Early Childhood Caries Introduction
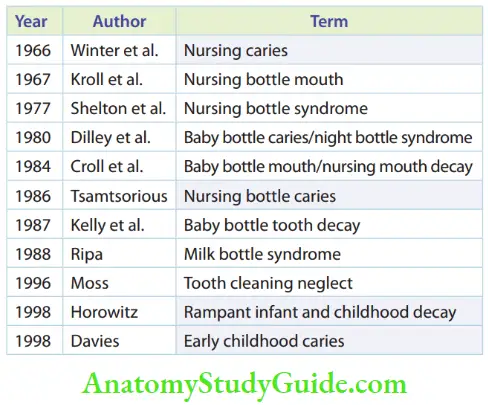
Carious involvement in primary dentition follows a pattern. This pattern of involvement has been distinctively described and appropriately termed by various authors. The terminologies are listed in Table. These terminologies are commonly used in clinical practice, namely nursing bottle caries, rampant caries, and early childhood caries.
Table of Contents
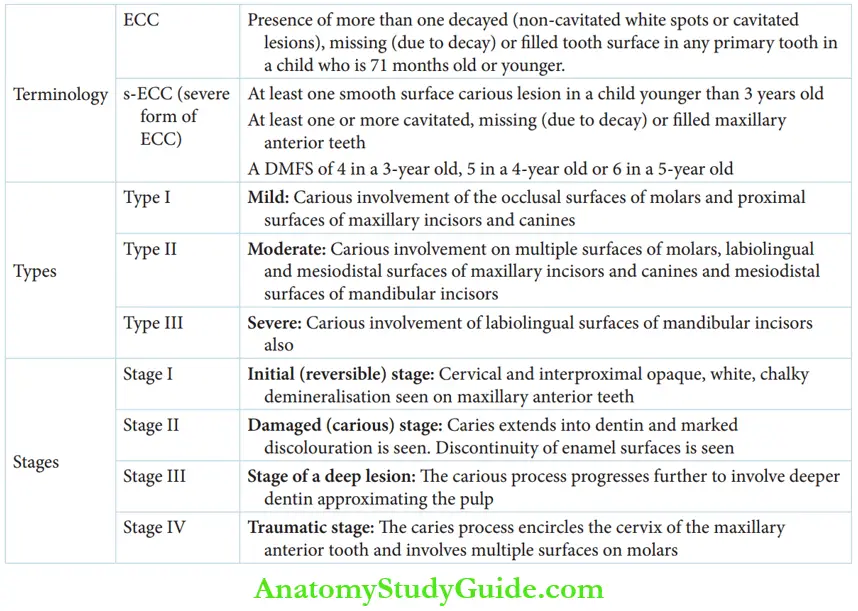
Of these, early childhood caries is a broader term that can envisage the other two common terms. Early childhood caries or ECC has been accepted by the American Academy of Pediatric Dentistry. It is characterised by the presence of more than one decayed
(non-cavitated white spots or cavitated lesions), miss ing (due to decay) or filed tooth surface in any primary tooth in a child of 71 months of age or younger.
| Body Fluids | Muscle Physiology | Digestive System |
| Endocrinology | Face Anatomy | Neck Anatomy |
| Lower Limb | Upper Limb | Nervous System |
Read And Learn More: Paediatric Dentistry Notes
Pattern Of Carious Involvement In Primary Dentition
Early childhood caries can be classified according to the age of occurrence and the extent of the lesion. The table lists the severity of lesions in accordance with the age of the children, namely less than 3 years, 3–5 years, and older than 5 years.
