Gastrointestinal Tract
Question 1. Write a note on Meckel’s diverticulum.
Answer:
Merkel diverticulum
- The most common true diverticulum
- The most common site is the ileum
- Occurs due to failed involution of the vitelline duct
- The solitary diverticulum extends from the anti-mesenteric side of the bowel
Read and Learn More Preparatory Manual of Pathology Question and Answers
Rule of “2s”
- This occurs in approximately 2% of the population
- Present within 2 feet (60 cm) of the ileocecal valve
- Approximately 2 inches (5 cm) long
- Twice as common in males
- Most often symptomatic by the age of 2 years
Question 2. Write the pathology, morphology, and clinical features of Hirschsprung’s disease.
Answer:
Hirschsprung’s disease
Pathogenesis
- The premature arrest of normal migration of neural crest cells from the cecum to the rectum
- Absence of Meissner submucosal and Auerbach my enteric plexus (“aganglionosis”)
- Peristaltic contractions are absent and functional obstruction occurs
- Results in dilation, proximal to the affected segment
Morphology
- Rectum is always affected
- An aganglionic segment is normal or constricted
- Proximal colon (normal): May undergo progressive dilation, resulting in megacolon
- Intraoperative frozen-section analysis is commonly used for diagnosis
- Microscopy: Absence of ganglion cells within the affected segment
Clinical Features
- Failure to pass meconium in the postnatal period
- Abdominal distention and bilious vomiting
Question 3. Write a note on Barrett’s esophagus.
Answer:
Barrett’s esophagus
- Occurs due to complications of chronic gastroesophageal reflux disease
- Characterized by intestinal metaplasia within the esophageal squamous mucosa
- Associated with an increased risk of esophageal adenocarcinoma
Morphology
- Gross: Patches of red, velvety mucosa extending upward from the gastroesophageal junction
Microscopy
- Intestinal-type metaplasia is seen
- Intestinal epithelium replaces the squamous esophageal epithelium and has goblet cells
- On H&E: Goblet cells have distinct mucous vacuoles that stain pale blue
- Dysplasia: Both low-grade and high-grade dysplasia can be seen
Question 4. Discuss etiopathogenesis and morphology of H. pylori gastritis.
Answer:
- The most commonly affected site is the antrum
Pathogenesis
- Presents as astral gastritis with normal or increased acid production
- Increased risk of duodenal ulcer
The virulence of H. pylori is because of its:
- Flagella: This allows the bacteria to be motile in viscous mucus
- Urease: This generates ammonia from endogenous urea and thereby elevates gastric pH
- Adhesins: Enhance bacterial adherence to the surface foveolar cells
- Toxin: Cytotoxic-associated gene A (CagA) is responsible for disease progression
Morphology
- Within the stomach, H. pylori are most often found in the antrum and are concentrated within the superficial mucus overlying epithelial cells in the surface and neck regions
- Can be detected with special stains like War thin-Starry silver stain, Giemsa stain, and toluidine blue
Gastric biopsy shows
- Neutrophils within the lamina propria and intraepithelial neutrophils
- Pit abscesses and increased plasma cells in the superficial lamina propria
- Increased numbers of sub-epithelial lymphocytes and macrophages
Question 5. Differences between benign and malignant ulcers of the stomach.
Answer:
Benign gastric ulcer
- A peptic ulcer is a round-to-oval, sharply punched-out defect
- The mucosal margin may overhang the ulcer base
- Gastric rugae reach close to the ulcer margin
Malignant gastric ulcer
- Ulcers have characteristic heaped-up margins
- Gastric rugae stop far away from the ulcer margin
Question 6. Discuss in detail the etiopathogenesis and morphology of gastric carcinoma.
