Crack Tooth Syndrome And Vertical Root Fracture
Cracked teeth or incompletely fractured teeth are commonly seen by clinicians in routine practice.
Table of Contents
The severity and treatment of the fracture can range from infraction line, needing minimum treatment, to severe, requiring endodontic treatment or even extraction. Patients usually present an extended history of pain of varying intensity; the origin of which may be difficult to locate.
The most common chief complaint in these cases is intermittent pain on biting.
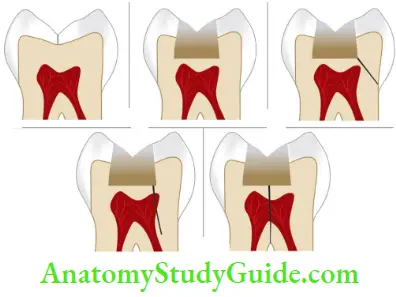
Symptoms normally depend on the extent and direction of the crack and the tissues involved. Cracks in teeth may occur in both horizontal and vertical directions involving the crown and/or root.
The etiology of these fractures is usually occlusal forces and iatrogenic procedures.
Read And Learn More: Endodontics Notes
Crack Tooth Syndrome And Vertical Root Fracture Definition
Many authors gave different definitions for cracks in teeth, for example, Gibbs first described incomplete fracture of posterior teeth as “cuspal fracture odontalgia,” Cameron as “cracked tooth syndrome,” and Ellis as incomplete tooth fracture.
Crack tooth syndrome is defined as an “incomplete tooth fracture extending through body of the tooth causing pain of idiopathic origin.”
The fracture commonly involves enamel and dentin but sometimes pulp and periodontal structure may also get involved.
Synonyms of Crack Tooth Syndrome
- Incomplete tooth fracture
- Tooth infraction
- Split tooth syndrome
- Greenstick fracture
- Hairline fracture
- Cuspal fracture odontalgia
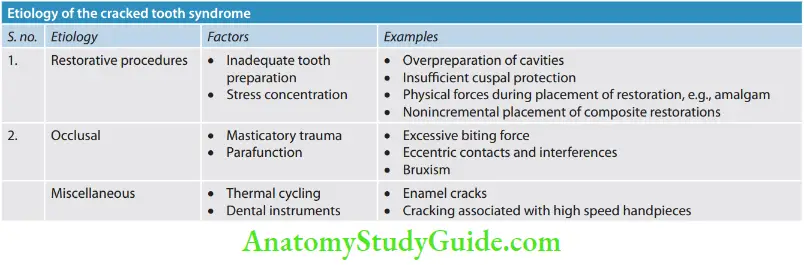
Crack Tooth Etiology
The etiology of cracked tooth syndrome is not specific but is commonly seen to be associated in teeth with large and complex restorations, leaving the teeth more susceptible to cracks.
Moreover, stressful lifestyles, parafunctional habits, and high masticatory forces are important contributing factors.
Etiological factors for cracked teeth can be classified as follows:
3. American Association of Endodontists classifications of cracked teeth
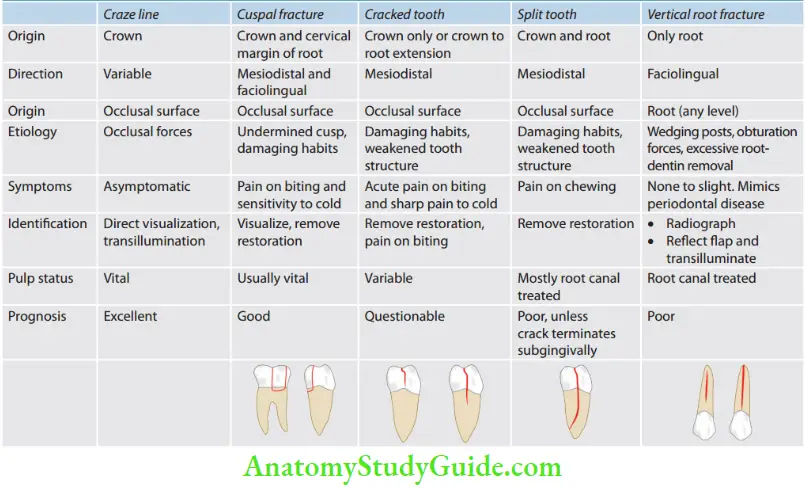
Crack Tooth Classification
American Association of Endodontists (AAE) divided cracks into five types which are described in Table.