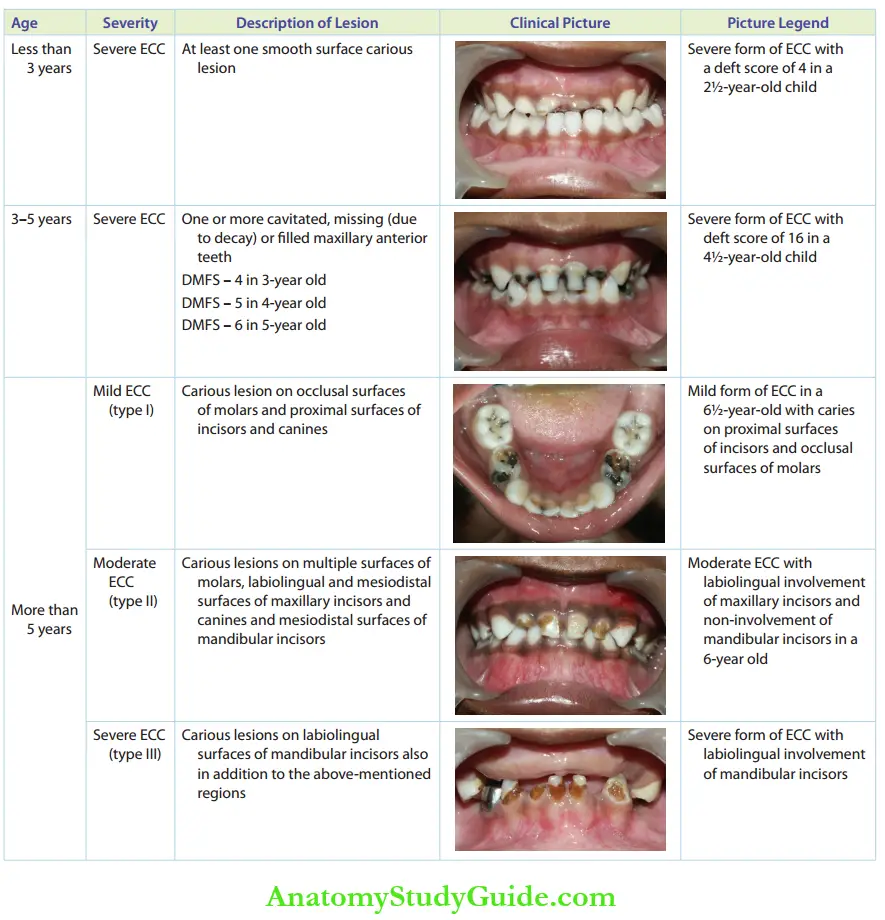
When at least one smooth surface carious lesion is demonstrated in a child younger than 3 years, it is denoted as severe ECC (s-ECC). The DMF scores decide the severity of carious involvement in 3–5-year old children. The extent of involvement can be classified into mild, moderate, and severe in children older than 5 years, depending upon the tooth surfaces involved.
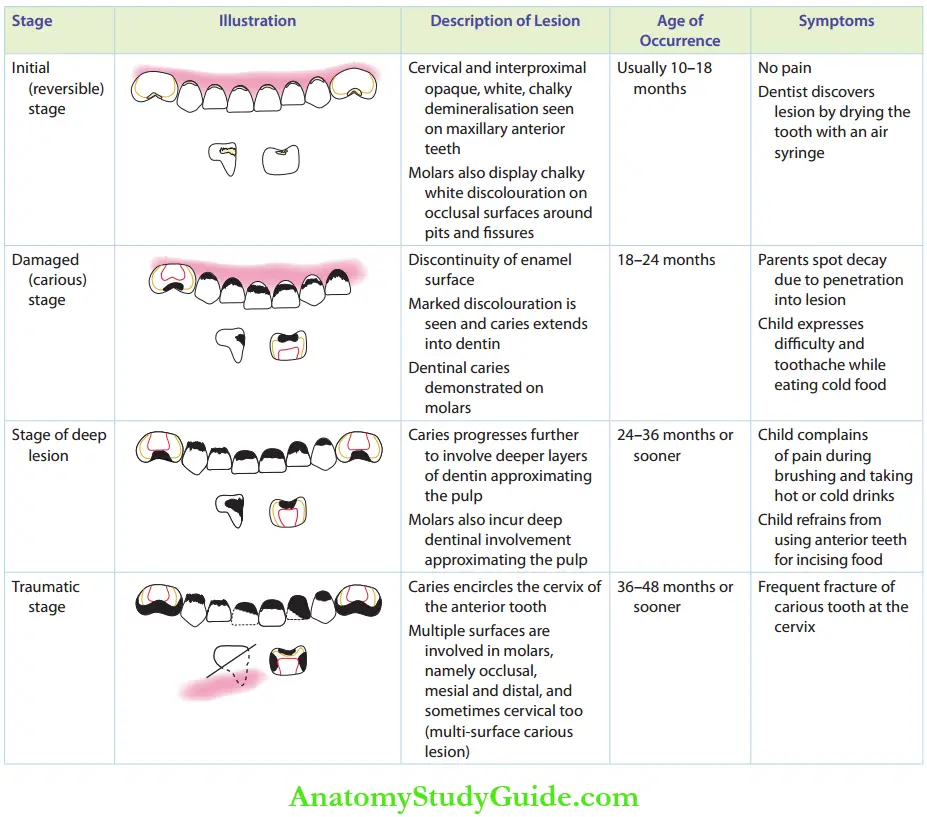
- Stages Early childhood caries has a characteristic rapid progression of decay. It progresses through the following four distinct stages:
- Stage 1: Initial (reversible) stage
- Stage 2: Damaged (carious) stage
- Stage 3: Stage of deep lesion
- Stage 4: Traumatic stageThe description of the lesion in each stage is discussed in Table.
