Diagnosis Of Pulpal Pathology Introduction
The assessment of the extent of pulpal pathology is essential to frame the diagnosis. The diagnosis should specify the following:
Table of Contents
- Tissue involved
- Nature of the lesion (acute/chronic)
- Prognosis of the lesion
- Location of the disease
- Aetiology
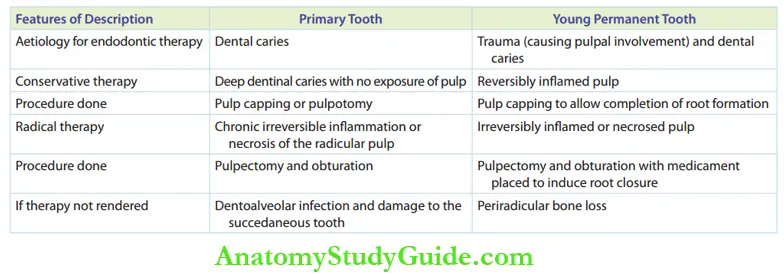
Paediatric endodontic therapy can be indicated for a primary tooth and a young permanent tooth.
The predominant aetiology that necessitates endodontic therapy in primary teeth is dental caries.
Read And Learn More: Paediatric Dentistry Notes
Dental fractures in young permanent incisors and dental caries in young permanent molars are the aetiologies that necessitate endodontic therapy in young permanent teeth.
The diagnosis of the stage of pulpal pathology by identification of the reversible or irreversible character of pulpal inflammation is essential for treatment planning.
Pulpal Pathology Diagnostic Parameters
The diagnosis of pulpal pathology is a composite decision derived on the basis of the following three parameters:
- A history of the presenting illness
- Intraoral and extraoral clinical presentation
- Clinical or radiographic investigation
A lucid history, thorough clinical examination and necessary investigation can help in framing an accurate diagnosis.
Diagnostic Parameters History Of The Presenting Illness
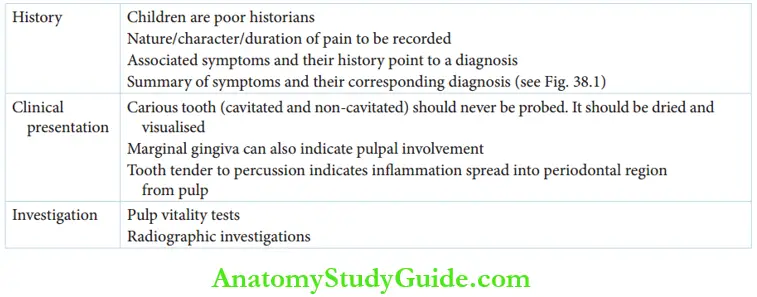
The history can be obtained from the parent or the child. Children are poor at history telling as they may not possess the cognitive capacity to identify or comprehend the symptoms.
A strict cookbook questionnaire approach may not be applicable in this situation.
Questions asked of the child can be framed by the dentist keeping in mind the age and willingness of the child to be able to comprehend the dentist.
A long questionnaire may make a disinterested child highly irritable.
Helps in obtaining a proper history from the parents and the complaints or symptoms that could be derived from their answers.
Deriving the Nature/Magnitude of the Disease from History
Questions for the parents
- Does the child prefer to chew only on one side?
- Is the sleep of the child disturbed?
- Does the child complain of an ant-bite feeling on the teeth?
- Does the child consciously avoid ice creams (cold) or soups (hot)?
- Does the child take too long time to eat too little food?
Descriptive questions to be asked when dental pain is the chief complaint
- The intensity of pain – Sharp and lancinating or dull and less intense
- Aggravating factor – Heat or cold
- Alleviating factor – Painkillers or antibiotics
- Type – Persistent or intermittent pain
- Nature – Spontaneous or on provocation
- Duration – Short duration or long duration
A tooth need not be symptomatic always to show pulpal involvement. A tooth with wide exposure to a pulp chamber and necrosed pulp is almost always asymptomatic.