1. Crack Tooth Clinical Symptoms
- Sharp pain on biting, which may get worse if the biting force is increased. “Rebound pain” i.e. sharp, fleeting pain occurs when the biting force is released from the tooth.
- Pain on biting occurs because fractured segments of the tooth move independently of each other, causing sudden movement of fluid within the dentinal tubules. This stimulates the A-delta fibers in the dentin-pulp complex causing pain. Pain when releasing biting pressure on an object occurs because when biting down, the segments are usually moving apart and thereby reducing the pressure on the nerves in the dentin. When the bite is released, the “segments” come back together sharply increasing the pressure in the nerves and causing pain.
- Sharp pain on eating or drinking cold and/or sugary substances because of stimulation of A delta fibers due to dentinal fluid movement.
- If the fracture propagates into the pulp, it may result in pulpitis or necrosis. If the crack propagates further into the root, a periodontal defect may develop or even a vertical root fracture.
- The patient may have difficulty in identifying the affected tooth as there are no proprioceptive fibers in the pulp
- Pulp is usually vital.
- The tooth is not tender to percussion in an axial direction
- Tooth often has an extensive intracoronary restoration or history of extensive dental treatment involving repeated occlusal adjustments or replacement of restorations, which fail to eliminate the symptoms.
2. Crack Tooth Diagnosis
The patient with cracked tooth syndrome gives a history of variable signs and symptoms which are difficult to diagnose.
Even the radiographs are inconclusive. A careful history of the patient, examination, diagnostic tests, radiographs, and sometimes surgical exposure are needed for an accurate diagnosis of cracked tooth syndrome.
-
- Clinical Examinations
- For definite diagnosis, one should obtain adequate information from the patient’s history and clinical examination.
- Chief Complaint
- The patient usually complains of pain on chewing and sensitivity to colds and sweets. If these symptoms are associated with noncarious teeth, one should consider the possibility of infraction.
- History of Patient The patient should be asked about
- Previous trauma if any
- Details regarding dietary habits
- Presence of abnormal habits like bruxism, etc.
- Visual Examination
- One should look for the presence of
- Large restoration
- Wear facets and steep cusps
- Cracked restoration
- Gap between tooth structure and restoration
- Sometimes removal of restoration is required for examination of fracture line in a cavity
- Tactile Examination
- While carrying out a tactile examination, one should gently pass the tip of the sharp explorer along the tooth surface, it may catch the crack.
- Periodontal Probing
- Through periodontal probing along the involved tooth may reveal a narrow periodontal pocket.
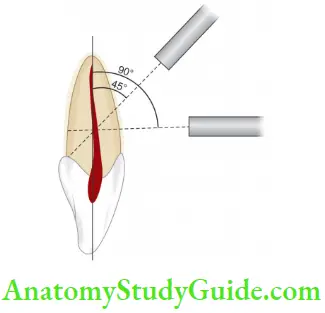
- Bite Test
- Orangewood sticks, rubber wheels, or tooth sloth are commonly used for detecting cracked teeth.
- The tooth is a small pyramid-shaped, plastic bite block with small concavity at the apex which is placed over the cusp and the patient is asked to bite upon it with moderate pressure and release.
- Pain during biting or chewing, especially upon the release of pressure is a classic sign of cracked tooth syndrome.
- Transillumination
- The use of fiber-optic light to transilluminate a fracture line is also a method of diagnosing cracked tooth syndrome.
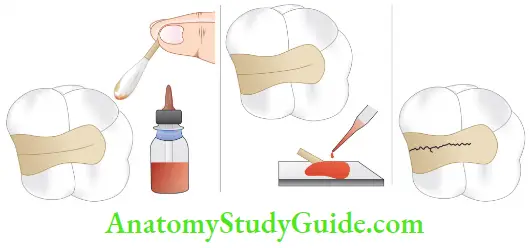
- Use of Dyes
1. Staining of fractured teeth with a dye such as methylene blue dye can aid in diagnosis.
2. The dye can be directly applied to the tooth to identify fracture, or it can be incorporated into a temporary restoration like zinc oxide eugenol and placed in the prepared cavity or the patient can be asked to chew a disclosing tablet.