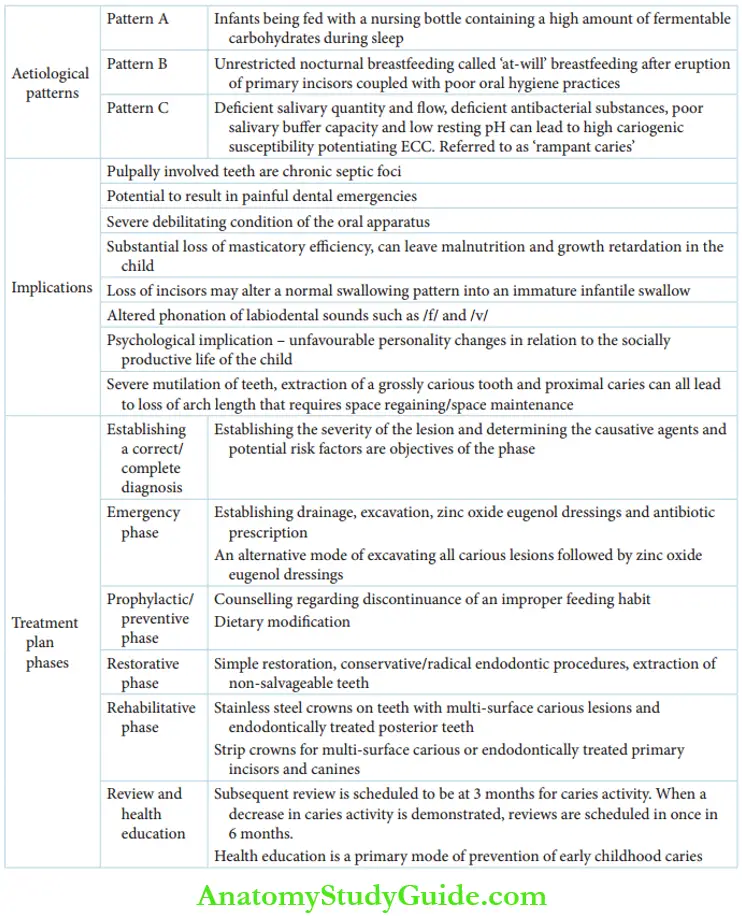
- Aetiology ECC can occur due to three main reasons, which are as follows:
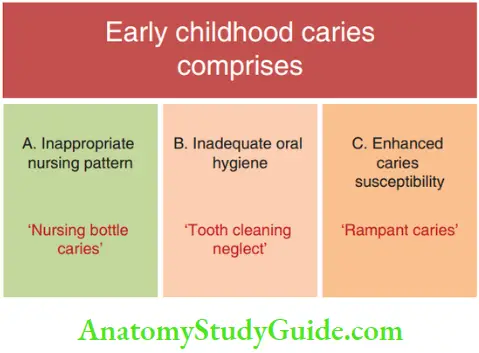
- Pattern A: Inappropriate nursing practices such as nocturnal bottle feeding and unrestricted ‘at-will’ breastfeeding
- Pattern B: Inadequate oral hygiene measures coupled with inappropriate nursing practices
- Pattern C: Enhanced caries susceptibility or poor caries resistance (example poor quality of saliva)
- Of these, the caries arising due to the first reason, or pattern A, can be described as nursing bottle caries. Caries caused due to pattern B can be called tooth cleaning neglect. Dental carious involvement with respect to pattern C refers to rampant caries.
