Complications Of Hernia
1. Irreducibility
Table of Contents
- It occurs due to adhesions formed between the omentum, sac, and the contents. Irreducibility produces dull aching pain.
Diagnosis of Irreducible Hernia
- Hernia is tense
- Tender
- Irreducible
- No impulse to cough
- The recent increase in the size of the swelling
2. Obstructed Hernia
- Irreducible hernia + obstruction to the lumen of the gut gives rise to obstructed herniClinically, it produces severe colicky abdominal pain, abdominal distension, vomiting, and step ladder peristalsis.
Abdominal Hernia Treatment
Urgent division of the neck of the sac followed by hernioplasty.
Factors Responsible for Obstructed Hernia
- Narrow neck
- Irreducibility
- Sudden straining
- Too many contents
- Long duration of hernia
- Sliding hernia
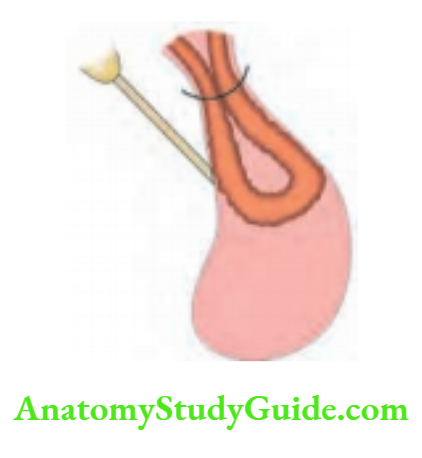
3. Strangulated Hernia
Irreducibility + obstruction + impairment of blood supply to the intestine.
Abdominal Hernia Pathology
- Strangulation commonly occurs in femoral hernia, obturator hernia, and indirect hernia.
- Initially, the venous return is occluded, the part gets congested, and mucosal ulceration and hemorrhage occur in the gut wall. It also results in edema due to capillary exudation.
- If the obstruction is not relieved, constriction of the artery takes place resulting in gangrene of the bowel. If this happens, there is a proliferation of bacteria.
- Gangrene appears at the ring of constriction first. Later it develops in the antimesenteric border.
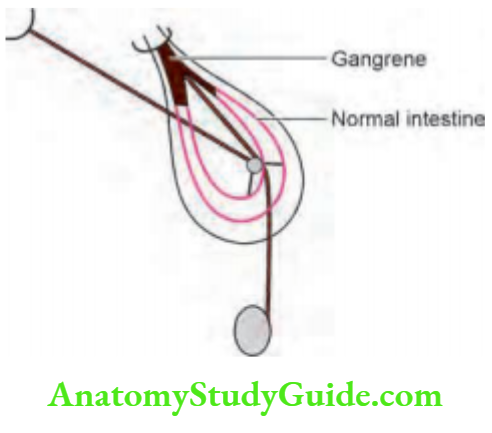
- Such a gangrenous segment contains decomposed blood in which gram-negative organisms multiply.
- They produce endotoxins resulting in endotoxic shock. If the gangrene extends into the intraabdominal segment of the bowel, peritonitis can occur.
- The deep ring and the external ring are the common constricting sites.
Abdominal Hernia Clinical Features
- Sudden, severe, prolonged pain with some features of shock are indicative of strangulation.
- Clinical examination of such hernia reveals:
- Tense (hernial sac is tense—differentiates it from obstructed hernia)
- Tender
- No impulse to cough
- Irreducible
- The recent increase in the size of the swelling
The general condition of the patient is poor:
- Feeble pulse, hypotension, rebound tenderness, absent bowel sounds, toxic look.


Abdominal Hernia Treatment
1. General measures
- The patient is hospitalized foot end of the bed is raised so that an irreducible hernia may be reduced by gravity. However, if there is a suspicion of gangrene, this step is not recommended.
- A Ryle’s tube is introduced to decompress the stomach, thus preventing vomiting and reducing abdominal distension.
- Intravenous fluids are given to correct dehydration and to prevent renal failure.
- Narcotic analgesics are required to reduce the pain.
- An attempt should be made to reduce the swelling when there is no gangrene by the following measures:
- Good sedation
- The patient’s thigh is flexed, adducted, and medially rotated.
- With the right hand, the sac is gently squeezed by applying pressure over the scrotum. At the same time with the left hand, the proximal portion of the sac is guided into the inguinal canal. This procedure is described as taxis. Taxis are contraindicated, if there is gangrene.
- Complications of forced reduction include contusion of the intestinal wall, rupture of the sac at the neck, and reduction en masse, i.e. the entire sac with the contents are reduced into the abdominal cavity but the intestine still remains strangulateThe patient is prepared for surgery and blood is grouped and cross-matched.

