Caries Activity Tests Introduction
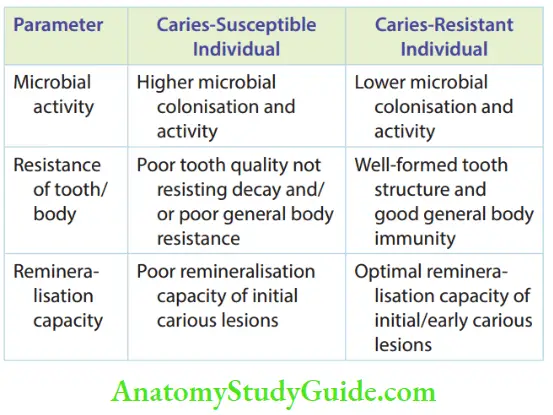
Dental caries is a multifactorial disease resulting due to the presence of a susceptible host, cariogenic microflora and a diet conducive to enamel demineralisation. The susceptibility or resistance of an individual to dental caries is assessed by the following three distinct factors.
Table of Contents
Read And Learn More: Paediatric Dentistry Notes
- Microbial activity: Microbial challenge against the integrity of the tooth.
- Resistance: Resistance of the tooth to decay (specific resistance) and the general resistance of the body to counter the microbial challenge.
- Repair (remineralisation capacity): The ability of the body to undergo repair in the reversible phase of dental caries. The initial and early carious changes cause demineralisation of the enamel surface. When calcium and phosphate ions are adsorbed by the tooth surface, these lesions undergo remineralisation.
Hence, this early phase of carious activity is referred to as a reversible or repairable phase.
The three parameters mentioned above indicate the extent of the challenge to the tooth and the repair capability f the tooth. These parameters are assessed with the help of caries activity tests.
A caries activity test should provide sufficient information about the challenge, resistance and remineralisation phases of the carious process. It should assess whether the tooth is at an increased risk of various attack
- Objectives The objectives of the caries activity test are as follows:
- To identify individuals with a higher probability of developing caries
- To permit public health dental personnel to screen a large segment of the population, such as school children, to determine prospective workloads
- To understand caries process better
An ideal caries activity test should carry the following attributes:
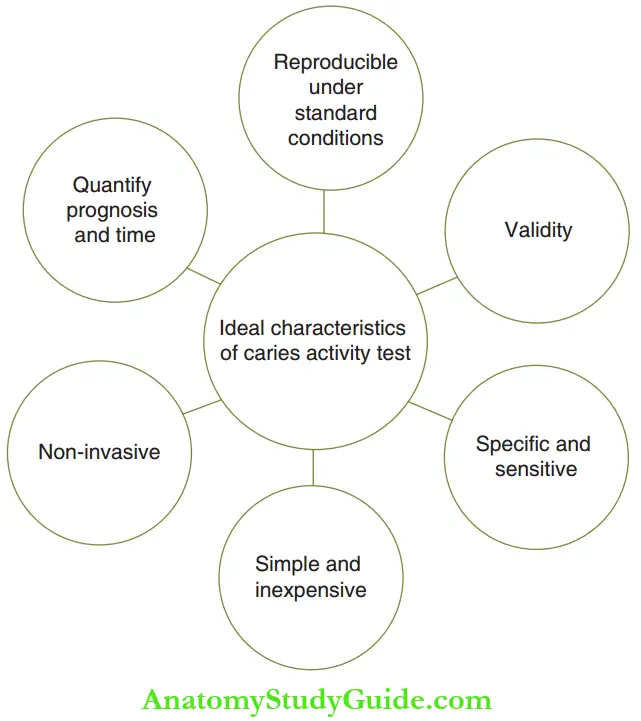
- The test should be reproducible under standardised conditions. Any chemical/bacteriological test should exhibit results of similar magnitude when repeated with the same specimen or a different specimen collected under standardised conditions.
