Spleen Pancreas And Liver
Enumerate The Functions Of The Spleen and Give Two Causes Of Its Enlargement.
1. Spleen Pancreas And Liver Functions
Table of Contents
- Phagocytosis: The spleen is an important component of the reticuloendothelial system.
- Haemopoiesis: The spleen is an important haemopoietic organ during fetal life.
- Lymphopoiesis: The spleen continues throughout life.
- Storage of RBC
- Immune response: It increases the production of lymphocytes in chronic infection.
2. Spleen Pancreas And Liver Causes of enlargement
- Liver disease: Cirrhosis, hepatitis
- Acute or chronic infection: HIV, malaria, and tuberculosis
- Blood malignancy: Lymphoma, leukaemia.
Read And Learn More: General Histology Questions and Answers
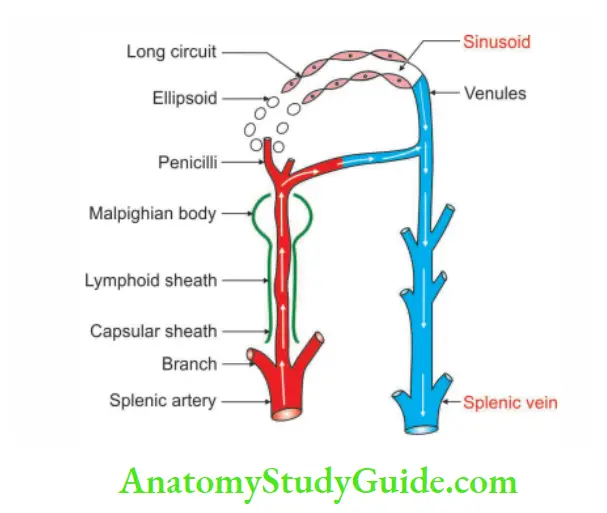
Blood Circulation In The Spleen
1. Splenic artery: The spleen is supplied by the splenic artery. It passes through the hilum of the spleen where it divides into 5 or more branches.
Within the spleen, these branches divide repeatedly and form straight vessels called penicilli.
The penicilli divide into ellipsoids and arterial capillaries.
The course of the blood is controversial
Closed theory of splenic circulation: The capillaries are continuous with the venous sinusoids that lie in the red pulp. The sinusoids join together to form veins.
Open theory of splenic circulation: The capillaries end by opening into the red pulp. In the red pulp, blood enters the sinusoids through their walls.
Compromise theory: Where the circulation is open in distended spleen and closed in the contracted spleen.
2. Purpose:
The splenic circulation is adapted for the mechanism of separation and storage of the red blood cells. On the basis of its blood supply, the spleen is said to have
Superior and inferior vascular segments. The two segments are separated by an avascular plane. Each segment may be subdivided into 1 to 2 disc-like middle segments and a cap-like pole segment.
Question – 1: Describe Spleen under the following heads
1. Spleen Gross anatomy
2. Spleen Histology
3. Spleen Development, and
4. Spleen Applied Anatomy.
Answer:
1. Spleen Gross anatomy
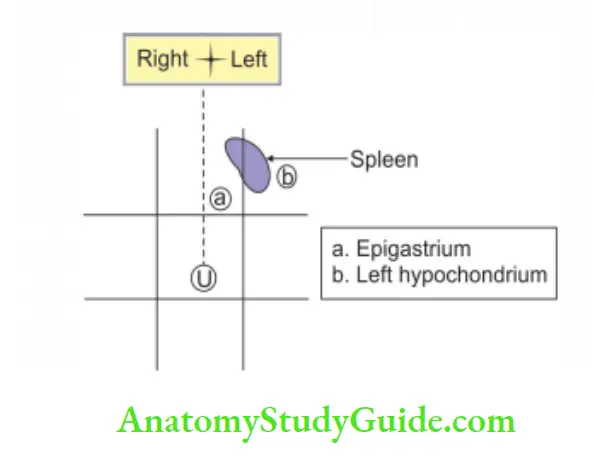
1. Spleen Location:
Spleen occupies:
- Mainly in the left hypochondrium.
- Partly in the epigastrium.
Spleen Shape: Wedge-shaped.
![]()
Spleen Dimension: Rule of odd numbers 1,3,5,7,9,11
- 1″ thick.
- 3″ width.
- 5″ length.
- 7 ounce (1 ounce = 30 g) 7 x 30 = 210 g weight.
- The 9th to 11th ribs are related to the spleen.
Spleen Axis: Oblique, downward, forward and laterally
2. Spleen External features:
2 ends:
- The anterior end is expanded and reaches the mid-axillary line.
- The posterior end is rounded and rests on the upper pole of the left kidney.
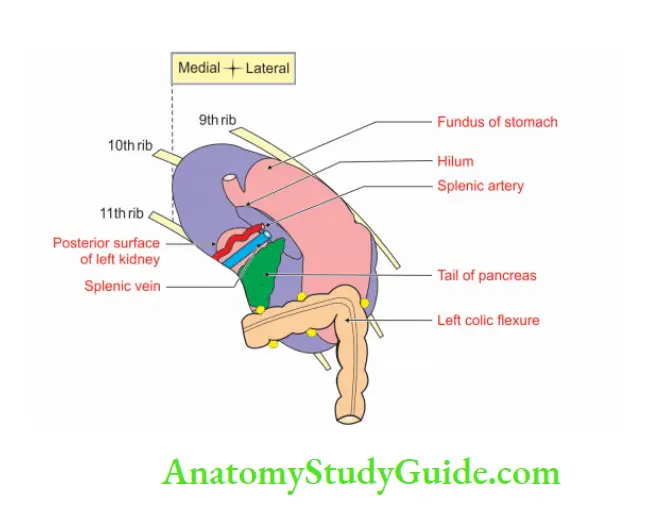
2 surfaces:
1. Diaphragmatic surface is convex and smooth.
2. Visceral surface is concave and irregular. It is occupied by many impressions.
- Gastric impression for the fundus of the stomach. It is the largest.