Answer:
Pathogenesis
- Intestinal-type gastric cancer is associated with mutations that result in increased signaling via the Wnt pathway and includes:
- Loss of function mutations in the adenomatous polyposis coli (APC) tumor suppressor gene
- Gain-of-function mutations in the gene encoding -catenin
Diffuse gastric cancer is associated with
- Familial gastric cancer—loss-of-function mutations in tumor suppressor gene CDH1, which encodes “E-cadherin”
- Sporadic gastric cancer—E-cadherin mutation
- Loss of E-cadherin—a key step in the development of “diffuse gastric cancer”
Morphology
- Sites—gastric antrum, lesser curvature is more commonly involved than greater curvature
Gastric cancers with intestinal morphology
- Presents as an ulcerated tumor or an exophytic mass
- Tumors are composed of glandular structures
- Tumor cells contain apical mucin vacuoles and mucin may be present in gland lumina
Gastric cancers with a diffuse infiltrative growth pattern
- Tumors produce a desmoplastic reaction that stiffens the gastric wall, leading to a leather bottle appearance termed limit plastic
- Composed of signet-ring cells, which are discohesive, with large mucin vacuoles
- Vacuoles expand the cytoplasm and push the nucleus to the periphery, creating a signet-ring cell morphology
Question 7. Write a note on carcinoid tumors.
Answer:
Carcinoid tumors
- Referred as well-differentiated neuroendocrine tumors
Sites
- The most common site is the gastrointestinal tract
- 40% occur in the small intestine (jejunum and ileum)
- Tracheobronchial tree and lungs are the next most common sites
Morphology
- Gross: Intramural or submucosal masses that create small polypoid lesions
- Cut surface: Yellow or tan in color
Microscopically
- Carcinoids are composed of islands, trabeculae, glands, or sheets of uniform cells with scant, pink granular cytoplasm and a round to oval stippled nucleus
- Rarely, pleomorphism, anaplasia, mitotic activity, and necrosis can be seen
- Immunohistochemical stains are positive for synaptophysin and chromogranin A
Question 8. Discuss intestinal morphology of celiac disease
Answer:
Morphology of celiac disease
- Biopsy sites: Second portion of duodenum or proximal jejunum
Microscopy
- Villus atrophy
- Increased numbers of intraepithelial CD8+ T lymphocytes (intraepithelial lymphocytes)
- Crypt hyperplasia
Note:
- The absence of a gluten-free diet leads to the restoration of normal mucosal histology
- Associations: Blistering skin lesion, dermatitis herpetiformis
Question 9. Write the morphology of Whipple disease.
Answer:
Whipple disease
- Causative agent: Gram-positive actinomycete, Tropheryma whipped
Morphology
- Hallmark is a dense accumulation of distended, foamy macrophages in the small intestinal lamina propria
- Macrophages contain periodic acid—Schiff (PAS)—positive granules that represent lysosomes stuffed with partially digested bacteria
Note:
- A similar infiltrate of foamy macrophages is present in intestinal tuberculosis (PAS positive organisms), however, mycobacteria show AFB positivity, while T. whipped does not