- The test should be valid. There should be a high level of correlation between caries activity scores and DMFS prevalence and/or incidence of caries in an individual. It implies that the clinical finding (number of carious lesions) and the test findings should be coherent.
- The test should be specific and sensitive. There should be a minimal occurrence of false-positive (specificity) and false-negative (sensitivity) responses.
- The test should be simple and inexpensive. It should be performed without the need for training or special equipment. It should to be easy to evaluate and applicable to any clinical setting.
- The test should be non-invasive.
- An ideal caries activity test should not only quantitate the microbial challenge and defence capabilities but also aid in forecasting the number of lesions that might be expected and the appropriate amount of time left before the lesions develop.
There is no caries activity test that meets all these criteria because no single test can simultaneously measure host susceptibility, host resistance, microbial pathogenicity and the cariogenic potential of diet. Caries activity tests can calibrate either the microbial challenge factors or the host defence factors.
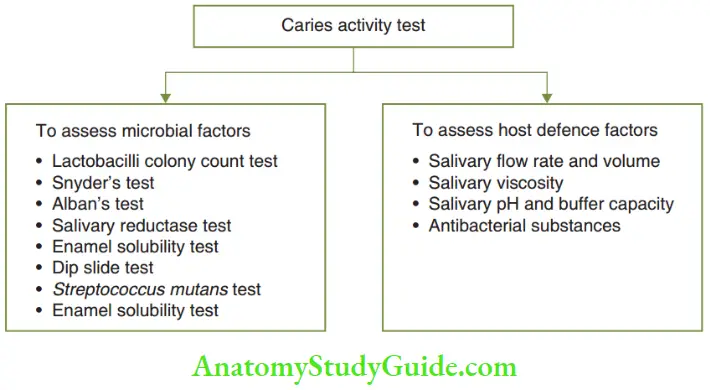
Tests To Assess Microbial Factors
The caries activity tests that calibrate microbial challenge factors assess either of the following:
- Number of Lactobacillus acidophilus
- Number of Streptococcus mutants
- The activity of acidogenic microbiota
Streptococcus mutans is related to the incipient lesion and Lactobacillus is more in overt carious lesions. It is more difficult to culture and counts streptococci more than lactobacilli. So, streptococci counting tests are utilised by dental researchers and Lactobacillus counts are used in clinical assessment.