- Renal impression for the left kidney. It lies between inferior and intermediate borders.
- Colic impression for the splenic flexure, and
- The tail of the pancreas.
3 borders:
- The superior border is characteristically notched near the anterior end.
- The absence of a notch makes it difficult to identify borders, poles and surfaces.
- The inferior border is rounded.
- The intermediate border is also rounded.
Hilum: It lies on the anteromedial part of gastric impression along the long axis of the spleen.
3. Spleen Relations:
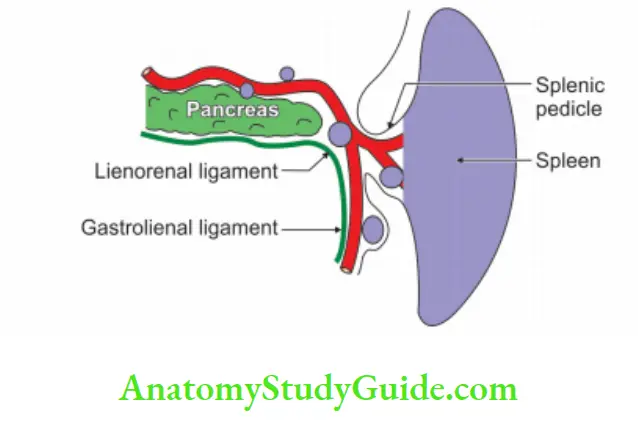
1. Peritoneal relations: Spleen is surrounded by 3. peritoneum and is suspended by following ligaments
- Gastrosplenic ligament
- Lienorenal ligament, and
- Phrenicocolic ligament.
- Visceral relations
2. The diaphragmatic surface is related to the inferior surface of the diaphragm.
3. Visceral surface is related to
- Fundus of the stomach
- The anterior surface of the left kidney
- Splenic flexure of the colon, and
- The tail of the pancreas.
4. Spleen Blood supply:
Arterial supply:
- The splenic artery is the largest tortuous artery.
- It breaks into 5 to 7 branches.
- It passes through the lienorenal ligament to supply the vascular segment of the spleen.
5. Spleen Venous drainage:
- It is drained by a splenic vein.
- It is formed at the hilum of the spleen.
- It joins the superior mesenteric vein behind the neck of the pancreas and forms the portal vein.
6. Spleen Nerve supply:
- They are derived from the coeliac plexus.
- They are mainly sympathetic in nature and are vasomotor in function.
- They also supply smooth muscle present in the capsule.
7. Spleen Lymphatic drainage:
- The splenic tissue has no lymphatics.
- A few lymphatics arise from the connective tissue of the capsule and trabeculae.
- They drain into the pancreaticosplenic group of lymph nodes, situated along the splenic artery.
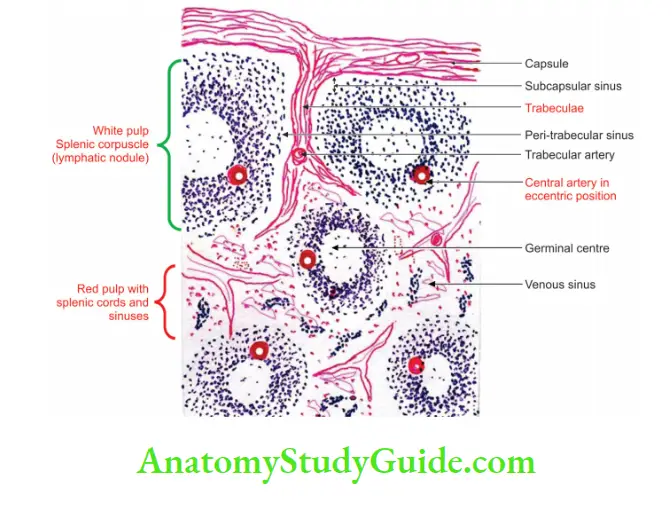
2. Spleen Histology
The section of the spleen shows
1. Serous coat, which is lined by simple squamous epithelium.
2. Fibroelastic coat consists of
- Fibrous coat: It sends trabeculae projecting into the substance of the spleen and branches to form a network.
- Elastic fibres: They are present in the capsule and trabeculae. These fibres bring contraction and relaxation of the spleen.
3. Splenic pulp: It is of two types depending upon the type of blood cells.
Red pulp:
1. It is scattered throughout the organ.
2. It is supported by a reticular network.
3. It is composed of
- Element of blood
- Debris of RBC
- Macrophages, and
- Reticuloendothelial cells.
White pulp:
- These are collections of lymphoid tissue, which are precursors of lymphocytes in the blood.
- The very striking point is an eccentric arteriole, a branch of the trabecular artery surrounded by lymphocytes.
- The germinal centre may be seen.
3. Spleen Development
Chronological age: It develops in the 5th week of intrauterine life.
Germ layer: Mesoderm.
Site: Dorsal mesogastrium near the posterior wall
Sources: Spleen is derived from the dorsal mesogastrium, not from the gut tube endoderm.