Question 10. Classify inflammatory bowel diseases. Discuss in detail the gross and microscopic morphology of Crohn’s Disease
Answer:
Inflammatory Bowel Disease
- Includes ulcerative colitis and Crohn’s disease
Crohn disease
Morphology
- The most common sites involved in a presentation are the terminal ileum, ileocecal valve, and cecum
- Earliest lesion: Aphthous ulcer, which may progress into elongated, serpentine ulcers oriented along the axis of the bowel
- Skip lesions: Characteristic feature that helps to differentiate from ulcerative colitis
- Strictures are common
- Cobblestone appearance: Diseased tissue is depressed below the level of normal mucosa
- Fissures develop between the mucosal folds and may lead to the development of fistulous tracts
- Creeping fat: Mesenteric fat extends around the serosal surface
Microscopy
- Crypt abscesses: Neutrophils within a crypt
- Crypt destruction and distortion of mucosal architecture
- Hallmark of Crohn’s disease—non-ca seating micro-granulomas
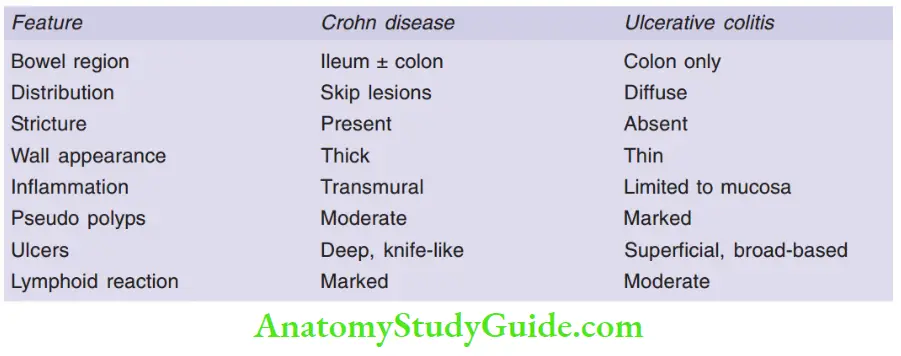
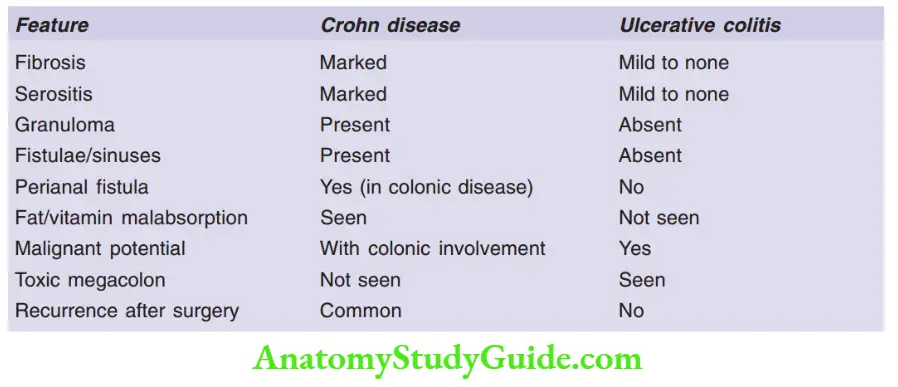
Question 11. Enumerate the differences between Crohn’s disease and ulcerative colitis.
Answer:
Differentiating features between ulcerative colitis and Crohn’s disease
Question 12. Write a note on Peutz-Jeghers syndrome.
Answer:
Peutz-Jeghers syndrome
- Autosomal dominant syndrome
- Presents with multiple GI hamartomatous polyps and mucocutaneous hyperpigmentation
- Associated with increased risk of cancers of the colon, pancreas, breast
- Occurs due to loss-of-function mutations in the gene LKB1/STK11
- The most common site of polyps—is the small intestine, followed by the stomach, colon, bladder, and lungs
- The microscopic hallmark is an arborizing polyp.
Question 13. Write a note on familial adenomatosis polyposis.
Answer:
Familial adenomatous polyposis (FAP)
In autosomal dominant disorder, patients develop numerous colorectal adenomas
- Caused by mutations of the adenomatous polyposis coli, or APC gene
- 100 polyps are necessary for a diagnosis of classic FAP
- Colorectal adenocarcinoma develops in 100% of untreated FAP patients, before 30 years of age
- Extra-intestinal manifestation: Congenital hypertrophy of the retinal pigment epithelium
Question 14. Write about gross and microscopic findings in colon carcinoma.
Answer:
Morphology of colon carcinoma
Gross:
- Carcinomas in the proximal colon (cecum and ascending colon): Polypoidal, exophytic masses that extend along one wall, and rarely cause obstruction
- Carcinomas in the distal colon: Annular lesions that produce “napkin-ring” constrictions and luminal narrowing
Microscopy
- Cuboidal to columnar cells in papillary, glandular, and trabecular pattern
- Pleomorphic nuclei, and increased mitotic activity
- Desmoplastic stromal response
- Abundant mucin accumulation can be seen within the intestinal wall
- Signet-ring cells can be seen
Leave a Reply