3. The dark stain present on the fracture line helps in detecting the fracture.
- Radiographs
1. Radiographs are not of much help, especially if the crack is mesiodistal in direction.
2. Even the buccolingual cracks will only appear if there is the actual separation of the segments or the crack happens to coincide with the X-ray beam
3. Taking radiographs from more than one angle can help in locating the crack
4. A tooth with a crack may show widened periodontal ligament space and diffused radiolucency, especially with an elliptical shape in the apical area. - Surgical Exposure
1. If a fracture is suspected, a full-thickness mucoperiosteal flap should be reflected for visual examination of the root surface.
- Clinical Examinations
Differential Diagnosis of Cracked Tooth Syndrome
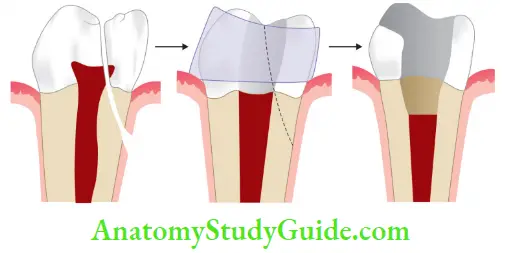
Crack tooth should be differentiated from a fractured cusp.
Th tooth crack occurs more toward the center of the occlusal surface as compared to the cusp fracture which is more peripheral in position.
To differentiate a cracked tooth from a fractured cusp, if a crack has been detected, use wedging to test the movement of the segments.
If there is no movement with wedging forces, it indicates a cracked tooth. A fractured cusp may break of under slight pressure with no further mobility.
If a fracture splits the tooth then tooth will show mobility with wedging force.
It should be differentiated from dentinal hypersensitivity, reversible pulpitis, acute periodontal disease, fractured restoration, postoperative sensitivity associated with microleakage from recently placed composite resin restorations, and areas of hyper occlusion from restorations, pain from bruxism, orofacial pain, or atypical facial pain.
The possibility of cracked tooth syndrome should be considered when there is pain in biting.
If the crack involves the pulp, the patient may have spontaneous pain or thermal sensitivity which lingers even after the removal of the stimulus.
Treatment of Cracked Teeth
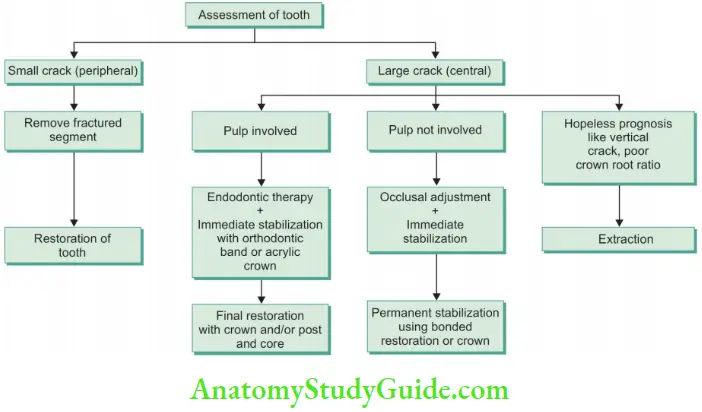
- Urgent care of the cracked tooth involves immediate reduction of its occlusal contacts by selective grinding of the tooth at the site of the crack or its antagonist
- Definitive treatment of the cracked tooth aims to preserve the pulpal vitality by providing full occlusal coverage for cusp protection
- When a crack involves the pulpal floor, endodontic access is needed but one should not make attempts to chase down the extent of the crack with a bur, because the crack may become invisible long before it terminates. Endodontic treatment can alleviate irreversible pulpal symptoms
- If the crack is partially visible across the floor of the chamber, the tooth may be bonded with a temporary crown or orthodontic band. This will aid in determining the prognosis of the tooth and protect it from further deterioration till the endodontic therapy is completed
- Apical extension and future migration of the crack apically onto the root determines the prognosis. If the fracture is not detected, pulpal degeneration and periradicular pathosis may be the initial indication that a complete vertical fracture is present. Depending upon the extensions of the crack and symptoms, the treatment may involve extractions, root resection, or hemisection

Crack Tooth Prevention
- Awareness of the existence and etiology of cracked tooth syndrome is important for its prevention
- Perform conservative tooth preparation if possible
- Line angles should be rounded instead of sharp to avoid stress concentration
- Incorporate adequate cuspal coverage if required
- Cast restorations should fi passively to avoid building of hydraulic pressure during placement
- Pins should be placed at an appropriate distance from the enamel to avoid stress concentration
- Remove eccentric contacts and adjust occlusion for patients with a history of cracked tooth syndrome to reduce the risk of crack formation
Vertical Root Fracture (VRF)
According to the AAE, a “true” vertical root fracture is defined as a complete or incomplete fracture initiated from the root at any level, usually directed buccolingually”.
