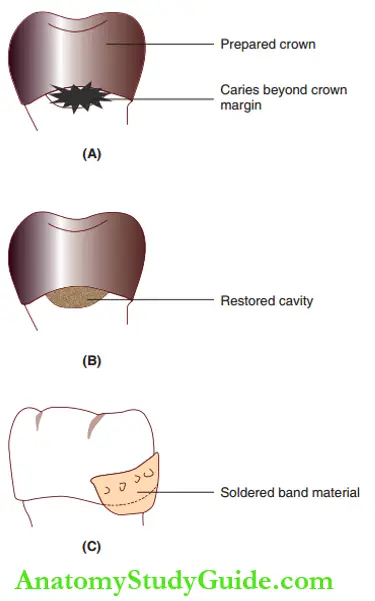
- (A) Caries beyond the conventional crown margin.
- (B) Caries excavated and cavity restored.
- (C) Band material soldered over the crown to cover the restored cavity.
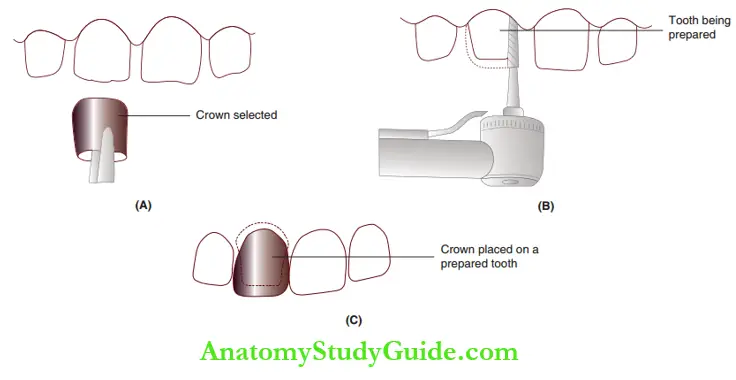
Stainless Steel Crowns For Anterior Teeth
SSCs for anterior teeth are dispensed in a box with serially increasing mesiodistal diameters. Crown selection is based on the mesiodistal length of the incisor at the incisal edge.
The cervical extent is trimmed so that it is 1 mm beyond the gingival margin, uniformly simulating the cervical line. The crown is cemented in place. The labial surface is cut open with a round diamond leaving a sleeve at the cervical region. These are called ‘open-faced stainless crowns’.
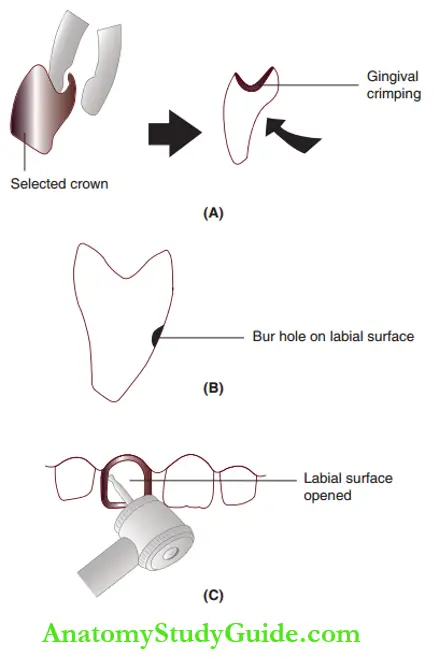
- (A) Gingival crimping done on the selected crown.
- (B) Bur hole made on the labial surface.
- (C) Complete labial surface is opened.
Cellulose Acetate Strip Crowns
Anterior teeth rehabilitation may be done with polycarbonate crowns. It is described in the following text but is not in use nowadays. Crown form templates are used to plaster composite resin to simulate the anterior tooth. The crown form templates are made of cellulose acetate.
Cellulose acetate strips are hence transparent crown forms and not true crowns such as polycarbonates. They are also called clear crown forms. The templates help in forming an anterior tooth crown with intricate morphological features incorporated into it.