- Mesenchymal cells
- Cells of the coelomic epithelium.
Spleen Anomalies:
1. Abnormal formation: Accessory spleen.
2. Abnormal site:
1. In the derivatives of the dorsal mesogastrium:
- Gastrosplenic ligament
- Lienorenal ligaments
- Greater omentum.
2. In the broad ligament
3. In the spermatic cord.
3. Spleen:
The spleen develops as splenic lobules, which combine together and form an adult spleen.
However, the superior border fails to fuse; hence it demonstrates a notch on the superior border.
4. Spleen Applied anatomy
Palpation of the spleen: Normally spleen is not palpable. It is palpable when it is enlarged to about 3 times its normal size. The slightly enlarged spleen can be palpated in the left lateral position.
Splenomegaly: The enlargement of the spleen is called splenomegaly. It projects towards the right iliac fossa in the direction of the axis of the 10th rib.
Splenectomy: The surgical removal of the spleen is called splenectomy.
Splenic laceration: The spleen can be lacerated by a fractured rib. The laceration of this vascular organ is a fatal condition. Immediate splenectomy is sometimes indicated.
During splenectomy: The tail of the pancreas should be sought first, before putting ligatures to the pedicles of the spleen.
Relations of liver
They are divided into peritoneal and visceral.
1. Peritoneal relation: Most of the liver is covered by the peritoneum except for bare areas.
- There are five bare areas
- The bare area
- Groove for inferior vena cava
- Porta hepatis
- Fossa for gallbladder, and
-
 lar area on the superior surface between two layers of falciform ligaments.
lar area on the superior surface between two layers of falciform ligaments.
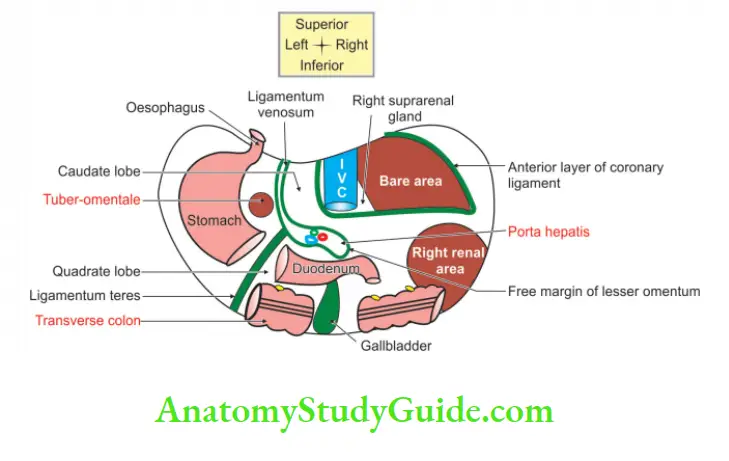
2. Visceral relation:
Anterior surface: It is related to
- Xiphoid process
- Anterior abdominal wall, and
- Tire diaphragm.
Posterior surface: It is lar. It is related to
- Vertebral column
- The diaphragm
- Right suprarenal gland
- Inferior vena cava, and
- Oesophagus
Superior surface: It is quadrilateral and is related to
- Heart, and
- The dome of the diaphragm.
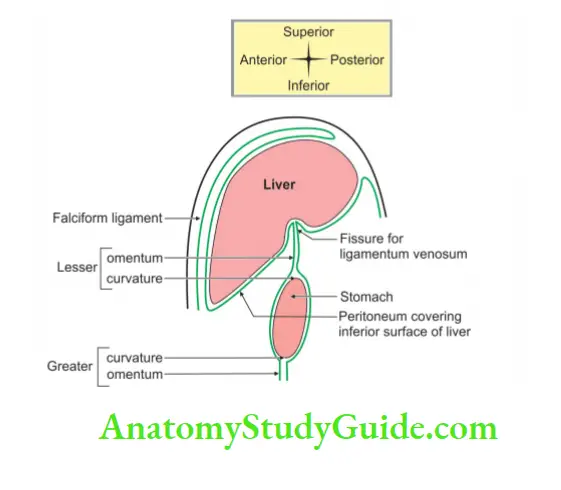
Inferior surface:
- Lesser omentum
- Impression for gallbladder
- Right suprarenal gland
- Right colic flexure.
- In porta hepatis, the relations are (from posterior to anterior) as follows:
- Portal vein (V)
- Hepatic artery, and (a)
- Hepatic duct (d)
The right lateral surface is related to: (D, DP and DPL)
- Lower one-third of the diaphragm.
- Middle one-third pleura and the diaphragm.
- Upper one-third lung, pleura and the diaphragm.
Portal lobule
1. It is based on the direction of the flow of bile.
2. It is large in shape.
![]()
3. Note: In the portal lobule, parenchyma surrounds the portal triad.
4. It has three central veins at the angle ![]() of and portal tract in the centre of
of and portal tract in the centre of ![]() .
.
5. The bile from the hepatocytes is collected into the bile duct.
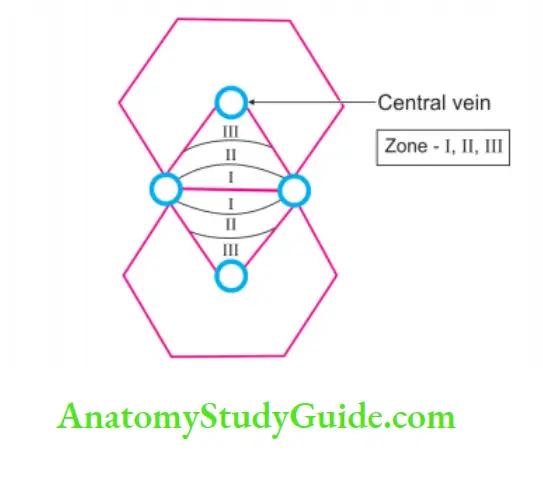
Acinus of liver
1. It is a functional unit of the liver.
2. It is diamond-shaped.
![]()
3. There are
- Two central veins at two opposite ends.