Nursing Bottle Caries
Nursing bottle caries is a unique pattern of dental caries in very young children due to prolonged or improper feeding habits. The infant may be fed with a nursing bottle containing a high amount of fermentable carbohydrates during sleep. The sugary liquid substrate from the bottle pools around the maxillary incisors. This retentive, sugary environment is highly cariogenic.
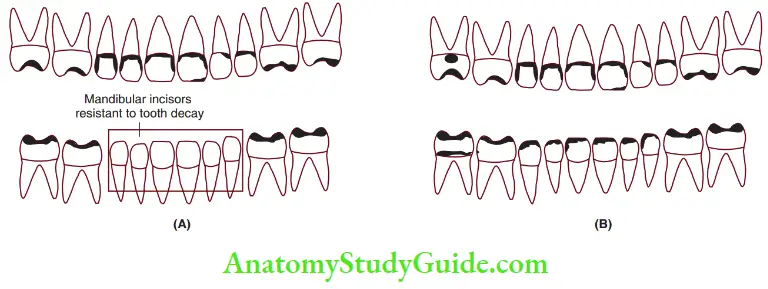
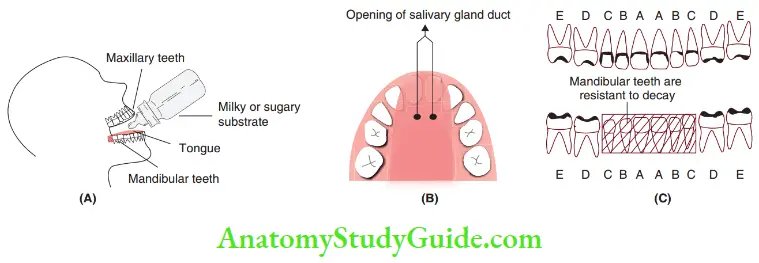 1. (A) Milky or sugary substrate accumulates around maxillary anterior and mandibular and maxillary molar teeth.
1. (A) Milky or sugary substrate accumulates around maxillary anterior and mandibular and maxillary molar teeth.
2. (B) The tongue covers the mandibular anterior teeth.
3. (C) Accumulation of a milky/sugary substrate on the cervical region of maxillary anterior teeth and occlusal surfaces of molars.
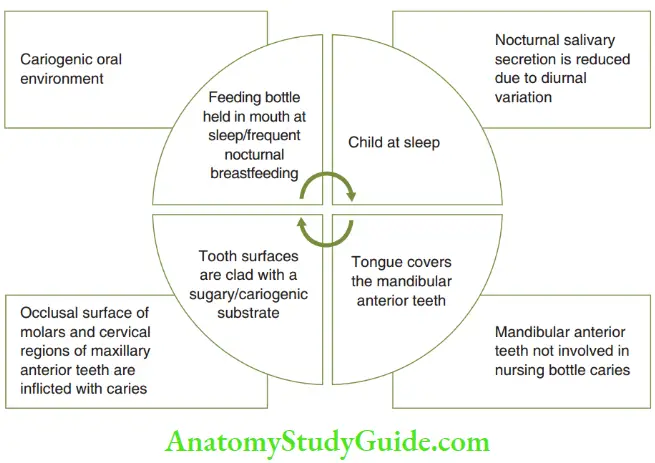
The fact that salivary secretion decreases during sleep also adds to the cariogenicity. Unrestricted nocturnal breastfeeding can be referred to as ‘at-will’ breastfeeding. This type of breastfeeding after the eruption of primary incisors also demonstrates nursing bottle caries.
- The mandibular incisors are usually spared for three reasons, which are as follows:
- The tongue covers the mandibular incisors.
- The salivary duct opens lingual to the mandibular incisors.
- The mandibular incisors are devoid of pits/fissures.
Tooth Cleaning Neglect
‘Tooth cleaning neglect’ implies inefficient oral hygiene measures that increase the susceptibility of young (newly erupted) primary teeth to decay.
The susceptibility to tooth decay is amplified when inadequate oral hygiene is coupled with poor feeding practices, that is, nocturnal bottle feeding and ‘at-will’ breastfeeding. The clinical presentation is primarily that of ECC.