The crown forms are available in different sizes and dispensed in a box along with SSCs for anterior teeth. Sequential sizes vary with increasing mesiodistal dimension at the incisal edge of the crown form.
Cellulose Acetate Strip Crowns Indications
With the advent of cellulose acetate strip crowns, SSCs are not used for anterior tooth rehabilitation. So, the indications of strip crowns are the same as for SSCs.
- Multisurface carious lesion of primary anterior teeth
- Pulpectomised/pulpotomies primary anterior teeth
- Primary anterior teeth with developmental defects
- Rehabilitation With Cellulose Acetate Strip Crowns
Three steps in the rehabilitation of cellulose acetate strip crowns are as follows:
- Crown form selection and preparation
- Tooth preparation
- Crown placement
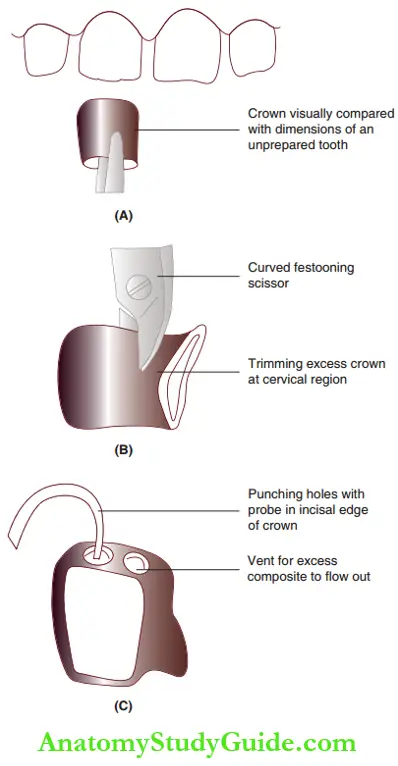
Crown Form Selection and Preparation
The crown form is selected by visual comparison with the mesiodistal dimension of the unprepared tooth. Curved festooning scissors are used to trim the excess crown form in the cervical region. A sharp probe is used to punch holes in the incisal edge of the crown. The holes act as a vent for the excess composite material to flow out.
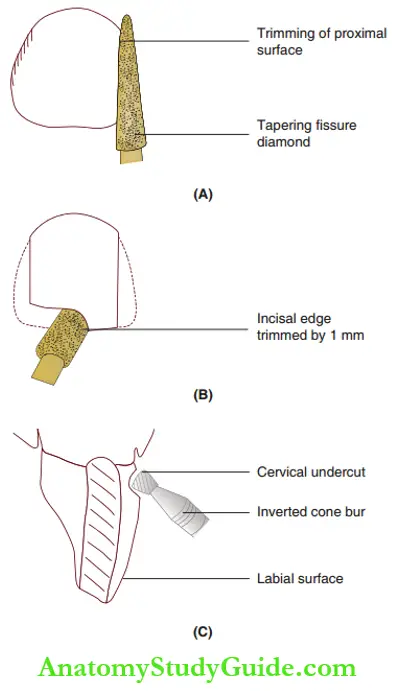
Tooth Preparation
The proximal surfaces are trimmed with a pouring fissure diamond producing a knife-edge finish line at the cervix. The incisal edge is reduced by 1 mm. All sharp line angles are rounded. Buccal and lingual surfaces may require minimal reduction.
A cervical undercut is placed at the gingival margin on the labial surface with an inverted cone bur. Further reduction is done to fit the selected crown form on the tooth. The remaining carious dentin is removed by a spoon excavator.
If the tooth is not pulp customized, medicament such as calcium hydroxide is placed on the excavated areas.
Crown Placement
The prepared crown form is trial-fitted to check if it is 1 mm beyond the gingival margin. The entire tooth surface is etched with 37% phosphoric acid gel and rinsed. A bonding agent is applied to the etched surfaces. The crown form is packed with composite without void entrapment.
The packed crown form is fitted onto the prepared tooth surface. Polymerization is completed. The crown form is removed by slicing it on the lingual surface with a scaler and peeling it off the polymerized crown.