These have an incidence of 2.3% in total fractured teeth with the highest incidence in endodontically treated teeth in patients older than 40 years of age.
VRF can occur at any phase of root canal treatment, that is, during biochemical preparation, obturation, or during postplacement.
This fracture results from wedging forces within the canal. Thse excessive forces exceed the binding strength of existing dentin causing fatigue and fracture.
Vertical Root Fracture Etiology
The most common reasons for VRF are
- Excessive dentin removal during biomechanical preparation
- Weakening of tooth during post-space preparation
Factors which predispose the Vertical Root Fracture VRF:
1. Anatomy of root: Roots with narrow mesiodistal diameter than buccolingual dimensions, are more prone to fracture, for example, roots of premolars and mesial roots of mandibular molar. The presence of root curvatures and depressions makes roots more prone to fracture
2. Amount of remaining tooth structure: Lesser is the amount of remaining tooth structure, more are the chances of VRF.
3. Presence of pre-existing cracks: Cracks present in dentin before treatment may later propagate to result in VRF
4. Loss of moisture in dentin: Thugh loss of moisture is not a main etiological factor, it can be a predisposing factor for VRF
5. During obturation: Use of a spreader results in the generation of stresses during lateral compaction of gutta-percha due to wedging effect of spreader on canal walls or through gutta-percha results in root fracture
6. Pathogenesis: As vertical root fracture progresses to the periodontal ligament, soft tissue grows into the fracture space causing the separation of the root segments.
When it communicates with the oral cavity through the gingival sulcus, bacteria enter the fracture area and initiate the inflammatory process in periodontal tissue causing the disintegration of the adjacent periodontal ligament, alveolar bone loss, and formation of granulation tissue.
Classification of Vertical Root Fracture (Flowchart)
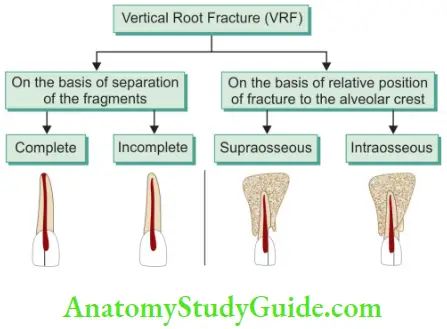
Vertical Root Fracture Signs and Symptoms
-
- The following signs and symptoms are seen in cases of VRF:
- Pain and swelling due to local chronic inflammation in response to infection. Pain is usually mild to moderate in nature, mostly accompanied by a bad taste. Palpation shows swelling and tenderness over the root itself, especially near the gingival area
- Sudden crunching sound accompanied by pain
- The sinus tract is commonly seen close to the gingival margin.
- The presence of two sinus tracts, i.e. at both buccal and lingual surface or multiple sinus tracts is the pathognomonic feature of vertical root fracture. In the case of non-vital teeth, sinus tracts are located more apically (differential diagnosis)
- Presence of deep, narrow, isolated periodontal pockets in an otherwise normal periodontal condition. Sharp cracking sound during obturation or post cementation
- Bleeding or lack of resistance within the canal during obturation
Vertical Root Fracture Diagnosis
-
- It is difficult to diagnose a case with VRF because of the following reasons:
- Signs and symptoms of VRF like pain on mastication, mobility, presence of sinus tract, bony radiolucency, and spontaneous dull pain can also be seen in failed root canal treatment or in periodontal disease
- VRF is not detected during or immediately after root canal treatment. It may take years to diagnose VRF.