- Two portal triads at the other two opposite ends.
4. The acinus is divided into three zones according to the area of distribution of blood supply.
- Zone one: Closed to the blood vessels and well-oxygenated.
- Zone Two: Slightly away from the blood vessels and less oxygenated.
- Zone Three: Away from the blood vessels and poorly oxygenated
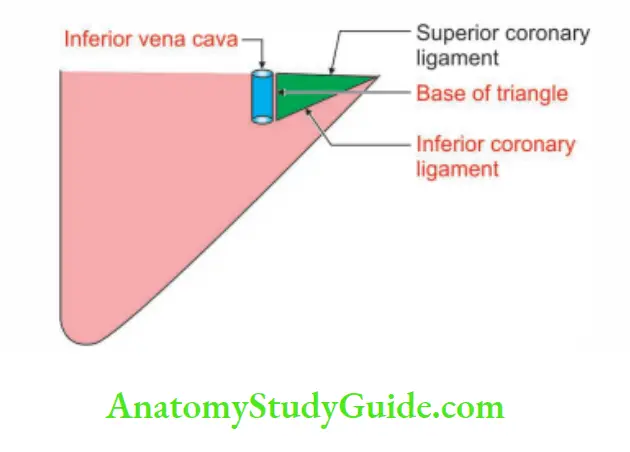
Bare areas of the liver
1. Areas of the liver which are not covered by the peritoneum are called bare areas.
2. There are five bare areas of the liver.
1. The bare areas of the liver:
- It is the largest area.
- It is present on the posterior surface of the right lobe.
- It is lar
 and presents the following boundaries.
and presents the following boundaries. - Apex: Right lar ligament.
- Base: Groove for inferior vena cava.
2. Upper and lower limits are formed by superior and inferior layers of coronary ligaments.
- The groove of the inferior vena cava
- Groove for porta heat
- Fossa for gallbladder
- Groove for ligamentum venosum
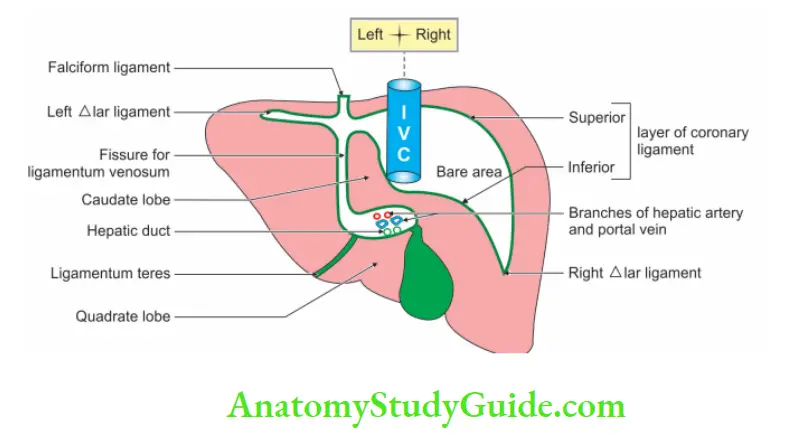
Lobes of liver
The liver is divided into two lobes: Anatomical and physiological lobes.
Anatomical lobes: The liver is divided into anatomical right and left lobes by the attachment of the
- Falciform ligament anteriorly and superiorly
- Fissure for the ligamentum teres inferiorly
- Fissure for the ligamentum venosum posteriorly.
1. The right lobe is much larger than the left lobe, and forms 5/6th of the liver. It contributes to all the five surfaces of the liver and presents the caudate and quadrate lobes.
The caudate lobe is situated on the posterior surface. The boundaries are:
- Right side by the groove for the inferior vena cava, on the.
- Left side by the fissure for the ligamentum venosum, and
- Inferior side by the porta hepatis.
The quadrate lobe is situated on the inferior surface and is rectangular in shape. The boundaries are:
- Anteriorly by the inferior border
- Posteriorly by the porta hepatis
- On the right by the fossa for the gallbladder, and
- Left by the fissure for the ligamentum teres.
2. The left lobe is 1/6th of the liver.
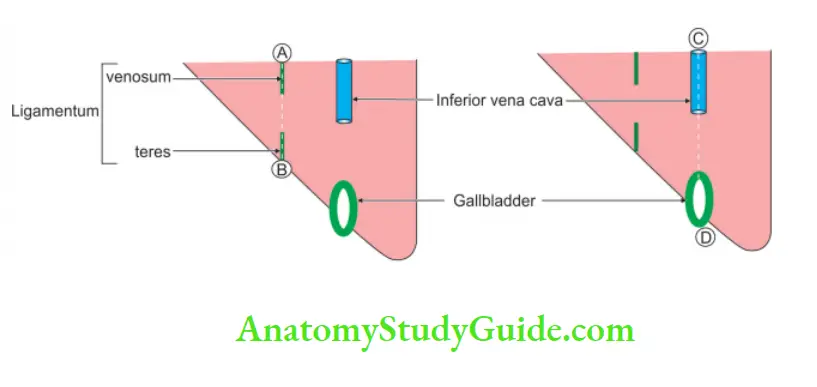
A – B – A vertical line passing through ligamentum venom to ligament teres divided the liver into anatomical right and left lobes.