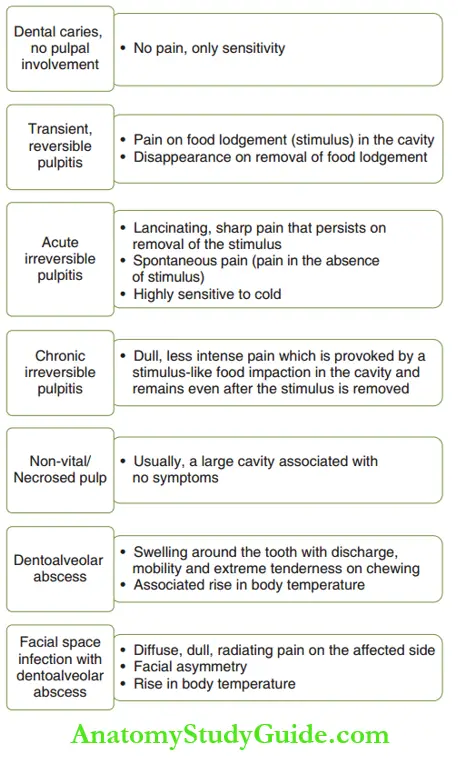
The parent of the child may provide a history of earlier symptoms. enlists the symptoms of the sequelae of pulpal inflammation.
This shall help in arriving at a diagnosis.
Pulpal Diagnostic Parameters Clinical Examination
This includes extraoral and intraoral examinations.
1. Extraoral examination:
It comprises the detection of facial asymmetry and lymph node examination.
- Detection of facial asymmetry: Dentoalveolar infection and subsequent infection of the facial spaces result in facial swelling of the involved side giving rise to facial asymmetry.
- Involvement of buccal space, canine space, submandibular space and submental space presents as diffuse facial swelling.
- Diffuse oedema of lips due to localised dentoalveolar sepsis of central incisors can also be detected during the extraoral examination.
- Lymph node examination: Submandibular, submental, facial and all the other deep cervical lymph nodes along the sternocleidomastoid muscle have to be palpated.
- Lymphadenopa thy makes these nodes palpable and tender to touch. It is most commonly associated with chronic irreversible pulpitis, necrosed pulp, dentoalveolar abscess and facial space involvement due to a dentoalveolar abscess.
2. Intraoral examination:
This comprises the soft-tissue and hard-tissue examination of the oral cavity.
- Soft tissue examination: The marginal gingiva is a marker to identify pulpal involvement.
- An oedematous marginal gingiva around a carious tooth, especially over the furcation area of the tooth, points to a probable pulpal involvement.
- A draining sinus on the attached or marginal gingiva indicates a dentoalveolar abscess.
- Hard-tissue examination: The carious tooth may be examined by inspection, palpation and percussion.
- Inspection: The tooth is observed for the extent of carious involvement and its prospected storability. Carious lesions are always best observed when the tooth is dry. The tooth has to be isolated, air-dried and visualised.
- Palpation: During palpation of the carious tooth, the cavity should not be probed. Probing may lead to pulp exposure or may even cavitate the ‘non-cavitated white spot lesion’.
-
- Wide carious lesions can be superficially excavated with a small, sharp spoon excavator. This removes the debris-laden in the cavity and allows visualising pulp exposure.
- The pulp can be exposed in case of irreversible pulpitis and its sequelae. However, the pulp need not necessarily be visually exposed for it to undergo degradation.
- The stimulus can leach in through the dentinal tubules leading to degenerative changes in the pulp.
- Percussion: When the involved tooth is percussed with the hind side of a mouth mirror, the tenderness elicits inflammation that has spread into the periodontal tissues from the pulp.
-
- A tooth with an acute dentoalveolar abscess is most sensitive to percussion.
Diagnostic Parameters Investigation
Investigations can only support or supplement a diagnosis.
A diagnosis is erroneous if it is purely based on an investigative finding without an emphasis on history or clinical presentation.
Investigations may be clinical investigations or radiographic investigations.
1. Clinical investigation:
Pulp vitality tests are the best modes of clinical investigation in case of pulp inflammation. They are as follows:
- Sensitivity tests: These tests are done to assess the integrity of the nerve supply of the pulp (teeth) as nerve supply cannot exist without a blood supply.