The following steps should be carried out to diagnose a case of vertical root fracture:
- Vertical Root Fracture History
- History of pain, swelling, presence of sinus tract, endodontic treatment, facial trauma, and dislodged restoration may suggest VRF
- Clinical examination including age, involved tooth, and history of previous dental treatment help reach the diagnosis. Rapid deterioration of the endodontic status of a tooth after a long time without symptoms, or re-appearance of radiolucencies after healing has previously taken place, is indicative of fracture.
- Vertical Root Fracture Clinical Tests
- Direct visualization with good illumination and magnification is important to see the crack
- A transillumination test is done by exposing fiber-optic light on the tooth. Light is deflected at the crack, reducing its transmission through the tooth, and making the fractured segment appear darker
- Staining the fracture line using dyes helps the clinician to visualize a crack
- Bite test using tooth smooth, rubber wheels, and cottonwood sticks can be used to reproduce the pain on chewing.
- Periodontal probing shows the presence of a narrow, isolated, periodontal defect in the gingival attachment
- Pulp testing usually shows nonvital tooth because the fracture line may extend to the pulp causing inflammation and necrosis. This is especially helpful in diagnosing fractures in otherwise sound tooth.

- Radiographic Examination
- Tracing the sinus tract using gutta-percha and taking radiographs helps to detect its origin.
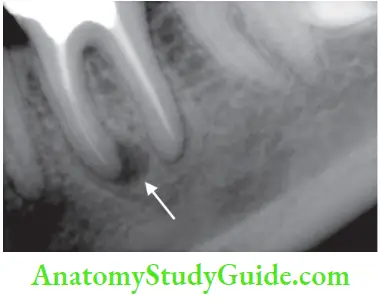
- “Halo-like” radiolucency running around the whole of the root surface is a classic sign of VRF. The radiolucent area may travel almost completely up the side of the root, resulting in a “J-type” lesion.
- Isolated V-shaped bone loss which is wider coronally, narrowing towards the apex is an important sign of VRF.
- The fracture line can be seen on the tooth as a vertical line along the root, root canal filling, or post-present in the tooth.
- If the separation of fragments occurs in a direction other than parallel to the X-ray beam, overlapping of fragments may result in double images of the external root surface.
- Extrusion of obturating material may occur into the fracture site which can be seen on the radiograph.
- Widening of periodontal ligament space along with bone loss is seen in cases of VRF. In case of the periapical lesion, bone loss occurs apically without destruction of the lamina dura along the root surface
- Furcation bone loss in otherwise sound molars without periapical or periodontal disease may indicate VRF.
- Cone Beam Computerized tomography (CBCT)
- CT gives a three-dimensional view of the tooth. It shows the separation of the adjacent root segments seen on at least two adjacent sections without the continuation of the hypoattenuating line into the contiguous tissue.
- Surgical Exposure
- Surgical exposure helps in definitive diagnosis if VRF is suspected from clinical and radiographic signs. After soft tissue retraction, visualization of the fracture line, and probing over the fracture line can confirm the VRF.
Treatment of Vertical Root Fracture
It involves extraction in most of cases. In multirooted teeth root, resection, or hemisection can be tried. Other treatment options include retention of the fractured fragment and placement of calcium hydroxide or cementation of the fractured fragments.
Recently, repair of root fracture have been tried by binding them with the help of adhesive resins, glass ionomers, and lasers. But to date, no successful technique has been reported to correct this problem.
Prevention of Vertical Root Fracture (VRF)
Prevention of root fracture basically involves avoidance of the causes of root fracture.
The principles to prevent root fracture are to
- Avoid weakening of the canal wa
- Minimize the internal wedging forces
- The following points should be kept in mind before during and after endodontic therapy:
- Evaluate the tooth anatomy before taking treatment
- Preserve as much tooth structure as possible during biomechanical preparation
- Use only optimal force during obturation for compaction of gutta-percha
- Use posts and pins if indicated
- Use posts with passive fits and round edges so as to reduce stress generation
Crack Tooth Syndrome And Vertical Root Fracture Conclusion
Early recognition of cracked tooth syndrome helps to prevent further propagation of crack into the pulp or subgingivally. The clinician should be aware of the existence of crack tooth syndrome and able to differentiate it from other mimicking conditions.
A good history, careful clinical examination, and inspection, along with some tests help to reach the diagnosis. The treatment of crack tooth depends on the position and extent of the crack. Treatment options vary from a simple restoration to placement of an extra coronal restoration with adequate cuspal protection.
Leave a Reply