The more commonly used caries activity tests that assess microbial factors are discussed next.
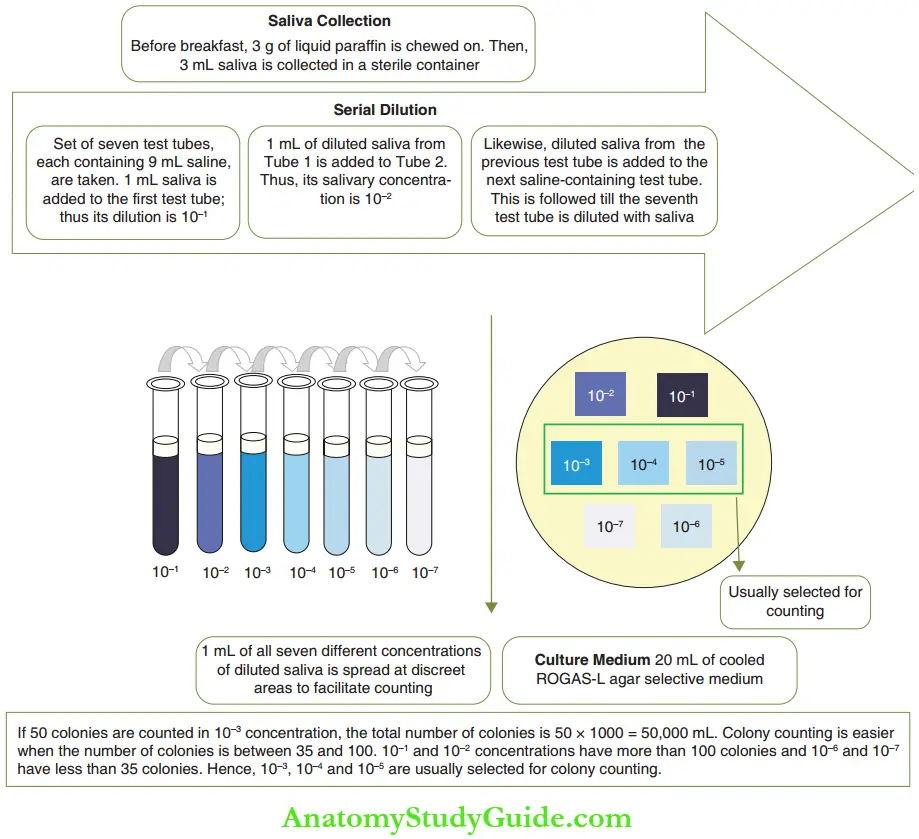
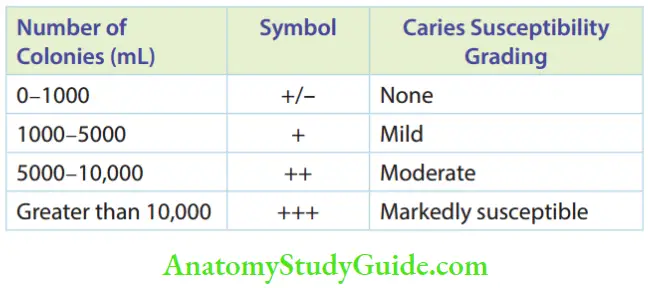
- Lactobacilli Colony Count Test The Lactobacilli colony count test is the first microbiologic caries activity test introduced by Hadley in 1933. It is extensively used by practitioners. The saliva obtained from patients with active caries usually has a high number of L. acidophilus organisms. The saliva of caries-free individuals has either no lactobacilli or significantly fewer lactobacilli than a caries-prone individual. Lactobacilli are associated with caries lesion development and may be responsible, in part, for the direct penetration of the lesions into coronal dentin. If lactobacilli are detected in caries-free individuals, carious lesions usually develop within the following year. Restriction of dietary carbohydrates can induce a dramatic decrease in salivary lactobacilli. The figure depicts the procedure of the lactobacilli colony counting. The observation and conclusion are given in Table. Despite the well-established direct relationship between lactobacilli counts and DMFS, this method of caries activity testing is not popularly used due to the introduction of other simpler tests such as Snyder’s test, Alban’s test and dip slide test.
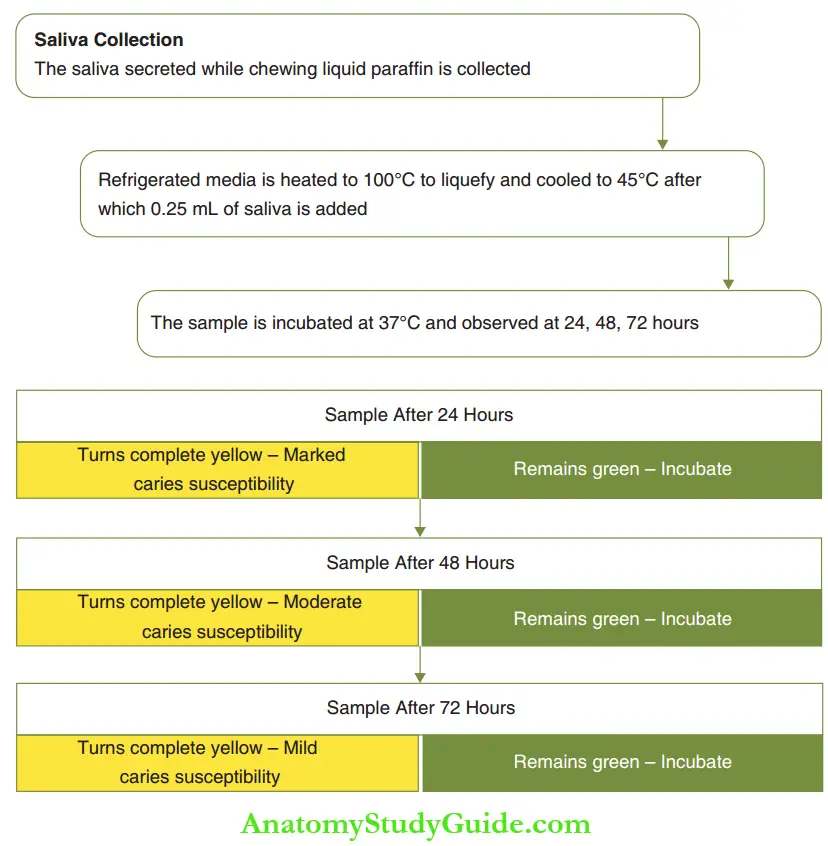
- Snyder’S Test In the early 1940s, Marshak L. Snyder proposed a lactobacilli test that was much easier to accomplish than the lactobacilli colony count test proposed by Hadley. This was based on the fact that lactobacilli are both acidogenic and acidic. As the amount of acid produced in a medium is proportionate to the number of lactobacilli, the amount of acid produced