2. Surgery
- With broad-spectrum antibiotic coverage, the hernia is explored by an inguinoscrotal incision, and the hernia sac is defined at this stage, the constricting ring should not be separated all the toxic fluid from the sac is aspirateThe constriction is then divided using a grooved director or hernia bistoury.
- While dividing the constricting ring, the inferior epigastric vessels which are situated medially may be damaged Therefore, care has to be taken to protect these vessels. High ligation of the sac should be done.
- Low ligation should not be done because it causes recurrence. If the bowel is gangrenous, resection of gangrenous segment and anastomosis is done. Closure of incision includes placement of tube drain, which is brought out through a separate incision.
- Mesh should not be used in this situation. A simple darning or herniorrhaphy can be done. If the viability of the bowel is doubtful, the intestinal loops are covered with warm wet mops for a period of 5–10 minutes, and 100% oxygen is given to the patient (request the anesthetist).
- Return to pink color, peristalsis of bowel and pulsations in the mesentery indicate viability. If the general condition of the patient permits, repair of the hernia may also be done.
- If evidence of peritonitis is present or if gangrene is spreading within, laparotomy should be done.
Surgery for Strangulation
- Generous inguinal incision, identify the sac
- First, aspirate toxic fluid
- Divide constricting agent
- Check for viability
- Resection of gangrene
- Repair of hernia—without mesh
- Broad-spectrum antibiotics
4. Incarcerated Hernia
It is an obstructed hernia due to obstruction caused by fecal matter. It generally occurs in a sliding hernia (Nowadays incarcerated hernia has been renamed as obstructed hernia
5. Inflamed Hernia
- It occurs when the contents of a hernia get inflamed, e.g. appendicitis in a hernial sac, Meckel’s diverticulitis in a hernial Thus, complications of hernia can be dangerous.
- It may range from a simple obstruction to a life-threatening strangulation. Hence, early diagnosis and early treatment are necessary in all cases of indirect hernia
- In a few selected cases of direct hernia, wherein the defect is big, the chances of strangulation are less.
- However, if there are no medical contraindications, surgery has to be adviseFollowing are a few examples of strangulations without obstruction. They have diarrhea and bleeding per rectum rather than constipation.
Summary of Complications of Hernia
- Irreducibility
- Obstructed hernia
- Strangulation
- Incarcerated hernia
- Inflamed hernia
Strangulation without Obstruction
- Omentocoele
- Richter’s hernia
- Littre’s hernia
Recurrent Hernia
An incidence of 10% recurrence is common medially.
1. Preoperative
- Chronic cough
- Weak muscle tone
- Straining while passing urine, constipation
- Obesity, ascites, anemia.
2. Intraoperative
1. Improper excision of the sac:
- The sac should be ligated at the level of the deep ring (neck).
- This is called high ligation of the saVery often, the sac is seen as soon as the inguinal canal is opened.
- If it is ligated at the fundus or body (low ligation), it invariably results in recurrence. A missed indirect sac can be a cause of recurrence.
2. Absorbable sutures:
- Such as catgut have a lifespan of 2–3 weeks. If they are used for reconstruction, they invariably result in recurrence.
3. Bleeding:
- At the end of the surgery, small bleeding points should be coagulated by using diathermy or ligatures.
- Hematoma formation predisposes to infection, which can be the cause of recurrence.
4. Tension:
- Between suture lines can cause strangulation and fibrosis of muscle fibers. Hence, care and gentleness are important while suturing conjoined tendons to the inguinal ligament.
Recurrent Hernia Postoperative
- Persistent postoperative cough weakens the suture line.
- Haematoma can get secondarily infected resulting in pus formation. The sutures give way leading to recurrence. Hence, if there is a significant hematoma, it should be drained.
- Infection: Even though hernia is a clean surgery, chances of infection are present, especially in diabetics, alcoholics, and immunocompromised patients.
- Prophylactic antibiotics such as 2nd generation cephalosporin should be given. If infection occurs, it should be treated accordingly.
- Exertion: Too much exertion in the postoperative period, in the form of lifting heavy weights or carrying heavy weights on the shoulder, may weaken the suture line, resulting in hernia
Most of the recurrences occur within one year. Incidence of recurrent hernia may vary from 2 to 8% even in experienced hands.
In a case of recurrent hernia, it is difficult to say whether it is a direct hernia or indirect herniFrom the management point of view, it does not matter.
Recurrent Hernia Treatment
- If the sac is present due to incomplete excision at the previous surgery, it should be completely excised up to the level of the deep ring, followed by hernioplasty.
- Meshplasty is the surgical treatment for a recurrent herniHowever, if mesh cannot be placed either due to infection or due to nonavailability, prolene darning can be done.
- Tuberculosis must be ruled out in cases of persisting infection.
