Skin
Question 1. Discuss in detail the pathogenesis and morphology of malignant melanoma.
Answer:
Pathogenesis
- Autosomal dominant transmission
- Predisposing environmental factor: Ultraviolet radiation (UVR) resulting in DNA damage
Molecular genetics
1. Mutations that disrupt cell cycle control genes
- Loss of p16/INK4a expression and CDK4 mutations
2. Increase in RAS and PI3K/ AKT signaling and BRAF mutations
3. Mutations that activate telomerase
TERT mutation leads to the reactivation of telomerase activity
Read and Learn More Preparatory Manual of Pathology Question and Answers
Morphology
- Melanomas appear as shades of black, brown, red, dark blue, and gray lesions with irregular and often notched-up borders
- Radial growth phase: Horizontal spread of melanoma within the epidermis and superficial dermis
- Vertical growth phase: Tumor cells invade downward into the deeper dermal layers as an expansile mass
- Tumor cells are larger than normal melanocytes and have large nuclei with irregular contours
- The nuclear chromatin is clumped at the periphery of the nuclear membranes, with prominent eosinophilic nucleoli
Read and Learn More Preparatory Manual of Pathology Question and Answers
Question 2. Discuss the prognostic factors and clinical features of malignant melanoma.
Answer:
I. Prognostic factors
1. Tumor depth (Breslow thickness)
- Distance from the superficial epidermal granular cell layer to the deepest intradermal tumor cells
- The probability of metastasis correlates with the depth of invasion
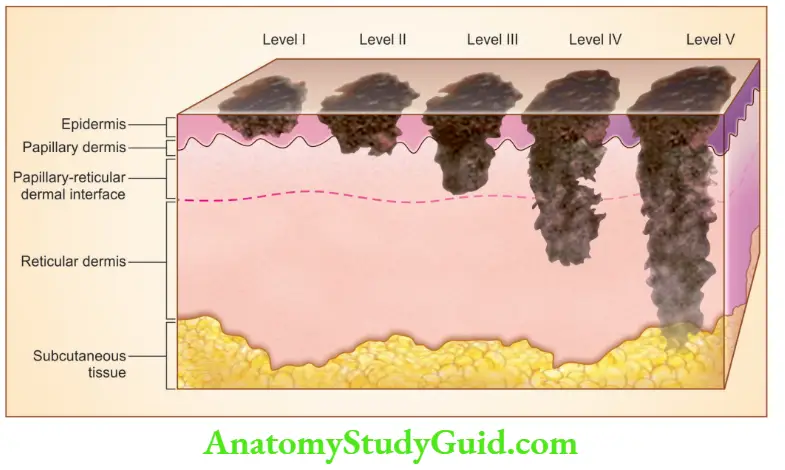
The level of invasion is assessed by Clarke’s five-level:
Level I: Intro-epidermal (in situ) melanocytes
Level II: Extension of melanoma cells in the papillary dermis
Level III: Melanoma cells fill the papillary dermis and stop at the interphase between the papillary and reticular dermis
Level IV: Melanocytes invading the reticular dermis
Level V: Invades the subcutaneous fat
2. Mitosis: Less mitotic index is a favorable prognostic factor
3. Tumor regression (due to the host immune response): Absence of regression indicates a good prognosis
4. Ulceration of the overlying skin: Lack of ulceration is a favorable prognostic factor
5. Presence and number of tumor-infiltrating lymphocytes and a brisk tumor-infiltrating lymphocyte response indicates a favorable prognosis
6. Sentinel lymph node biopsy: Microscopic involvement of a sentinel node by a small number of melanoma cells (micrometastases) confers a worse prognosis
II. Clinical features (warning signs. ABCDE of melanoma)
- Asymmetry
- Irregular borders
- Variegated color
- Increasing diameter
- Evolution or change over time
Question 3. Discuss the pathogenesis and microscopic features of basal cell carcinoma.