concludes on the cariogenic potential. A selective medium, called the Snyder medium, with an inherent pH of 5.0 is used for optimal lactobacillus growth. In order to visually evaluate the rapidity and the extent of acid production, a pH change indicator, Bromcresol green, is incorporated into the medium. On adding the indicator, the medium turns blue at pH 5.0, green at 4.6, yellowish at 4.2 and yellow at 3.8. A standardised colour chart is used to determine the colour changes. Five millilitres of the medium (with an indicator) can be refrigerated in sterile test tubes to be used when required. The figure shows the procedure, observation and conclusions of the Snyder test. The advantage of Snyder’s test is that it requires only one tube of medium and no serial dilutions as in the lactobacilli colony count test. Though there is a need to use a controlled temperature to melt the medium before adding the saliva specimen, the test is still best accomplished in a laboratory environment. However, it requires 72 hours to deliver conclusions.
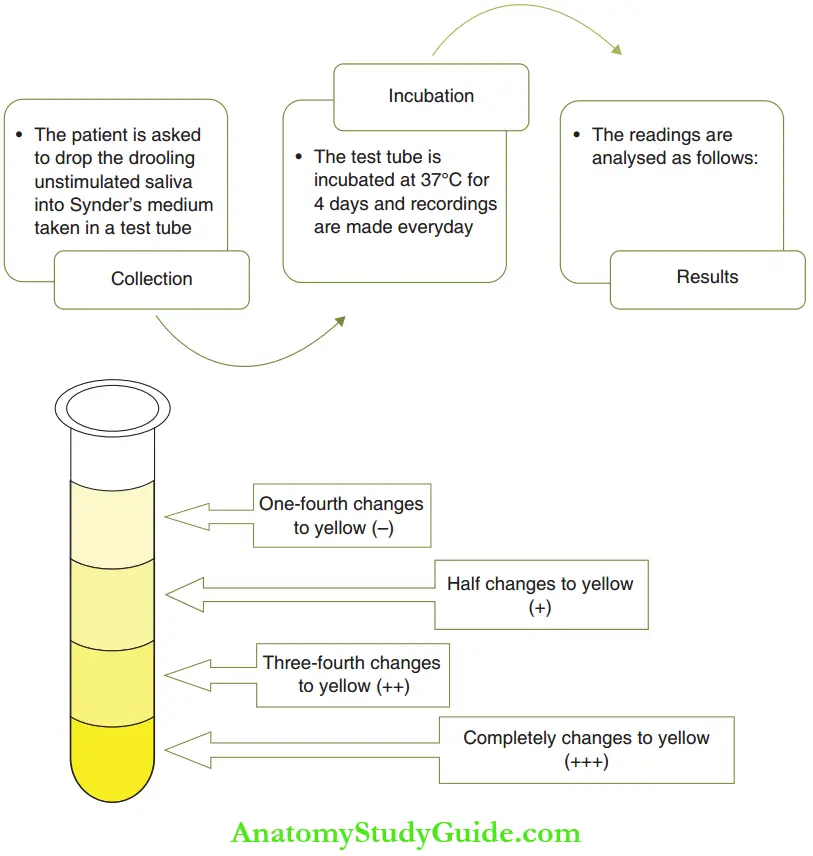
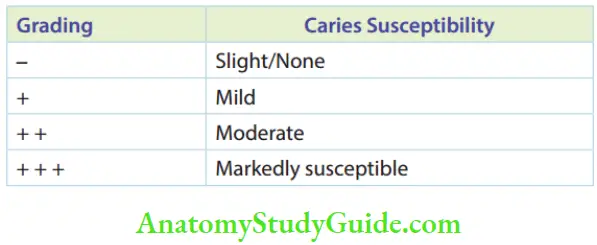
- Alban’S Test (Modified Snyder Test) Arthur L. Alban, a pedodontist from California, modified the Snyder test for routine use in the dental office. The modified Snyder’s method uses the same Snyder’s media. Figure depicts Alban’s test procedure and Table gives the observations and conclusions. The advantage of Alban’s test is that it is ideal for patient education. It can also be useful in achieving patient cooperation. Favourable changes in diet intake and plaque control procedures are reflected within a few weeks by corresponding changes in Alban’s test score.
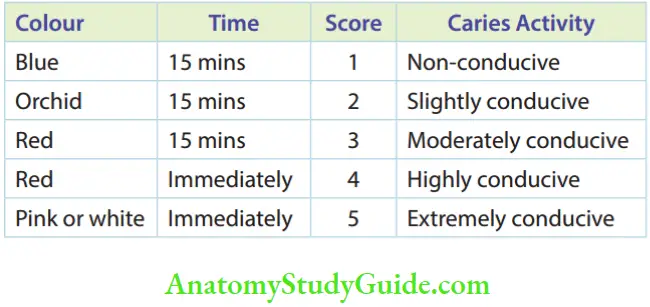