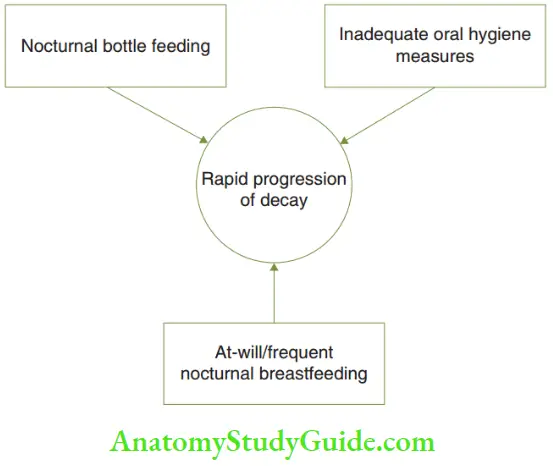
The magnitude of the car ous presentation is higher and carious involvement/progression of decay is quicker. This is so because one feature (inadequate oral hygiene) is coupled with a preexistent decay-susceptible environment with poor feeding practices.
Rampant Caries
Rampant caries is a suddenly appearing, widespread, rapidly spreading, burrowing type (deep decay with a minute opening) of ECC. It affects those teeth that are usually regarded as immune to decay – the mandibular anterior. It results in an early involvement of the pulp owing to its burrowing pattern of spread.
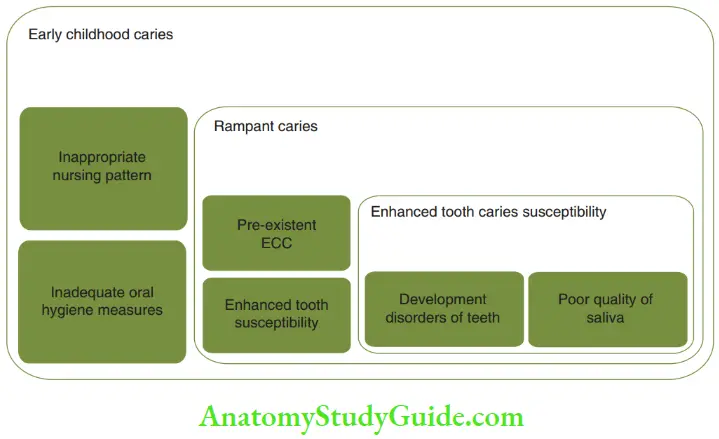
It may occur due to enhanced susceptibility of primary teeth to decay. When inappropriate feeding practices and inadequate oral hygiene measures are coupled with enhanced susceptibility of teeth to decay, the pattern of carious involvement follows a rapid and widespread course. This is typical of rampant caries.
The factors that increase the susceptibility of teeth to the rampant form of ECC are as follows:
- Hypomineralisation of teeth due to developmental causes
- Dentinogenesis imperfect
- Acute xerostomia resulting from systemic causes
- Syndromes or drug intake
- Poor quality/quantity of saliva
- Deficient quantity or flow of saliva
- Deficient antibacterial substances in saliva
- Poor salivary buffer capacity
- Low resting pH
It can be understood that rampant caries is not pertinent to very young children alone. It can occur in children and adults, involving primary and permanent teeth.
- Clinical Implications Of Ecc ECC (nursing bottle caries and rampant caries of the primary dentition) is a seriously debilitating condition of the oral apparatus. It is a very common disease with up to 65% prevalence. ECC can be differentiated well between the two categories. Caries occurring due to inappropriate feeding practices (nursing bottle caries) do not involve the mandibular anterior teeth while caries occurring due to increased tooth susceptibility (rampant caries) involve the mandibular anterior teeth also. Apart from this, it can have serious functional, aesthetic, infectious, and psychosocial implications on the child. They are as follows:
- Infectious implications: Pulpally involved teeth are chronic septic foci unless eliminated. Septic foci have the potential to result in painful dental emergencies.
- Functional implications
- It results in a substantial loss of masticatory efficiency. It can lead to malnutrition and growth retardation in the child.
- Loss of incisors may alter a normal swallowing pattern into an immature infantile swallow.
- Loss of incisors leads to mispronunciation of labiodental sounds – /f/ and /v/. Hence, significant alterations in phonation are induced.
- Psychosocial implication: According to Freud, children develop a primitive peer identity at 4 years. This implies that they compare what they have with their peers. This is coherent with a surge of circulating corticosteroids in the body. The child is very emotional and cannot take upsets. The mental psyche of any child who is made fun of the unaesthetic appearance of the upper front teeth can take two turns:
- The child turns very aversive and violent to stop the bullying.