C- D – The vertical line passing through the inferior vena cava and gallbladder divides the liver into left and right physiological lobes.
Question 2: Describe the liver under the following heads
1. Liver Gross anatomy
2. Liver Histology
3. Liver Development, and
4. Liver Applied Anatomy.
Answer:
Liver Introduction: It is the largest mixed gland in the body.
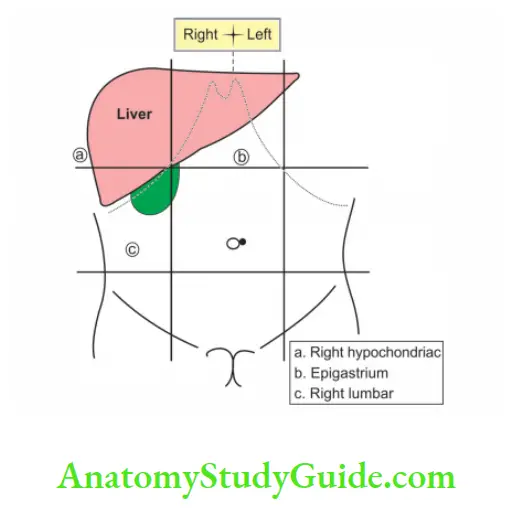
1. Liver Gross anatomy
1. Liver Location:
1. The liver is situated in the right upper quadrant of the abdominal cavity. It occupies
- The whole of the right hypochondrium.
- The greater part of the epigastrium.
- Left hypochondrium.
2. Liver Shape: Wedge ![]() shaped.
shaped.
3. Liver Weight: About 1500 g.
2. Liver External features:
5 structures each structure has 5 items.
1. 5 surfaces:
- Superior
- Inferior
- Anterior
- Posterior and
- Right lateral.
2. 5 borders: They are defined except the inferior border which is well defined.
3. 5 fissures: It is H shaped. Each limb of H indicates structure.
- Fissure for ligamentum teres
- Fissure for ligamentum venosum
- Groove for inferior vena cava
- Fossa for gallbladder, and
- Porta hepatis.
4. 5 lobes:
- Anatomical right and left lobes: The liver is divided by a line extending from falciform.
- The ligament to the ligamentum teres divides into anatomical right and left lobes.
- A vertical line passing through the Inferior vena cava and Gallbladder divides the Physiological right and left lobes of the liver. (IGP)
- Caudate lobe.
- Quadrate lobe.
- Riedel’s lobe: Sometimes a tongue-like projection arises from the lower border of the liver called Riedel’s lobe.
- It extends below the right costal margin.
5. Peritoneal ligaments:
- Falciform ligament
- Coronary ligament
- Right lar
 ligament
ligament - Left lar ligament
- Lesser omentum.
3. Relations:
Relations of the liver:
Relations on inferior and posterior surfaces of the liver:
4. Liver Blood supply:
Anenalsupply: The liver receives blood from two sources.
1. The oxygenated blood or arterial blood is received by the hepatic artery which divides into right and left branches in the porta hepatis.
2. The division is Y-shaped in contrast to the T-shaped division of the portal vein.
3. Venous blood is carried to the liver by the portal vein which is divided in the porta hepatis into right and left branches which in turn give segmental branches like the arteries.
4. This portal vein carries the products of digestion which are absorbed from the alimentary canal and get metabolized in the liver.
5. There is no communication between the right and left halves of the liver.
6. Even the arteries are end arteries within each half of the liver.
7. Hence, the right lobe shows toxic changes in ingested liver poison.
8. The left lobe shows cirrhotic changes.
Venous drainage: It is different from the arterial supply, there is the mixing of the venous blood of the right and left halves of the liver.
There are three main hepatic veins that drain into the inferior vena cava. The veins have no extrahepatic course.
5. Liver Nerve supply:
Sympathetic fibres arise from the coeliac ganglion. They run with the vessels in the free edge of the lesser omentum and enter the porta hepatis.
Parasympathetic fibres arise from the vagus nerve. The above nerves form the hepatic plexus in the porta hepatis.
6. Liver Lymphatic drainage:
1. Lymphatics of the liver drain into 3 or 4 hepatic nodes in the porta hepatis.
They drain downwards along the hepatic artery to the retropyloric nodes and to the coeliac nodes.
2. The lymphatics from the bare area drain into extraperitoneal lymphatics which perforate the diaphragm. They drain to the nodes in the posterior mediastinum.