- Salivary reductase test The salivary reductase test assesses the quantity of bacterial reductase enzyme in saliva. When saliva contains more non-specific microbiota, the cumulated amount of reductase enzyme is higher. Diazoresorcinol is the reagent used in this test to observe the time of colour change proportional to the quantity of enzyme. The colour changes from blue to red to colourless in the course of time. The quicker the change in colour, the higher the number of micro-organisms, implying higher caries conduciveness. The reductase test is available in a kit (Treatex) that includes calibrated saliva collection tubes with reagents and flavoured paraffin on the inside of the tubes’ caps. Saliva is collected by chewing the paraffin and expectorating directly into the collection tube. When saliva reaches the calibration mark (5 mL), the reagent cap is placed. The sample is mixed with a fixed amount of diazo resorcinol reagent. The change in colour after 30 seconds and after 15 minutes is taken as a measure of caries activity. The th procedure is depicted in Figure and the observations and conclusions of the reductase test are mentioned in Table.
- Fosdick Calcium Dissolution Test (Enamel Solubility Test) The Fosdick calcium dissolution test assesses the enamel solubility of saliva. The patient’s saliva is mixed with glucose and powdered enamel is available in the test kit. The amount of powdered enamel in milligrams dissolved in 4 hours by the acid formed is measured. With increased enamel solubility, the calcium content of saliva increases. Increased enamel solubility implies cariogenic conductivity. The clinical correlation of this test with cariogenicity is reasonably good. But it requires complex equipment and trained personnel and involves higher costs. The method is not suited for clinical assessment.