- In all these cases, precipitating factors if any, should be treated first.
- The only way to totally prevent recurrence is by closure of the deep ring. This can be done only after dividing the spermatic cord (Kuntz procedure). It is indicated in elderly patients who have multiple recurrences.
Special Hernias
1. Giant hernia: Sac extends up to mid-thigh.
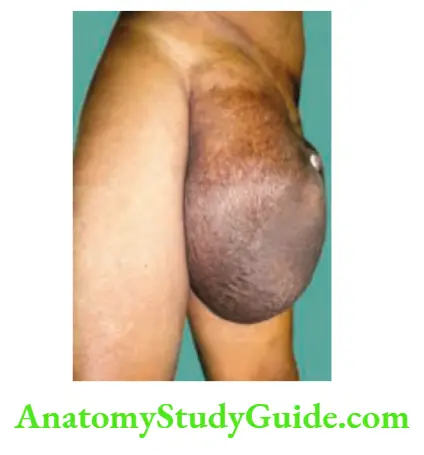
Special Hernias Definition: A giant inguinoscrotal hernia is defined as a hernia that extends below the midpoint of the inner thigh in the standing position.
Special Hernias Clinical features
- Most patients would have had their hernia for several years.
- The contents often include colon, small intestines, and bladder.
- A few of these are also sliding inguinal hernias. Hence, more prone to complications such as incarceration, intestinal obstruction, and scrotal ulceration. The last complication is due to pressure necrosis or due to friction while walking or moving. Differential diagnosis includes scrotal elephantiasis.
- A few precautions to be taken during surgery are:
- Preoperative chest physiotherapy.
- Catheterize the bladder. This will decrease the incidence of urinary bladder injury.
- Bowel wash before surgery.
- Dissect the sac carefully all around.
- Perfect haemostasis
- Omentectomy and rarely colectomy may be required.
- If the bowel is not resected, the mesh can be placed safely.
- In cases of emergency and patients with co-morbid factors including cardiac problems, take consent for orchidectomy—the best option will be to divide the cord at the level of the deep ring and close the deep ring during orchidectomy.
2. Dual hernia: It has two sacs, one direct and another indirect, connected by an isthmus which is behind the inferior epigastric artery. It is also known as saddlebag hernia, pantaloon hernia, dual hernia, or Romberg hernia.
Special Hernias Significance
- Deep ring occlusion test: The inference of the test may not be correct.
- It is the cause of recurrence if one sac is not treated properly.
3. Prevesical hernia: It is also called a funicular direct hernia is a hernia containing a portion of the bladder with pre-vesical fat through the defect in the conjoined tendon on the medial side.
History of the swelling becoming less prominent after micturition may be present. Due to its narrow neck, it is prone to strangulation.
4. Littre’s hernia: It is referred to as a hernia containing Meckel’s diverticulum. When the diverticulum gets infected, such hernias are called inflamed hernias. Infection may be precipitated by partial obstruction to the diverticulum by constricting agents.
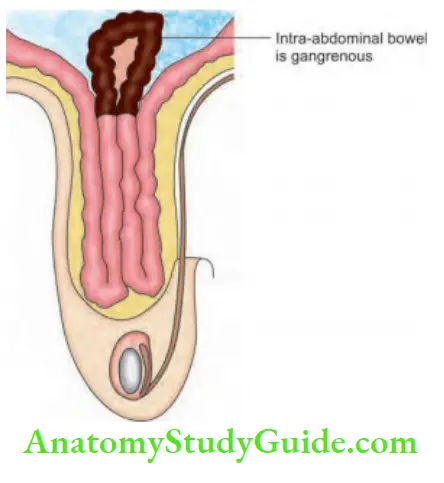
5. Maydl’s hernia (Hernia-en-W):
- It is a W hernia wherein the intra-abdominal bowel loop segment becomes gangrenous very early but in the scrotum, there are no signs of gangrene. The patient presents with an obstructed hernia and at operation, the inguinoscrotal segment has no gangrene.
- The intra-abdominal segment must be examined and the gangrenous portion should be exciseIt can also be called retrograde strangulation. Clinically, there is tenderness above the inguinal ligament.