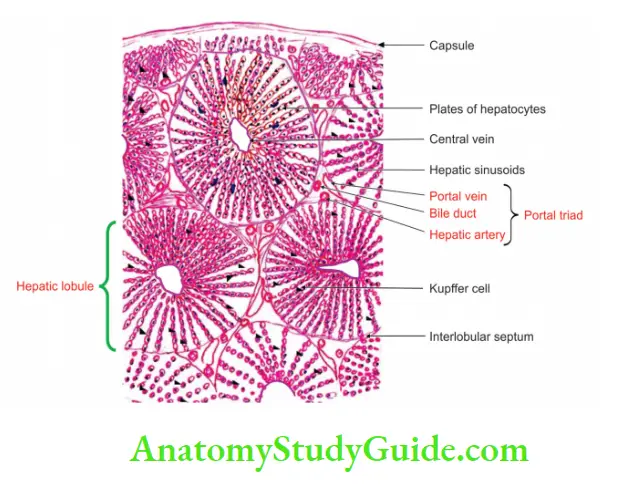
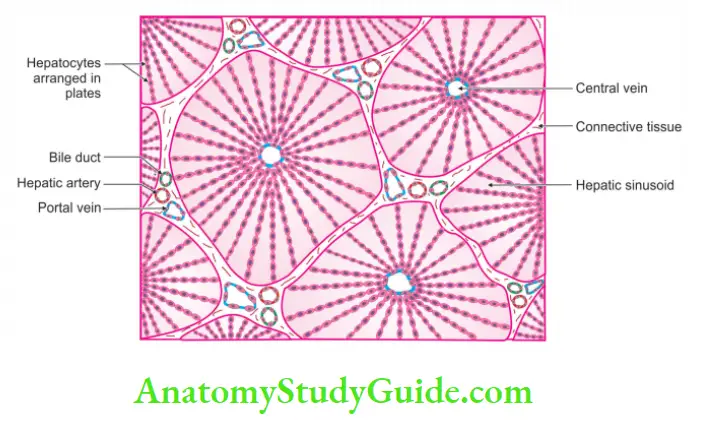
2. Liver Histology
1. The liver is made up of liver cells (hepatocytes) arranged in the form of hexagonal areas called hepatic lobules.
2. The lobules are separated by the connective tissue.’
Each lobule has a central vein and shows numerous sinusoids between the cords of hepatocytes.
3. Portal triad: Between the lobules, there are areas filled by connective tissue which contain
- A branch of the portal vein
- A branch of hepatic artery, and
- Interlobular bile duct.
4. There are phagocytic cells called Kuffer cells in the walls of sinusoids.
3. Liver Development
Chronological age: It develops in the 4th week of intrauterine life.
Germ layer: Hepatocytes develop from endoderm and the remaining structure develops from mesoderm.
Site: It develops in the ventral mesogastrium and septum transversum.
Source
1. It arises as a hepatic bud at the junction of the foregut and midgut.
2. It develops from an endodermal bud which arises from the ventral aspect of the gut (at the junction of foregut and midgut).
3. It grows into the ventral mesogastrium and passes through it into the septum transversum.
4. The endodermal cells of the hepatic bud give rise to parenchyma of the liver and to bile capillaries.
5. The mesoderm of the septum transversum forms the capsule and fibrous tissue of the liver.
Anomalies: They are rare
- Rudimentary left lobe
- Abnormal lobulation
- Reidel’s lobe
- Absence of quadrate lobe associated with absence of gallbladder
- Accessory lobe in falciform ligament
4. Liver Applied anatomy
1. The ligation of the right and left hepatic arteries does not usually lead to infarction of the liver.
2. This is because about 75% of total hepatic blood flow is derived from the portal vein. The remaining 25% comes from the hepatic artery.
3. The toxic substances are absorbed from the midgut. The vein of the midgut is a superior mesenteric vein.
4. It opens into the right lobe of the liver. Hence, the right lobe of the liver is susceptible to toxic changes.
5. The choline and methionine are water-soluble compounds.
6. They prevent the deposition of fat in the liver. They are absorbed through the midgut.
7. Very little is absorbed through the hindgut. Therefore, the left lobe of the liver is not protected by alcoholics.
8. Hence, the left lobe of the liver is susceptible to cirrhosis.
9. Amoebic liver abscess is more common in the right lobe of the liver.
10. Inflammation of the liver is referred to as hepatitis.
11. Under certain conditions, liver tissue undergoes fibrosis and shrinks. This is called cirrhosis of the liver.
Question 3: Describe the Head of the Pancreas under the following heads
1. Pancreas Gross anatomy
2. Pancreas Histology
3. Pancreas Development, and
4. Pancreas Applied anatomy
Answer:
Pancreas Introduction: It is the mixed gland situated in the upper part of the left abdomen.
1. Pancreas Gross anatomy
1. Pancreas Situation: It is situated in the C-shaped curvature formed by the 1st, 2nd, and 3rd parts of the duodenum.
2. Pancreas External features:
1 process: Uncinate process.
2 surfaces:
- Anterior, and
- Posterior.
3 borders:
- Superior
- Inferior, and
- Right lateral.
3. Relations:
Peritoneal:
- The upper part of the anterior surface is non-peritoneal and related to the transverse colon.
- The lower part is covered with peritoneum and is related to coils of jejunum.
- The posterior surface is non-peritoneal.
Visceral:
1. Uncinate process:
- Anteriorly: Superior mesenteric vessels.
- Posteriorly: Abdominal aorta.
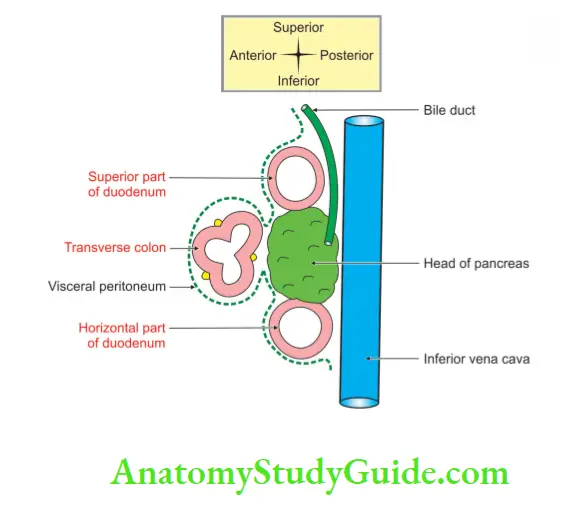
2. Surfaces:
Anterior surface:
- Near the middle: Transverse colon separated by areolar tissue.