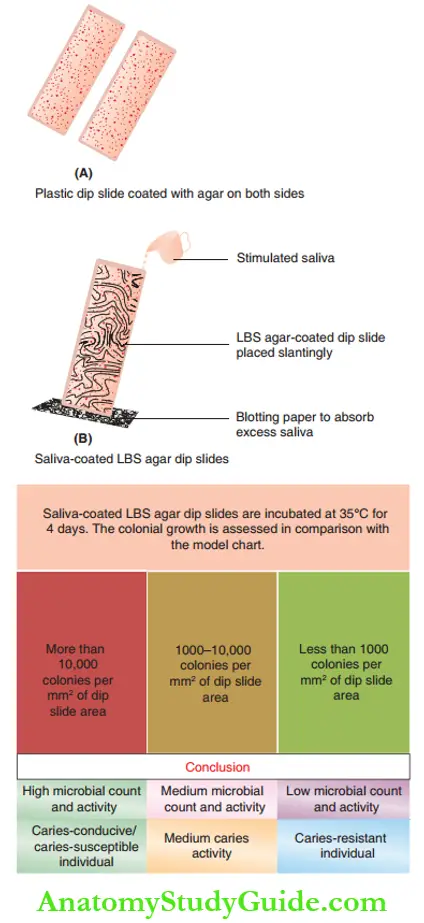
- Dip Slide Method The dip slide method can be easily applied in the dental office to quantitate lactobacilli. The test kit has a specially designed dip slide of plastic. This slide is coated with LBS agar on both sides. Undiluted stimulated saliva obtained by chewing paraffin is flowed over both the agar surfaces. The amount of saliva sample on the dip slide is relatively constant. The plastic slide holders are positioned vertically with a slight tilt to assure that both agar surfaces are totally wetted with saliva. Excess saliva is allowed to drain into a clean absorbent paper. The slide is then placed into a sterile tube, which is tightly closed and incubated at 35°C for 4 days. It is then removed and the lactobacilli colony density is determined by comparing it with the model chart supplied with the test kit. The lactobacilli growing on the LBS agar surface form either white or transparent colonies. A reading of more than 10,000 colonies per mm2 of dip slide area is considered high bacterial activity, implying higher caries susceptibility of the individual. A reading of less than 1000 colony counts is considered to be a low number of bacterial activity, implying the relative resistance of the individual to dental caries. Any results between 1000 and 10,000 are considered as a medium. The procedure is depicted in Figure. When bacterial colonies are more in number, a confluent carpet-like growth is found on the agar surfaces. This technique can be utilised in a private dental office as the technique is simple and inexpensive and the results are easy to read.
- S. Mutans Test The number of S. mutans colony-forming units (CFUs) per unit volume of saliva has been proposed as a reliable indicator of caries activity. S. mutans are the primary initiators of dental caries. They are highly acidogenic organisms that primarily colonise on the tooth surface. S. mutans CFU are evaluated by scrapping the tongue with a wooden spatula to obtain a sample of microorganisms. The scrapped sample is pressed against a selective medium for S. mutans – MSB agar (mitis salivarius-bacitracin agar). Bacitracin eliminates the growth of other facultative organisms, hence selectively augmenting the growth of S. mutans. This is followed by an incubation period of 4 days. A CFU count of greater than 105 indicates a caries-susceptible individual.
Tests To Assess The Host Defence Factors
Decay is a cumulative product of the microbial challenge to teeth in the presence of a suitable substrate for microbial colonisation, multiplication and activity. However, the host defence factors can retard the activity. The salivary parameters are the host factors that retard decay progression. This forms the first line of defence of the host to tooth decay. The salivary flow rate, its cumulative volume, the viscosity of saliva, chemistry (pH and buffer capacity) and the presence of antibacterial substances are directly associated with the individuals’ proneness to tooth decay.