Answer:
Basal cell carcinoma
- Slow-growing, locally aggressive cutaneous tumor, that rarely metastasizes
Pathogenesis
- Associated with nevoid basal cell carcinoma syndrome: Basal cell carcinoma, medulloblastomas, ovarian fibromas, jaw cysts
- NBCCS and basal cell carcinoma patients have a loss of function mutations of the tumor suppressor gene PTCH
Morphology
Gross
- Presents as pearly papules with prominent dilated sub-epidermal blood vessels (telangiectasias)
- Rodent ulcers: Advanced lesions may ulcerate, and extensive local invasion of the bone or facial sinuses may occur
Microscopy
- Tumor cells resemble the basal cell layer of the epidermis
-
- Multifocal growth pattern: Tumor cells proliferate superficially in the epidermis
- Nodular growth pattern:
- Basophilic tumor cells grow deep into the dermis and are arranged in cords and islands
- Tumor cells have hyperchromatic nuclei and are embedded in a mutinous matrix, surrounded by fibroblasts and lymphocytes
- Peripheral palisading of tumor cells is seen
- Retraction clefts occur when the stoma retracts away from tumor cells
Question 4. Write a note on the morphology of psoriasis.
Answer:
Morphology of psoriasis
- Site: Elbows, knees, scalp, lumbosacral areas, intergluteal cleft, and glans penis
- Early lesions: Dominated by the presence of small pustules and erythema
- Chronic lesions: Erythematous and covered by a characteristic silver-white scale
- Nail changes: Yellow-brown discoloration, with pitting, dimpling, and glycolysis
Microscopy
- Acanthosis (marked epidermal thickening), with elongation of rete ridges (appears like test tubes in a rack)
- Thinning or absent stratum granulosum
- Extensive parakeratosis
- Auspitz sign: Multiple, minute, bleeding points when the scale is lifted from the plaque (due to close proximity of dermal vessels to parakeratotic scale)
- Munro microabscesses: Neutrophils form small aggregates within the parakeratotic stratum corneum
Note:
- Koebner phenomenon: Psoriatic lesions can be induced in susceptible individuals by local trauma
Question 5. Write a short note on lichen planus.
Answer:
Lichen planus
- Self-limited disorder, resolves spontaneously in 1 to 2 years after onset
- Complication: Squamous cell carcinoma in chronic lesions
Morphology
- Pruritic, purple, polygonal, planar, papules, and plaques (6 Ps), seen on skin and mucosa
- Wickham striae: White lacelike pattern of lines on papules
- Sites: Extremities, wrists and elbows, glans penis
Microscopy
- Acanthosis, hypergranulosis, hyperkeratosis
- Interface dermatitis: Dense, continuous band-like infiltrate of lymphocytes along the demo-epidermal junction
- Dermoepidermal interface shows angulated zigzag contour (Sawtooth)
- Destruction of basal keratinocytes, which show degeneration, necrosis, and squamatization
- Colloid or Civatte bodies: Anucleate, necrotic basal cells
Question 6. Write a note on tuberculoid leprosy.
Answer:
Tuberculoid leprosy
- Neuronal involvement dominates tuberculoid leprosy
- Nerves become enclosed within granulomatous inflammatory reactions and are destroyed
- The patient presents with dry, scaly skin lesions that lack sensation
- There is asymmetric involvement of large peripheral nerves
- As the host immune response is strong, with resultant granulomatous inflammation, lepra bacilli are never found on microscopic examination, hence it is termed paucibacillary leprosy
Question 7. Write a note on lipomatous leprosy.
Answer:
Lepromatous leprosy
- Severe form
- Includes symmetric skin thickening and nodules
- Mycobacterium invades Schwann cells and into end-neural and perineal macrophages, with resultant damage to the peripheral nervous system
- Can involve skin, peripheral nerves, the anterior chamber of the eye, upper airways, testes, hands, and feet
- Lesions contain macrophage aggregates which are filled with masses (“globe”) of acid-fast bacilli
- On the face, nodular lesions coalesce to yield a distinctive leonine facies
Leave a Reply