- Above transverse colon: Overlapped by 1st part of duodenum.
- Below transverse colon: Coils of jejunum.
Posterior surface:
- Inferior vena cava.
- Bile duct: Runs downwards and to the right, embedded in the substance of the pancreas.
- Right crus of diaphragm.
- Terminal part of renal veins.
- Right middle suprarenal artery.
- Right sympathetic trunk.
- Bodies of L1, and L2 vertebrae with intervertebral discs.
Borders:
1. Superior border:
- 1st part of the duodenum, and Superior
- pancreaticoduodenal vessels.
2. Inferior border:
- 3rd part of duodenum, and
- Inferior pancreaticoduodenal vessels.
3. Right lateral border:
- 2nd part of duodenum
- Terminal part of the bile duct
- Anastomosis between superior and inferior pancreaticoduodenal vessels, and
- Pancreaticoduodenal lymph nodes.
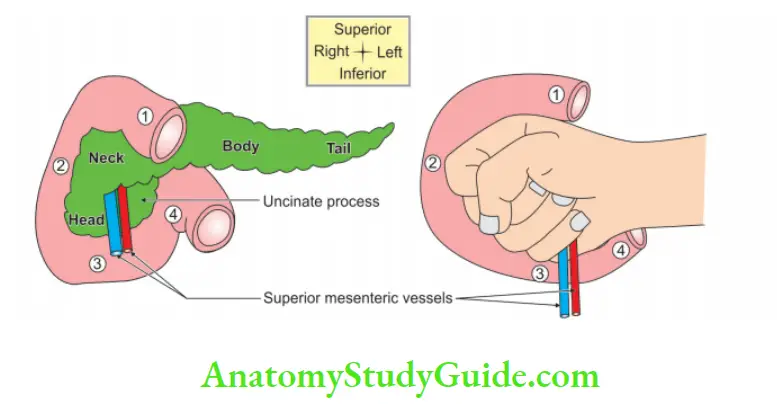
Relations of boards of the head of the pancreas with the 1st, 2nd, and 3rd, 4th part of the duodenum and superior mesenteric vessels
First and pancreas:
The relations between the duodenum and pancreas are best illustrated by Stephan Goldberg through the simile of a fist holding two straws.
The hand fist represents the body of the pancreas and the fingers signify the uncinate process.
The left straw of the 2 indicates superior mesenteric artery and the right straw signifies superior mesenteric vein.
The lower portion of the straw rests on 3rd part of the duodenum. The direction of the fist is towards 2nd part of the duodenum.
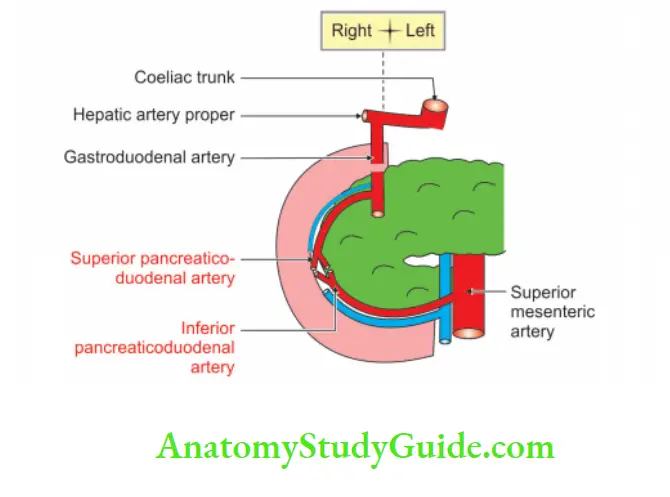
4. Pancreas Blood supply:
Arterial supply:
- The superior pancreaticoduodenal artery is one of the terminal branches of the gastroduodenal artery.
- The inferior pancreaticoduodenal artery is a branch of the inferior mesenteric artery
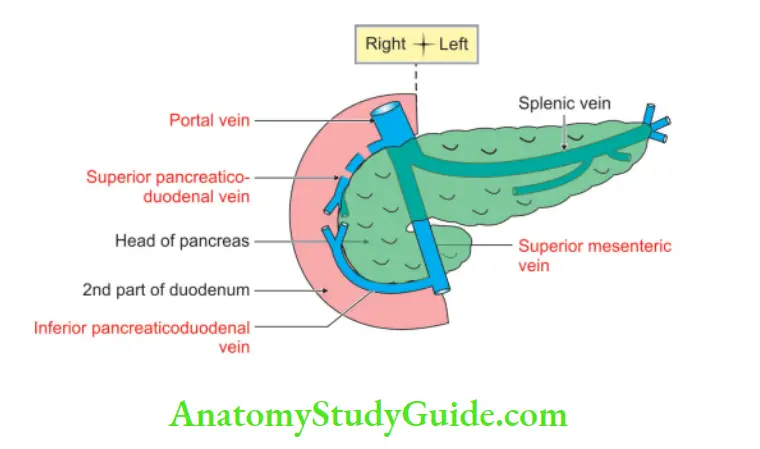
Venous drainage:
- The superior pancreaticoduodenal vein drains directly into the portal vein
- The inferior pancreaticoduodenal vein drains into a superior mesenteric vein. It joins with the splenic vein and forms the portal vein.