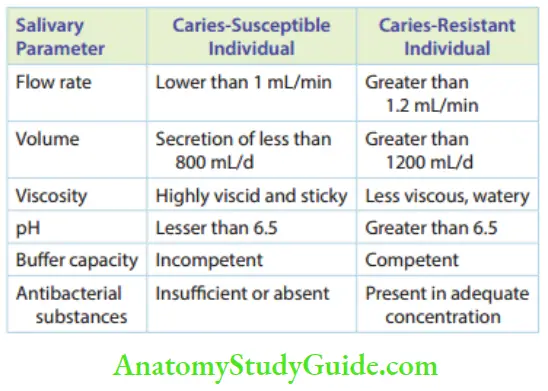
- Salivary flow rate and salivary volume: Salivary flow rate implies the volume of saliva secreted per minute. Flow rate is determined by collecting saliva in a calibrated cylinder or test tube stimulated by chewing paraffin over a 5-minute period. The normal range is around 0.8–1.5 mL/min. The higher the flow rate, the higher the volume of saliva. Saliva enhances the oral clearance of foodstuff It dilutes the acids formed by microbial activity. Hence, a decay-resistant individual is expected to have a higher salivary rate of secretion and higher salivary volume. A decrease in the flow rate and volume is related to an increase in caries susceptibility. Less than 5 mL of saliva in 5 minutes denotes xerostomia and signifies high cariogenicity.
- The viscosity of saliva: This is indirectly proportional to the decay susceptibility of the individual. When the viscosity is high, it affects the saliva’s flow and oral clearance properties. Hence, the proneness to tooth decay is high. Conversely, when the saliva is less viscous or more fluid, it demonstrates better flow and enhances oral clearance of the substrate particles, thus decreasing the decay proneness of the individual. The viscosity of saliva is determined by comparing it with water. A special Ostwald pipette with a calibrated bore is used to measure the viscosity of saliva. Five millilitres of water is introduced into the pipette and allowed to flow, by gravity, from an upper mark on the pipette to the lower mark. The time in seconds required to pass these two points is recorded. The procedure is then repeated with 5 mL of the saliva specimen. The relative viscosity is calculated by the following formula:
 The relative viscosity is in the range of approx. 1.5.
The relative viscosity is in the range of approx. 1.5.
A value greater than 1.8 denotes that saliva as viscid. - pH and buffering capacity of saliva: Saliva has a pH of around 7. It also contains bicarbonate ions. These bicarbonate ions act with acid molecules produced by microbial activity. Enhanced acid formation decreases pH. Hence, saliva resists the drop in pH, which is called its buffer capacity. When saliva has an inherent acidic pH (lesser than 6.5), its capacity to dilute/counter the acid formation from microbial activity becomes insufficient. When the bicarbonate ion concentration of saliva is decreased, its buffer capacity is compromised. A caries-susceptible individual is expected to have acidic saliva and less competent buffer capacity in contrast to a caries-resistant individual whose resting salivary pH is greater than 6.5. Antibacterial substances: Saliva usually contains antibacterial substances such as bacterial lysozyme, which is bactericidal. When these endogenous antibacterial substances are low in quantity, the host becomes decay conducive.
Cardiogram
Cardiogram is an educational, interactive software program developed by Malmo University, Sweden, for better understanding of the multifactorial aspects of dental caries and estimation of caries risk. The program is applicable for a clinical set-up and an academic venture. It demonstrates caries risk graphically, encouraging the introduction of preventive measures.
- Objectives
- The objectives of a cartogram are as follows:
- To illustrate the interaction of caries-related factors
- To illustrate the chances of avoiding caries
- To express caries risk graphically
- To recommend targeted preventive actions
Ten parameters are fed to run the program. The parameters to be assessed; the factors to be investigated, examined or recorded; and appropriate scores fed into the computer are listed in Table.