- The child turns meek and submissive; this is the beginning of an inferiority complex.
- Both these personality changes are unfavorable to the socially productive life of the child.
- Necessitates orthodontic treatment: Severe mutilation of teeth, extraction of a grossly carious tooth, and proximal caries can lead to loss of arch length. Space regaining/space maintenance is required for correction.
- Treatment Plan The treatment is carried out in six phases.
- Establishing a correct/complete diagnosis
- Emergency phase
- Prophylactic/preventive phase
- Restorative phase
- Rehabilitative phase
- Review and health education
- Establishing complete correct diagnosis: Establishing the severity of the lesion and determining the causative agents and potential risk factors are objectives of the phase. A complete history, diet chart, clinical examination, caries activity tests, and radiographic examination can all help to arrive at a specific diagnosis of the cause and measure of caries activity.
- Emergency phase: When the child reports with a dental emergency such as pain, swelling, or an acute abscess, relieving the symptoms is the primary step before structuring a definitive and elaborate treatment schedule. Establishing drainage, excavation of caries, zinc oxide eugenol dressings, and antibiotic prescription are the procedures resorted to appropriately. This procedure
- arrests the progression of decay;
- prevents the incidence of dental emergency till definitive treatment is administered; and
- brings down the number of microbial colonies at large and decreases caries activity.
- Prophylactic/preventive phase: This is the phase of counseling and dietary modification. Counseling is done to discontinue improper feeding habits. Abrupt cessation of the habit is not advised. A gradual withdrawal schedule is framed. The habit must be reduced by 30% at the end of the first week, 50% by the end of the second week, 20% at the end of the third week, and completely between 6 and 8 weeks. Infants must be weaned at 12–14 months of age. On-demand, nocturnal breastfeeding must be denied. Consumption of juices from a bottle should be avoided. Juices should be offered in the cup. Serial dilution is a mode to help toddlers discontinue the bottle-feeding habit. The sugary feed/milk is initially diluted up to 20% with water. mThs dilution is stepped up to 40%, 60%, and 80% serially in 4–6 weeks. Finally, the child is adapted to drinking only plain water (100%) by 8 weeks.
- Restorative phase: It encompasses the following procedures:
- Simple restoration for teeth with no pulp involvement
- Conservative/radical endodontic procedures for a palpably involved tooth
- Extraction of-salvageable teeth
- Rehabilitative phase: It encompasses the following:
- Stainless steel crowns (SSC) on teeth with multisurface carious lesions
- SSC for endodontically treated posterior teeth
- Strip crowns for multi-surface carious or endodontically treated primary incisors and canines
- Review and health education phase: Review is scheduled at 3 months to observe caries activity. When a decrease in caries activity is demonstrated, the review is done once in 6 months. Health education is a primary mode of prevention of ECC. The following lessons are imparted to (expectant) mothers:
- Unrestricted nocturnal breastfeeding should be avoided after the eruption of the first primary tooth.
- Breast milk is the best infant food and is the sole nutrient till the first 6 months. At 6 months, the infant is incrementally, yet systematically, weaned in stages from breast milk to other nutrient supplements. At 1 year, it is recommended by the AAPD that the infant is weaned out of breastfeeding completely.
- When fed at night, the child’s teeth need to be rubbed offers using a wet gauze cloth.
- Infants should not be put to sleep with a bottle containing a sugary feed.
- Parents should encourage infants to drink from a cup as the child approaches the first birthday. Weaning from the bottle should be done at best at 12–14 months of age.
- The infants may be encouraged to use a ‘sipper cup’ than a ‘straw cup’ before changing into a drinking cup to avoid messy spillage.
- Strategic oral hygiene measures comprise rubbing the gum pads/erupted teeth with a wet gauze cloth. It has to be performed even before the eruption of the first primary tooth (dentate jaws).
- A child’s first oral health consultation should occur at the latest by 6 months after the eruption of the first tooth and no later than 12 months of age.
- Regular oral health education and reassurance are necessary to ensure discontinuation of the improper feeding habit.
In conclusion, although appropriate treatment measures exist, prevention alone remains the best method of combating a highly prevalent, distressing, and debilitating condition such as ECC.