5. Pancreas Never supply:
- Sympathetic nerve: It is derived from coeliac and superior mesenteric plexus. It is vasomotor in function.
- Parasympathetic nerve: It is derived from the vagus nerve. It controls pancreatic secretion.
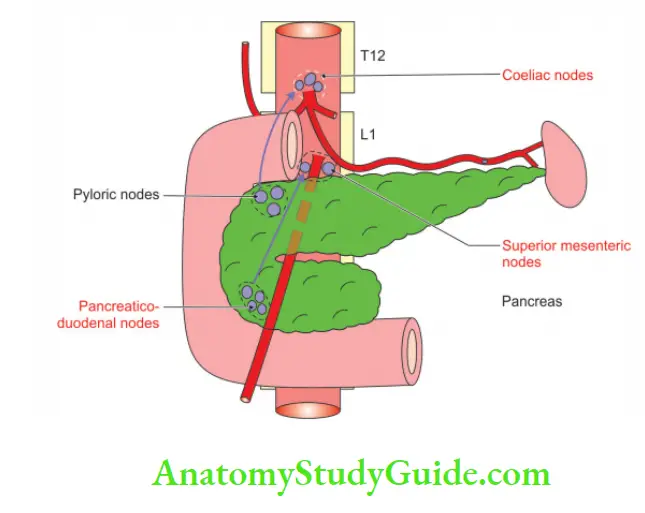
6. Pancreas Lymphatic drainage:
- The lymphatics of the upper part of the head drain into a coeliac group of lymph nodes.
- The lower part of the head and the uncinate process drain into the superior mesenteric group of pre-aortic lymph nodes.
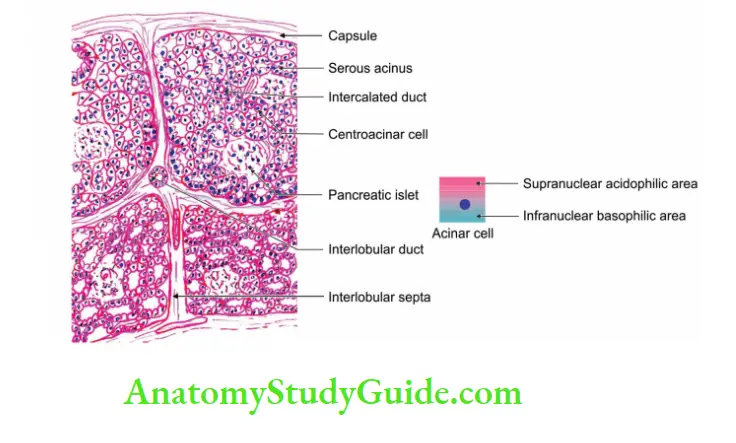
2. Histology
It is a lobulated gland, composed of endocrine and exocrine parts
1. The exocrine part shows:
- Plenty of serious acini.
- Very few ducts.
- The basal part of the cell of the alveolus is deeply stained and is basophilic.
- The area near the lumen of the cell is stained less heavily and is acidophilic.
- The nuclei are large.
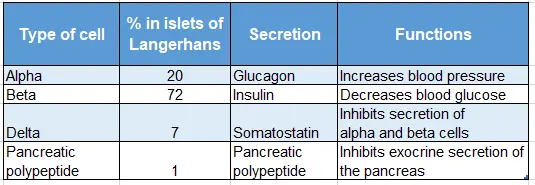
2. The endocrine part shows:
- The islets of Langerhans are scattered in the deeply stained pancreatic tissue.
- They vary in size and diameter.
- They are composed of a tightly packed mixture of acidophilic and basophilic small round cells.
- The details of various cells are described in Table
- Various cells of the pancreas
Various cells of the pancreas:
3. Development
Chronological age: It develops in the 4th to 8th week of intrauterine life.
Germ layer: Endoderm and mesoderm.
Site: It develops as ventral and dorsal pancreatic bud, at the junction of foregut and midgut.
Sources
1. The ventral pancreatic bud forms:
- The main pancreatic duct.
- The uncinate process.
- The lower part of the head of the pancreas.
2. The dorsal pancreatic bud forms:
- The accessory pancreatic duct, and
- The remaining part of the head of the pancreas is not formed by the ventral bud.
Anomalies:
1. Annular pancreas: Encircles the 2nd part of the duodenum (may cause duodenal obstruction).
2. The right part of the ventral bud migrates along the normal route but the left part migrates in an opposite direction.
3. In this manner, the duodenum becomes completely surrounded by pancreatic tissue, and an annular pancreas is formed.
4. Accessory pancreatic tissue: It is formed in the walls of the stomach, small intestine, gallbladder or spleen. This is a common finding.
5. Inversion of the pancreatic duct: The accessory pancreatic duct is larger than the main duct.
4. Applied anatomy
1. carcinoma of the pancreas is uncommon. However, it commonly occurs in the head of the pancreas (80%).
2. It obstructs the common bile duct or hepatopancreatic ampulla.
3. It presents as painless obstructive jaundice.
4. This needs to be compared with painful jaundice of common duct stones.
Cancer usually tends to project in one of the three directions:
- Between stomach and liver.
- Between the stomach and transverse colon.
- Below transverse colon.
5. The prognosis is usually poor because of the early involvement of the portal vein and other structures.
6. acute pancreatitis is secondary to complications of mumps.
7. Pain of pancreatic origin is referred to as T6-T10 dermatomes. However, involvement of the local parietal peritoneum causes severe intense pain in the middle of the back.
Leave a Reply