-
- Heat test, cold test, electric test and test cavity preparation are all sensitivity tests.
- Sensibility tests: These tests are done to assess the integrity of the blood supply of pulp. Laser flow, Doppler flowmetry.
-
- Hughes probe eye camera, infrared camera and transmitted light photoplethysmography are sensibility tests.
- However, pulp vitality tests are less commonly used in paediatric dentistry as children are poor historians.
- Vitality tests rely on the patient’s response to the conclusion. The child’s reply may not be as appropriate as required.
- This decreases the sensitivity of the test as the frequency to receive false-positive responses and false-negative responses is higher.
- The children may lack cognitive/communicative maturity to respond to the tests.
Apart from this, the other reasons for not using vitality tests commonly in a pedodontics clinic are as follows:
-
- Dental carious involvement of the pulp is far more common than trauma, where sensitivity tests are more ambiguous.
- Lack of organised infrastructure to supply sensibility test gadgets.
2. Radiographic investigations:
Intraoral periapical radiographs and bitewing radiographs are appropriate supplements for pulpal diagnosis.
Bitewing radiographs are very useful in the diagnosis of the extent of proximal lesions.
An IOPA radiograph is useful in four ways for diagnosis and treatment planning in paediatric endodontics.
- The extent of carious involvement: The breach of pulp by the carious lesion or the amount of the overlying intact dentin indicates the pulpal status and more importantly helps to choose the endodontic procedure.
- Foci of rarefaction (radiolucency) at furcation: The presence of a discrete radiolucency at the furcation area is a contraindication for endodontic therapy.
- A discrete furcal radiolucency implies established dentoalveolar infection with bone resorption.
- Endodontic therapy is contraindicated in such cases because the following reasons:
- The prognosis of therapy is poor as endodontic therapy alone cannot eliminate the septic foci at the furcation.
- The existence of established sepsis at the furcation can cause hypoplastic spots on the developing premolars despite good endodontic therapy.
- Root length of the primary tooth: This decides the strategic importance of the primary tooth to indicate the appropriate endodontic therapy. The foci of internal/external resorption can also be identified.
- Stage of development of the permanent tooth: This also decides the strategic importance of the primary tooth. If the crown formation is incomplete, the primary tooth is very important.
- If it has to be salvaged by extraction, the space has to be maintained till the respective permanent tooth erupts.
Choice Of Endodontic Therapy
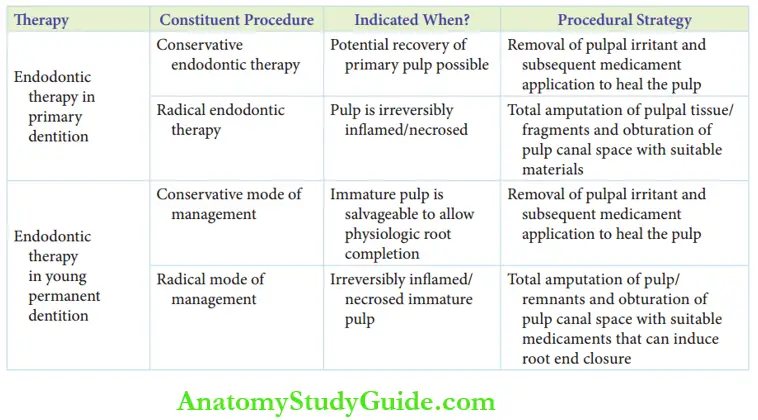
Pulpal involvement warrants pulp therapy or endodontic therapy. The two major groups of endodontic therapy are the conservative mode and the radical mode of endodontic therapy.
1. Endodontic pulp therapy in the primary tooth:
It may be conservative or radical depending upon the extent of involvement of the pulp.
- Conservative endodontic therapy: Thendodontic therapy pertaining to a deep dentinal carious lesion, where the pulp may be inflamed but not exposed, can be termed conservative endodontic therapy.
-
- In this therapy, the pulp is either medicated by the pulp capping procedure or excised partially by pulpotomy.