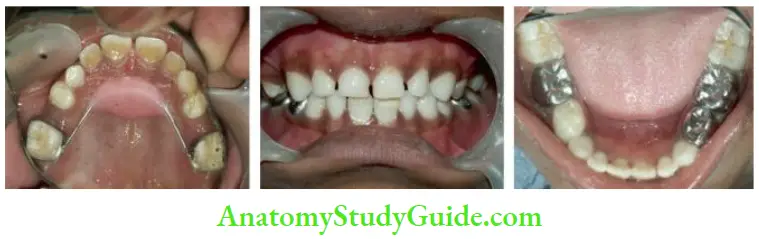
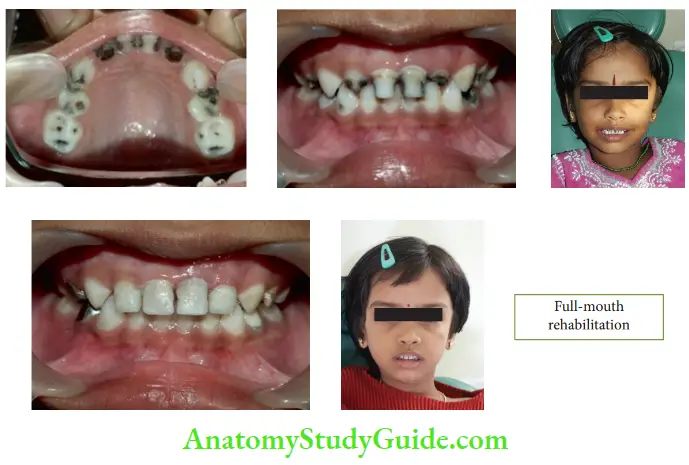
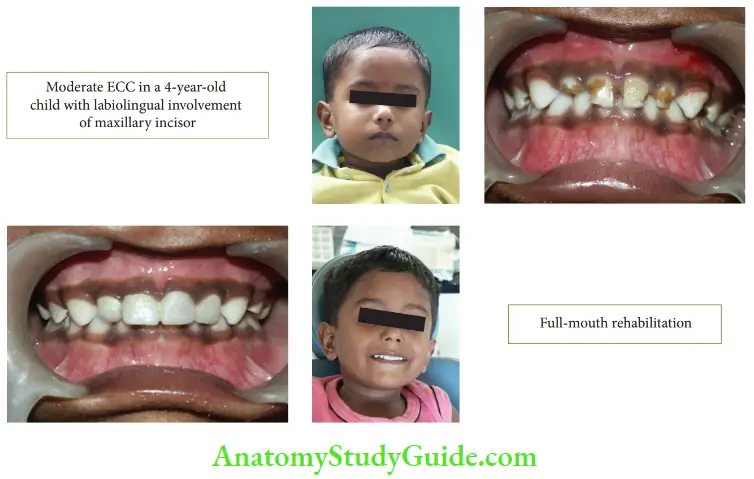
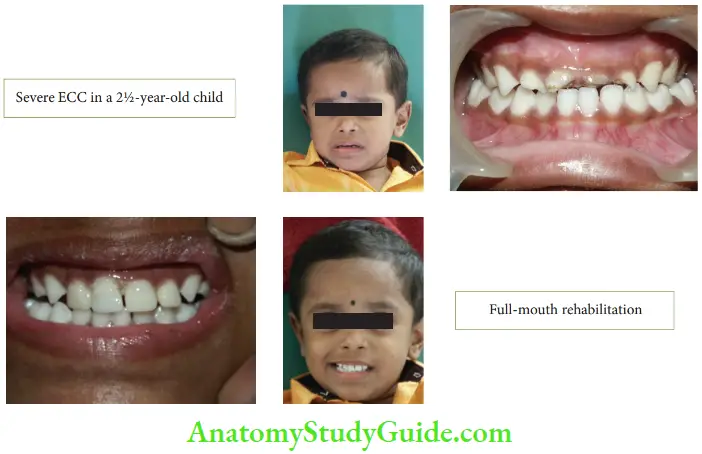
Case Description
Clinical pictures of early childhood caries and treatment with full-mouth rehabilitation.
- Case 1
- Case 2
- Case 3
Early Childhood Caries Summary
Early childhood caries is the most recently accepted terminology proposed by Davies in 1998 to denote rapid widespread carious involvement of primary teeth.
Leave a Reply