The labial surface requires no finishing as the polymerization of the resin against a plastic surface gives the smoothest and stain-resistant finish.
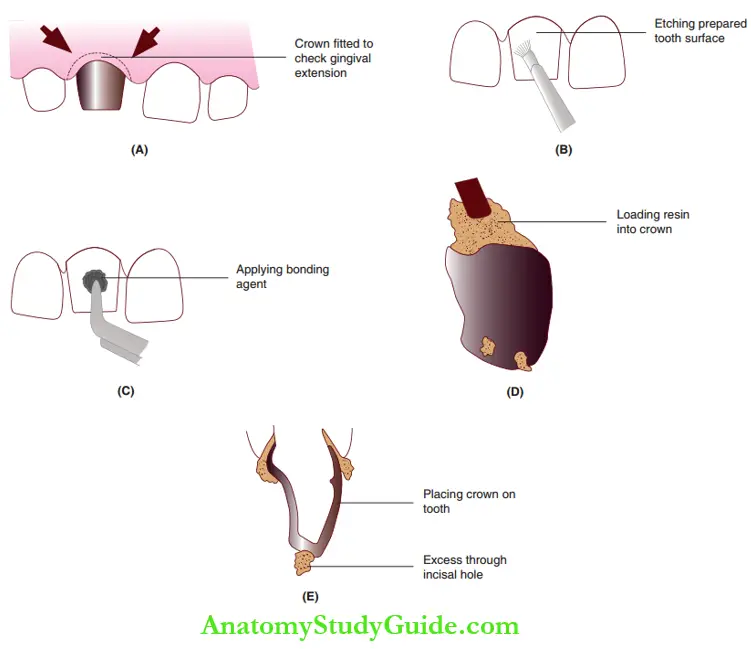
- (A) The selected crown is trial fitted to check gingival extension.
- (B) Etching of the prepared tooth surface.
- (C) Application of the bonding agent.
- (D) Loading composite resin into the crown form.
- (E) Placement on the tooth with excess expressed through the incisal holes.
Polycarbonate Crowns
Polycarbonate crowns are tooth-colored, pre-fabricated crowns indicated for primary anterior teeth. They are available in increasing sizes and are selected on the basis of increasing mesiodistal measurements. They are not in use in current practice.
Tooth preparation is similar to that of cellulose acetate strip crowns. The selected crown can be trimmed by stone burs, polished with pumice, and luted with glass ionomer cement.
- (A) Selection of an appropriately sized crown coherent with the mesiodistal dimension of the tooth.
- (B) Tooth preparation.
- (C) Cementation of the crown in place.
Summary
1. Full-coverage restorations or crowns meant to rehabilitate compromised tooth structures are called semipermanent restorations.
They are best expected to serve for an average span of 2–5 years, hence called ‘semipermanent’. They can be SSCs, cellulose acetate strip crowns, and polycarbonate crowns.
2. Indications of full-coverage restorations:
- Grossly carious primary tooth (incisor or a molar with carious involvement of three or more surfaces)
- Pulpotomised/pulpectomised primary teeth
- Teeth that have developmental defects such as enamel hypoplasia/dentinogenesis are prone to undergo rapid wear and tear.
3. Stainless steel crowns
4. Rehabilitation of anterior teeth can be done with cellulose acetate strip crowns and polycarbonate crowns apart from open-faced SSCs.
5. Cellulose acetate strip crowns (clear crown forms)
- Cellulose acetate or ‘clear’ crowns are transparent crowns that are ‘crown forms’ rather than true crowns.
- Indications
- Multisurface carious lesion of primary anterior teeth
- Pulpectomised/pulpotomies primary anterior teeth
- Primary anterior teeth with developmental defects
6. Polycarbonate crowns
- Polycarbonate crowns are tooth-colored prefabricated crowns for primary anterior teeth.
- Tooth preparation is similar to that of strip crowns.
Leave a Reply