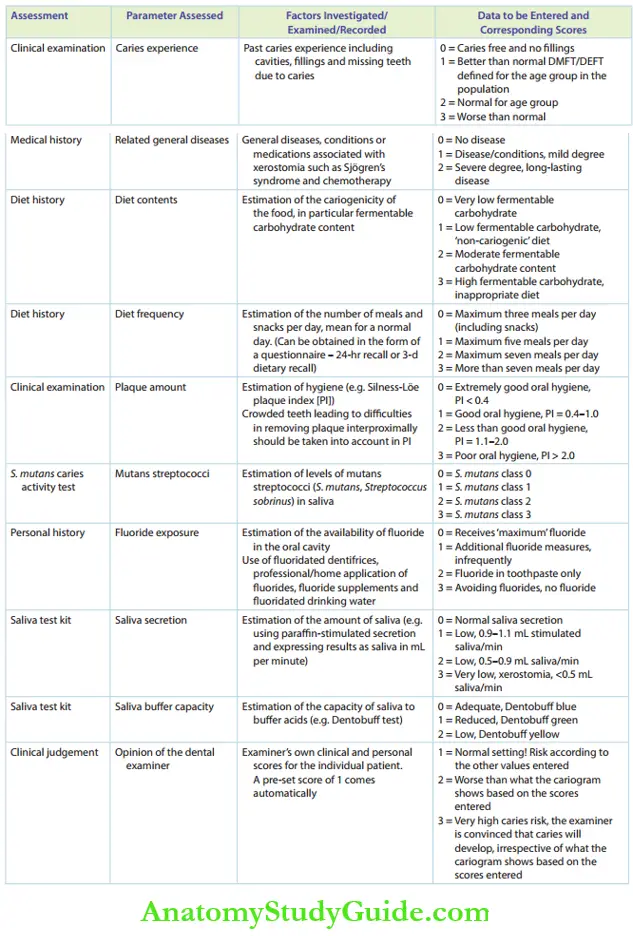
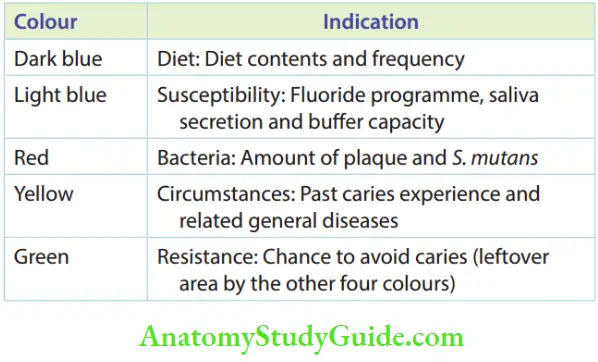
When 7 out of 10 parameters are entered, a pie circle diagram is generated. The generated cardiogram contains fie colours spread in a pie-circle diagram.
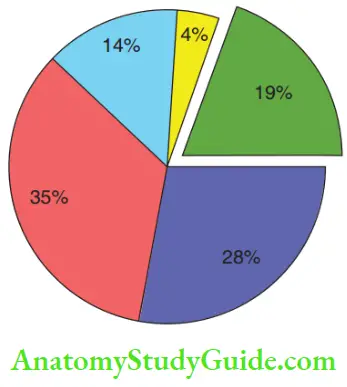
The colours and their indications are listed in Table.
The cardiogram shows the following features:
- If the patient is at a high, intermediate or low overall risk for caries
- Aetiological factors considered responsible for the caries risk
- Results to indicate targeted actions to counteract the caries risk
Caries Activity Tests Summary
- The objective of caries activity testing is to identify parameters associated with the caries process to indicate the extent of challenge and adequacy of the defence or repair capability of the tooth.
- The caries activity test identifies individuals with high caries susceptibility.
- The ideal caries activity test should be reproducible, valid, specific and sensitive, simple and inexpensive and noninvasive. The test should quantitate microbial challenge and defence capabilities and forecast the number of lesions that might be expected and the appropriate time for lesions to develop.
- The caries activity test calibrates microbial factors or host factors.
- The tests done for microbial factors are as follows:
- Lactobacilli colony count test
- Snyder’s test
- Alban’s test
- Salivary reductase test
- Enamel solubility test
- Dip slide test
- S. mutans test
- The tests done for host (defence) factors are as follows:
- Saliva test: Flow rate, viscosity, pH and buffer capacity
- Cardiogram is a software-based caries risk assessment. The table lists the parameters to be assessed in the cardiogram.
Leave a Reply