- These methods are grouped under conservative therapy as all of the pulp is not excavated.
- Conservative endodontic therapy is considered when the recovery of the pulp is possible with partial removal of the pulp, followed by the application of a suitable medicament for healing.
- Radical mode of endodontic therapy: Endodontic therapy involves total amputation of the pulpal tissue by pulpectomy followed by obturation or closure of the pulp.
- Space with a suitable material can be termed the radical mode of endodontic therapy in primary teeth.
- It is performed in teeth showing chronic irreversible inflammation or necrosis of the radicular pulp.
2. Endodontic therapy in a young permanent tooth:
A tooth is specified as a young permanent tooth when it clinically erupts but the root formation is incomplete.
A young permanent tooth has a voluminous pulp chamber and high pulpal horns as pulpal regression has not taken place.
The clinical significance of young permanent teeth can be attributed to the following reasons:
- Pulpal involvement is relatively quicker as enamel is thin and dentinal thickness is only half as compared to that in permanent teeth. Also, dentinal tubules are wider allowing the microorganism to reach the pulp chamber with less resistance.
- Root formation is incomplete, and a healthy vital pulp organ is necessary to complete the root formation.
- The young permanent tooth pulp is highly vascular with a higher proportion of undifferentiated mesenchyme compared to a mature pulp. Hence, the reparative ability or the expected potential for recovery on reversible inflammation is higher.
A conservative or radical mode of endodontic therapy is indicated for young permanent teeth depending upon the extent of inflammation of the pulp.
- Conservative mode of endodontic treatment: It is always preferred in young permanent teeth as the pulp can be left behind to complete the root formation.
- However, it can be done only when the pulp is reversibly inflamed. This means that the pulp can be expected to recover to a normal status on the removal of the irritant and subsequent application of suitable medicament.
- Radical endodontic therapy: When the pulp is irreversibly inflamed or necrosed, a radical mode of endodontic therapy becomes necessary. A medicament has to be placed to induce root closure at the apices.
- If endodontic therapy is not rendered when indicated, an oral septic focus exists.
- Untreated caries in the primary tooth can lead to serious dentoalveolar infections causing a change in the shape/colour/quality (hypoplasia) of the succedaneous tooth.
- Untreated caries in the permanent tooth can result in progressing periradicular bone loss.
- summarises the indications of endodontic therapy.
Indications of Endodontic Therapy
1. The primary tooth should be strategically important, that is, it should be bound to stay in the oral cavity for at least 2 years after treatment.
This is decided on the basis of the following:
- The dental age of the patient
- The presence of at least two-thirds of the root length was checked with the help of a radiograph
2. The tooth should account for optimal post-endodontic storability. The following factors make the tooth non-restorable:
- Carious involvement below the gingiva
- Caries involvement on the walls or floor of the pulp chamber
3. Motivation of parents to bring their children for subsequent appointments and reviews Economic considerations should not be discussed here.
-
- as it is absolutely irrational to choose an affordable treatment plan (extraction) just because the right treatment (endodontic therapy) is not affordable.
- Endodontic treatment need not be contraindicated when it is not affordable by the parent.
- Instead, the patients may be referred to centres that offer these services at affordable prices (as in post-graduate teaching institutions).
- Poor behaviour presentation of the child is also not a contraindication for endodontic therapy.
- A dentist wishing to practice ‘effective paediatric dentistry’ has to appropriately manage the child’s behaviour with psychological/pharmacological modes of behaviour management.
Pulpal Pathology Summary
1. Framing a diagnosis:
The diagnosis of pulpal pathology should specify the tissue involved, nature of the lesion (acute/chronic), prognosis of the lesion, location of the disease and aetiology.
2. Endodontic therapy in paediatric dentistry:
3. Diagnosis is a composite decision based on the following:
4. Investigations:
5. Pulp therapy is indicated in a palpably involved tooth only when
- The primary tooth is strategically important
- The tooth accounts for optimal post-endodontic storability
- The good motivation of parents to bring back children for additional appointments and reviews
- Economic considerations and poor behaviour of the patient are not necessary contraindications
Leave a Reply