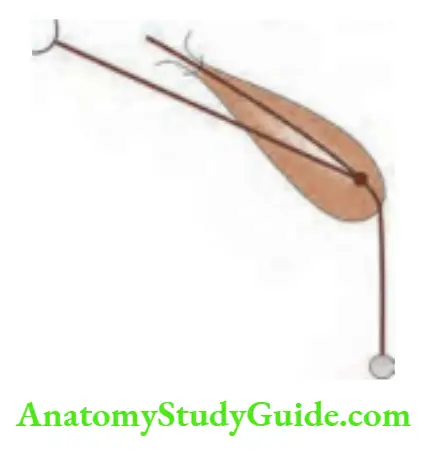
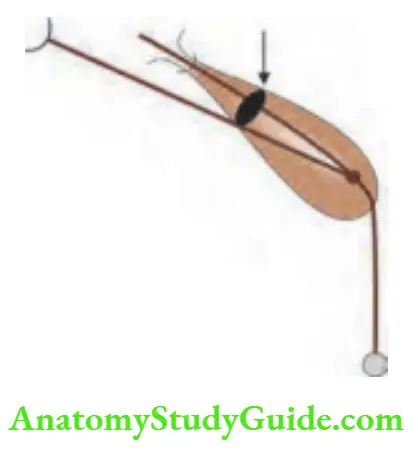
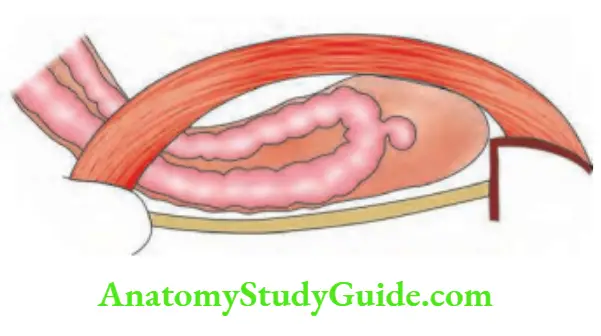
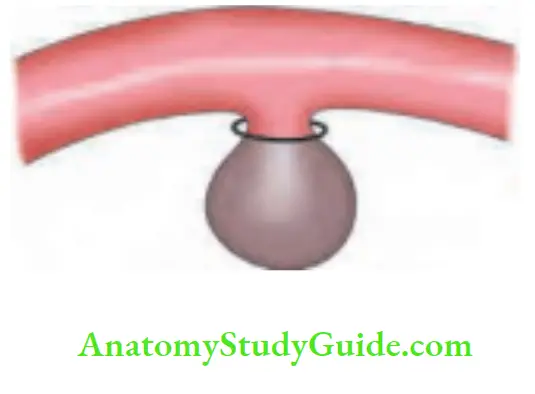
6. Richter’s hernia
- When only part of the circumference of the bowel becomes strangulated, it is called Richter’s hernia.
- It may spontaneously reduce
- Thus, gangrene may be overlooked at operation.
- Even though the patient has features of intestinal obstruction, there will be diarrhea and often blood in stools.
- Femoral hernia and obturator hernia are a few examples of hernia which can sometimes present as Richter’s hernia.
7. Sliding hernia (Hernia-en-glissade)
- Incidence: 1–3%
- Always acquired hernia
- It occurs as a result of the slipping of the posterior peritoneum along with the retroperitoneal viscus. As a result, the caecum, on the right side, and the sigmoid colon on the left side, form the posterior wall of the sac.
- If the caecum and appendix are the contents of the hernial sac, it is not a sliding hernia.
- However, a true hernial sac containing omentum or intestines exists.
- Weakness of the abdominal wall at the deep ring lateral to inferior epigastric vessels is also a contributing factor.
- The urinary bladder can also be the content of the hernial sac.
Sliding hernia (Hernia-en-glissade) Clinical features
- It almost always occurs in males.
- It commonly affects elderly patients.
- It can be suspected when there is a large hernia descending down into the scrotum.
- Left-sided is more common than right-sided hernia.
- It practically always occurs in long-standing cases of inguinal hernia.
- They are not completely reducible.
Complications: These hernias can easily strangulate and since their wall contents include the large intestine, the mortality and morbidity increase.
Sliding hernia (Hernia-en-glissade) Treatment
- Truss is absolutely contraindicated.
- Once the hernial sac is opened, the sac should not be twisted.
- A purse-string suture is applied within to avoid injury to the caecum/sigmoid colon.
- The sac is removed and the repair of the hernia is done.
- In elderly patients, orchidectomy is advised to give a permanent cure for hernia.
Sliding hernia—key points
- Always acquired
- Always (almost) in males
- Always occur in long-standing hernias
- Always irreducible
- Always colon or urinary bladder forms the wall of the sac
- Always requires a repair
- Technical difficulties are always encountered by junior surgeons while operating on these patients
8. Sportsman’s hernia
- This is common in men who play rugby or football wherein injury due to the ball may occur.
- Pain is in the groin radiating to the scrotum and upper thigh.
- On examination, there may be tenderness in the inguinal region.
- Orthopedic disorders must be ruled out first by MRI or CT scan. They are soft tissue injury in the groin, pubic bone diastasis, adductor spasm, etc.
- If the hernia is due to the tearing of muscles (Gilmore’s groin)—it should be repaired in the usual manner.
Leave a Reply